")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Impact of COVID-19 Pandemic on Dental Treatment in Children: A Retrospective Cross-Sectional Analysis in Jeddah City
Authors Alamoudi RA , Basudan S, Mahboub M , Baghlaf K
Received 11 January 2022
Accepted for publication 5 April 2022
Published 13 April 2022 Volume 2022:14 Pages 95—102
DOI https://doi.org/10.2147/CCIDE.S353514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Christopher E. Okunseri
Rana A Alamoudi,1 Shahad Basudan,2 Mona Mahboub,2 Khlood Baghlaf1
1Pediatric Dentistry Department, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 2General Dentist, Private Sector, Jeddah, Saudi Arabia
Correspondence: Rana A Alamoudi, Pediatric Dentistry Department, Faculty of Dentistry, King Abdulaziz University, Jeddah, 21589, Saudi Arabia, Tel +966-50-459-9971, Email [email protected]
Background/Purpose: The novel coronavirus disease (COVID-19) outbreak has affected individuals worldwide. Considering the nature of dental treatments and direct exposure to saliva, blood, aerosols, or droplets from infected individuals, dentists are at significant risk of COVID-19 infection. Therefore, to decrease aerosol-generating procedures, minimally invasive dentistry (MID) is recommended during this pandemic. The goal of this research was to compare the flow of patients during a pandemic at a single university hospital in Jeddah City, Saudi Arabia, and to retrospectively assess the impact of the COVID-19 pandemic on pediatric dental treatments including MID.
Materials and Methods: This study was a retrospective cross-sectional analysis of pediatric patient records, dental procedures performed, and minimally invasive techniques using the database of the King Abdul-Aziz University Dental Hospital (R4) system during the period of COVID 19 pandemic compared to the same period in the previous year.
Results: During the COVID-19 pandemic, pediatric dental patient flow included only 699 patients compared to 1151 patients during the same period in the previous year. The most common pediatric dental procedures performed during the pandemic period were simple restorative treatments, including fissure sealants, followed by dental extractions, and fluoride varnish applications. During the pandemic period, more minimally invasive treatments were performed, including the Hall technique, silver diamine fluoride, resin infiltration, and atraumatic restorative techniques.
Conclusion: Based on this data, the COVID-19 pandemic had an impact on dental patient flow and the type of dental procedures performed on children. Minimally invasive treatments that minimize air generation are recommended; however, to establish the long-term effectiveness of minimally invasive treatments in pediatric dentistry, more follow-up studies with bigger sample sizes are required. More recommendations regarding conservative pediatric dental management after the COVID-19 era are suggested.
Keywords: coronavirus, cross-infection, aerosol, minimally invasive dentistry, MID, pediatric dentists
Introduction
In December 2019, a novel coronavirus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified. The virus causes Coronavirus Disease 2019 (COVID-19), which originated in the city of Wuhan, China.1 It is an unpredictable virus that has transmitted rapidly, infecting over 40.6 million people worldwide. The virus transmission from an infected person’s droplets and aerosols released from the mouth or the nose while they are talking, breathing, coughing or sneezing.2
This pandemic, first targeting the communities of China, Europe, and the USA, continues to expand worldwide. The speed of global COVID-19 infection has increased significantly in a short period of time, and has presented a significant challenge to medical and dental schools.3 In response to the pandemic, the WHO considered the outbreak a public health emergency of international concern.1
In Saudi Arabia, the first case was confirmed by the Ministry of Health on March 2, 2020. In order to limit the virus’s transmission, major changes have been implemented in routine dental treatment.4 Since the beginning of the epidemic, dentistry has been suspended in several nations worldwide, causing substantial disruptions in the availability of oral health services.5 In many regions, the COVID-19 pandemic has imposed a major strain on the healthcare system.6
Studies have shown that healthcare providers are considered at higher risk of contamination due to the nature of their work.7 Dental procedures require the dentist to be in close proximity to patients, which violates the recommended one-meter safe distance between individuals.8 Thus, the WHO has updated and added extra safety measures and protocols before and during treatment to minimize the spread of infection between the dentist, patient, and other healthcare workers.9 It is strictly forbidden to perform aerosol-generating procedures (AGPs), such as those that require the use of a handpiece.
