")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Impact of Air Pollutants and Pollen on the Severity of Nonallergic Rhinitis: A Data-Oriented Analysis
Authors Huang Y, Zhang Y, Wang J, Li X, Wang C, Chen R, Zhang L
Received 30 April 2022
Accepted for publication 24 July 2022
Published 6 August 2022 Volume 2022:15 Pages 1045—1054
DOI https://doi.org/10.2147/JAA.S372927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Yanran Huang,1– 3,* Yuan Zhang,1– 3,* Jiajia Wang,4,5 Xiaobo Li,4,5 Chengshuo Wang,1,2 Rui Chen,4,5 Luo Zhang1– 3
1Department of Allergy, Beijing TongRen Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Otolaryngology Head and Neck Surgery, Beijing TongRen Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Beijing Key Laboratory of Nasal Diseases, Beijing Institute of Otolaryngology, Beijing, People’s Republic of China; 4Beijing Key Laboratory of Environmental Toxicology, Capital Medical University, Beijing, People’s Republic of China; 5School of Public Health, Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Luo Zhang, Beijing Key Laboratory of Nasal Diseases, Beijing Institute of Otolaryngology, No. 17, HouGouHuTong, DongCheng District, Beijing, 100005, People’s Republic of China, Email [email protected] Rui Chen, Beijing Key Laboratory of Environmental Toxicology, Capital Medical University, 10 Xitoutiao, You’anmen, Fengtai District, Beijing, 100069, People’s Republic of China, Email [email protected]
Background: Rhino-conjunctivitis symptoms are more severe in nonallergic rhinitis (NAR) patients during pollen season than in other seasons. Little is known about the role of pollen and air pollutants on the severity of NAR.
Objective: The aim of this study is to assess the cross-sectional effects of both pollen and air pollutants on NAR patients during the pollen and non-pollen seasons, and to further explore the possible relationship among these triggers.
Methods: A total of 2411 clinically diagnosed NAR outpatients from 2018 to 2019 were recruited for this study. The severity of NAR was measured using rhinoconjunctivitis symptom scores. Associations of daily exposure to pollen, PM2.5, PM10, NO2, SO2, CO, O3, and rhinoconjunctivitis symptom scores were evaluated using Logistic regression models. Distributed Lag Nonlinear models were used to explore single-day and accumulative Lag effects of environmental factors mentioned above.
Results: During the pollen season, pollen concentration, higher exposure levels of PM10, PM2.5, NO2, and SO2 increased the severity of NAR group when compared with the low-moderate severity group. The high severity group was associated with lower exposure levels of O3. However, during non-pollen seasons, no significant association was found in air pollutant metrics, pollen concentration, and severity of NAR. The exposure-severity effects of pollen were different when different ambient pollutants were stratified.
Conclusion: Synergistic effect of pollen and air pollutants, including PM2.5, PM10, SO2, NO2, and O3, might be responsible for aggravating the symptoms of NAR patients during pollen seasons.
Keywords: air pollution, pollen, nonallergic rhinitis
Introduction
As a common inflammatory disease, chronic rhinitis manifests at least 2 nasal symptoms, including itching, sneezing, rhinorrhea, and nasal congestion for more than 12 weeks.1 With approximately 30% global prevalence, chronic rhinitis could tremendously impair the patients’ quality of life and pose a tremendous financial burden to our society.2,3 Based on its etiology, chronic rhinitis is usually divided into 2 phenotypes, allergic rhinitis (AR) and nonallergic rhinitis (NAR); the former affects 10–40% of the global population,3 while the latter affects 17–52% of the population in different regions.4–7 An observational study showed that the prevalence of AR and NAR in a rural area in northern China was 16.78–24.60%.8
Although AR and NAR share similar clinical symptoms, their clinical characteristics remain distinctive, especially in different seasons.9 Unlike AR, the diagnosis of NAR depends on thorough medical history and a series of exclusion tests for allergen sensitization and rhinosinusitis, which leaves this disease underestimated and undervalued. Segboer et al10 compared the impairment of quality of life between AR and NAR patients and found NAR patients were equally bothered and for some aspects even more affected than AR patients, such as by nasal symptoms, tiredness and lack of sleep, demonstrating that the quality of life was significantly impaired in NAR patients. Usually, NAR patients present perennial symptoms, which are associated with environmental factors, such as air pollutants.11 Our group compared the clinical manifestation of the first-visit NAR patients, who were diagnosed based on positive medical history and negative serum allergen test.9 However, to our surprise, for NAR patients, the severity of all common rhino-conjunctivitis symptoms, including nasal itching, sneezing, rhinorrhea, nasal congestion, watery eyes, and gritty eyes, was significantly higher during pollen seasons than in other seasons.
Since pollen is usually considered to be associated with a specific allergic response, this observation provokes us to understand what triggers these severe symptoms in NAR patients during pollen seasons. In fact, nonspecific nasal hyperreactivity is one of the most prominent features of NAR.12 In recent years, studies have shown that environmental factors, such as air pollution and climate change, have a significant impact on human well-being and contribute significantly to various chronic respiratory diseases.13 With the development of urbanization and industrialization, air pollution has become increasingly severe, and the pollutants were found to be responsible for epithelial barrier dysfunction.14,15 To date, the association between air pollution and NAR is not yet clear.
