")
Back to Journals » Cancer Management and Research » Volume 11
Impact of antiviral therapy with nucleos(t)ide analog on survival of patients with HBV-related small hepatocellular carcinomas
Authors Wei Y , Yi Y, Tao C, Ye W , Zhao W
Received 16 January 2019
Accepted for publication 5 August 2019
Published 17 September 2019 Volume 2019:11 Pages 8475—8486
DOI https://doi.org/10.2147/CMAR.S201744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Yanyan Wei,1,2,* Yongxiang Yi,3,* Chen Tao,1,3 Wei Ye,1,3 Wei Zhao1,3
1Department of Infectious Diseases, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 2Department of Infectious Diseases, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Department of Hepatobiliary Surgeon, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Ye; Wei Zhao
Department of Infectious Diseases, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, No. 1-1 Zhongfu Road, Nanjing, Jiangsu, People’s Republic of China
Email [email protected]; [email protected]
Background: Hepatocellular carcinoma (HCC) is the second leading causes of cancer-related death. HCC is usually based on chronic liver disease, mainly including chronic hepatitis C virus infection or chronic hepatitis B virus (HBV) infection.
Objective: The objective of the study was to evaluate the impact of the nucleos(t)ide analog (NA) use on the prognosis of patients with HBV-related small hepatocellular carcinomas (HBV-SHCC).
Methods: In this retrospective study, there were 134 patients who had been treated with long-term NA before SHCC diagnosis as NA-experienced group, 43 patients received NA-naïve treatment after SHCC diagnosis as NA-naïve group, and 15 patients who did not receive NA treatment as untreated group. Among these patients, some patients underwent surgical resection and others with local recurrence were treated with transarterial chemoembolization (TACE), TACE-percutaneous microwave coagulation therapy or TACE alone. The Kaplan–Meier and Cox-proportional hazard model were used to calculate the survival analysis.
Results: The data showed that 1-year, 3-year, 5-year overall survival rate of HBV-SHCC patients in NA-experienced group were 90.27%, 90.69%, 65%, NA-naïve group were 70.81%, 73.95%, 47.39%, and untreated group were 54.96%, 40.44%, 47.39%, respectively (Log-rank, P=0.031). The median survival time of HBV-SHCC patients treated with adefovir dipivoxil (ADV) or LAM+ADV has the longest survival time. Patients who have received rescue treatment after viral breakthrough or gotten maintained viral response had longer survival times than those who have not received rescue treatment after viral breakthrough or non-response. Compared with timely rescue treatment, viral breakthrough (hazard ratio=3.624, 95% CI, 1.035–12.687, P=0.044) was an independent risk factor for HBV-SHCC patients with Cox-proportional hazard model. For these patients conforming to NA-treatment indications, commencement of NA treatment should be given even after HBV-SHCC diagnosis. Moreover, HBV-SHCC patients who were suffering from virus break through should be treated timely rescue therapy even if their liver function was normal.
Conclusion: SHCC patients treated with low drug resistance barrier drugs may not change the treatment regimen if they have gotten virological response.
Keywords: chronic hepatitis B, hepatocellular carcinoma, liver cirrhosis, nucleos(t)ide analog, virus breakthrough, timely rescue therapy
Introduction
Liver cancer is common and the second leading causes of cancer-related death. Moreover, the majority of hepatocellular carcinoma (HCC) cases occur in Asia and Africa, especially in China, which accounts for more than 50% of HCC cases worldwide.1,2 HCC is the major histological subtype among all types of primary liver cancers.3 Hepatotropic virus including hepatitis B virus (HBV) and hepatitis C virus (HCV) are major causes of HCC.4 Besides, the mechanism of HBV promoting HCC progression was the induction of liver fibrogenesis, cirrhosis, genetic and epigenetic alterations, and the expression of viral-coded proteins.5
The definition of small hepatocellular carcinomas (SHCC) consists of a single HCC nodule <5 cm or up to 3 nodules and a maximum diameter of each nodule <3 cm, and single HCC nodule <3 cm is generally considered to early stage HCC in the Barcelona Clinic Liver Cancer (BCLC) criteria.6 Up to date, intervention treatments for SHCC patients mainly include surgical resection, liver transplantation, local mini-invasive therapies including transarterial chemoembolization (TACE), percutaneous microwave coagulation therapy (PMCT), percutaneous ethanol injection, etc.7–9 A series of studies previously have reported that the local mini-invasive therapies (monotherapy or combined therapy) were safe and effective for HBV-SHCC patients in the short term.10–12 However, little attention has been focused on the medical treatment of HBV-SHCC patients, such as nucleos(t)ide analog (NA) treatment combined with TACE treatment.
Antiviral treatment for HBV patients can reduce but not completely eliminate the occurrence of HCC.1 Therefore, patients with chronic hepatitis B were still at high risk of HCC even if receiving NA treatment. Additionally, HBV reactivation could be present in patients who received aforementioned intervention treatments, even caused liver function failure.13 Therefore, the inhibition of viral replication might be a reasonable target for SHCC treatment to prolong the survival time of SHCC patients. Currently, antiviral therapy mainly includes interferon and NA. NA includes lamivudine (LAM), telbivudine (TBV), adefovir dipivoxil (ADV), entecavir (ETV) and tenofovir (TDF). Previous researches have proven that NA was an appropriate option for all HCC patients with viral replication. Jiang et al and Huang et al reported that prophylactic NA treatment should be routinely performed as a key adjuvant therapy undergoing surgical resection for HBV-HCC patients.14,15 Furthermore, Huang et al reported that antiviral therapy with TBV can significantly decrease the preoperative reactivation of viral replication in patients with HBV-HCC undergoing surgical resection.16 Wu et al reported that NA use was linked to a lower risk of HCC recurrence among patients with HBV-related HCC after liver resection in 2012.17 Then, Wu and colleagues reported that NA use was also associated with mortality of HBV-related HCC patients following TACE in 2013.18 However, to our best knowledge, there were scarce of reports of the impact of antiviral therapy on the survival of HBV-SHCC patients, especially for patients suffering from viral breakthrough. Therefore, data were collected and analyzed to assess the effect of NA treatment and viral load fluctuation on the survival of HBV-SHCC patients.
In this study, our study attempted to indicate whether NA treatment could improve the prognosis of HBV-SHCC patients. Then, the appropriate treatment protocols for HBV-SHCC patients were found and selected. Furthermore, the importance of surveillance viral response was emphasized during antiviral treatment. The timely rescue treatment was critical to improve prognosis once viral breakthrough occurring irrespective of liver function status.
Methods
Ethics
This investigation conforms to the principles outlined in the Declaration of Helsinki. This study was approved by the Ethics Committee of the Second Hospital of Nanjing, Nanjing, China. All patients provided written informed consent prior to participation in the study protocol.
