")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Impact of arterial hypertension and type 2 diabetes on cardiac autonomic modulation in obese individuals with recommendation for bariatric surgery
Authors Carvalho NNC, de Oliveira Junior FA , da Silva G, Baccin Martins VJ , Braga VA, Costa-Silva JH , Fernandes Pimenta FC, de Brito Alves JL
Received 7 February 2019
Accepted for publication 13 July 2019
Published 21 August 2019 Volume 2019:12 Pages 1503—1511
DOI https://doi.org/10.2147/DMSO.S204414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Nara Nóbrega Crispim Carvalho,1,2 Francisco Antônio de Oliveira Junior,3 Gitana da Silva,4 Vinícius José Baccin Martins,3 Valdir de Andrade Braga,5 João Henrique da Costa-Silva,6 Flávia Cristina Fernandes Pimenta,4 José Luiz de Brito Alves1
1Department of Nutrition, Health Sciences Center, Federal University of Paraiba, João Pessoa, Brazil; 2Department of Endocrinology, Lauro Wanderley University Hospital, Federal University of Paraiba, João Pessoa, Brazil; 3Department of Physiology and Pathology, Health Sciences Center, Federal University of Paraiba, João Pessoa, Brazil; 4Lauro Wanderley Hospital, Federal University of Paraiba, João Pessoa, Brazil; 5Department of Biotechnology, Center of Biotechnology, Federal University of Paraíba, João Pessoa, Brazil; 6Department of Physical Education and Sport Sciences, Federal University of Pernambuco, Vitória De Santo Antão, PE, Brazil
Correspondence: José Luiz de Brito Alves; Nara Nóbrega Crispim Carvalho
Department of Nutrition, Federal University of Paraiba, Campus I – Jd. Cidade Universitária, João Pessoa, PB CEP: 58051-900, Brazil
Tel/fax +55 8 199 845 5485
Email [email protected]; [email protected]
Background and aim: Obese individuals with recommendation for bariatric surgery (BS) exhibit increased cardiovascular risk. The association of obesity with comorbidities, such as arterial hypertension (HTN) and type 2 diabetes mellitus (T2DM) can worsen cardiovascular dysfunction. This study aimed to investigate the effect of HTN on cardiac autonomic function and whether diabetes exacerbates HTN-related impairment of autonomic function in obese subjects.
Methods: Samples (n=63) were allocated to three groups: Obese without HTN and T2DM (n=29), Obese with HTN (OHTN, n=17) and OHTN with T2DM (OHTN+T2DM, n=17), in which anthropometric measures, body composition, blood biochemical parameters, blood pressure (BP) and heart rate variability (HRV) were evaluated.
Results: The age was higher in OHTN+T2DM and OHTN than in obese groups (p<0.05). OHTN+T2DM individuals had increased neck circumference and compromised glycemic profile when compared to obese and OHTN groups (p<0.05). Mean values for standard deviation of RR (SDRR), square root of the mean squared differences of successive RR interval (RMSSD) and number of pairs of successive normal-to-normal beat intervals that differed by 50 ms (pRR50) were significantly lower in OHTN+T2DM and OHTN groups when compared to patients with obesity alone (p<0.05). The low frequency (LF), low frequency/high frequency (LF/HF) ratio were higher in the OHTN+T2DM and OHTN than subjects with obesity alone (p<0.05). Nonlinear parameters SD2 and SD1 were also lower in the OHTN+T2DM when compared to the obese group (p<0.05). However, the SD2/SD1 ratio was higher in the OHTN+T2DM and OHTN groups than the obese group. 
Conclusion: T2DM and/or HTN impair the cardiac autonomic function in obese patients. However, the presence of T2DM did not exacerbate the hypertension-related impairment of autonomic function.
Keywords: heart rate variability, blood pressure, glucose metabolism, obesity, cardiovascular risk
Introduction
Obesity is a chronic disease of high prevalence and complex management. In most cases, the excessive body weight has been associated with several comorbidities, such as type 2 diabetes mellitus (T2DM), arterial hypertension (HTN), dyslipidemia and obstructive sleep apnea syndrome, which contribute to high cardiovascular morbidity and mortality in this group of patients.1,2
The sympathetic activity and sympathovagal tone imbalances are markedly increased in obese subjects,3 which are independently associated with increased cardiovascular risk.4–6 In addition to obesity, diabetes and HTN are comorbidities that impair the cardiac autonomic function.7 For example, among patients with diabetes, the mortality rate is higher in those with autonomic dysfunction than in those subjects with well-controlled autonomic function.5,8,9
Weight loss has been associated with a remarkable improvement in the autonomic cardiac function.3,10–12 However, sustained weight loss in morbidly obese patients is difficult and repeatedly unsuccessful. Thus, bariatric surgery (BS) has been considered the more effective treatment approach for these patients.13 Despite BS has been shown effective in reducing body weight, the improvement of comorbidities and greater weight loss after BS is not always satisfactory achieved. As a result, cardiac autonomic dysfunction (CAD) in obese subjects prior to BS is associated with a lower resolution of those comorbidities after surgery.14
The early CAD may exhibit no symptoms and only be detected by abnormal indices of heart rate variability (HRV). The HRV reflects the oscillation in the time intervals between consecutive heartbeats (usually stated as RR intervals) and is extensively used to evaluated autonomic modulation of the cardiac function.7,15,16 Reduced HRV is associated with increased sympathovagal tone in several disorders such as HTN, diabetes7 and, obesity17 and predicts greater cardiovascular risk. The association of these comorbidities, such as diabetes and HTN, appears to impair HRV more than either the diseases alone.18
In this way, the understanding of the autonomic function in obese subjects with or without comorbidities before BS might be essential for predicting clinical outcomes after surgery. Therefore, the aim of the study was to examine the impact of HTN with or without T2DM on HRV in obese subjects with a recommendation for BS.