To sum up, the aim of the present study was, therefore, to assess the effects of both pollen and air pollutants on NAR patients during the pollen seasons and other seasons, and to further explore the possible relationship among these triggers and understand why such patients experience more severe symptoms during pollen seasons.
Materials and Methods
Data Source and Study Design
The 2411 study participants were first-visit outpatients complaining about suffering with chronic rhinitis from the Otorhinolaryngology and Allergy Department of Beijing TongRen Hospital, China, between January 2018 and December 2019. All the enrolled participants were residents in Beijing. In this retrospective study, chronic rhinitis was diagnosed with more than 2 nasal symptoms, such as rhinorrhea, sneezing, nasal congestion, and itching for more than 12 weeks. NAR was then diagnosed using negative allergen test measured by serum-specific IgE (sIgE; UniCAP system, Phadia, Uppsala, Sweden) using a panel of aeroallergen mixture (house dust mites, trees, weed/grass pollen, molds and animal dander). Upper respiratory infections and chronic rhinosinusitis were excluded by nasal endoscopy. Serum sIgE sensitization tests were performed, and population characteristics and detailed medical history were documented. Clinical information on nasal and ocular symptoms was recorded with a 0-to-3-point visual analog scale (VAS). Total nasal symptom score (TNSS) was calculated as the sum of 4 nasal symptoms (rhinorrhea, sneezing, nasal congestion, and itching). Rhinoconjunctivitis symptom scores were calculated by the sum of TNSS and conjunctivitis scores (gritty eyes and watery eyes), from 0 to 15 points.8
The study was approved by the Ethics Committee of Beijing TongRen Hospital and Beijing Institute of Otolaryngology, China, in accordance with the Declaration of Helsinki. Written informed consent was obtained from the participants.
Definition of Pollen Season and Concentration of Air Pollutants
Total pollen concentration and various air pollutants in μg/m3, including NO2, PM2.5, PM10, O3, SO2 and CO, were obtained from Beijing Meteorological Bureau. The pollen season was defined based on total pollen grains provided by Beijing Meteorological Bureau as previously reported, beginning from ≥5 pollen grains/m3 per day for more than 3 consecutive days and ending until <10 pollen grains/m3 per day for more than 3 successive days.9 The pollen seasons were March 13th to May 28th and August 20th to October 1st in 2018, and from March 2nd to June 3rd and August 13th to October 2nd, in 2019.9 Accordingly, the rest of the years was defined as non-pollen seasons.
Statistical Analyses
A descriptive analysis of the basic demographic information of the study population was performed using R: The R Project for Statistical Computing (R 4.1.0 version). Chi-square analysis was used to compare the differences between subgroups. A value of P<0.05 was considered to be statistically significant.
The risk was expressed as an odds ratio (OR) per one interquartile range (IQR, Q3 minus Q1) of each air pollutant. During the study period, the IQR levels of air pollutants were 2 (Q1-Q3;2–4) μg/m3 for sulfur dioxide (SO2), 16 (23–39) μg/m3 for nitrogen dioxide (NO2), 44 (60–104) μg/m3 for ozone (O3), 54 (32–86) μg/m3 for particulate matter ≤10 μm in aerodynamic diameter (PM10), 40(15–55) μg/m3 for particulate matter ≤2.5 μm in aerodynamic diameter (PM2.5), and 0.44 (0.4–0.84) μg/m3 for carbon monoxide (CO).
Patients were divided into two groups based on the severity of the disease; patients with rhinoconjunctivitis symptom scores <9 were classified as low-moderate severity group, while patients with scores ≥9 were classified as high-severity group. The OR and 95% Confidence Intervals (95% CI) were estimated by using a multi-variable Logistic Regression model to evaluate the association between pollen exposure, air pollution exposure and the severity of NAR. The distributed lag nonlinear model (DLNM)16 was used to assess the single-day (lag0-lag14) and accumulative (lag0-1, lag0-2, —-lag0-14) lag effects of pollen and ambient air pollutants during the pollen seasons.
To further understand whether the effects of pollen on the severity of NAR could be modified by air pollutants, a stratified analysis was performed based on the different levels of air pollutant exposure. The cut-off concentrations to classify the low and high exposure levels of PM10, PM2.5, SO2, NO2 and O3 were 50, 35, 50, 80, and 100 μg/m3, respectively, according to the primary standards of the national air quality standards (GB3095-2012) of China. All data analyzed in this study were performed by using packages “MASS”,17 “dlnm”,16 “tsModel”18 based on R 4.1.0.
Results
Demographic and Clinical Information of the Study Population
The demographic information of the study population is shown in Table 1. In total, the current study included 2411 NAR patients, with sufficient data on demographic and clinical data. Participants were on an average 34.74 years old, of which 45.58% were women, and 4.1% had asthma. The average TNSS and Rhinoconjunctivitis symptom scores were 8.56 and 10.03, respectively. In the higher severity category, participants were younger, but the asthma comorbidity was comparable.