Collection of data
We checked all SHCC patients admitted and treated in the second hospital of Nanjing from August 2006 to August 2015. The inclusion criteria for the study population were as follows: a) HBsAg positive; b) patients aged between 13 and 81 years; c) single SHCC (≤3 cm) or multifocal HCC <3.0 cm in greatest dimension; d) diabetes mellitus and hypertension, if present, were controlled with medications; and e) no multiple organ failure and no severe underlying diseases; f) treated with TACE. Patients were excluded from the study if they a) follow-up <12 months; b) HBsAg negative or HCV antibody (HCV-Ab) positive; c) received other antiviral therapy (ART) treatments or local mini-invasive therapies in other hospitals; d) were missing data; e) were not tracked adequately; f) withdraw drug; g) irregularly taken medication; h) received systemic chemotherapy; i) received sorafenib; or j) had another type of malignant tumor.
SHCC was diagnosed according to the Barcelona criteria for the study of Liver Disease guidelines. A total of 192 patients with single SHCC (≤3 cm) or multifocal
HCC <3.0 cm in greatest dimension were included in this study. The inclusion criteria and excluded criteria of HBV-SHCC are summarized in Figure 1. Newly-diagnosed SHCC patients who received the treatment (all follow-ups were completed in August 2016) were included. Informed consent of therapeutic protocols and use of clinicopathological data for this study was obtained from all patients. We collected clinical, laboratory data from each patient at the time of SHCC diagnosis including age, gender, etiology of liver disease and other chronic diseases, Child-Pugh grade and BCLC stage, AFP levels, antiviral therapeutic process. From the radiological outcomes, tumor characteristics were collected including tumor size, tumor numbers, intrahepatic metastases and vascular invasion.
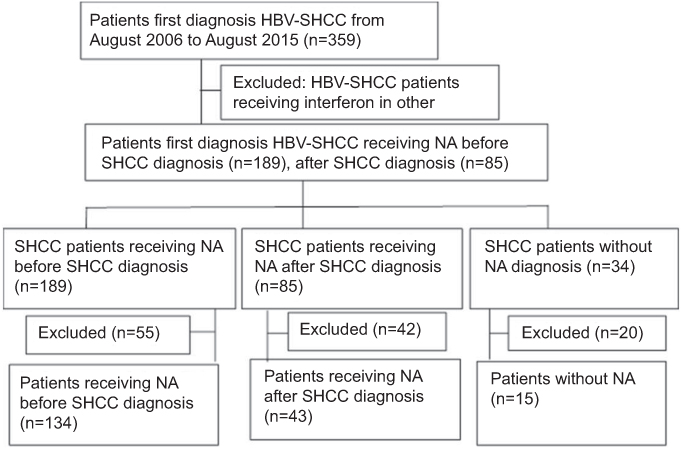 |
Figure 1 Flow diagram shows exclusion criteria. Abbreviations: HBV-SHCC, hepatitis B virus-small hepatocellular carcinoma; NA, nucelos(t)ide analog. |
The main endpoint was survival time, which was defined as the duration from the time point of primary treatment for HBV-SHCC to death, otherwise to August 2016. The second endpoint was outcomes including survival and death during follow-up.
Treatments and follow-up
After antiviral therapy, patients were monitored every 1–3 months. HBV-SHCC patients were assessed for treatment response by combining HBV viral load with liver function. For patients who experienced viral breakthrough, subsequent rescue treatment was administered by physicians after obtaining informed consent.
Statistical analyses
Continuous data were presented as mean ± SD for normal distribution, M (Q1–Q3) for skewed distribution. They were compared by Kruskal–Wallis test or one-way ANOVA adjusted for multiple comparisons, as appropriate. For categorical variables, Chi-square test and Fisher exact test were performed. The cumulative survival rates were generated using the Kaplan–Meier method. Cox-regression analysis was performed to screen the influence factor of outcomes. All statistical tests were 2-sided, and P<0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS 22.0 software (SPSS Inc., Chicago, IL, USA).
Results
Patient population
In total, 359 patients with HBV-SHCC were initially admitted and treated in the Second Hospital of Nanjing from August 2006 to August 2015. According to the included and excluded criteria, 192 patients treated with TACE were enrolled, including 148 male and 44 female (mean age, 55.24±10.69 years; range, 13–82 years). As showed in Table 1, the majority of patients had cirrhosis (89.1%). A total of 147 patients (76.6%) had well-preserved liver function (Child-Pugh A), whereas 43 patients (22.4%) and 2 patients (1.0%) had Child-Pugh B and C functional status, respectively. Among the 192 patients, most patients (88.5%) had early stage of the tumor (BCLC stage A), while 9 patients (4.7%) and 13 patients (6.8%) had BCLC stage B and C, respectively. The mean number of tumors was 1.29±0.613 (range, 1–3), and the mean tumor length and tumor width were 2.14±0.55 cm (range, 0.5–3 cm) and1.6±0.56 cm (range, 0.5–2.5 cm), respectively. Of these patients, 26 (13.5%) had intrahepatic metastasis (IM), and 13 (7.3%) had portal vein tumor thrombus (PVTT).
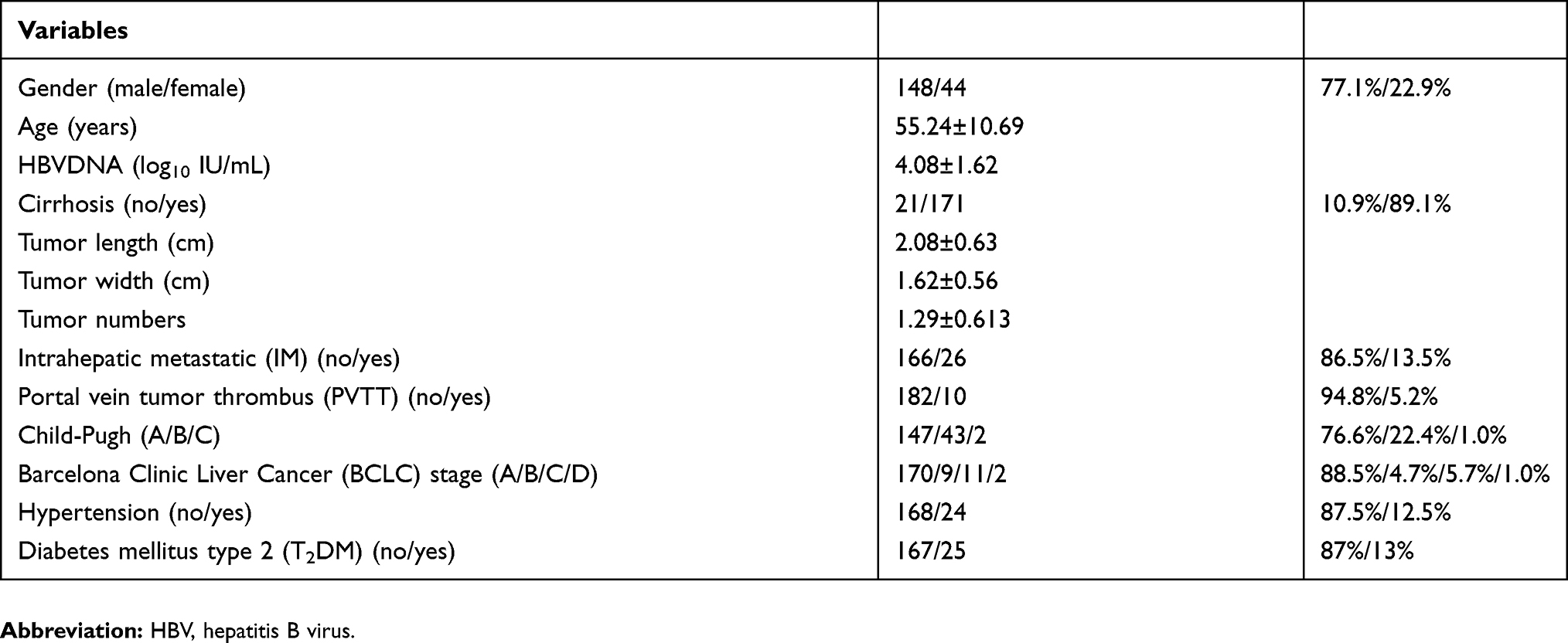 |
Table 1 Demographic data and tumor characteristics |
Subgroup analysis of antiviral therapy timing
By subgroup analysis, 192 HBV-SHCC patients treated with TACE, including 134 patients in NA-experienced group (69.8%), 43 patients in NA-naïve group (22.4%) and 15 patients in untreated group (7.8%) were included as three groups, respectively. NA-naïve group meant that HBV-SHCC patients were diagnosed for the first time before taking antiviral drugs. Untreated group meant that HBV-SHCC patients never were treated with antiviral therapy during the whole course of treatment. The detailed information about demographic and clinical characteristics of the subjects is listed in Table 2. There are no significant differences in demographic and clinical characteristics of the subjects by comparison of NA-experienced group, NA-naïve group and untreated group. However, the median survival time of HBV-SHCC patients was 38 (24–52) months in NA-experienced group, 31 (18.5–42.5) months in NA-naïve group, and 13 (11–31.5) months in the untreated group. There were significant difference among three groups (P=0.013). Therefore, it illustrates that there is no significant interaction among the variables in each group. However, ART timing might be one of the crucial factors to prolong the survival time of HBV-SHCC patients.
