")
Back to Journals » Vascular Health and Risk Management » Volume 13
Impact of around-the-clock in-house cardiology fellow coverage on door-to-balloon time in an academic medical center
Authors Kohan LC, Nagarajan V, Millard MA, Loguidice MJ, Fauber NM, Keeley EC
Received 14 January 2017
Accepted for publication 21 March 2017
Published 18 April 2017 Volume 2017:13 Pages 139—142
DOI https://doi.org/10.2147/VHRM.S132405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Luke C Kohan,1,* Vijaiganesh Nagarajan,1,* Michael A Millard,2 Michael J Loguidice,2 Nancy M Fauber,1 Ellen C Keeley1
1Division of Cardiology, 2Department of Medicine, University of Virginia, Charlottesville, VA, USA
* These authors contributed equally to this work
Objectives: To assess if a change in our cardiology fellowship program impacted our ST elevation myocardial infarction (STEMI) program.
Background: Fellows covering the cardiac care unit were spending excessive hours in the hospital while on call, resulting in increased duty hours violations. A night float fellow system was started on July 1, 2012, allowing the cardiac care unit fellow to sign out to a night float fellow at 5:30 pm. The night float fellow remained in-house until the morning.
Methods: We performed a retrospective study assessing symptom onset to arrival, arterial access to first device, and door-to-balloon (D2B) times, in consecutive STEMI patients presenting to our emergency department before and after initiation of the night float fellow system.
Results: From 2009 to 2013, 208 STEMI patients presented to our emergency department and underwent primary percutaneous coronary intervention. There was no difference in symptom onset to arrival (150±102 minutes vs 154±122 minutes, p=0.758), arterial access to first device (12±8 minutes vs 11±7 minutes, p=0.230), or D2B times (50±32 minutes vs 52±34 minutes, p=0.681) during regular working hours. However, there was a significant decrease in D2B times seen during off-hours (72±33 minutes vs 49±15 minutes, p=0.007). There was no difference in in-hospital mortality (11% vs 8%, p=0.484) or need for intra-aortic balloon pump placement (7% vs 8%, p=0.793).
Conclusion: In academic medical centers, in-house cardiology fellow coverage during off-hours may expedite care of STEMI patients.
Keywords: door-to-balloon time, 24/7 in-house call, cardiology fellow
Introduction
Door-to-balloon (D2B) or first device time for patients with ST elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) is associated with clinical outcomes.1–5 Because of this, D2B time has become a core quality measure publicly reported by the Centers for Medicare and Medicaid Services and the Joint Commission on Accreditation of Healthcare Organizations.6–8 While the American College of Cardiology/American Heart Association recommends D2B times of <90 minutes in PCI-capable hospitals,9 investigators have shown that every minute of delay is associated with increased short- and long-term mortality, and so promote an “as soon as possible approach” even in STEMI programs that routinely provide primary PCI within 90 minutes.4,5 Our STEMI program already incorporates many of the processes shown to decrease D2B times, including a team-based approach, prehospital activation of the STEMI alert process, emergency physician activation of the on-call team, emergency department (ED) bypass to the cardiac catheterization laboratory, use of a single page system to activate the cardiac catheterization laboratory on-call team, and real-time feedback to the ED staff.10–12 Starting July 1, 2012, the cardiology fellowship program at our institution underwent a significant change because fellows covering the coronary care unit (CCU) were spending an excessive amount of time in the hospital at night, which led to duty hours violations and fatigue. In order to improve this situation, the call schedule was changed such that a separate fellow covers the CCU only during the night (night float fellow). The purpose of this study was to assess what impact, if any, this change had on our STEMI program and specifically our D2B times.
Methods
Following approval from the University of Virginia Institutional Review Board (IRB), we performed a retrospective chart review to identify consecutive STEMI patients who presented to the University of Virginia cardiac catheterization laboratory and underwent primary PCI from 2009 to 2013. Due to the design of the study, a waiver of consent was approved by the IRB. Data were collected from dedicated data fields within the University of Virginia cardiac catheterization database, which is part of the National Cardiovascular Data Registry (NCDR®, American College of Cardiology, Washington, DC, USA), the acute MI treatment registry of the American College of Cardiology. Data confidentiality was maintained at all times. The University of Virginia performs primary PCI 24 hours a day, 7 days a week. Off-hour (5:30 pm to 7:30 am), weekend, and holiday emergency procedures are performed by the on-call team, which consists of 2 cardiac catheterization laboratory nurses, a cardiac radiology technician, an interventional cardiology fellow, and an attending interventional cardiologist. Call is equally shared among 6 interventional cardiologists. A single call to activate the on-call team is used, and the alert is routinely activated by the ED staff on the basis of electrocardiograms performed in the field or in the ED. All members of the on-call team are expected to arrive within 30 minutes of STEMI alert activation.