Methods
Ethical aspects of the research
This cross-sectional study was conducted in accordance with the Declaration of Helsinki. The protocol of the original study entitled “Cardiovascular, metabolic and muscular evaluation in sarcopenic and non-sarcopenic obese patients indicated for bariatric surgery” was submitted and approved by the Research Ethics Committee of Lauro Wanderley University Hospital, Federal University of Paraiba (Reference number 80984817.9.0000.5183) and all procedures were conducted in agreement with the Resolution 466/2012 of the National Health Council and the International. After the patients gave written informed consent they underwent screening procedures.
Subjects
Obese subjects aged 18–60 years, BMI ≥40 kg/m2 or ≥35 kg/m2 with a recommendation for BS and belonging to the surgical obesity outpatient clinic of Lauro Wanderley University Hospital were included in the study between March and September 2018.
Exclusion criteria consisted of a history consistent with pregnancy, cardiac transplantation, presence of arrhythmias (eg, ventricular atrial block, atrial fibrillation), cardiac pacemakers, clinical history of renal dysfunction, ischemic and non-ischemic cardiomyopathy, important psychiatric diseases and active malignant neoplasms.
The participants were divided into three groups: 1) obese individuals without diagnosis of HTN and T2DM (obese, n=29); 2) obese individuals with diagnosis of HTN (OHTN, n=17); and 3) obese individuals with diagnosis of HTN and T2DM (OHTN+T2DM, n=17). All participants underwent a careful clinical assessment before the study.
Clinical and anthropometric evaluation
A questionnaire was administered to participants in order to retrieve information regarding their age, sex, physical activity (moderate physical activity ≥150 min/week), nutritional counseling, smoking, previous diseases, time of illness and use of medication. The duration of T2DM and HTN was recorded based on the date of diagnosis self-reported by patients.
Body weight was measured to the nearest 0.1 kg (Inbody 370, Model JMW140, Chungcheongnam-do, KOREA). Height was measured to the nearest 0.5 cm using a stadiometer (anthropometric balance caumaq mechanical capacity 300 kg) and BMI (kg/m2) was calculated as the weight divided by the square of the height (Kg/m2). Neck circumference (NC) was measured using a flexible ruler at the thyroid cartilage level.19
Assessment of body composition
The body composition was evaluated by bioimpedance (Inbody 370, Model JMW140, Chungcheongnam-do, KOREA), tetrapolar, multifrequency, segmental, with 15 impedance measurements using 3 different frequencies (5 KHz, 50 KHz, 250 KHz) of each of the 5 segments (right arm, left arm, right leg and left leg) through an electric current of 250 μA.
To perform the test, all subjects follow the following recommendations: fast for 12 hrs, empty the bladder before the test, do not perform extenuating or vigorous physical exercises the day before, not being in the menstrual period and the ambient temperature is between 20 and 25 ºC. Body fat percentage was provided from the manufacturer’s algorithm.20
Blood sample and biochemical analyses
Blood samples were collected with fasting of 12 hrs, without alcoholic beverage intake 72 hrs before. Fasting glucose, cholesterol, triglycerides, and high-density lipoprotein cholesterol (HDL-cholesterol) concentrations were determined with an automated enzymatic method (Autoanalyzer; Technicon, Tarrytown, NY, USA). LDL cholesterol was calculated using the Friedwald formula.21 Fasting insulin was determined with the chemiluminescence immunoassay kit (Siemens Healthcare Brasil). The insulin resistance was estimated with the homeostasis model assessment of insulin resistance (HOMA) method22 and glycated hemoglobin (HbA1c) was measured by high-performance liquid chromatography-HPLC (method certified by the National Glycohemoglobin Standardization Program).23 Lastly, high sensitivity quantitative C-reactive protein (C-RP) was measured by turbidimetry.24
Blood pressure, electrocardiogram recording and heart rate variability analysis
All subjects abstained from intense physical activity 24 hrs prior to examination. In addition, patients abstained from caffeinated beverage consumption or any stimulant drink 36 hrs prior to blood pressure (BP) and electrocardiogram (ECG) recording25 as well as no alcohol intake 72 hrs prior to the observations. Lastly, patients were asked to fast overnight for 12 hrs before ECG.
The recordings were performed during the morning (8 AM–11 AM) in a quiet room. The BP was measured in seated subjects after 3 mins of rest, through the Welch Allyn sphygmomanometer with appropriate arm circumference cuff following the recommendations of the 2013 ESH/ESC Guidelines for the management of arterial hypertension.26
After an initial stabilization period of 5 mins, subjects were instructed to remain silent, breathing normally at tidal volume and with the subjects at rest and in the supine position.16 Following, ECG measurements were recorded for 10 mins. The ECG model 26T-LTS (ADinstruments®, Bella Vista, NSW, Australia) was used and recordings were made with the 5-electrode configuration through LabChart® data acquisition software (ADinstruments®, Bella Vista, NSW, Australia). ECG was set to a sampling rate of 1 KHz, range of 2 millivolts using a digital filter of 50 Hz (low pass). All data were exported and blindly analyzed by an independent trained researcher using LabChart 8 software.