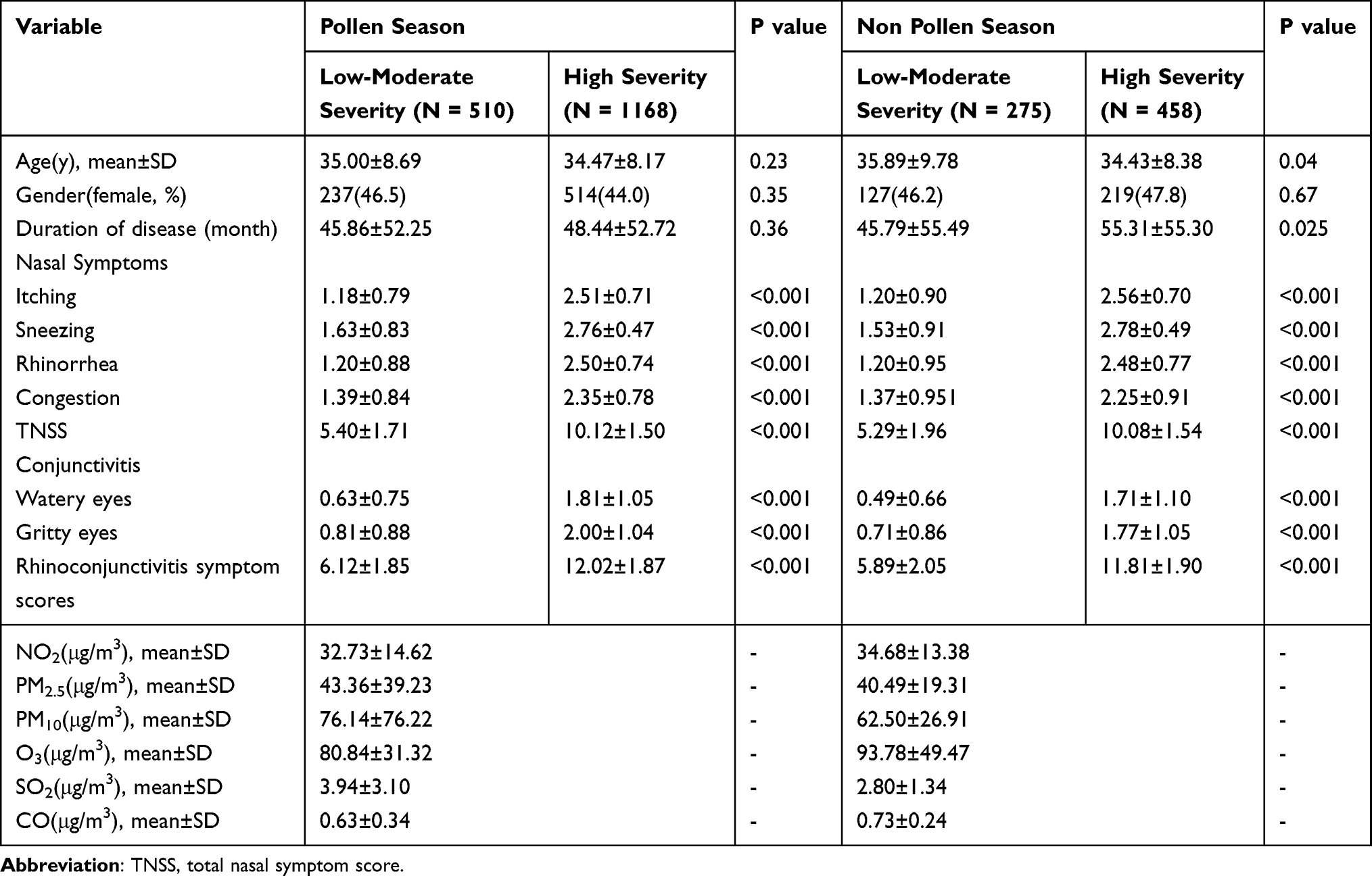 |
Table 1 Characteristics of the Participants by Levels of Severity in NAR Patients |
During the pollen season, the age and gender distribution, as well as the duration of disease were comparable between the two severity groups. Nevertheless, in non-pollen seasons, patients in the high severity group were younger and had a longer period of disease than the low-moderate severity group; gender distribution remained indistinguishable.
Associations Between Pollen Concentration, Air Pollutants and Severity of NAR
As shown in Figure 1, within pollen seasons, the IQR was higher in the concentration of pollen and air pollutants, and the OR (95% CI) of rhinoconjunctivitis symptom scores, when compared with the low-moderate severity group, were as follows: 1.172 (1.072~1.295) for pollen, 1.101 (1.012~1.213) for PM10, 1.125 (1.008~1.260) for PM2.5, 1.283 (1.123~1.471) for NO2 and 1.198 (1.077~1.339) for SO2. The low-moderate group was more susceptible to the exposure of O3 (OR = 0.828 [0.711 ~ 1.339]; P = 0.014). However, no statistically significant association was found in air pollutant metrics, pollen concentration, and the severity of disease during the non-pollen seasons.