An aerosol generating procedure is a medical procedure that creates liquid or solid particles in the air along with those created by the patient from breathing, coughing, sneezing, and talking.10 Droplet is usually large (>5 microns) aqueous bodies. However, the transmission of the COVID-19 virus has been proposed in relation to airborne (or aerosolized) transmission.11
Considering the nature of dental treatments and direct exposure to saliva, blood, aerosols, or droplets from infected individuals, dentists are at significant risk of COVID-19 infection.9 Therefore, minimally invasive dentistry (MID) is recommended during this pandemic. MID is based on three main aspects: 1) understanding of disease etiology and prognosis; 2) oral healthcare measures taken either by the patient at home or by the dentist in the clinic; 3) the preservation of cavitated, carious teeth using preventative modalities.12,13 Several MID techniques are safe and high-quality alternatives to aerosol-generating procedures. These techniques involve pit and fissure sealants (PFS), resin infiltration (RI), silver diamine fluoride (SDF), Hall technique (HT), and atraumatic restorative technique (ART).
Worldwide, few studies had investigated the impact of COVID-19 pandemic on pediatric dental practice.14–16 However, at King Abdulaziz University Dental Hospital (KAUDH), no studies have been conducted to assess the impact of COVID-19 on dental treatments in pediatric patients. The null hypothesis was that COVID-19 pandemic has no impact on pediatric dental treatment. Therefore, the goal of this research was to assess the influence of the COVID-19 pandemic on pediatric dental treatment retrospectively and compare patient flow before and after the pandemic.
Materials and Methods
Study Design
The study design was a retrospective cross-sectional analysis, with ethical approval (#129-11-20), used to evaluate pediatric patient data and procedures performed during the pandemic period. All dental records of pediatric patients who attended dental clinics during the epidemic period between March 2020 and December 2020 were included. We included all pediatric dental patient records during the same period in the previous year (March 2019–December 2019) for comparison.
Study Technique
Data were retrieved from the electronic database (R4) of King Abdulaziz University Faculty of Dentistry (KAUFD). The data collected from the patients’ files included patient demographic data, treatment providers, type of treatment provided, and progress notes. The inclusion criteria were children aged 14 years or younger who were assigned to emergency dental clinics or regular pediatric dental clinics who were classified as ASA I. The data was collected by one calibrated dentist through the electronic filing system. Retrospective analysis of the flow of pediatric dental patients during the epidemic period was performed and compared to the previous year. Additionally, the percentage of medically compromised patients and ASA classification were assessed. All medically compromised patients (ASA II and above) and patients treated or referred to GA were excluded from this study.
Statistical Analysis
All data were anonymized and saved on a password-encrypted desktop. The data were entered in an Excel sheet for more organization and for easier analysis and comparison. Then, the data were entered and analyzed using SPSS Statistical analysis version 22.0 (SPSS Inc., Chicago. II, USA). Descriptive analysis reported the mean, frequencies, and percentages of the outcomes (treatment procedures) and the variables (demographic variables).
Results
Patient Flow and Demographic Characteristics
Table 1 shows the demographic data of pediatric dental patients during the COVID epidemic (2020) and the previous year (2019). At KAUDH, the flow of pediatric dental patients decreased by 60.7% compared to the previous year. During the COVID-19 period from March 2020 to December 2020, only 699 pediatric patients visited the clinic seeking dental treatment, compared to 1151 pediatric patients during the same period in the previous year (March 2019–December 2019).