 |
Table 2 Comparison of demographic data and tumor characteristics among the three groups of patients with hepatitis B virus-related small hepatocellular carcinomas |
Subgroup analysis of NA strategies
As a result of previous national regulations on antiviral drugs, there were 4 NAs in our hospital, including ETV, LAM, ADV and TBV; 177 patients receiving NA treatment were enrolled by subgroup analysis, including 138 male and 39 female (mean age, 55.25±10.65 years; range, 13–82 years). The median survival time of HBV-SHCC patients was 41 (20–57) months in the ADV group, 44 (23.5–53.25) months in the LAM+ADV group, 27 (17.75–45) months in the ETV group, 37 (23.25–53) months in the LAM group, and 31 (20–52.25) in the TBV group. By comparing variables, the data shows that there are no significant differences in demographic and clinical characteristics of the subjects by comparison of five groups mentioned above. However, it indicates that HBV-SHCC patients with different NA strategies could have different survival time. Obviously, HBV-SHCC patients treated with ADV or combined with LAM have longest survival time. Of these patients, 48 (78.68%) patients treated with ADV and 22 (84.62%) patients treated with LAM+ADV in the experienced NA group, 13 (21.31%) patients treated with ADV and 4 patients (15.38%) treated with LAM+ADV in the naive NA group.
Subgroup analysis of viral response after NA treatment
HBV-SHCC patients receiving different NA treatment had different viral responses. Most patients have gotten maintained viral response (MVR) after antiviral treatment, but some patients suffered from viral breakthrough and non-response. In our study, of these patients, we found that 33 (18.6%) patients have gotten viral breakthrough from these patients receiving NA treatment. However, the viral load and liver function of 10 patients recovered after receiving timely rescue treatment. Twenty-three patients refused to receive timely rescue treatment or received the invalid rescue treatment after viral breakthrough were still low-level viral replication and transaminase level close to normal. The median survival time of HBV-SHCC patients was 38 (24–52) months in the MVR group, 15 (12.5–41) months in the viral breakthrough group, 36 (21–57) months in the non-response group, and 45.5 (34.25–56.25) months in the rescue treatment group. By comparison the variable of four groups mentioned above, the data showed that there were no significant differences in demographic and clinical characteristics of the subjects (all of them, P>0.05). Similarly, the data suggested that patients who have received rescue treatment after viral breakthrough or gotten MVR had longer survival times than those who have not received rescue treatment after viral breakthrough or non-response.
Survival rate
Risk factors associated with the survival of HBV-SHCC by subgroup analyses. The Kaplan–Meier survival analyses were used to analyze the influence factors of survival rates among the different subgroups. There were no significant differences in the cumulative survival rate when classifying by gender (Log-rank, P=0.735), cirrhosis (Log-rank, P=0.539), IM (Log-rank, P=0.487), NA strategies (Log-rank, P=0.190). However, there were significant differences in the cumulative survival rate of SHCC patients with Child-Pugh grade, BCLC stage, PVTT, ART timing, viral response (all of them, Log-rank, P<0.05). As shown in Figure 2A–C, patients with Child-Pugh A, BCLC stage A and without PVTT have higher cumulative survival rate than patients classified as Child-Pugh B and BCLC stage B or classified as Child-Pugh C, BCLC stage C and BCLC stage D, with PVTT (Log-rank, P=0.008, P<0.001 and P<0.001, respectively). Likewise, the data indicated that patients who have received NA-experienced treatment and getting MVR have higher cumulative survival rate than those of NA-naive treatment group or untreated treatment group from Figure 3A. Moreover, according to the calculation of Figure 3B, patients who have gotten MVR or received timely rescue therapy after viral breakthrough have higher cumulative survival rate than those of sustained lower level viral after viral breakthrough or non-response (Log-rank, P<0.001).