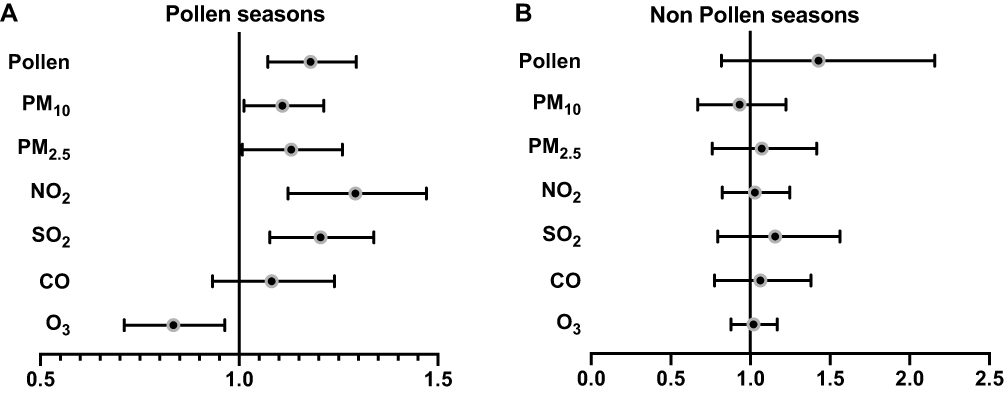 |
Figure 1 Associations between air pollutant metrics and levels of severity score of NAR, within pollen seasons (A) and non-pollen seasons (B). |
Lag Effect of Pollen and Ambient Air Pollutant During Pollen Seasons
Subsequently, we analyzed the single-day and accumulative lag effects of pollen and ambient air pollutants during pollen seasons (Figure 2). Pollen exposure has shown profound effects on the rhinoconjunctivitis symptoms in NAR patients. During the pollen seasons, effects even lasted for 14 days. For PM10, the first-day effect was the most significant and the lag effects remained positive until day 3; for PM2.5, the most significant effect also appeared on day 1, and the overall lag effects sustained 6 days. Lag effects for NO2 lasted 14 days, with relatively higher effects on the first 6 days, which slowly went down afterward. The effect of SO2 slowly went higher with an increasing lag from 1 to 5 days, and thereafter it decreased from 6 to 14 days. The 3-dimensional graph demonstrates the exposure–outcome relationship for ambient pollen and pollution from lag day 1 to day 14 (Figure 3).
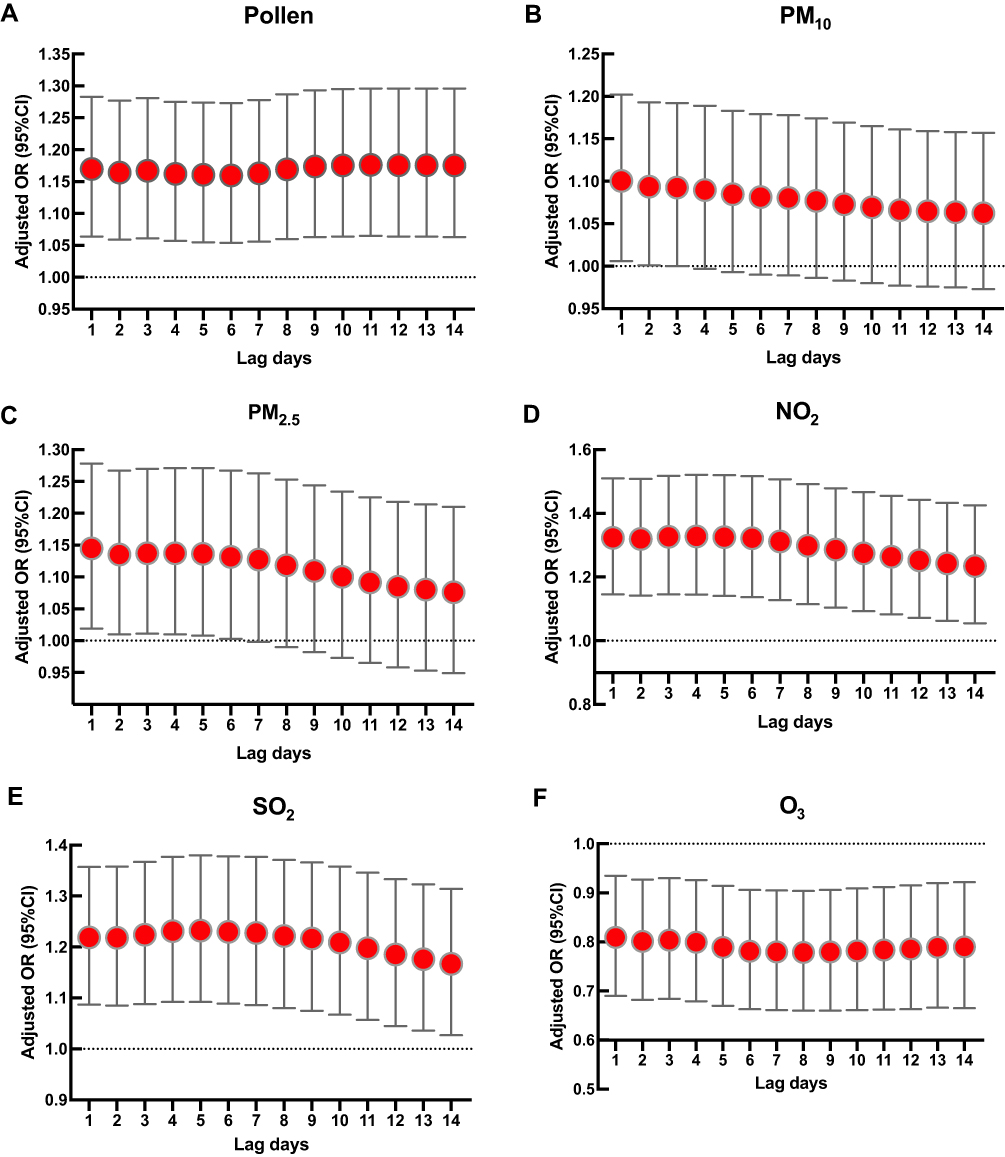 |
