")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 11
Impact of assessment of bone status before corrective surgery of lumbar spine in patients over 50 years old
Authors Banse C, Ould-Slimane M, Foulongne E, Perez A, Avenel G, Daragon A , Vittecoq O
Received 5 December 2018
Accepted for publication 11 March 2019
Published 6 May 2019 Volume 2019:11 Pages 111—115
DOI https://doi.org/10.2147/OARRR.S197218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Christopher Banse,1,2 Mourad Ould-Slimane,3 Emmanuel Foulongne,3 Alexis Perez,4 Gilles Avenel,1 Alain Daragon,1 Olivier Vittecoq1
1Rheumatology Department, Rouen University Hospital, 76000 Rouen, France; 2Rheumatology Department, Polyclinique Saint Côme, 60200 Compiègne, France; 3Department of Orthopaedic Surgery, Rouen University Hospital, 76000 Rouen, France; 4Department of Neurosurgery, Rouen University Hospital, 76000 Rouen, France
Background and objective: There is absence of data on the prevalence of osteoporosis before corrective surgery of the lumbar spine. We do not know the impact of bone assessment before corrective spine surgery, regarding the prevalence of osteoporosis, risk factors for osteoporosis, and prescription of osteoporotic treatment. Our objective was to evaluate the impact of assessment of bone status before corrective surgery of the lumbar spine.
Methods: This retrospective study was conducted over a period of 30 months. Patients included were over 50 years old and had been referred to rheumatology consultation prior to corrective surgery of the lumbar spine with osteosynthesis, for scoliosis or spondylolisthesis. Assessment of bone status consisted in looking for risk factors for osteoporotic fracture, performing bone densitometry with the calculation of TBS (trabecular bone score) and the possible introduction of treatment for osteoporosis. Data were collected on complications related to bone fragility during follow-up.
Results: Twenty-eight patients with a median age of 71.2 years (55.5–84.8) were included; 89% were women. T score was <−2.5 in 14.3% (4/28) and −1 to −2.5 in 42.9% (12/28) on at least one of the three sites analyzed. Fifty percent of patients had a TBS <1.2, a history of more than four falls per year, a duration of more than 20 s in the Timed Up and Go Test, and/or sedation treatment. Vitamin-calcium supplementation and treatment for osteoporosis were prescribed in 71.4% and 17.8% of cases, respectively. During follow-up, 3 patients had one or more osteoporotic vertebral fractures and 4 patients had loosening of implanted devices.
Conclusion: Despite a low prevalence of densitometric osteoporosis and therapeutic management, one in four patients had a bone complication, suggesting the superiority of TBS as an indicator of bone status.
Keywords: osteoporosis, spine surgery, bone evaluation, fracture, TBS
Introduction
With the aging of the population, spine surgeons have to operate older patients with bone fragility associated with osteoporosis.1 Currently, preoperative assessment includes an evaluation by anesthetists, and sometimes by geriatric physicians, to assess the nutritional, cognitive, and functional status of elderly patients. This assessment can help identify patients at risk for perioperative and postoperative complications.2 In this context, before the introduction of implanted devices in the lumbar spine, it could be interesting to assess bone status, and particularly the risk of osteoporotic fracture and loosening of implanted devices.3
The objectives of our study were, on the one hand, to determine the frequency of osteoporosis and its therapeutic consequences (indication or not for osteoprotective therapy) in patients requiring corrective surgery of the spine, and on the other hand, to collect data on fracture complications and/or loosening of implanted devices within 2 years after the surgical procedure.
Methods
This retrospective and longitudinal study was carried out at Rouen University Hospital between February 2015 and August 2017. Patients included were >50 years old and had been referred for a rheumatology consultation for assessment of bone status before corrective surgery of the lumbar spine (scoliosis and spondylolisthesis) with placement of screw. Data collected were: demographic characteristics (age, sex, body mass index, and history of lumbar spine surgery), risk factors for osteoporosis, of falling, and osteoporotic fractures. During the consultation, data on several parameters were collected: the calculation of daily calcium intake, the calculation of the percentage of probability of major fracture at 10 years using the Fracture Risk Assessment Tool (FRAX) score (in the absence of a T score less than −3 and osteoporotic fracture), results of biology tests (serum calcium, blood protein electrophoresis, serum 25 OH vitamin D, blood count, renal function, and liver enzymes) and results of bone densitometry tests using a Hologic Horizon Wi device (T score for the lumbar spine, femoral neck and/or ultra-distal radius as well as calculation of the trabecular bone score). At the end of the bone assessment, the rheumatologist decided on the initiation or not of osteoprotective therapy independently of the indication for spine surgery and in the absence of specific recommendations.4 The characteristics related to spine surgery were: the duration of spinal symptomatology, the maintenance of operative decision, and the search for osteoporotic fractures and/or loosening of implanted devices, occurring within 2 years after the intervention. Patients were followed in consultations by the surgeon who had operated.