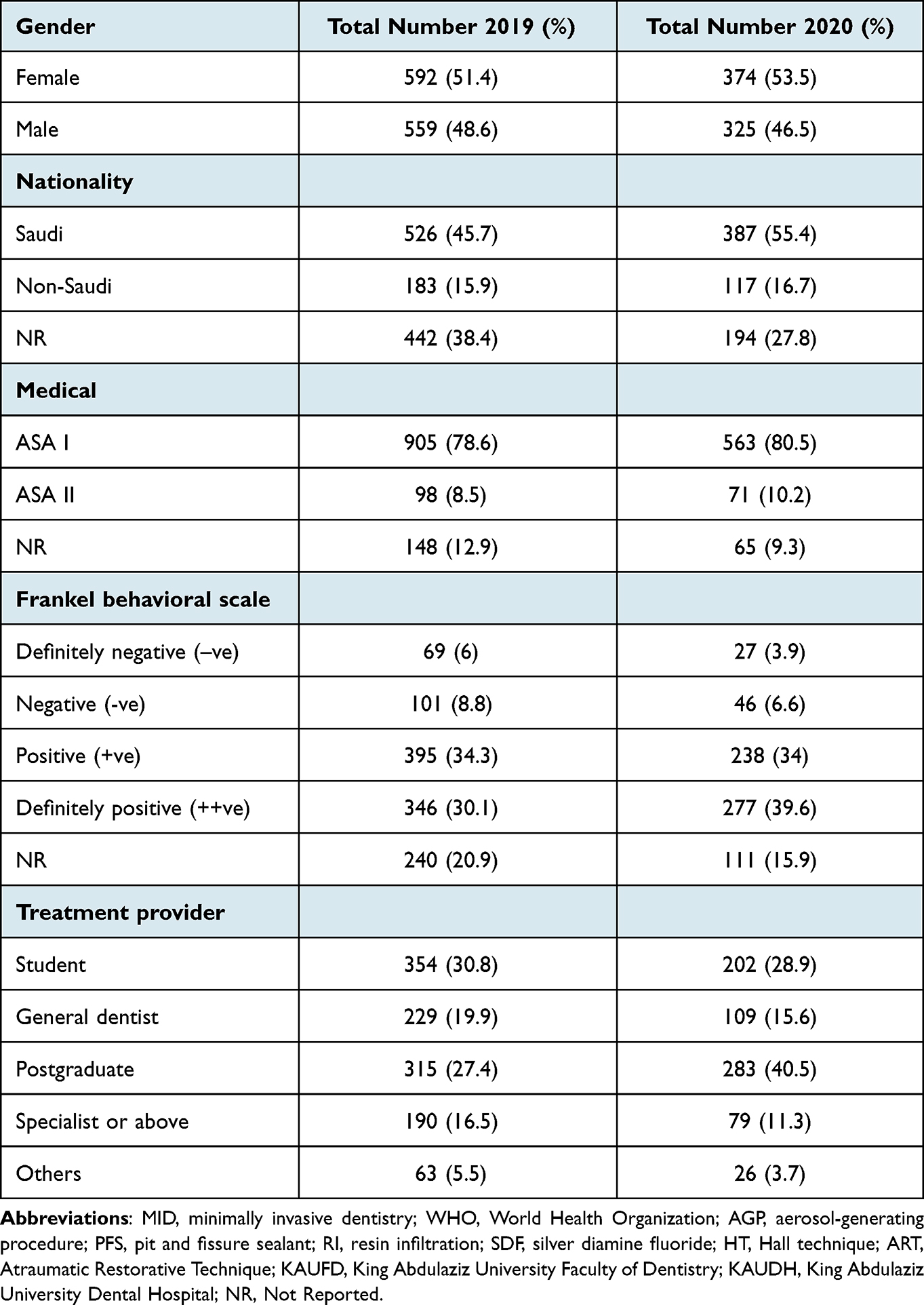 |
Table 1 Demographic Data of Pediatric Dental Patients During the COVID Epidemic in 2019 and 2020 |
In the COVID period (2020), a total of 71 pediatric patients were classified as ASA II, and 25 `were referred to GA, compared to 98 pediatric patients classified as ASA II and 13 cases referred to GA in 2019 (Figures 1 and 2). However, there are no records of patients classified as ASA III and IV.