Figure 2 The lag effect of pollen (A) and ambient air pollutants including PM10 (B), PM2.5 (C), NO2 (D), SO2 (E) and O3 (F) during pollen seasons on the severity of NAR patients. |
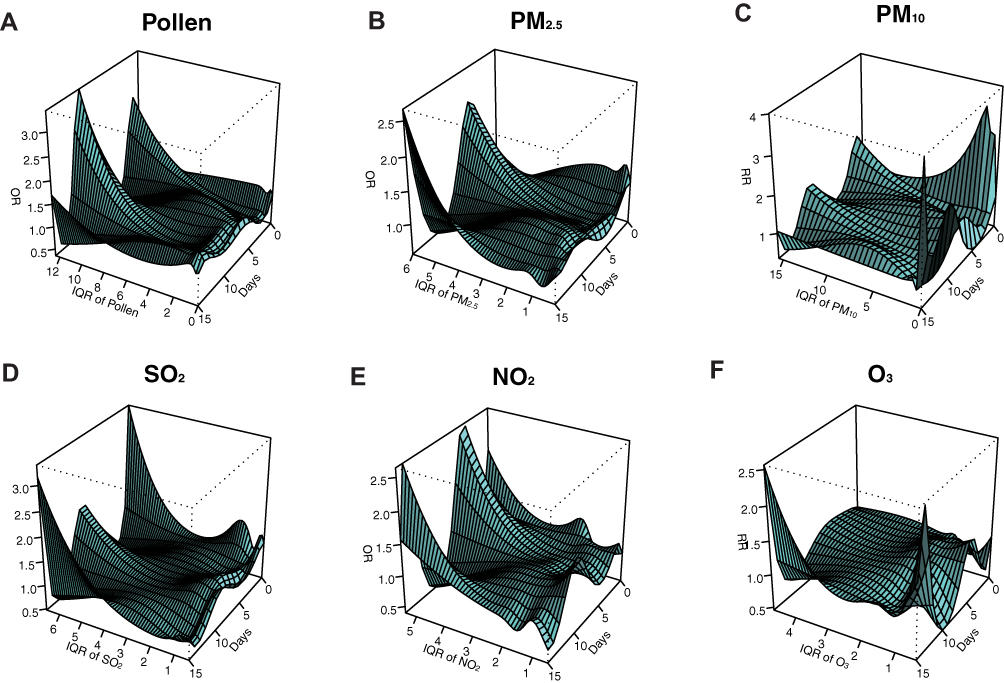 |
Figure 3 The 3-dimensional graph demonstrates the exposure–outcome relationship for ambient pollen (A) and pollution including PM10 (B), PM2.5 (C), NO2 (D), SO2 (E) and O3 (F) from lag day 0 to day 14. |
Stratification of Ambient Pollutants
To further analyze the effect of pollen severity at different concentrations of air pollutants, a stratification of ambient pollutants was performed according to the primary standards of the national air quality standards (GB3095-2012) of China (Figure 4). In the current study, stratification of SO2 was not performed because the concentration was too narrow for stratification. For PM10 and PM2.5, significant pollen-severity effects and profound lag effects could be found when undergoing high-level of exposure but not low-level of exposure. During low-level exposure of NO2 and O3, significant pollen-severity effects and lag effects could be seen; while under high exposure, the effects were indistinguishable between the low-moderate and high severity groups.