ECG recordings were processed by computer software (ECG analysis module for LabChart Pro; ADInstruments) for automatic detection of the R waves and beat-by-beat calculation of RR interval. For detection of ECG, 80 ms was used to determine typical QRS width and for R waves at least 300 ms apart. For ECG analysis, 240 ms was used for the maximum PR and 240 ms for maximum RT.
The heart rate (HR) and the following measures of HRV analysis were determined; 1) time-domain parameters: average R-R interval, standard deviation between the duration of RR intervals (SDRR), the square root of the mean of the sum of the squares of the successive differences between adjacent normal-to-normal beats (RMSSD), and the number of pairs of successive normal-to-normal beat intervals that differed by 50 ms (pRR50); 2) frequency-domain parameters: low frequency (LF) band (from 0.04 to 0.15 Hz) and high frequency (HF) band (from 0.15 to 0.40 Hz) and the LF/HF ratio, the power of each spectral component was calculated in normalized units (un); 3) Nonlinear parameters (SD1 and SD2). Poincaré scatters plots were constructed and investigated as a nonlinear tool, including the transverse axes (SD1, an indicator of parasympathetic activity) and the longitudinal axes (SD2, an function of sympathetic and vagal activity).12,15
Statistical analysis
Values are reported as mean (95% confidence interval). The variables age and NC were analyzed using one-way ANOVA test, following Tukey post-test. BP, body composition, biochemical parameters, ECG analysis and HRV measures were analyzed using one-way ANCOVA with correction for age and NC. Categorical data were analyzed by chi-square. The Pearson correlation coefficient (r) was used to explore the relationship between the clinical, anthropometric, body composition and laboratory variables obtained with the HRV parameters. The correlations obtained