Results are presented as medians with lower and upper limits or as percentages.
The study was approved by the noninterventional ethics committee of Rouen University Hospital (E2018-01). Since the study was retrospective, carried out from data collected according to a standardized procedure in usual care, no patient consent is required at the Rouen University Hospital. Only the agreement of the Ethics Committee for retrospective noninterventional studies is sufficient. Declaration of Helsinki was followed in respect to privacy and confidentiality of patient data.
Results
Demographic characteristics
Spine surgeons at Rouen University Hospital referred 28 patients for rheumatology consultation over a period of 30 months. Their characteristics are summarized in Table 1. The median age was 71.2 years (55.5–84.8) and 89% were women. The median body mass index was 30.7 (19.6–50.7) kg/m2; 32% of patients had previously undergone surgery of the lumbar spine.
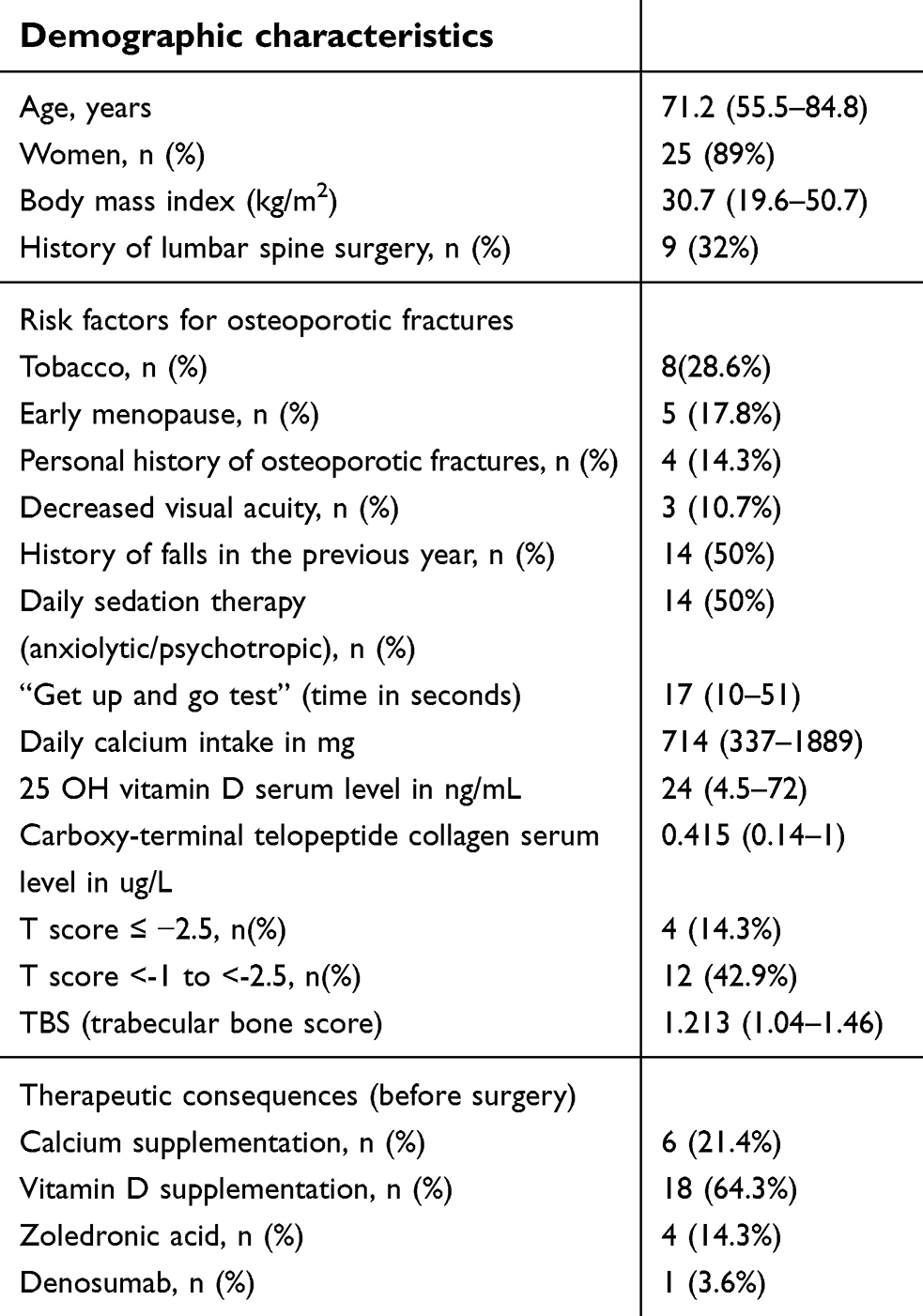 | Table 1 Demographic data and assessment of bone condition prior to surgical correction of the spine in 28 patients |
Assessment of bone status
In our population, risk factors for osteoporosis were: active smoking in 28.6% (8/28), early menopause (<40 years) in 17.8% (5/28), corticosteroid therapy (more than 7.5 mg/day prednisone equivalent), and rheumatoid arthritis in one case (Table 1). Risk factors for osteoporotic fracture were: a history of falls (4 falls per year) in the previous year and sedation treatment in 50% (14/28), a personal history of major osteoporotic fracture in 14.3% (4/28), a decrease in visual acuity in 10.7% (3/28), and a history of fracture of the upper extremity of the femur in first degree relatives. The median duration of the timed-up-and-go test (TUG) was 22.56 (10–51) s with a score >20 s in 44% of cases (11/25). Median daily calcium intakes were estimated at 714 mg (337–1889). Median hydroxy-vitamin D assay was 24 (4.5–72) ng/mL (N: 30–80 ng/mL). The median C-telopetide dosage of collagen was 0.415 (0.14–1) µg/L (N: 0.33–0.88). The results obtained