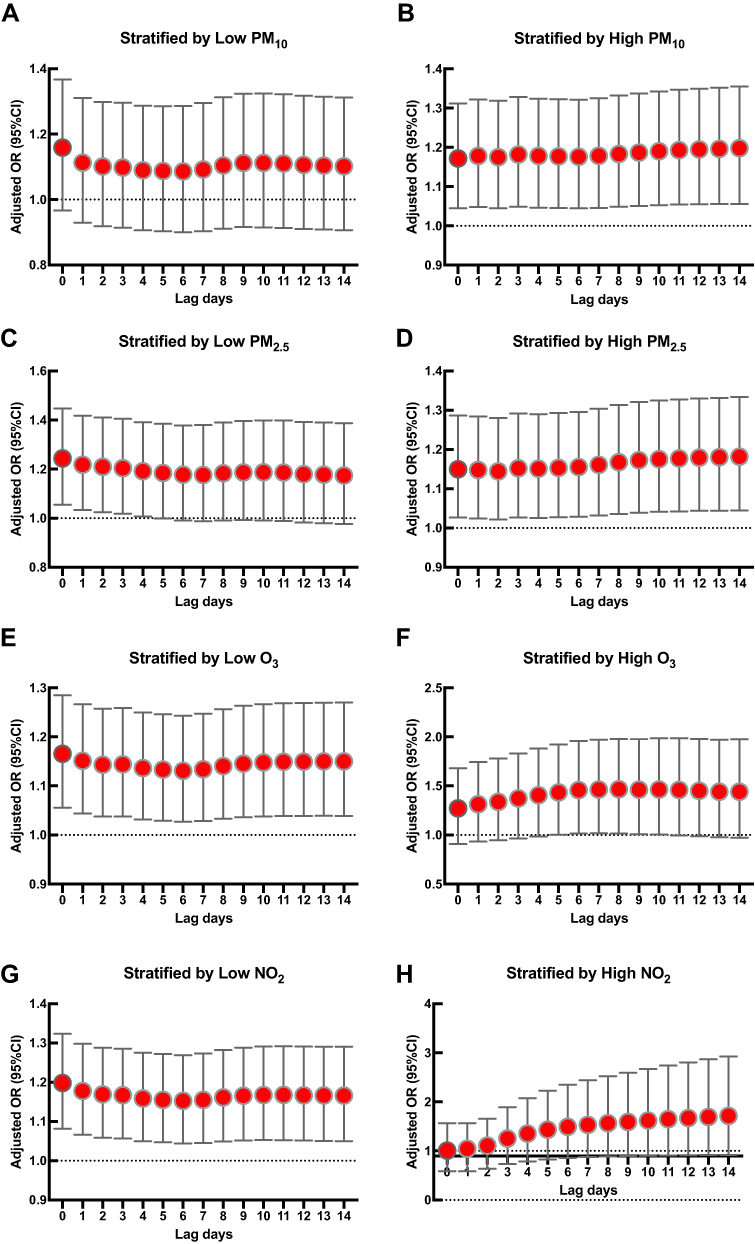 |
Figure 4 The lag effect of pollen during pollen seasons on the severity of NAR. patients when major ambient pollutants ((A and B), PM10; (C and D), PM2.5; (E and F), O3; (G and H), NO2) were stratified. |
Discussion
For a long time, NAR has been hugely underestimated and underrated since the diagnosis of the disease lacks direct objective tests and is mainly dependent on clinical manifestations and exclusion of positive allergen tests.19 Studies that focused on objective tests in NAR population were limited. The current study is the first real-world study assessing the association of ambient pollen, pollution and severity of the disease.
China is a country with a large number of chronic rhinitis patients. In recent years, chronic rhinitis is emergingly considered an umbrella disease with homogeneous nasal symptoms but with differentiating etiological features.20 It is estimated that the prevalence of NAR varied from 17% to 52% worldwide.4–7 One recent study in northern China reported that confirmed standardized prevalence of NAR was 24.60% with help of skin prick test, while the confirmed standardized prevalence of AR was 16.78%.8 Therefore, the population of NAR patients is much larger than those with AR, although AR is usually considered a more severe disease than NAR. In our previous study, we were intrigued by the finding that the severity of disease in NAR patients was significantly higher during pollen seasons than in other seasons. In the current study, we compared the effects of both pollen and major air pollutants during pollen and non-pollen seasons on the NAR disease severity. We found that in pollen seasons, high pollen concentration alongside high air pollution showed a synergistic effect on the severity of NAR, which might be the reason why NAR patients suffered worse during pollen seasons.