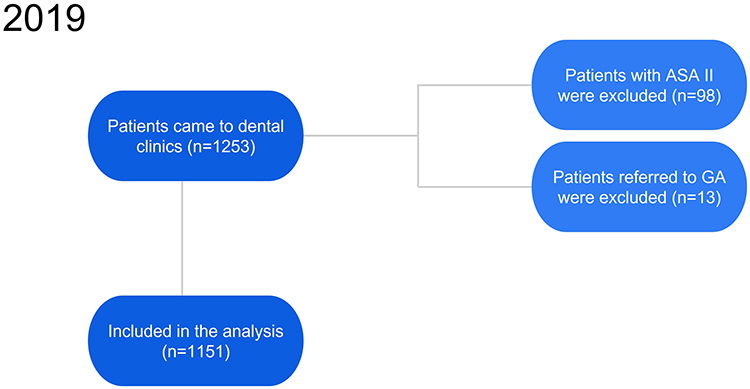 |
Figure 1 Inclusion and exclusion criteria for 2019. |
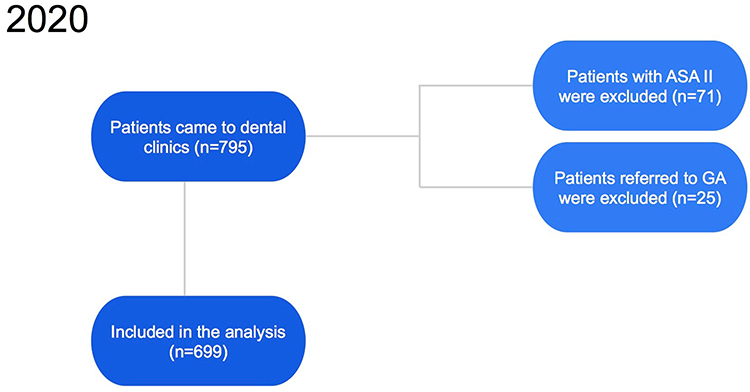 |
Figure 2 Inclusion and exclusion criteria for 2020. |
Out of 1151 patients in 2019, 621 (54%) were 8–11 years old, with a mean age at the time of treatment of 9.5 ± 2.5. During the COVID period of 2020, out of 699 patients, 472 (67.7%) were 6–10 years old with a mean age at the time of treatment of 8.4 ±2.6.
Dental Procedures During COVID-19 Period
Figure 3 shows the number and percentage of pediatric dental procedures performed during the COVID-19 period compared to the same period in the previous year. The percentages of the treatments provided in the two years were comparable, but the most common procedure was performed during the COVID period compared to the previous year was extraction, with 406 (58.10%) and 619 (53.80%) cases, respectively, while the least common procedure in both years was celluloid strip crowns, with 3 (0.30%) and 17 (1.50%) cases, respectively.
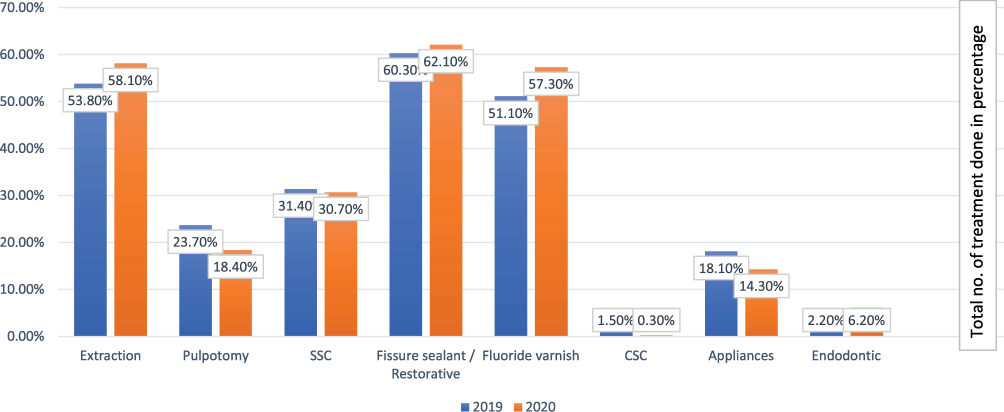 |
Figure 3 Comparison between regular dental procedures during COVID pandemic during (2020) and the previous year (2019). |
Minimally Invasive Procedures During COVID-19 Period
Figure 4 shows the number and percentage of minimally invasive procedures performed during the COVID-19 period compared to the same period in the previous year. During the epidemic period, the Hall technique and ART were used more frequently compared to the same period in the previous year. During the COVID-19 period, the most used technique was the Hall technique, representing 2.2% of the MID treatments used to restore teeth in 15 patients. The least common technique among MID treatments was ART, which was used for only three (0.3%) patients. During the epidemic period, only five (0.7%) patients were treated using SDF.