during the rheumatology consultation detected hyperparathyroidism in two patients and monoclonal gammapathy of undetermined significance in one patient. The median T scores at the lumbar spine (n=17), femoral neck (n=27), and at the lower end of the radius (n=10) were −0.6 (−2.9; +3.8), −1 (−2.6; +1.3), and −0.85 (−3.1; +1.5), respectively. Four patients (14.3%) had a T score of ≤ −2.5 and 12 patients (42.9%) had osteopenia (T score <-1 to <-2.5) on at least one of the three sites analyzed. The median trabecular bone score (TBS) was 1.213 (1.04–1.46). Based on the current recommendations,4 six patients were on osteoprotective treatment, four of whom had a history of major fractures, one patient had a T score <–3, and one patient was above the threshold for therapeutic intervention after calculation of the FRAX score.5 The decision to introduce calcium and vitamin D supplementation was applied in 6 and 18 patients, respectively. For four patients, zoledronic acid was introduced, while for one patient, denosumab was initiated. One patient refused osteoprotective treatment.
Impact of bone assessment on surgical procedure
Patients had surgery for static lumbar spine disorder (scoliosis, sagittal disorder) in 71% of cases and/or lumbar spondylolisthesis in 39% of cases. Among these patients, 75% had lumbar spinal stenosis. The surgical decision was maintained in 43% of cases (8 patients were lost due to comorbidities, 4 patients were lost to follow-up, and 3 patients were improved with medical treatment). The median time between surgical consultation and rheumatologic consultation was 84.5 (2–201) days. Four patients had loosening of their implanted device within 2 years of surgery. These patients had no osteoprotective treatment because they were not eligible according to current recommendations (Table 2). Three patients had one or more vertebral fractures in the year following the rheumatologic consultation despite the introduction of zoledronic acid or denosumab for two of them. Of the three patients who developed an operative site infection, two had osteopenia.