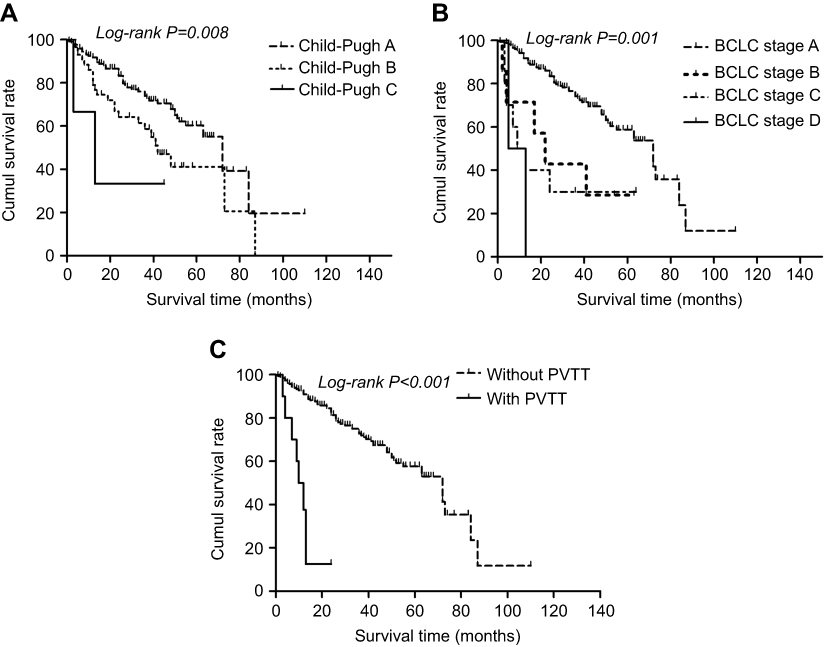 |
Figure 2 The Kaplan–Meier survival curves for patients with HBV-related small hepatocellular carcinomas: (A) significantly higher cumulative survival rate of patients with Child-Pugh A (dashed line) compared to those with Child-Pugh B (dotted line) or C (solid line). (B) Significantly higher cumulative survival rate of patients with BCLC stage A (dashed line) compared to those with BCLC stage B (bold-dotted line), C (dotted line) or D (solid line). (C) Significantly higher cumulative survival rate of patients without PVTT (dashed line) compared to those with PVTT (solid line). Abbreviations: HBV, hepatitis B virus; BCLC, Barcelona Clinic Liver Cancer; PVTT, portal vein tumor thrombus. |
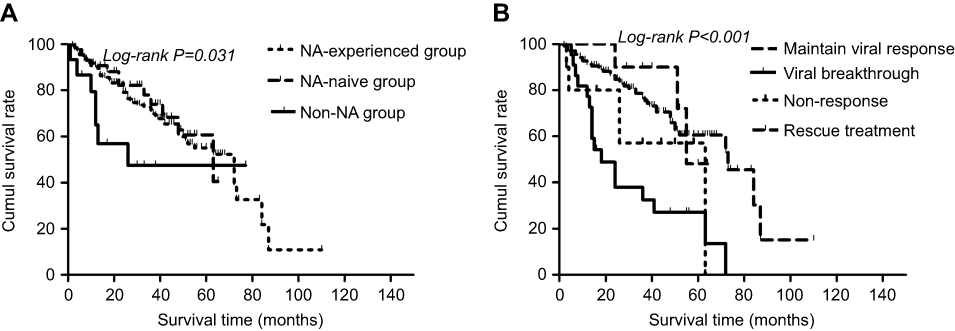 |
Figure 3 The Kaplan–Meier survival curves for patients with HBV-related small hepatocellular carcinomas: (A) significantly higher cumulative survival rate of patients with NA-experienced treatment group (dashed line) compared to those with NA-naïve treatment (dotted line) or untreated treatment (solid line). (B) Significantly higher cumulative survival rate of patients with timely rescue treatment group (bold-dashed line) compared to patients with maintained viral response group (dashed line), non-response (dotted line) and viral breakthrough (solid line). Abbreviations: HBV, hepatitis B virus; NA, nucleos(t)ide analog. |
Results of univariate survival analysis demonstrated that viral breakthrough was a prognostic predictor. Viral breakthrough was associated with worse overall survival rate (HR =4.537, P=0.016). Other prognostic variables were presented in Table 3. Of these variables, patients with Child-Pugh A (HR=0.059, P<0.001), BCLC stage A (HR=0.048, P<0.001), without PVTT, MVR were related to better overall survival rate.
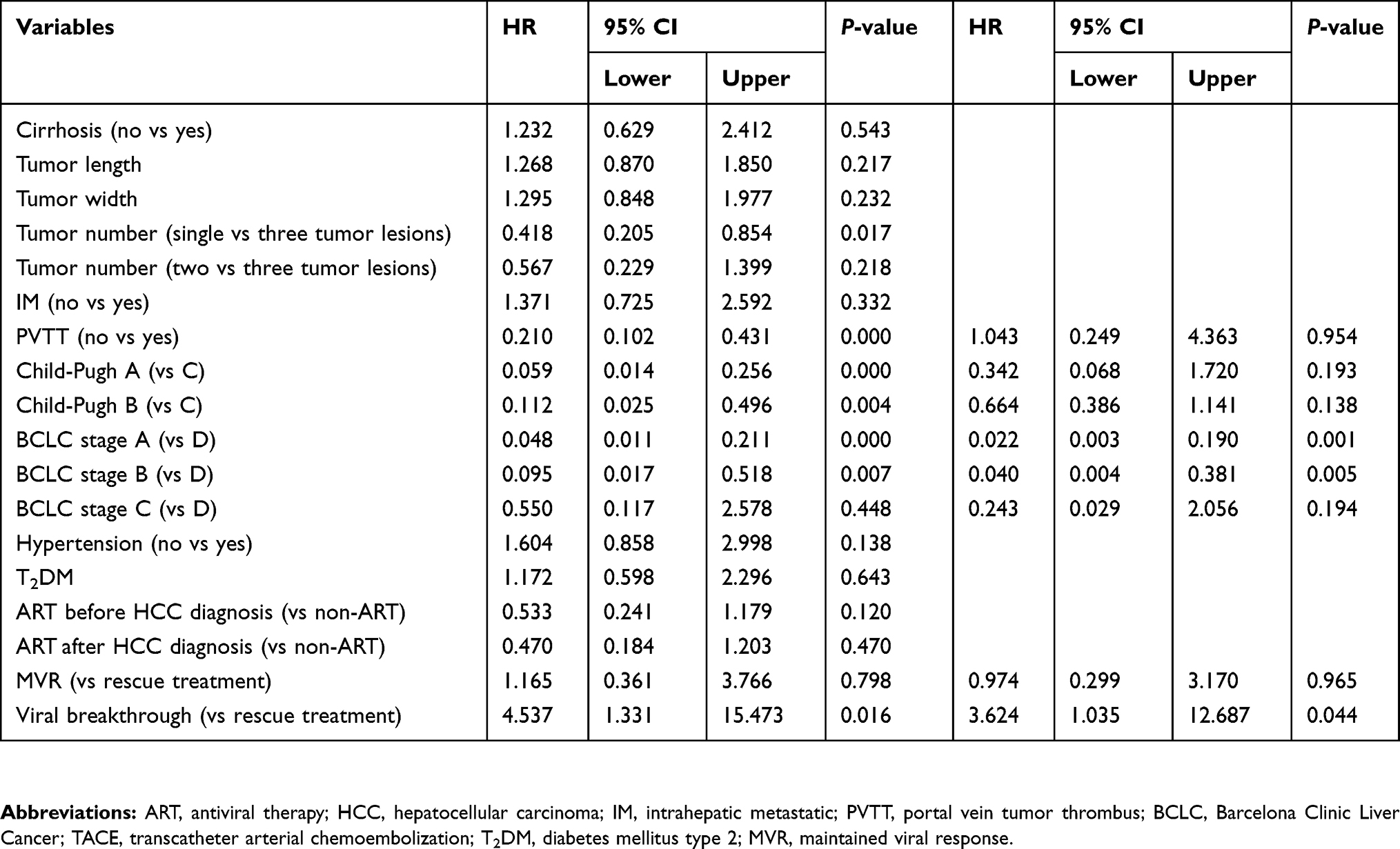 |
Table 3 Results of univariate and multivariate analyses in 192 patients with hepatitis B virus-related small hepatocellular carcinomas |
In order to eliminate the confounding factors, Cox-proportional hazards model was used to evaluate the risk factors for the survival of HBV-SHCC. Variables included in the analysis were Child-Pugh grades, BCLC stages, PVTT, and virology response. Table 3 shows that viral breakthrough (HR=3.624, P=0.044) was an independent risk factor of the survival of HBV-SHCC. In contrast, BCLC stage A (HR=0.022, P=0.001) and BCLC stage B (HR=0.040, P=0.005) were independent protective factors for the survival of HBV-SHCC. Namely, viral breakthrough was a significant risk factor for HBV-SHCC development with a HR of 3.624 (95% CI, 1.035–12.687; P=0.044) together with worse BCLC stages.