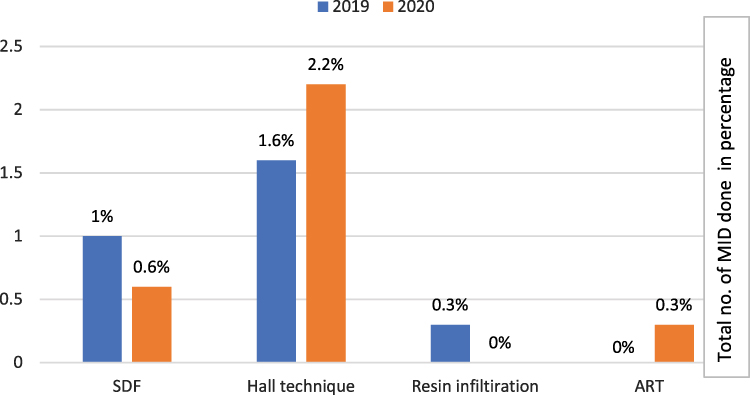 |
Figure 4 Comparison between MID procedures during COVID pandemic (2020) and the previous year (2019). |
Discussion
This study was a retrospective cross-sectional study that aimed to assess the influence of the COVID-19 pandemic on pediatric dental treatment and compare patient flow before and after the pandemic. Additionally, to compare different dental procedures performed, and minimally invasive techniques used during the COVID-19 period at a single university hospital in Saudi Arabia. Similarly to previous published studies in Egypt and China,17,18 the present results showed a reduction of dental care utilization services by children during the epidemic period.
Our findings showed an increase in the GA referral cases during the COVID period. Similarly a recent study conducted in UK,19 explained this increase in GA number as a parental response avoiding dental appointment during COVID pandemic unless their children reported severe dental symptoms. Previous studies have shown that the use of dental handpieces can increase the risk of exposure and transmission of COVID-19 between patients and healthcare workers; thus, the treatment provided to patients should be as minimally invasive as possible, without the use of handpieces, to lower the risk of infection transmission.20,21
In Saudi Arabia, no study has evaluated the use of alternative, non-invasive dental treatments such as ART and SDF, as opposed to dental handpieces, in pediatric patients during the pandemic period. The Ministry of Health (MOH) guidelines recommended the use of conservative techniques to reduce the risk of aerosols during dental treatment.22 These techniques have been used to effectively restore primary carious teeth.13,23 A critical review for the clinical recommendations post COVID-19 by Alhalabi et al showed non-restorative treatment and minimally invasive restorative techniques that generate minimal aerosol are recommended in treating pediatric dental patients.2
The study findings showed that the SDF technique was applied in five (0.7%) pediatric dental patients during the epidemic. Several systematic reviews have assessed the effectiveness of SDF on primary teeth and found that SDF is superior to the other tested techniques in arresting dental caries. Studies have found that SDF is more effective than fluoride varnish and ART.23–29 In agreement with our study’s aim, this study concluded that the use of SDF achieves the World Health Organization (WHO) goals for oral health, contributes to the reduction of caries activity, and provides a minimally invasive treatment method for clinics in pediatric specialties.