After the STEMI alert is activated by the ED staff, a cardiology fellow covering the CCU is one of the first members of the team to evaluate the STEMI patient in the ED as part of the STEMI activation protocol. This cardiology fellow explains the PCI procedure to the patient, obtains consent, assesses access site choices, identifies important comorbidities such as bleeding diatheses, and helps transport the patient to the cardiac catheterization laboratory when the team is ready to receive the patient. Moreover, they remain in constant contact with the cardiac catheterization laboratory staff to provide updates on the hemodynamic stability of the patient prior to transfer from the ED to the cardiac catheterization laboratory, and also remain with the patient in the cardiac catheterization laboratory during the emergency procedure. Starting July 1, 2012, the cardiology fellowship program at our institution underwent a major change in order to decrease duty hours violations. A night float fellow, separate from the CCU fellow, starts in-hospital call at 5:30 pm and remains in the hospital until morning, when the CCU fellow returns. This change resulted in a cardiology fellow physically present in-house 24 hours a day, 7 days a week. During this time, no other systematic changes were made to our STEMI program that would have impacted D2B times.
We collected angiographic data and detailed time information data including time of arterial access and time of the first device from the cardiac catheterization laboratory database, which is part of the NCDR®, and clinical information from the electronic medical record. We only included patients who presented to our ED (excluding patients transferred from outside hospitals). Categorical variables were compared using the χ2 test, and values are reported as percentages. Continuous variables were compared using the Mann–Whitney U test, and values are reported as mean with standard deviation. A two-sided P-value less than 0.05 was considered statistically significant. All analyses were performed using GraphPad Prism (Version 7.0, GraphPad Software, Inc., La Jolla, CA, USA).
Results
From June 1, 2009, to June 30, 2013, 377 patients presented to our hospital with a STEMI. A total of 169 patients were excluded from analysis due to being identified as having a NCDR®-defined nonsystem delay, incomplete time data, not undergoing coronary angiography, or a hospital-to-hospital transfer. As part of the NCDR® registry, median D2B times from 2009 to July 2012 were calculated and ranged from 51 to 64 minutes (51–64 minutes in 2009; 51–62 minutes in 2010; and 51–59 minutes in 2011). A total of 208 patients were included: 118 before and 90 after the cardiology fellowship program change in July 2012 (Table 1). There were no significant differences between the two groups with respect to gender and cardiac risk factors. There was no difference in symptom onset to arrival times (150±102 minutes vs 154±122 minutes, p=0.758), arterial access to first device times (12±8 minutes vs 11±7 minutes, p=0.230), or D2B times during regular working hours (50±32 minutes vs 52±34 minutes, p=0.681). However, there was a significant decrease in D2B times after the fellowship program change in patients presenting during off-hours (72±33 minutes vs 49±15 minutes, p=0.007). There was no difference in in-hospital mortality (11% vs 8%, p=0.484) or need for intra-aortic balloon pump placement (7% vs 8%, p=0.793) before and after the change.
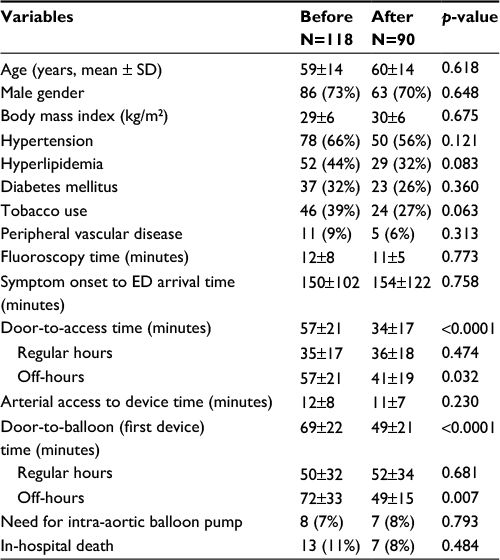 | Table 1 Characteristics before and after night float cardiology fellow coverage Notes: Data are expressed as number (percentage), and as mean ± SD. Abbreviations: ED, emergency department; SD, standard deviation. |
Discussion
D2B time is a core quality measure publicly reported by the Centers for Medicare and Medicaid Services and the Joint Commission on Accreditation of Healthcare Organizations.6–8 Our hospital already implements many of the systems and processes shown to reduce D2B.12,13 Others have shown that having an attending interventional cardiologist on-site 24/7 is associated with shorter D2B times.10,13 This option, however, may be too costly or impractical to sustain for most hospitals with STEMI programs. A major change in the call schedule for our cardiology fellows on July 1, 2012, resulted in a cardiology fellow being on-site 24/7. We were interested in whether this simulated having an attending interventional cardiologist on-site 24/7. We found that our D2B times off-hours (but not during regular working hours) were significantly shorter (by ~20 minutes) after our cardiology fellowship program started the night float schedule. Bradley et al10 report data from a web-based survey study focused on STEMI care and found that among the strategies that were associated with lower D2B times, the presence of an attending interventional cardiologist always at the hospital decreased D2B times by a mean of 14.6 minutes. Nguyen et al13 studied the impact of a newly created 24/7 in-house interventional team, including the interventional cardiologist, and found that there was a 57% reduction in D2B time.13 In addition, they also found that differences between regular working hours and off-hours D2B times were completely eliminated.13 The results of these studies underscore the potential time-saving effect of having the entire on-call team or part of the on-call team physically present in the hospital during off-hours.