Discussion
HCC is one of the major causes of cancer-related mortality worldwide, with most of the cases associated with sustained HBV or HCV infection.19,20 In particular, chronic HBV infection is the main risk factor for the development of HCC in Asian and African populations.21 Surgical resection, liver transplantation, PMCT, and TACE are increasingly used for the treatment of HCC.22–24 Of these treatments for HCC, TACE is effective in prolonging survival time. Moreover, it has been shown to be as effective as surgical resection.25,26 However, with regard to TACE in patients with HBV-SHCC, HBV reactivation and the subsequent hepatic failure directly caused by HBV reactivation have been reported scarcely and taken seriously by radiologist and clinician. Therefore, our study focused on investigating the impact of NA treatment on the survival of HBV-SHCC patients treated with TACE. The medical history, imaging features and laboratory results of HBV-SHCC patients were analyzed comprehensively. Three aspects of this problem have been addressed in the present study. The first question involved the comparison of NA-experienced, NA-naïve and non-NA treatment modalities for HBV-SHCC patients undergoing TACE. The second aspect demonstrated that patients treated with ADV and LAM+ADV had longer survival time than those treated with ETN, LAM and TBV. The third question was associated with the exploration of predictive factors for HBV-SHCC patients. It was confirmed that there were significant differences in the cumulative survival rate of HBV-SHCC patients, including Child-Pugh grade, BCLC stage, PVTT, and virology response. Then, Cox-regression analysis indicated that BCLC stages and virology response were independent predictors for HBV-SHCC patients.
HCC is the malignancy with the highest association with HBV infection.27 Moreover, HBV reactivation and abnormal liver function might be accompanied by severe clinical symptoms in the development of chronic hepatitis. Therefore, antiviral therapy timing was vital to prevent the development of chronic hepatitis. The ultimate goal of treatment for CHB is to prevent HCC, but not completely eliminate HCC.28 Moreover, once HCC occurred, patients might undergo surgical resection, liver transplantation, and local mini-invasive therapies.7 Of these treatments might be one of the reasons leading to HBV reaction.29 It was controversial that the incidence of HBV reactivation of HCC patients during or after TACE was not as frequent as with systemic chemotherapy for hematological malignancies.30 Some research team reported that postoperative HBV-HCC patients receiving NA treatment might have longer survival times compared to patients without NA.29,31–33 In our study, it was demonstrated that ART timing was not only associated with the survival times, but the cumulative survival rate of NA-experienced group was higher than NA-naïve group or untreated group for HBV-SHCC patients. Namely, patients receiving NA-experienced group had longer survival times than receiving NA-naïve group or untreated group.
During the last decade, great strides have been made in the treatments of HBV infection, especially in Asian. Shim et al reported that extending of oral antiviral indication may reduce the HCC risk in Korea.34 The inhibition of viral replication could represent a reasonable target for HCC prevention.35 However, there were different views about the choice of NAs. Some research groups have drawn different values about the type of NAs in HBV-HCC patients. Papatheodoridis et al indicated that CHB patients treated with mid-term nucleoside analogs had a significantly lower incidence of HCC than untreated patients, but could not completely eliminate the risk of HCC and prevent the development of HCC.36,37 Yoo et al reported that current treatment with NAs can successfully suppress the virus replication but cannot eradicate cccDNA. Thus, there still remains a great need for a cure for HBV.38,39 In brief, patients should continue to undergo HCC surveillance even if they have achieved successful HBV suppression.40,41
Up to date, ETV and TDF are considered to be high resistance barrier antiviral drugs, which belong to the first-line antiviral therapy of chronic HBV infection.42 We strive to find out the evidence and literature that ETV can prolong the survival time of patients with HCC. However, by searching for a large number of relevant literature, it also has not been confirmed that ETV can prolong the survival time of patients and improve the overall survival rate compared with other antiviral drugs.33,43–45 Based on the conclusions of our article, we analyze the reasons as follows. First of all, we cannot rule out the result bias caused by our small sample size. Secondly, Stalke et al has indicated that low HBV viral load predicted positive response to antiviral therapy.46 The ideal candidate for antiviral therapy is an immunocompetent, young female with low HBV viral load and elevated alanine transaminase activity.46 Although there was no statistical difference among all patients receiving antiviral therapy, ADV accounted for the highest proportion of patients before SHCC diagnosis. This may be responsible for the inhibition of the virus after ADV treatment, resulting in longer survival time of patients treated with ADV than other antiviral drugs. Thirdly, Jin et al have reported that ETV monotherapy can improve hepatic function in HBV-related HCC patients. An early virological response to ETV is prognostic of improved survival following curative therapy against HBV-related HCC in 2011.45 In the same year, Wong et al reported that anti-viral therapy has potential beneficial effects after the curative treatment of HBV-related HCC in terms of tumor recurrence, liver-related mortality and overall survival. Anti-viral therapy should be considered after curative treatment of HCC.44 Then, Kim et al showed that overall survival and recurrence-free survival were better in the ETV-treated patients than in the LAM treated-patients, indicating that the potent antiviral drug should be the preferred choice in HBV-related HCC patients in 2016.47 Cho et al reported that antiviral agents with high genetic barrier to resistance (ETV and TDF) reduced the risk of HCC recurrence compared with other antivirals and no antiviral treatment, especially in patients with high baseline viral load in 2018.48 However, there are conflicting or ambiguous views on the difference of therapeutic outcomes between nucleoside analogs and HCC. Firstly, Hsu et al reported that the risk of HCC in patients with chronic hepatitis B receiving ETV or TDF declines over time and is determined by age, male sex, cirrhosis, diabetes, and HCV coinfection.49 In addition, Arends et al reported that cumulative incidence of HCC is low in patients treated with ETV, but ETV does not eliminate the risk of HCC.43 Shin et al and Liu et al reported that the antiviral efficacy of ETV and LAM was similar and the type of antiviral agents did not influence overall survival in patients with HBV-HCC.33,50 Then, Huang et al reported that ART with TBV can significantly decrease the preoperative reactivation of viral replication in HBV-HCC patients undergoing surgical resection.16 Zhong et al reported that LAM and ADV were associated with similar survival benefit in patients with HBV-HCC after surgical resection treatment.28 What is more, Liu et al further affirmed that in HBV-HCC patient after curative treatment, NA improve the prognosis; ETV was not found to be superior to other NA based on available data by using meta-analysis.33 We also found an interesting phenomenon that the incidence of complete suppression of HBV DNA replication after initial antiviral therapy with ETV after SHCC diagnosis was not high, and the specific reasons are not yet clear. There are a small number of literature supporting that ADV antiviral therapy can prolong the survival time of patients. Huang et al reported that patients with hepatitis B-related HCC receiving ADV treatment reduced late HCC recurrence and significantly improved overall survival after R0 hepatic resection in the randomized controlled trial in 2015.16 Additionally, Akima et al reported that their findings suggest that the addition of ADV to ongoing LAM therapy cannot completely suppress hepatocarcinogenesis, but is useful for improving liver function in patients with LAM-resistant HBV-related cirrhosis, allowing HCC surgery.51 However, due to the drug properties of ADV, the therapeutic effects of ADV have been evaluated in some literature. First of all, Elefsiniotis et al indicated that ADV suppresses viral replication in more than 70% of LAM-R cirrhotic patients during the first year of treatment in 2009.52 Then, Hosaka confirmed that HCC can develop in cirrhotic patients receiving ADV add-on LAM. Hence, the patients with baseline AST≥70 IU/L and YIDD mutants would need to be monitored closely for HCC in 2010.53
To sum up, larger samples and further prospective studies should be carried out to confirm the results of this study in the future. There were rare reports about the relationship between NA treatment and survival of HBV-SHCC patients in China. In our study, we found that ART timing was not only associated with survival time, but also patients receiving ADV monotherapy or combined with LAM had longer survival time than those of other three NA groups. This result was not completely the same to other research groups.33,50 We found that most patients receiving ADV or LAM+ADV had longer survival time than ETV groups. Of these patients, it was found that 48 (78.68%) patients treated with ADV and 22 (84.62%) patients treated with LAM+ADV in the experienced NA group and got MVR or timely rescue treatment, 13 (21.31%) patients treated with ADV and 4 patients (15.38%) treated with LAM+ADV in the naive NA group by further analysis. Therefore, it might be appropriate to continue to take ADV or LAM+ADV for HBV-SHCC patients who have gotten MVR, even from theoretical point of view, the rate of drug resistance of ADV was higher than ETV. However, mechanisms leading to this kind of results were unclear and needed further study.