Our findings show that the Hall technique is the most common MID technique used during COVID-19. The results also showed that, during the pandemic period, pediatric patients were more frequently treated using the Hall technique compared to the same period in the previous year. The analysis revealed that most patients treated using the Hall technique were treated by postgraduate students. Undergraduate students might not have sufficient knowledge about the prognosis and success rate of the Hall technique. Several randomized clinical trials have assessed the Hall technique and the conventional method clinically and radiographically and found that the Hall technique was slightly superior compared to the conventional stainless steel preparation method.30–33
However, the literature has reported that the Hall technique might temporarily affect occlusion due to the increase in the vertical dimension.34–36 Previous studies have reported that preformed metal crowns can cause an open bite, forcing the patient to cope with premature contact for a few weeks.35 These studies also reported an increase in the occlusal vertical dimension post-operatively for a few weeks after cementation of the crown, and occlusion reestablished after 15–30 days.34–36 Other reported problems in pilot studies related to the Hall technique include TMJ symptoms, reduction in masseter muscle activity, and extrusion of newly erupted permanent molars.37,38
Regarding the other MID techniques, our results show that the ART was used frequently during the pandemic period, but in the statistics of the previous year, no one used this technique. In Nigeria, a study evaluated the placement of ART restorations among primary school children, and after 12 weeks of follow-up, most restorations were sound and intact.39
The main limitation of this study that it was conducted retrospectively. All clinical data was gathered through reviewing patient medical records, which resulted in underreporting of errors. The data collected from the system were taken from each patient’s file individually, specifically from the progress notes written in their files. Some of the data and procedures were not written in sufficient detail for us to collect the information needed for the study, and some dentists did not write any progress notes, which may have affected our study results. One of the limitations of the study is that it was conducted in one dental center so generalizability could not be established. However, King Abdulaziz University Hospital is considered one of the main dental centers in the western region, which has followed the updated of the international dental guidelines. Despite these disadvantages, the data are in line with those of previous studies, which have reported that COVID-19 had an impact on dental flow and on the use of different MID techniques.
Conclusion
The main findings of this study showed that the flow of patients during the COVID-19 period decreased in comparison to the same period in the previous year. The most used minimally invasive dentistry techniques in the pandemic period were the Hall technique, followed by SDF, with a slight difference between them in the same year. More recommendations for minimally invasive dental techniques in pediatric dentistry after the COVID-19 era are suggested. Minimizing air-generating procedures and shifting to less invasive or non-invasive treatment methods is recommended. However, to establish the long-term effectiveness of COVID-19 on pediatric dental treatment, more follow-up studies with bigger sample sizes are required.
Ethics Approval and Informed Consent
This study was conducted according to the guidelines laid down in the declaration of Helsinki and all procedures involving research study documents were approved by the Institutional Review Board of King Abdulaziz University Research Committee (proposal number #129-11-20) in Jeddah, Saudi Arabia. The informed consent was waived for the current study by Institutional Review Board of King Abdulaziz University Research Committee due to the retrospective nature of the study.
Consent for Publication
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. The authors declare that this paper was not published before.
Funding
This work did not receive any funding.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Turkistani KA, Turkistani KA. Dental risks and precautions during COVID-19 pandemic: a systematic review. J Int Soc Prev Community Dent. 2020;10(5):540. doi:10.4103/jispcd.JISPCD_295_20
2. Al-Halabi M, Salami A, Alnuaimi E, Kowash M, Hussein I. Assessment of paediatric dental guidelines and caries management alternatives in the post COVID-19 period. A critical review and clinical recommendations. Eur Arch Paediatr Dent. 2020;21(5):543–556.