were classified as poor (r≤0.20), weak (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80), and excellent (0.81–1.00).27,28 Differences were considered significant when p≤0.05. ANCOVA and chi-square were performed using SPSS 20.0 (IBM Corporation, Armonk, NY) and the others statistical analyses were performed using the GraphPad Prism 5.0 software (GraphPad Software Inc., La Jolla, CA, USA).
Results
Subject characteristics
Sixty-three obese individuals with a recommendation for BS were evaluated over a six-month period. Clinical, anthropometric, body composition and laboratory characteristics of subjects studied are shown in Table 1.
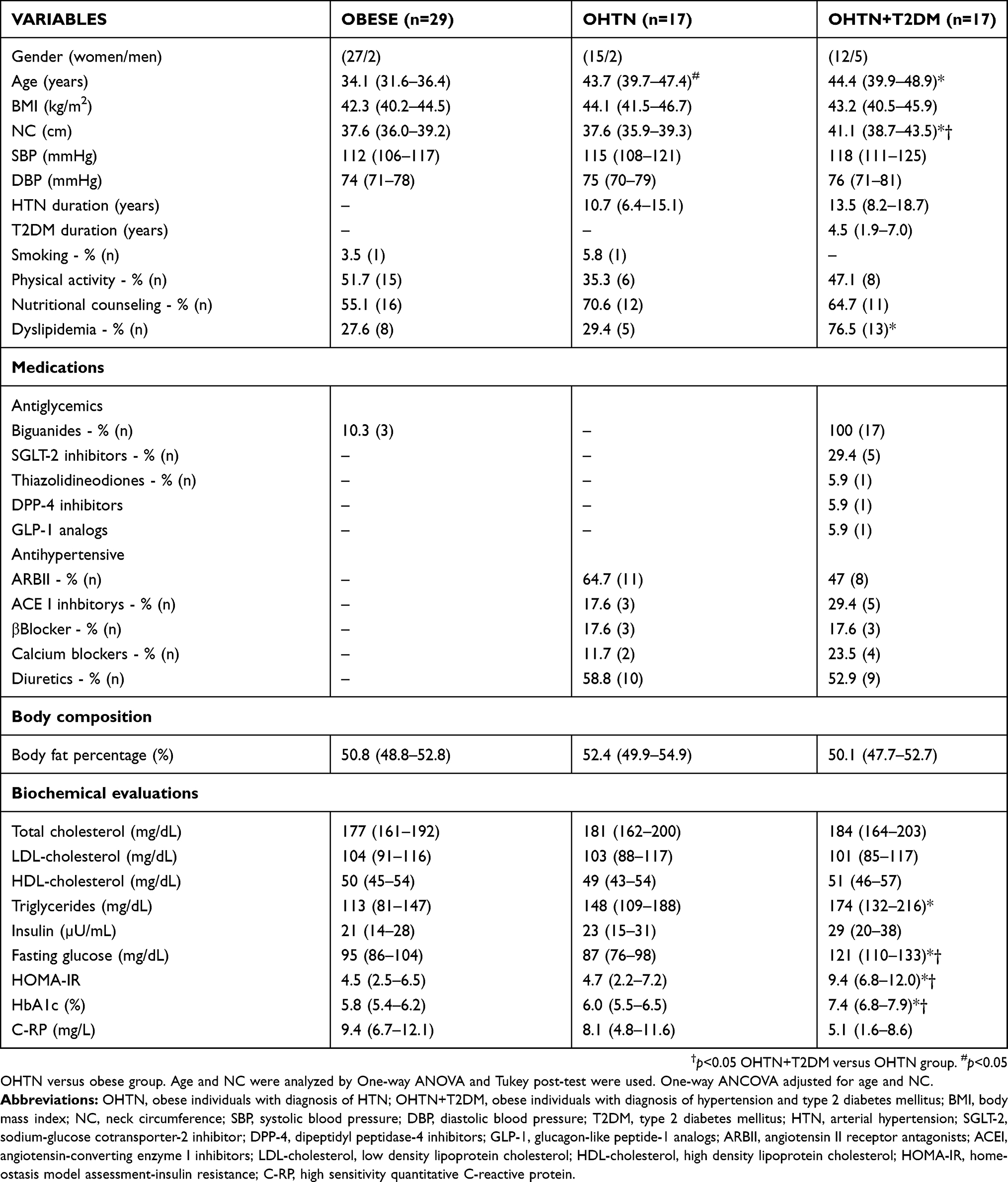 |
Table 1 Assessment of clinical, anthropometric, body composition and laboratory variables |
The study sample included three groups: 29 obese patients (mean BMI of 42.9±4.3 kg/m2), 17 OHTN (mean BMI of 43.7±6.1 kg/m2) and 17 OHTN+T2DM (mean BMI of 44.1±7.1 kg/m2). OHTN and OHTN + T2DM groups were older than the obese subjects, p<0.05. NC was higher in OHTN+T2DM than OHTN and obese groups (Table 1).
Although the BMI and body fat percentage were similar among groups, the OHTN+T2DM subjects presented worse glycemic profile (fasting glucose, HOMA-IR, and HbA1c) than the obese and OHTN. In addition, subjects of OHTN+T2DM group showed higher triglycerides when compared to obese individuals (Table 1). Due to differences in age and NC between groups, all other results were corrected for these variables.
The comparison among the groups studied for HRV in the time domain, frequency domain and nonlinear measurements are reported in Table 2. HRV analyses in time domain demonstrated that SDRR, RMSSD, and pRR50 were significantly lower in OHTN and OHTN+T2DM groups when compared to obese subjects (Table 2). Regarding the frequency domain measurements, we found that LF band and LF/HF ratio