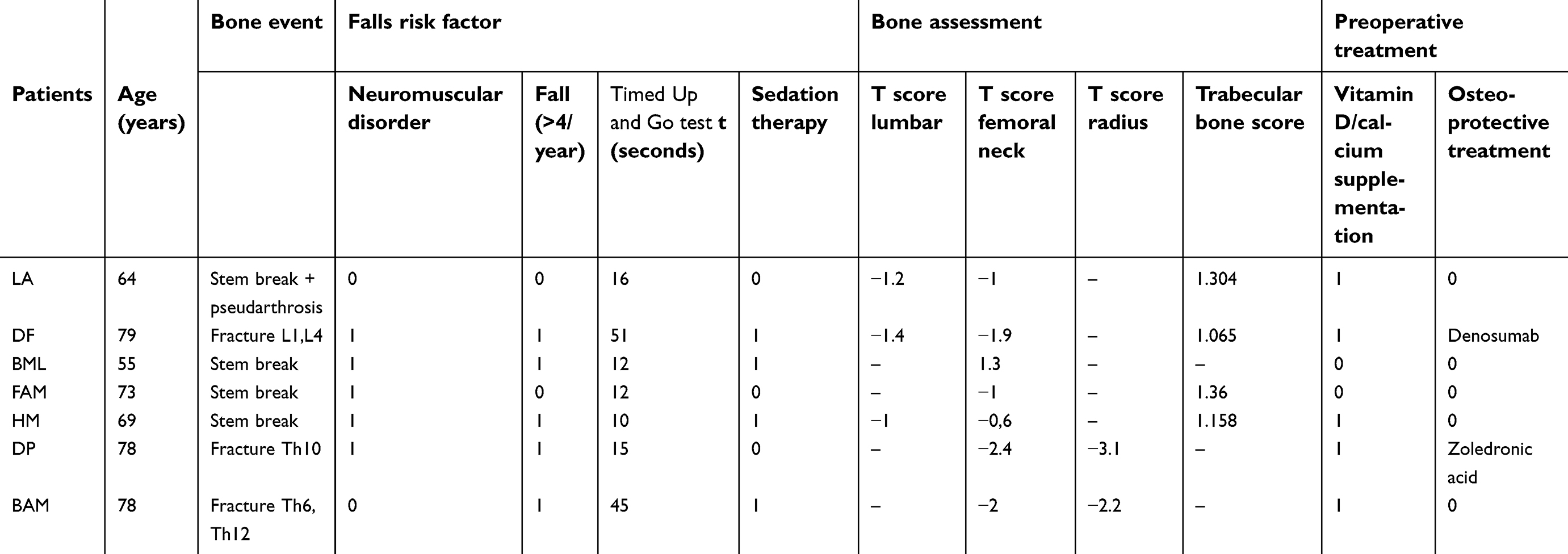 | Table 2 Preoperative data on risk factors for falls, and bone status for each patient who presented an event following corrective spine surgery |
Discussion
Prior to corrective surgery of the lumbar spine, osteoporosis and osteopenia were detected in 14.3% and 42.9% of cases, respectively, in a single-center population of 28 patients over the age of 50 years for whom a status assessment was requested. After assessment, vitamin D/calcium supplementation and osteoprotective treatment were prescribed in 71.4% and 17.8% of cases, respectively. After surgery, three patients had vertebral osteoporotic fractures, while four other patients had loosening of their implanted device.
Osteoporosis is observed in 21.2% of women in the 50- to 84-year age group, 6 representing a higher prevalence than that of the patients in our population with a significant risk of falling. According to James et al, osteoporosis is present in 8.4% of patients waiting for hip or knee arthroplasty.7 To our knowledge, no work has investigated the prevalence of osteoporosis before corrective surgery of the lumbar spine. During follow-up, we observed a prevalence of 25% of vertebral fractures or loosening of implanted devices. In the absence of assessment of bone status, it is not excluded that the impact would have been greater. None of our patients were treated with teriparatide, and only one patient was treated with denosumab because the use of these treatments was restricted in France (at least two vertebral fractures for the first, 3 months of bisphosphonate use in the previous year for the second). However, administration of teriparatide resulted in a significant increase in bone mineral density in 17 patients who had total knee arthroplasty.8 In addition, in another work, denosumab versus placebo reduced the area of peri-prosthetic osteolysis.9 In addition, a TBS <1.2 reflects a poor structural state of bone microarchitecture.10 In our population, 47% of patients were below this threshold. However, it is not a threshold for therapeutic intervention, even though TBS may predict the occurrence of osteoporotic vertebral fracture regardless of densitometric results in postmenopausal white Europeans without osteoporosis.10 In practice, in a population >50 years who must benefit from corrective spine surgery, the value of TBS and the search for risk factors for falls should be taken into account more.