3. Aly MM, Elchaghaby MA. Impact of novel coronavirus disease (COVID-19) on Egyptian dentists’ fear and dental practice (a cross-sectional survey). BDJ Open. 2020;6(1):1–5. doi:10.1038/s41405-020-00047-0
4. Ferrazzano GF, Salerno C, Sangianantoni G, Caruso S, Ingenito A, Cantile T. The effect of dental treatment under general anesthesia on quality of life and growth and blood chemistry parameters in uncooperative pediatric patients with compromised oral health: a pilot study. Int J Environ Res Public Health. 2020;17(12):4407. doi:10.3390/ijerph17124407
5. Dar Odeh N, Babkair H, Abu-Hammad S, Borzangy S, Abu-Hammad A, Abu-Hammad O. COVID-19: present and future challenges for dental practice. Int J Environ Res Public Health. 2020;17(9):3151. doi:10.3390/ijerph17093151
6. Tanne JH, Hayasaki E, Zastrow M, Pulla P, Smith P, Rada AG. Covid-19: how doctors and healthcare systems are tackling coronavirus worldwide. BMJ. 2020;368:m1090. doi:10.1136/bmj.m1090
7. Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020;105(1):100–101. doi:10.1016/j.jhin.2020.03.002
8. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
9. World Health Organization. Considerations for the Provision of Essential Oral Health Services in the Context of COVID-19: Interim Guidance, 3 August 2020. World Health Organization; 2020.
10. Morgenstern J. Aerosols, droplets, and airborne spread: everything you could possibly want to know. First10EM blog; 2020:6.
11. Jayaweera M, Perera H, Gunawardana B, Manatunge J. Transmission of COVID-19 virus by droplets and aerosols: a critical review on the unresolved dichotomy. Environ Res. 2020;188:109819. doi:10.1016/j.envres.2020.109819
12. Banerjee A. Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and techniques. Br Dent J. 2013;214(3):107–111. doi:10.1038/sj.bdj.2013.106
13. Leal S. Minimal intervention dentistry in the management of the paediatric patient. Br Dent J. 2014;216(11):623–627. doi:10.1038/sj.bdj.2014.449
14. Jayaraman J, Dhar V, Moorani Z, et al. Impact of COVID-19 on pediatric dental practice in the United States. Pediatr Dent. 2020;42(3):180–183.
15. Ahmadi H, Ebrahimi A, Ghorbani F. The impact of COVID-19 pandemic on dental practice in Iran: a questionnaire-based report. BMC Oral Health. 2020;20(1):1–9. doi:10.1186/s12903-020-01341-x
16. Yang J, Yang G, Jin R, Song G, Yuan G. Changes in paediatric dental clinic after reopening during COVID-19 pandemic in Wuhan: a retrospective study. BMJ open. 2022;12(1):e048430. doi:10.1136/bmjopen-2020-048430
17. Ma H, Hu J, Tian J, et al. A single-center, retrospective study of COVID-19 features in children: a descriptive investigation. BMC Med. 2020;18(1):1–11. doi:10.1186/s12916-020-01596-9
18. Abd Al Gawad R, Hanafy R. The impact of COVID-19 pandemic on the utilization of pediatric dental care of Egyptian children: a retrospective study. Egypt Dent J. 2021;67(1):131–137. doi:10.21608/edj.2020.52574.1396
19. Zaitoun H, Kandiah P, Yesudian G, Rodd H. COVID-19: implications for paediatric dental general anaesthetic services. Fac Dent J. 2020;11(3):114–119. doi:10.1308/rcsfdj.2020.89
20. Abramovitz I, Palmon A, Levy D, et al. Dental care during the coronavirus disease 2019 (COVID-19) outbreak: operatory considerations and clinical aspects. Quintessence Int. 2020;51(5):418–429. doi:10.3290/j.qi.a44392
21. Cirillo N. COVID-19 outbreak: succinct advice for dentists and oral healthcare professionals. Clin Oral Investig. 2020;24(7):2529–2535. doi:10.1007/s00784-020-03323-3
22. Ministry of Health. guidance for providing dental services in governmental and private sectors during COVID-19 pandemic; 2020: 21.
23. Contreras V, Toro MJ, Elías-Boneta AR, Encarnación-Burgos MA. Effectiveness of silver diamine fluoride in caries prevention and arrest: a systematic literature review. Gen Dent. 2017;65(3):22.