Sustained HBV replication was associated with the HCC development.5 Patients with serum HBV replication levels between 4 and <6 log(10) copies/mL were most likely to present with HCC.54 Moreover, it was reported that a high serum concentration of HBV DNA (≥4 log (10) copies/mL) was a strong risk factor for HCC recurrence after surgical resection.55 Therefore, NA treatment had been giving for these patients. However, beneficial effect of ART might be blunted by the development of viral resistance.56 Furthermore, the effect of viral breakthrough in the HBV-SHCC patients with low viral load and timely rescue treatment for viral breakthrough remains unclear.57 Our study indicated that degree of viral suppression after NA treatment was not only associated with survival time, but affected the survival rate of patients with HBV-SHCC. Patients got MVR had longer survival times than other groups. By comparison of subgroup analysis, we found that patients got MVR had longer survival time than patients with viral breakthrough. Patients receiving timely rescue treatment had longer survival time than without rescue treatment for viral breakthrough. Therefore, the selection of antiviral drugs and timely rescue treatment to maintain HBV suppression were necessary and essential for HBV-SHCC patients.
Kaplan-Meier survival analysis demonstrated that Child-Pugh grade and BCLC stage were beneficial factors for the survival time of patients with SHCC. Conversely, PVTT was identified as an adverse factor. Those results were similar to other associated HCC types.58–60 Cox-regression analysis demonstrated that BCLC stage was a protective factor for survival time and patients with SHCC who classified as BCLC stage A or BCLC stage B had higher survival rates than those grouped in BCLC stage C. Previous publications have reported that diabetes mellitus type 2 and impaired glucose tolerance are predictors of poor prognosis for patients with SHCC (≤5 cm).61 However, it was not determined in the present study that there was any association between diabetes mellitus type 2 and the prognosis of SHCC (≤3 cm).
In conclusion, the NA treatment and virology response played crucial role in prolonging survival time and was protective factor for HBV-SHCC patients undergoing TACE. Therefore, regardless of before or after treatment of the local tumor lesions, NA treatment should be administrated to HBV-SHCC patients as soon as possible in order to sustain or maintain HBV suppression. Viral breakthrough was an independent risk factor for HBV-SHCC patients. HBV-SHCC patients who received NA treatment should be followed carefully and regularly, and timely rescue treatments were needed to manage once the virus mutates, regardless of liver function status. If patients treated with ADV or LAM+ADV got MVR, it was appropriate to continue to previous therapeutic schedule. In addition, BCLC stage was an independent protective factor for HBV-SHCC patients.
Ethical approval and informed consent
All procedures in the current study were in accordance with the ethical standards of the Institutional Research Committee and with the Helsinki declaration. The study was approved by the Ethics Committee of the Second Hospital of Nanjing and written informed consent for participation was obtained. This study had no influence on the subsequent management of patients.
Acknowledgments
This research was partially supported by grants from Jiangsu Provincial Special Program of Medical Science (No. BL2014005 to Yongxiang Yi), the Science and Technology Commission of Nanjing (No. 201605033 to Wei Ye), the Project of Six Talent Peaks of Jiangsu Province (No. WSN-177 to Wei Ye) and the Project of Jiangsu Provincial Medical Youth Talent (Wei Ye), Nanjing Medical Science and Technology Development Foundation (No. YKK-17173 to Wei Ye).
Author contributions
YW and YY contributed to study concept and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, and statistical analysis. CT contributed to study concept and design, technical support and data acquisition. WY performed statistical analysis. YY, CT and WY contributed to technical support and data acquisition. WY and WZ contributed to study concept and design, analysis and interpretation of data, critical revision of the manuscript for important intellectual content, and study supervision. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qin S, Bai Y, Lim HY, et al. Randomized, multicenter, open-label study of oxaliplatin plus fluorouracil/leucovorin versus doxorubicin as palliative chemotherapy in patients with advanced hepatocellular carcinoma from Asia. J Clin Oncol. 2013;31:3501–3508. doi:10.1200/JCO.2012.44.5643
2. Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012;30:2212–2219. doi:10.1016/j.vaccine.2011.12.116
3. Ariizumi S, Takasaki K, Yamamoto M, Ohtsubo T, Katsuragawa H, Katagiri S. Histopathologic differentiation of the main nodule determines outcome after hepatic resection for synchronous multicentric hepatocellular carcinomas. Hepatogastroenterology. 2004;51:500–504.