were higher in the OHTN+T2DM and OHTN than subjects with obesity alone (p<0.05). HF was lower in the OHTN+T2DM and OHTN groups than the obese group (Table 2). Lastly, non-linear measures SD1, SD2 was also lower in the OHTN+T2DM group than in the obesity alone group, while SD2/SD1 ratio was higher in the OHTN+T2DM and OHTN when compared to obese (p<0.05). Taken together, the findings shown higher sympathetic power in the group with comorbidities.
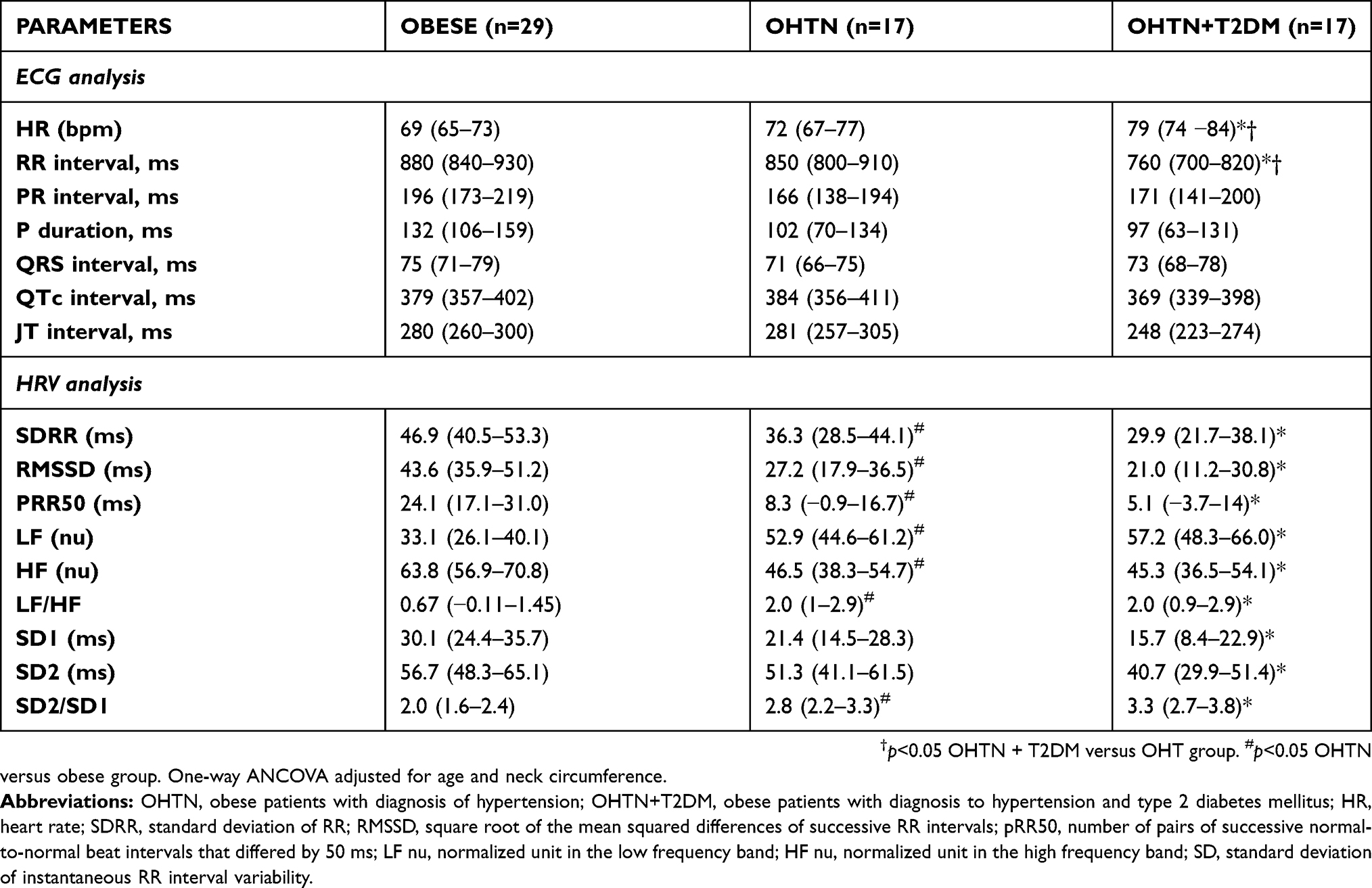 |
Table 2 Comparison of ECG analysis and heart rate variability measures between the three groups studied |
All ECG measures analyzed, such as PR, QRS, QTc, and ST intervals, and P duration, were similar among all three groups, with the exception of a higher HR and a shorter RR interval in the OHTN+T2DM group than in the other groups (Table 2).
We correlated clinical parameters, anthropometric measures, body composition, HR, BP and laboratory parameters with measurements of HRV in the time domain, frequency and nonlinear measurements (Table 3). Older patients exhibited increased SBP, DBP and lower values for SDRR and SD2 (Table 3). There was a positive correlation between BMI and NC with SBP, DBP, LF, LF/HF, and SD2/SD1. In the evaluation of the body composition, body fat percentage did not correlate with any other parameter of HRV (Table 3).
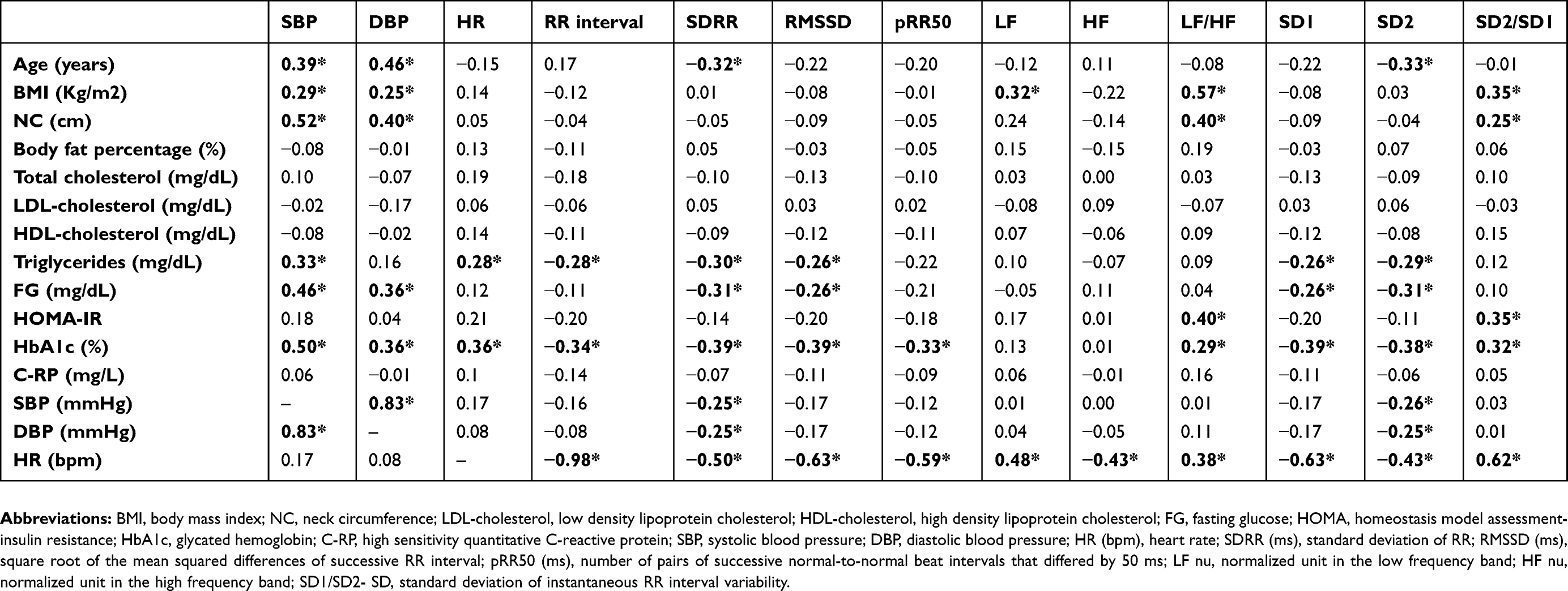 |
Table 3 Correlation coefficients between clinical, anthropometric, body composition and laboratory variables with the heart rate variability measures |
In addition to the obesity, HR, BP and metabolic profile also correlated with worse HRV (Table 3). HR correlated with all HRV measures evaluated, positively with measures expressing more sympathetic domain LF, LF/HF, and SD2/SD1, and negatively with measures expressing the parasympathetic domain RR, SDRR, RMSSD, pRR50, HF, SD1 and SD2 (Table 3).