24. Gao S, Zhao I, Hiraishi N, et al. Clinical trials of silver diamine fluoride in arresting caries among children: a systematic review. JBR Clin Transl Res. 2016;1(3):201–210. doi:10.1177/2380084416661474
25. Duangthip D, Chu CH, Lo EC. A randomized clinical trial on arresting dentine caries in preschool children by topical fluorides–18 month results. J Dent. 2016;44:57–63. doi:10.1016/j.jdent.2015.05.006
26. Oliveira BH, Rajendra A, Veitz-Keenan A, Niederman R. The effect of silver diamine fluoride in preventing caries in the primary dentition: a systematic review and meta-analysis. Caries Res. 2019;53(1):24–32. doi:10.1159/000488686
27. Trieu A, Mohamed A, Lynch E. Silver diamine fluoride versus sodium fluoride for arresting dentine caries in children: a systematic review and meta-analysis. Sci Rep. 2019;9(1):1–9. doi:10.1038/s41598-019-38569-9
28. Chibinski AC, Wambier LM, Feltrin J, Loguercio AD, Wambier DS, Reis A. Silver diamine fluoride has efficacy in controlling caries progression in primary teeth: a systematic review and meta-analysis. Caries Res. 2017;51(5):527–541. doi:10.1159/000478668
29. Chibinski ACR. The use of silver diamine fluoride in pediatric dentistry. In: Dental Caries. IntechOpen; 2020.
30. Innes NP, Evans DJ, Stirrups DR. The hall technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health. 2007;7(1):1–21. doi:10.1186/1472-6831-7-18
31. Elamin F, Abdelazeem N, Salah I, Mirghani Y, Wong F. A randomized clinical trial comparing Hall vs conventional technique in placing preformed metal crowns from Sudan. PLoS One. 2019;14(6):e0217740. doi:10.1371/journal.pone.0217740
32. Simpson S, Waterhouse P. Hall technique: is it superior in success and savings to conventional restorations? Evid Based Dent. 2020;21(4):128–129. doi:10.1038/s41432-020-0134-2
33. Binladen H, Al Halabi M, Kowash M, Al Salami A, Khamis A, Hussein I. A 24-month retrospective study of preformed metal crowns: the Hall technique versus the conventional preparation method. Eur Arch Paediatr Dent. 2021;22(1):67–75. doi:10.1007/s40368-020-00528-8
34. van der Zee V, van Amerongen WE. Short communication: influence of preformed metal crowns (Hall technique) on the occlusal vertical dimension in the primary dentition. Eur Arch Paediatr Dent. 2010;11(5):225–227. doi:10.1007/BF03262751
35. Gallagher S, O’connell B, O’connell A. Assessment of occlusion after placement of stainless steel crowns in children–a pilot study. J Oral Rehabil. 2014;41(10):730–736. doi:10.1111/joor.12196
36. Nair K, Chikkanarasaiah N, Poovani S, Thumati P. Digital occlusal analysis of vertical dimension and maximum intercuspal position after placement of stainless steel crown using hall technique in children. Int J Paediatr Dent. 2020;30(6):805–815. doi:10.1111/ipd.12647
37. Kaya MS, Kınay Taran P, Bakkal M. Temporomandibular dysfunction assessment in children treated with the Hall Technique: a pilot study. Int J Paediatr Dent. 2020;30(4):429–435. doi:10.1111/ipd.12620
38. Abu Serdaneh S, AlHalabi M, Kowash M, et al. Hall technique crowns and children’s masseter muscle activity: a surface electromyography pilot study. Int J Paediatr Dent. 2020;30(3):303–313. doi:10.1111/ipd.12611
39. Nkwocha F, Akinyamoju G, Ogbode S, Lawal F. Management of dental caries with atraumatic restorative treatment under field condition in primary schools in Oyo State, Nigeria. Ann Ib Postgrad Med. 2019;17(1):75–80.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.