4. de Martel C, Maucort-Boulch D, Plummer M, Franceschi S. World-wide relative contribution of hepatitis B and C viruses in hepatocellular carcinoma. Hepatology. 2015;62:1190–1200. doi:10.1002/hep.27969
5. Zhou JY, Zhang L, Li L, Gu GY, Zhou YH, Chen JH. High hepatitis B virus load is associated with hepatocellular carcinomas development in Chinese chronic hepatitis B patients: a case control study. Virol J. 2012;9:16. doi:10.1186/1743-422X-9-16
6. Llovet JM, Fuster J, Bruix J. Barcelona-clinic liver cancer G. The barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004;10:S115–S20. doi:10.1002/lt.20034
7. Kim GA, Shim JH, Kim MJ, et al. Radiofrequency ablation as an alternative to hepatic resection for single small hepatocellular carcinomas. Br J Surg. 2016;103:126–135. doi:10.1002/bjs.9960
8. Watanabe S, Morishita A, Deguchi A, et al. Ethanol injection therapy for small hepatocellular carcinomas located beneath a large vessel using a curved percutaneous ethanol injection therapy needle. Oncol Lett. 2014;7:1831–1834. doi:10.3892/ol.2014.2053
9. Lei J, Wang W, Yan L. Surgical resection versus open-approach radiofrequency ablation for small hepatocellular carcinomas within milan criteria after successful transcatheter arterial chemoembolization. J Gastrointest Surg. 2013;17:1752–1759. doi:10.1007/s11605-013-2311-5
10. Terzi E, Piscaglia F, Forlani L, et al. TACE performed in patients with a single nodule of hepatocellular carcinoma. BMC Cancer. 2014;14:601. doi:10.1186/1471-2407-14-601
11. Yang WZ, Jiang N, Huang N, Huang JY, Zheng QB, Shen Q. Combined therapy with transcatheter arterial chemoembolization and percutaneous microwave coagulation for small hepatocellular carcinoma. World J Gastroenterol. 2009;15:748–752. doi:10.3748/wjg.15.748
12. Kitamoto M, Imagawa M, Yamada H, et al. Radiofrequency ablation in the treatment of small hepatocellular carcinomas: comparison of the radiofrequency effect with and without chemoembolization. AJR Am J Roentgenol. 2003;181:997–1003. doi:10.2214/ajr.181.4.1810997
13. Gong WF, Zhong JH, Lu SD, et al. Effects of antiviral therapy on post-hepatectomy HBV reactivation and liver function in HBV DNA-negative patients with HBV-related hepatocellular carcinoma. Oncotarget. 2017;8(9):15047.
14. Jiang E, Shangguan AJ, Chen S, Tang L, Zhao S, Yu Z. The progress and prospects of routine prophylactic antiviral treatment in hepatitis B-related hepatocellular carcinoma. Cancer Lett. 2016;379:262–267. doi:10.1016/j.canlet.2015.07.016
15. Huang S, Xia Y, Lei Z, et al. Antiviral therapy inhibits viral reactivation and improves survival after repeat hepatectomy for hepatitis B virus-related recurrent hepatocellular carcinoma. J Am Coll Surg. 2017;224:283–93 e4. doi:10.1016/j.jamcollsurg.2016.11.009
16. Huang G, Lau WY, Wang ZG, et al. Antiviral therapy improves postoperative survival in patients with hepatocellular carcinoma: a randomized controlled trial. Ann Surg. 2015;261:56–66. doi:10.1097/SLA.0000000000000858
17. Wu CY, Chen YJ, Ho HJ, et al. Association between nucleoside analogues and risk of hepatitis B virus-related hepatocellular carcinoma recurrence following liver resection. J Am Med Assoc. 2012;308:1906–1913. doi:10.1001/2012.jama.11975
18. Wu CY, Lin JT, Lee TT, Chen YJ, Hsu YC, Wu MS. Association between nucleoside analogues and mortality of hepatitis B virus-related hepatocellular carcinoma following transarterial chemoembolization. Gastroenterology. 2013;144:S967–S8. doi:10.1016/S0016-5085(13)63593-3
19. Huo TI, Wu JC, Hsia CY, et al. Hepatitis C virus infection is a risk factor for tumor recurrence after resection of small hepatocellular carcinomas. World J Surg. 2004;28:787–791. doi:10.1007/s00268-004-7320-9
20. Chen CH, Huang GT, Yang PM, et al. Hepatitis B- and C-related hepatocellular carcinomas yield different clinical features and prognosis. Eur J Cancer. 2006;42:2524–2529. doi:10.1016/j.ejca.2006.06.007
21. Cheon JH, Park JW, Park KW, et al. [The clinical report of 1,078 cases of hepatocellular carcinomas: national cancer center experience]. Korean J Hepatol. 2004;10:288–297.
22. Ochiai T, Sonoyama T, Kikuchi S, et al. [Multiple hepatocellular carcinomas successfully treated by combined therapies]. Gan To Kagaku Ryoho. 2005;32:1809–1811.
23. Blendis L. Percutaneous ethanol ablation of small hepatocellular carcinomas: twenty years on. Gastroenterology. 2006;130:280–282. discussion 2. doi:10.1053/j.gastro.2005.10.063
24. Masuda T, Beppu T, Ishiko T, et al. [Local ablation therapy combined with liver resection for multiple hepatocellular carcinomas]. Gan To Kagaku Ryoho. 2007;34:2077–2079.
25. Llovet JM, Real MI, Montana X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359:1734–1739. doi:10.1016/S0140-6736(02)08649-X
26. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37:429–442. doi:10.1053/jhep.2003.50047
27. Bruix J, Llovet JM. Hepatitis B virus and hepatocellular carcinoma. J Hepatol. 2003;39(Suppl 1):S59–S63. doi:10.1016/S0168-8278(03)00140-5
28. Zhong JH, Yang T, Xiang BD, Li LQ, Ma L. Antiviral therapy for hepatitis B virus-related hepatocellular carcinoma after surgery: a comment for moving forward. World J Hepatol. 2016;8:605–606. doi:10.4254/wjh.v8.i13.605
29. Ke Y, Wang L, Li LQ, Zhong JH. Nucleos(t)ide analogues to treat hepatitis B virus-related hepatocellular carcinoma after radical resection. World J Hepatol. 2014;6:652–659. doi:10.4254/wjh.v6.i9.652
30. Jang JW. Hepatitis B virus reactivation in patients with hepatocellular carcinoma undergoing anti-cancer therapy. World J Gastroenterol. 2014;20:7675–7685. doi:10.3748/wjg.v20.i24.7675
31. Sakamoto K, Beppu T, Hayashi H, et al. Antiviral therapy and long-term outcome for hepatitis B virus-related hepatocellular carcinoma after curative liver resection in a Japanese cohort. Anticancer Res. 2015;35:1647–1655.
32. Yuan P, Chen P, Qian Y. Evaluation of antiviral therapy performed after curative therapy in patients with HBV-related hepatocellular carcinoma: an updated meta-analysis. Can J Gastroenterol Hepatol. 2016;2016:5234969.
33. Liu GM, Huang XY, Shen SL, Hu WJ, Peng BG. Adjuvant antiviral therapy for hepatitis B virus-related hepatocellular carcinoma after curative treatment: a systematic review and meta-analysis. Hepatol Res. 2016;46:100–110. doi:10.1111/hepr.12584
34. Shim JJ, Oh IH, Kim SB, et al. Predictive value of antiviral effects in the development of hepatocellular carcinoma in the general Korean population with chronic hepatitis B. Gut Liver. 2016;10:962–968. doi:10.5009/gnl15426
35. Hann HW. Active antiviral therapy for chronic hepatitis B and hepatocellular carcinoma. Minerva Gastroenterol Dietol. 2008;54:19–30.