In the evaluation of the metabolic profile, HbA1c was the one that had the greatest impact on HRV, correlating positively with HR, LF/HF, SD2/SD1 and negatively with RR, SDRR, RMSSD, pRR50, SD1 and SD2 (Table 3).
Discussion
This study evaluated the impact of HTN with or without T2DM on cardiovascular autonomic function in obese with a recommendation for BS. Our findings demonstrated that the presence of these comorbidities impairs cardiovascular autonomic function, with a decrease in parasympathetic activity and a predominance of the sympathetic component.
The weight gain enhanced the appearance of multiple pathophysiological disorders, such as ectopic fat deposition, inflammation, insulin resistance, and increased sympathetic nervous activity, which contributes to high cardiovascular morbidity and mortality.3
Previous studies verified that some HRV indices have good accuracy for diagnostic of CAD in some populations.29,30 It was demonstrated that subjects with morbid obesity exhibit impaired HRV when compared to non-obese individuals.17 Notably, the authors observed that the time domain components, such as SDNN, RMSSD, and pNN50 were reduced in obese subjects prior to BS, as well as, individuals with morbid obesity exhibited high LF/HF ratio. Although the findings suggested that the sympathovagal balance is impaired in individuals with morbid obesity,17 the authors did not assess the risk factors that could be involved with the worsening of HRV in these subjects.
Many risk factors for cardiovascular disease are associated with altered autonomic function. For example, decreased HRV is frequently observed in patients with T2DM or HTN.31–33 Of note, the presence of HTN in diabetic subjects appears to worsen the HRV. Recently Bassi and colleagues evaluated the influence of HTN on cardiac autonomic modulation and cardiopulmonary capacity in diabetic individuals.18 The authors found that hypertensive condition negatively affected the HRV in patients with T2DM, however, a higher BMI and BP levels in the group with T2DM and HTN could have interfered with the results. On the other hand, a recent study related that the existence of well-controlled hypertension in the diabetic subject without obesity did not alter cardiac dysautonomia.33 In the present study, we showed that HRV variables in the time, frequency and non-linear domain measurements were worse in the OHTN and OHTN+T2DM groups than in obese subjects.
It is known that diabetic individuals with longer disease duration and higher glycemic levels are subject to lower HRV.12 In our study, diabetic patients had less than five years of disease, but the glycemic levels were poorly controlled. Despite this, the presence of diabetes in obese individuals with HTN did not worsen HRV more than in OHTN individuals.
Early stages of glucose dysmetabolism already increase the risk of CAD. In present study, we found that OHTN and obese individuals had HbA1c levels compatible with prediabetes conditions.34 This may have been one of the reasons why the presence of diabetes in hypertensive patients did not have an impact on worsed HRV.
A recent study demonstrated that approximately 24% of subjects with glucose homeostasis dysfunction (HbA1c >6.0%) exhibit increased risk of autonomic dysfunction and CAD.35 In our study, the glycemic parameters were positively correlated with SBP, DBP LF/HF, and SD2/SD1. This suggests that elevated glycemic levels are associated with the increased sympathetic activity, low HRV and augmented cardiovascular risk in morbidly obese.
HRV may be influenced by gender, age, and physical activity. Older individuals and women have lower HRV, while more trained people have higher HRV.15 Among the obese subjects studied, we found that patients from the OHTN and OHTN+T2DM groups were older (43.7±1.8 and 44.4±2.1, respectively) and that age was positively correlated with SBP and DBP and negatively correlated with measures of SDRR and SD2. A previous study demonstrated that subjects with age greater than 53 years had a sensitivity of 76% and specificity of 61% for the presence of CAD.35 Due to the difference in age among groups, we corrected all the result by the age of each subject.
Another cause associated with the risk of CAD in the early stages of glucose dysmetabolism is a QTc interval greater than 423ms.35 This interval is associated with arrhythmias and increased risk for cardiovascular mortality.36 In our study, the QTc interval was similar between the groups, not exceeding more than 400 ms.
Regarding the impact of the increased BMI among obese individuals on HRV,37 it was demonstrated that higher BMI effectively depresses the HF component, a marker of parasympathetic activity. Some data from the literature show that other measures of adiposity, such as body fat percentage, visceral adipose tissue and waist circumference correlated with worse HRV, whereas there was no significant association with BMI.38,39 In our study, body fat percentage was not associated with any of the HRV parameters, but conversely, BMI positively correlated with LF, LF/HF and SD2/SD1. Indicating that excessive body weight impair autonomic function.