Regarding the occurrence of infection after spine surgery, a Chinese study found osteoporosis as a risk factor for infection of the operative site, with the hypothesis of poor fixation of the implanted device in the vertebra but also a more complex operating procedure (bleeding and longer operative time).11
There are two main limits in this study. First, this study was performed in a population of limited size since among the 28 patients included, only 13 of them have benefited from a surgical intervention. Second, patients of this study have been referred to rheumatology consultation for assessment of bone status prior to corrective surgery, which means they had probably more risk factors of osteoporosis and/or of falls.
Conclusion
Although the number of patients included is low, this is, to the best of our knowledge, the first study to assess both the quantitative and qualitative (bone texture) bone status of an active line of patients over the age of 50 years who had corrective lumbar spine surgery. A quarter of our patients presented a complication related to bone fragility, even though densitometric data were rather reassuring, leading only to low eligibility for osteoprotective treatment. In contrast, our population had risk factors for osteoporotic fractures, including falls and a structural state of altered bone microarchitecture, suggesting the superiority of TBS as an indicator of bone status prior to surgery of the lumbar spine, but a study on a larger population is needed to confirm this hypothesis.
Data availability
Data are available from the corresponding author for 5 years after publication. Send requests to: [email protected].
Acknowledgments
The authors are grateful to Nikki Sabourin-Gibbs, Rouen University Hospital, for her help in editing the manuscript.
No financial support or other benefits from commercial sources were received for the work reported in the manuscript.
Disclosure
Alexis Perez reports a link with MEDICREA, but that does not relate to this work. The authors declare that they have no conflicts of interest in relation to this article.
References
1. Curran D, Maravic M, Kiefer P, Tochon V, Fardellone P. Epidemiology of osteoporosis-related fractures in France: a literature review. Joint Bone Spine. 2010;77(6):546–551. doi:10.1016/j.jbspin.2010.02.006
2. Oresanya LB, Lyons WL, Finlayson E. Preoperative assessment of the older patient: a narrative review. JAMA. 2014;311(20):2110–2120. doi:10.1001/jama.2014.4573
3. Bégué T, Adam P, Fessy MH, et al. Periprosthetic fractures around total hip and knee arthroplasty. Introduction and study objectives. Rev Chir Orthop Reparatrice Appar Mot. 2006;92(5):2S34–2S36.
4. Briot K, Cortet B, Thomas T, et al. 2012 update of French guidelines for the pharmacological treatment of postmenopausal osteoporosis. Joint Bone Spine. 2012;79(3):304–313. doi:10.1016/j.jbspin.2012.02.014
5. Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int. 2008;19(4):385–397. doi:10.1007/s00198-007-0543-5
6. Kanis JA, Johnell O, Oden A, Jonsson B, De Laet C, Dawson A. Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone. 2000;27(5):585–590.
7. James SJ, Mirza SB, Culliford DJ, Taylor PA, Carr AJ, Arden NK. Baseline bone mineral density and boneturnover in pre-operative hip and knee arthroplasty patients. Bone Joint Res. 2014;3(1):14–19. doi:10.1302/2046-3758.31.2000218
8. Suzuki T, Sukezaki F, Shibuki T, Toyoshima Y, Nagai T, Inagaki K. Teriparatide administration increases periprosthetic bone mineral density after total knee arthroplasty: a prospective study. J Arthroplasty. 2018;33(1):79–85. doi:10.1016/j.arth.2017.07.026
9. Sköldenberg O, Rysinska A, Eisler T, Salemyr M, Bodén H, Muren O. Denosumab for treating periprosthetic osteolysis; study protocol for a randomized, double-blind, placebo-controlled trial. BMC Musculoskelet Disord. 2016;17:174. doi:10.1186/s12891-016-1134-4
10. Boutroy S, Hans D, Sornay-Rendu E, Vilayphiou N, Winzenrieth R, Chapurlat R. Trabecular bone score improves fracture risk prediction in non-osteoporotic women: the OFELY study. Osteoporos Int J. 2013;24:77–85. doi:10.1007/s00198-012-2188-2
11. Lai Q, Song Q, Guo R, et al. Risk factors for acute surgical site infections after lumbar surgery: a retrospective study. J Orthop Surg Res. 2017;12(1):116. doi:10.1186/s13018-017-0612-1.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.