36. Papatheodoridis GV, Lampertico P, Manolakopoulos S, Lok A. Incidence of hepatocellular carcinoma in chronic hepatitis B patients receiving nucleos(t)ide therapy: a systematic review. J Hepatol. 2010;53:348–356. doi:10.1016/j.jhep.2010.02.035
37. Papatheodoridis GV, Manolakopoulos S, Touloumi G, et al. Virological suppression does not prevent the development of hepatocellular carcinoma in HBeAg-negative chronic hepatitis B patients with cirrhosis receiving oral antiviral(s) starting with lamivudine monotherapy: results of the nationwide HEPNET. Greece cohort study. Gut. 2011;60:1109–1116. doi:10.1136/gut.2010.221846
38. Yoo J, Hann HW, Coben R, Conn M, DiMarino AJ. Update treatment for HBV infection and persistent risk for hepatocellular carcinoma: prospect for an HBV Cure. Diseases. 2018;6(2):27. doi:10.3390/diseases6020027
39. Shinn BJ, Martin A, Coben RM, et al. Persistent risk for new, subsequent new and recurrent hepatocellular carcinoma despite successful anti-hepatitis B virus therapy and tumor ablation: the need for hepatitis B virus cure. World J Hepatol. 2019;11:65–73. doi:10.4254/wjh.v11.i1.65
40. Vlachogiannakos J, Papatheodoridis G. Hepatocellular carcinoma in chronic hepatitis B patients under antiviral therapy. World J Gastroenterol. 2013;19:8822–8830. doi:10.3748/wjg.v19.i47.8822
41. Dargan A, Wong SY, Coben R, Conn M, Dimarino AJ, Hann HW. Persistent risk for hepatocellular carcinoma after more than a decade of successful hepatitis B virus suppression. Minerva Gastroenterol Dietol. 2017;63:74–76. doi:10.23736/S1121-421X.16.02350-3
42. Rago A, Lichtner M, Mecarocci S, et al. Antiviral treatment including entecavir plus tenofovir disoproxil fumarate for HBV reactivation following a rituximab-based regimen. Antiviral Ther. 2010;15:929–932. doi:10.3851/IMP1633
43. Arends P, Sonneveld MJ, Zoutendijk R, et al. Entecavir treatment does not eliminate the risk of hepatocellular carcinoma in chronic hepatitis B: limited role for risk scores in caucasians. Gut. 2015;64:1289–1295. doi:10.1136/gutjnl-2014-307023
44. Wong JS, Wong GL, Tsoi KK, et al. Meta-analysis: the efficacy of anti-viral therapy in prevention of recurrence after curative treatment of chronic hepatitis B-related hepatocellular carcinoma. Aliment Pharmacol Ther. 2011;33:1104–1112. doi:10.1111/j.1365-2036.2011.04634.x
45. Jin YJ, Shim JH, Lee HC, et al. Suppressive effects of entecavir on hepatitis B virus and hepatocellular carcinoma. J Gastroenterol Hepatol. 2011;26:1380–1388. doi:10.1111/j.1440-1746.2011.06776.x
46. Stalke P, Rybicka M, Wroblewska A, et al. An initial assessment of correlations between host- and virus-related factors affecting analogues antiviral therapy in HBV chronically infected patients. Med Sci Monit. 2014;20:321–328. doi:10.12659/MSM.889788
47. Kim JH, Sinn DH, Kim K, et al. Lamivudine versus entecavir for newly diagnosed hepatitis B virus-related hepatocellular carcinoma. Gut Liver. 2016;10:939–947. doi:10.5009/gnl15527
48. Cho H, Ahn H, Lee DH, et al. Entecavir and tenofovir reduce hepatitis B virus-related hepatocellular carcinoma recurrence more effectively than other antivirals. J Viral Hepat. 2018;25:707–717. doi:10.1111/jvh.12855
49. Hsu YC, Ho HJ, Lee TY, et al. Temporal trend and risk determinants of hepatocellular carcinoma in chronic hepatitis B patients on entecavir or tenofovir. J Viral Hepat. 2018;25:543–551. doi:10.1111/jvh.12832
50. Shin HS, Kim SU, Park JY, et al. Antiviral efficacy of lamivudine versus entecavir in patients with hepatitis B virus-related advanced hepatocellular carcinoma. J Gastroenterol Hepatol. 2012;27:1528–1534. doi:10.1111/j.1440-1746.2012.07145.x
51. Akima T, Tamano M, Yamagishi H, Kubota K, Fujimori T, Hiraishi H. Surgical treatment of HCC in a patient with lamivudine-resistant hepatitis B cirrhosis with adefovir dipivoxil. World J Hepatol. 2010;2:318–321. doi:10.4254/wjh.v2.i8.318
52. Elefsiniotis I, Buti M, Jardi R, Vezali E, Esteban R. Clinical outcome of lamivudine-resistant chronic hepatitis B patients with compensated cirrhosis under adefovir salvage treatment. Importance of HCC surveillance. Eur J Intern Med. 2009;20:478–481. doi:10.1016/j.ejim.2008.12.013
53. Hosaka T, Suzuki F, Kobayashi M, et al. Development of HCC in patients receiving adefovir dipivoxil for lamivudine-resistant hepatitis B virus mutants. Hepatol Res. 2010;40:145–152. doi:10.1111/j.1872-034X.2009.00582.x
54. Xu J, Lin Y, Wang YP, et al. Hepatitis B virus DNA in patients with hepatitis B-related liver cirrhosis with or without hepatocellular carcinomas: a matched case-control study. J Dig Dis. 2009;10:138–144. doi:10.1111/j.1751-2980.2009.00376.x
55. Urata Y, Kubo S, Takemura S, et al. Effects of antiviral therapy on long-term outcome after liver resection for hepatitis B virus-related hepatocellular carcinoma. J Hepatobiliary Pancreat Sci. 2012;19:685–696. doi:10.1007/s00534-011-0489-z
56. Lai CL, Yuen MF. Prevention of hepatitis B virus-related hepatocellular carcinoma with antiviral therapy. Hepatology. 2013;57:399–408. doi:10.1002/hep.25937
57. Chen JL, Lin XJ, Zhou Q, Shi M, Li SP, Lao XM. Association of HBV DNA replication with antiviral treatment outcomes in the patients with early-stage HBV-related hepatocellular carcinoma undergoing curative resection. Chin J Cancer. 2016;35:28. doi:10.1186/s40880-016-0089-z
58. Bholee AK, Peng K, Zhou Z, et al. Radiofrequency ablation combined with transarterial chemoembolization versus hepatectomy for patients with hepatocellular carcinoma within Milan criteria: a retrospective case-control study. Clin Transl Oncol. 2017;19:844–852. doi:10.1007/s12094-016-1611-0
59. Choi D, Lim HK, Rhim H, et al. Percutaneous radiofrequency ablation for early-stage hepatocellular carcinoma as a first-line treatment: long-term results and prognostic factors in a large single-institution series. Eur Radiol. 2007;17:684–692. doi:10.1007/s00330-006-0461-5
60. Kim BK, Ahn SH, Seong JS, et al. Early alpha-fetoprotein response as a predictor for clinical outcome after localized concurrent chemoradiotherapy for advanced hepatocellular carcinoma. Liver Int. 2011;31:369–376. doi:10.1111/j.1478-3231.2010.02368.x
61. Khan MMH, Saito S, Takagi S, et al. Relationship between hepatocellular carcinoma and impaired glucose tolerance among Japanese. Hepato-Gastroenterol. 2006;53:742–746.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.