With the development of industrialization, various forms of air pollutants have increased in developing countries. Power generation and traffic have always been major sources of air pollution, which are estimated to contribute towards 3% of the disability-adjusted life years lost globally.21 There is emerging evidence of the detrimental effects of air pollution, such as asthma, allergic rhinitis, chronic obstructive lung disease, cardiovascular diseases, tumors, immune dysfunction, and even mental disorders.13,22–24 In the current study, we included 6 most common air pollutants, PM2.5, PM10, SO2, NO2, CO and O3, among which, PM2.5 and PM10 were the best-studied forms of air pollutants. PMs are classified by fractions based on their size; smaller PMs such as PM2.5 and ultra-fine particulate matter could easily reach the lower airway and lungs, while larger particles mostly affect the upper airway.24 It has been proven that air pollution has a huge effect on airway epithelium. A recent genome-wide analysis revealed that the stimulation of organic PM2.5 extract activated IL-1 inflammatory pathway, increased mucus secretion and induced airway remodeling in human nasal mucociliary airway epithelial cultures.25 Xian et al investigated the effects of PM2.5 in nasal mucosal tissue using an air–liquid interface culture and found that it led to an epithelial barrier integrity deficiency.26 A retrospective cross-sectional study in Shanghai reported that exposure to NO2 and PM10 were significantly and positively associated with airway symptoms in 13,335 preschoolers.27 Apart from PMs, oxidizing gases such as NO2 and O3, are also substantial causes of airway diseases. In our study, we found significant pollen-severity effects and profound lag effects even under low exposure of NO2 and O3, indicating that these two pollutants should be strictly controlled, especially in pollen season. Li et al reported that black carbon and pollen were associated with oxidative stress in the nasal mucosa and the combination of these two could even aggregate the inflammation.28 In fact, NO2 is a relatively weak oxidant, while O3 is a strong oxidant. In mice and rat models, ozone induced nasal type 2 immunity and aggravated eosinophilic inflammation.29,30 In our study, we found that even with low exposure to O3, high symptoms already appeared in NAR patients, indicating that it was a relatively strong symptom inducer.
To date, little is known about the association between air pollutants and the severity of chronic rhinosinusitis, especially NAR. In 2002, a time-series analysis that included 16 NAR patients and healthy volunteers found that O3 and NO were associated with nasal symptoms.31 In the current study, we found that air pollutants were significantly associated with the severity of NAR. Consistently, a European cross-sectional study showed that the air pollutants-severity effect was higher in NAR than in AR patients.32
Additionally, little is known about the association between pollen concentration and the severity of NAR. Our study implied that pollen, a specific stimulus of patients with allergic diseases such as AR and allergic asthma, is also a strong stimulus to NAR patients. Nonspecific nasal hyperreactivity, a nasal abnormal overactivated reaction towards stimuli, was first considered to be the most prominent and unique characteristic of NAR.12 Later, a study found that nasal hyperreactivity evaluated by cold dry air stimulation test was comparable between AR patients and NAR patients.33 For NAR patients, pollen could also induce nasal hyperreactivity, leading to significant nasal symptoms. Moreover, pollen could induce nasal inflammation by being the vector for some strong immunologic and inflammatory effectors. A recent study reported that Artemisia pollen is responsible for airborne endotoxin dispersion, which is capable of inducing airway inflammation.34 Artemisia annua happens to be the most common and important autumnal pollen allergen in northern China.35
However, the current study has some limitations. First, as a retrospective real-world study, only the first-visit clinically diagnosed NAR patients were included in our study. The whole population might be limited by national holidays and the hospital appointment system. Second, as a cross-sectional study, the long-term exposure effects in the same population were unable to be evaluated. Thus, large-scale, prospective studies, and mechanism studies, are needed to further improve the understanding of the synergistic effects of pollen and air pollution. Third, as a real-world study, no nasal provocation test was applied in this study; thus, there might be some local AR patients included into the enrolled subjects.
Conclusion
In summary, this study has provided preliminary information on the synergistic effect of pollen and air pollutants, including PM2.5, PM10, SO2, NO2, and O3, in aggravating symptoms in NAR patients. These results bring us new insights into the management of NAR. Therefore, it is essential to protect NAR patients from pollen, especially during the pollen seasons. Finally, the findings also contribute to understanding the environmental stimuli that directly influence the severity of NAR and thus reemphasize that air pollution needs to be better controlled.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Program for Changjiang Scholars and Innovative Research Team (IRT13082); National Key R&D Program of China (2016YFC20160905200), National Natural Science Foundation of China (81630023 and 82071022), and Beijing Talents Foundation (2018000021223ZK14).
Disclosure
All authors declare that they have no conflict of interest.