It has been described that a NC greater than 38cm has been associated with obstructive sleep apnea syndrome, metabolic syndrome and increase in muscle sympathetic nerve activity.40,41 In our study, a positive correlation was found between NC and SBP, DBP, LF/HF and SD2/SD1. These associations show the importance of the NC measurement for evaluate the possibility of cardiovascular complications in obese subject with or without comorbities.
Conclusion
HTN and T2DM impair the cardiac autonomic function in obese individuals with a recommendation for BS. The presence of T2DM did not exacerbate the hypertension-related impairment of autonomic function.
Abbreviations
ACEI, angiotensin-converting enzyme I inhibitors; ARBII, angiotensin II receptor antagonists; ASM, appendicular skeletal muscle mass; BMI, body mass index; BP, blood pressure; BS, bariatric surgery; CAD, cardiac autonomic dysfunction; C-RP, high sensitivity quantitative C-reactive protein; DBP, diastolic blood pressure; ECG, electrocardiogram; FFMI, fat-free mass index; HbA1c, glycated hemoglobin; HDL-cholesterol, high density lipoprotein cholesterol; HF, high frequency; HOMA, homeostasis model assessment-insulin resistance; HR, heart rate; HRV, heart rate variability; HTN, hypertension; LDL-cholesterol, low density lipoprotein cholesterol; LF, low frequency; MMI, muscle mass index; NC, neck circumference; OHTN, obese individuals with diagnosis of HTN; OHTN+T2DM, obese individuals with diagnosis of hypertension and type 2 diabetes mellitus; pRR50, number of pairs of successive normal-to-normal beat intervals that differed by 50 ms; RMSSD, square root of the mean squared differences of successive RR interval; RR, RR interval; SBP, systolic blood pressure; SD, standard deviation; SDRR, standard deviation of RR; T2DM, type 2 diabetes mellitus.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work
Disclosure
The authors report no conflicts of interest in this work.
References
1. Apovian CM. Obesity: definition, comorbidities, causes, and burden. Am J Manag Care. 2016;22(7 Suppl):s176–s185.
2. Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. Jama. 2013;309(1):71–82. doi:10.1001/jama.2012.113905
3. Adachi T, Sert-Kuniyoshi FH, Calvin AD, et al. Effect of weight gain on cardiac autonomic control during wakefulness and sleep. Hypertension. 2011;57(4):723–730. doi:10.1161/HYPERTENSIONAHA.110.163147
4. Vinik AI, Erbas T, Casellini CM. Diabetic cardiac autonomic neuropathy, inflammation and cardiovascular disease. J Diabetes Investig. 2013;4(1):4–18. doi:10.1111/jdi.12042
5. Wheeler SG, Ahroni JH, Boyko EJ. Prospective study of autonomic neuropathy as a predictor of mortality in patients with diabetes. Diabetes Res Clin Pract. 2002;58(2):131–138.
6. Kim JA, Park YG, Cho KH, et al. Heart rate variability and obesity indices: emphasis on the response to noise and standing. J Am Board Family Pract. 2005;18(2):97–103.
7. Vinik AI, Casellini C, Parson HK, Colberg SR, Nevoret ML. Cardiac autonomic neuropathy in diabetes: a predictor of cardiometabolic events. Front Neurosci. 2018;12:591. doi:10.3389/fnins.2018.00044
8. Rathmann W, Ziegler D, Jahnke M, Haastert B, Gries FA. Mortality in diabetic patients with cardiovascular autonomic neuropathy. Diabetic Med. 1993;10(9):820–824.
9. Astrup AS, Tarnow L, Rossing P, Hansen BV, Hilsted J, Parving HH. Cardiac autonomic neuropathy predicts cardiovascular morbidity and mortality in type 1 diabetic patients with diabetic nephropathy. Diabetes Care. 2006;29(2):334–339. doi:10.2337/diacare.29.02.06.dc05-1242
10. Gandolfini MP, Coupaye M, Bouaziz E, et al. Cardiovascular changes after gastric bypass surgery: involvement of increased secretions of glucagon-like peptide-1 and brain natriuretic peptide. Obes Surg. 2015;25(10):1933–1939. doi:10.1007/s11695-015-1643-5
11. Nault I, Nadreau E, Paquet C, et al. Impact of bariatric surgery–induced weight loss on heart rate variability. Metabolism. 2007;56(10):1425–1430. doi:10.1016/j.metabol.2007.06.006
12. Wu JM, Yu HJ, Lai HS, Yang PJ, Lin MT, Lai F. Improvement of heart rate variability after decreased insulin resistance after sleeve gastrectomy for morbidly obesity patients. Surg Obes Relat Dis. 2015;11(3):557–563. doi:10.1016/j.soard.2014.09.011
13. Caravatto PP, Petry T, Cohen R. Changing guidelines for metabolic surgery: now it’s the time. Curr Atheroscler Rep. 2016;18(8):47. doi:10.1007/s11883-016-0600-7
14. Auclair A, Biertho L, Marceau S, et al. Bariatric surgery-induced resolution of hypertension and obstructive sleep apnea: impact of modulation of body fat, ectopic fat, autonomic nervous activity, inflammatory and adipokine profiles. Obes Surg. 2017;27(12):3156–3164. doi:10.1007/s11695-017-2737-z
15. Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. 2017;5:258. doi:10.3389/fpubh.2017.00081
16. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task force of the European Society of Cardiology and the North American society of pacing and electrophysiology. Circulation. 1996;93(5):1043–1065.