How could the physical presence of a cardiology fellow who does not usually participate in the procedure itself, impact D2B times during off-hours? We contend that they are an integral part of the STEMI team by doing the following: having the patient ready and consented as the on-call team is traveling to the hospital, fast-tracking transport from the ED to the cardiac catheterization laboratory, providing continual updates about the patient’s hemodynamic status allowing us to better prepare the laboratory for what equipment will be needed, and remaining in the cardiac catheterization laboratory during the procedure and available to help in a variety of ways, especially during off-hours when there is limited manpower.
There are several limitations to this study. First, this is a single-center retrospective study; therefore, we can only say that the presence of the night float fellow was associated with shorter D2B times, but cannot prove causation. Second, while no other quality improvement change to our STEMI program was made during the time period, it is possible although unlikely that unknown factors could have impacted our D2B times during off-hours. Third, our results only apply to hospitals with cardiology fellowship programs. Fourth, during the time period of our study, 94% of the cases were performed via femoral artery access. More recently, however, our preferred access is the radial artery for all patients undergoing angiography, including STEMI patients. It is not known how this change in practice has impacted our D2B times. Fifth, although we did not see any difference in the need for intra-aortic balloon pump or death rates before and after the fellowship program change, the sample size is too small to assess impact on clinical outcomes. Sixth, in addition to the known confounders that impact D2B times, there may be unknown confounders that we did not control for, leading to potential bias. Finally, our study was underpowered to compare clinical outcomes, and so our findings, including the effect on D2B times shortening, should be considered hypothesis-generating only.
Conclusion
In-house cardiology fellow coverage may expedite care of STEMI patients, particularly during off-hours. Additional studies with larger sample sizes are needed to test this hypothesis.
Acknowledgment
This work was supported by the American Heart Association (13IRG14560018 and 16IRG27180006 to ECK).
Disclosure
The authors report no conflicts of interest in this work.
References
Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283(22):2941–2947. | ||
Maeng M, Nielson PH, Busk M, et al. Time to treatment and three-year mortality after percutaneous intervention for ST-segment elevation myocardial infarction—a Danish trial in acute myocardial infarction-2 (DANAMI-2) substudy. Am J Cardiol. 2010;105(11):1528–1534. | ||
McNamara RL, Wang Y, Herrin J, et al. Effect of door-to-balloon time on mortality in patients with ST-elevation myocardial infarction. J Am Coll Cardiol. 2006;47(11):2180–2186. | ||
Rathore SS, Curtis JP, Nallamothu BK, et al. Association of door-to-balloon time and mortality in patients ≥65 years with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Am J Cardiol. 2009;104(9):1198–1203. | ||
Rathore SS, Curtis JP, Chen J, et al. Association of door-to-balloon time and mortality in patients admitted to hospital with ST elevation myocardial infarction: national cohort study. BMJ. 2009;338:b1807. | ||
McCabe JM, Kennedy KF, Eisenhauer AC, et al. Reporting trends and outcomes in ST-segment elevation myocardial infarction national hospital quality assessment programs. Circulation. 2014;129(3):194–202. | ||
Krumholtz HM, Anderson JL, Brooks NH, et al; American College of Cardiology; American Heart Association Task Force on Performance Measures; Writing Committee to Develop Performance Measures on ST-Elevation and Non ST–Elevation Myocardial Infarction. ACC/AHA clinical performance measures for adults with ST-elevation and non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures on ST-Elevation and Non ST-Elevation Myocardial Infarction). J Am Coll Cardiol. 2006;47(1):236–265. | ||
Duffy PL, Naidu SS, Kurian KC, Marshall JJ. Rationale for ST-elevation myocardial infarction call compensation by healthcare systems. Catheter Cardiovasc Interv. 2013;81(6):909–911. | ||
O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):529–555. | ||
Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med. 2006;355(22):2308–2320. | ||
Peterson MC, Syndergaard T, Bowler J, Doxey R. A systematic review of factors predicting door to balloon time in ST segment elevation myocardial infarction treated with percutaneous intervention. Int J Cardiol. 2012;157(1):8–23. | ||
Camp-Rogers T, Kurz MC, Brady WJ. Hospital-based strategies contributing to percutaneous coronary intervention time reduction in the patient with ST-segment elevation myocardial infarction: a review of the “system-of-care” approach. Am J Emerg Med. 2012;30(3):491–498. | ||
Nguyen B, Fennessy M, Leya F, et al. Comparison of primary percutaneous coronary intervention in patients with ST elevation myocardial infarction during and prior to availability of an in-house STEMI system: Early experience and intermediate outcomes of the HARRT program for achieving routine D2B times <60 minutes. Catheter Cardiovasc Interv. 2015;86(2):186–196. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.