17. Sant Anna Junior M, Carneiro JR, Carvalhal RF, et al. Cardiovascular autonomic dysfunction in patients with morbid obesity. Arq Bras Cardiol. 2015;105(6):580–587. doi:10.5935/abc.20150125
18. Bassi D, Cabiddu R, Mendes RG, et al. Effects of coexistence hypertension and Type II diabetes on heart rate variability and cardiorespiratory fitness. Arq Bras Cardiol. 2018;111(1):64–72. doi:10.5935/abc.20180105
19. Ben-Noun L, Sohar E, Laor A. Neck circumference as a simple screening measure for identifying overweight and obese patients. Obes Res. 2001;9(8):470–477. doi:10.1038/oby.2001.61
20. Jang IY, Jung HW, Lee CK, Yu SS, Lee YS, Lee E. Comparisons of predictive values of sarcopenia with different muscle mass indices in Korean rural older adults: a longitudinal analysis of the Aging Study of PyeongChang Rural Area. Clin Interv Aging. 2018;13:91–99. doi:10.2147/CIA.S155619
21. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18(6):499–502.
22. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419.
23. Sullivan K, Raskin P. Evaluation of a new automated affinity-chromatographic method for the measurement of glycated hemoglobin. Diabetes Res Clin Pract. 1991;13(1–2):103–106.
24. Hamwi A, Vukovich T, Wagner O, et al. Evaluation of turbidimetric high-sensitivity C-reactive protein assays for cardiovascular risk estimation. Clin Chem. 2001;47(11):2044–2046.
25. Ernst G. Hidden signals-the history and methods of heart rate variability. Front Public Health. 2017;5:265. doi:10.3389/fpubh.2017.00081
26. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC practice guidelines for the management of arterial hypertension. Blood Press. 2014;23(1):3–16. doi:10.3109/08037051.2014.868629
27. Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45(1):255–268.
28. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135–160.
29. Silva A, Christofaro DGD, Bernardo AFB, Vanderlei FM, Vanderlei LCM. Sensitivity, specificity and predictive value of heart rate variability indices in type 1 diabetes mellitus. Arq Bras Cardiol. 2017;108(3):255–262. doi:10.5935/abc.20170024
30. Khandoker AH, Jelinek HF, Palaniswami M. Identifying diabetic patients with cardiac autonomic neuropathy by heart rate complexity analysis. Biomed Eng Online. 2009;8:3. doi:10.1186/1475-925X-8-3
31. Takahashi N, Nakagawa M, Saikawa T, et al. Effect of essential hypertension on cardiac autonomic function in type 2 diabetic patients. J Am Coll Cardiol. 2001;38(1):232–237. doi:10.1016/s0735-1097(01)01363-8
32. Istenes I, Korei AE, Putz Z, et al. Heart rate variability is severely impaired among type 2 diabetic patients with hypertension. Diabetes Metab Res Rev. 2014;30(4):305–312.
33. Solanki JD, Basida SD, Mehta HB, Panjwani SJ, Gadhavi BP. Comparative study of cardiac autonomic status by heart rate variability between under-treatment normotensive and hypertensive known type 2 diabetics. Indian Heart J. 2017;69(1):52–56. doi:10.1016/j.ihj.2016.07.013
34. American Diabetes Association.2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S13–S27. doi:10.2337/dc18-0733
35. Dimova R, Tankova T, Chakarova N, Grozeva G, Dakovska L. Cardio-metabolic profile of subjects with early stages of glucose intolerance and cardiovascular autonomic dysfunction. Diabetes Res Clin Pract. 2017;126:115–121. doi:10.1016/j.diabres.2017.02.004
36. Cox AJ, Azeem A, Yeboah J, et al. Heart rate-corrected QT interval is an independent predictor of all-cause and cardiovascular mortality in individuals with type 2 diabetes: the Diabetes Heart Study. Diabetes Care. 2014;37(5):1454–1461. doi:10.2337/dc13-1257
37. Laederach-Hofmann K, Mussgay L, Ruddel H. Autonomic cardiovascular regulation in obesity. J Endocrinol. 2000;164(1):59–66. doi:10.1677/joe.0.1640059
38. Poliakova N, Despres JP, Bergeron J, Almeras N, Tremblay A, Poirier P. Influence of obesity indices, metabolic parameters and age on cardiac autonomic function in abdominally obese men. Metabolism. 2012;61(9):1270–1279. doi:10.1016/j.metabol.2012.02.006
39. Yadav RL, Yadav PK, Yadav LK, Agrawal K, Sah SK, Islam MN. Association between obesity and heart rate variability indices: an intuition toward cardiac autonomic alteration - a risk of CVD. Diabetes Metab Syndrome Obes. 2017;10:57–64. doi:10.2147/DMSO.S123935
40. Straznicky NE, Grima MT, Sari CI, et al. Neck circumference is associated with muscle sympathetic nerve activity in overweight and obese men but not women. Front Physiol. 2017;8:203. doi:10.3389/fphys.2017.00203
41. Onat A, Hergenc G, Yuksel H, et al. Neck circumference as a measure of central obesity: associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference. Clin Nutr. 2009;28(1):46–51. doi:10.1016/j.clnu.2008.10.006
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.