References
1. Meng Y, Lou H, Wang Y, et al. Endotypes of chronic rhinitis: a cluster analysis study. Allergy. 2019;74(4):720–730. doi:10.1111/all.13640
2. Bousquet J, Schunemann HJ, Samolinski B, et al. Allergic Rhinitis and its Impact on Asthma (ARIA): achievements in 10 years and future needs. J Allergy Clin Immunol. 2012;130(5):1049–1062. doi:10.1016/j.jaci.2012.07.053
3. Brożek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J Allergy Clin Immunol. 2017;140(4):950. doi:10.1016/j.jaci.2017.03.050
4. Bachert C, van Cauwenberge P, Olbrecht J, van Schoor J. Prevalence, classification and perception of allergic and nonallergic rhinitis in Belgium. Allergy. 2006;61(6):693–698. doi:10.1111/j.1398-9995.2006.01054.x
5. Chiang WC, Chen YM, Tan HK, et al. Allergic rhinitis and non-allergic rhinitis in children in the tropics: prevalence and risk associations. Pediatr Pulmonol. 2012;47(10):1026–1033. doi:10.1002/ppul.22554
6. Bernstein JA, Singh U. Neural abnormalities in nonallergic rhinitis. Curr Allergy Asthma Rep. 2015;15(4):18. doi:10.1007/s11882-015-0511-7
7. Hellings PW, Klimek L, Cingi C, et al. Non-allergic rhinitis: position paper of the European Academy of allergy and clinical immunology. Allergy. 2017;72(11):1657–1665. doi:10.1111/all.13200
8. Huang Y, Zhang Y, Zhang L. Prevalence of allergic and nonallergic rhinitis in a rural area of northern China based on sensitization to specific aeroallergens. Allergy Asthma Clin Immunol. 2018;14:77. doi:10.1186/s13223-018-0299-9
9. Huang Y, Wang C, Zhang Y, Zhang L. Developing nomograms for identifying allergic rhinitis among chronic rhinitis: a real-world study. World Allergy Organ J. 2021;14(4):100534. doi:10.1016/j.waojou.2021.100534
10. Segboer CL, Terreehorst I, Gevorgyan A, Hellings PW, van Drunen CM, Fokkens WJ. Quality of life is significantly impaired in nonallergic rhinitis patients. Allergy. 2018;73(5):1094–1100. doi:10.1111/all.13356
11. Hoshino T, Hoshino A, Nishino J. Relationship between environment factors and the number of outpatient visits at a clinic for nonallergic rhinitis in Japan, extracted from electronic medical records. Eur J Med Res. 2015;20:60. doi:10.1186/s40001-015-0151-3
12. Bonini S, Rasi G, Brusasco V, et al. Nonspecific provocation of target organs in allergic diseases: EAACI-GA(2)LEN consensus report. Allergy. 2007;62(6):683–694. doi:10.1111/j.1398-9995.2007.01382.x
13. Eguiluz-Gracia I, Mathioudakis AG, Bartel S, et al. The need for clean air: the way air pollution and climate change affect allergic rhinitis and asthma. Allergy. 2020;75(9):2170–2184. doi:10.1111/all.14177
14. Qing H, Wang X, Zhang N, et al. The effect of fine particulate matter on the inflammatory responses in human upper Airway Mucosa. Am J Respir Crit Care Med. 2019;200(10):1315–1318. doi:10.1164/rccm.201903-0635LE
15. Celebi Sozener Z, Cevhertas L, Nadeau K, Akdis M, Akdis CA. Environmental factors in epithelial barrier dysfunction. J Allergy Clin Immunol. 2020;145(6):1517–1528. doi:10.1016/j.jaci.2020.04.024
16. Gasparrini A. Distributed lag linear and non-linear models in R: the package dlnm. J Stat Softw. 2011;43(8):1–20. doi:10.18637/jss.v043.i08
17. Venables W, Ripley B. Modern Applied Statistics with S.
18. Peng R. tsModel: time series modeling for air pollution and health. Available from: https://CRAN.R-project.org/package=tsModel.
19. Greiwe J, Bernstein JA. Nonallergic Rhinitis: diagnosis. Immunol Allergy Clin North Am. 2016;36(2):289–303. doi:10.1016/j.iac.2015.12.006
20. Mullol J, Del Cuvillo A, Lockey RF. Rhinitis Phenotypes. J Allergy Clin Immunol Pract. 2020;8(5):1492–1503. doi:10.1016/j.jaip.2020.02.004
21. Guarnieri M, Balmes JR. Outdoor air pollution and asthma. Lancet. 2014;383(9928):1581–1592. doi:10.1016/S0140-6736(14)60617-6
22. Buoli M, Grassi S, Caldiroli A, et al. Is there a link between air pollution and mental disorders? Environ Int. 2018;118:154–168. doi:10.1016/j.envint.2018.05.044
23. Landrigan PJ, Fuller R, Acosta NJR, et al. The lancet commission on pollution and health. Lancet. 2018;391(10119):462–512. doi:10.1016/S0140-6736(17)32345-0
24. Glencross DA, Ho TR, Camina N, Hawrylowicz CM, Pfeffer PE. Air pollution and its effects on the immune system. Free Radic Biol Med. 2020;151:56–68. doi:10.1016/j.freeradbiomed.2020.01.179
25. Montgomery MT, Sajuthi SP, Cho SH, et al. Genome-wide analysis reveals mucociliary remodeling of the Nasal Airway Epithelium Induced by Urban PM2.5. Am J Respir Cell Mol Biol. 2020;63(2):172–184. doi:10.1165/rcmb.2019-0454OC
26. Xian M, Ma S, Wang K, et al. Particulate matter 2.5 causes deficiency in barrier integrity in human Nasal Epithelial Cells. Allergy Asthma Immunol Res. 2020;12(1):56–71. doi:10.4168/aair.2020.12.1.56
27. Liu W, Cai J, Fu Q, et al. Associations of ambient air pollutants with airway and allergic symptoms in 13,335 preschoolers in Shanghai, China. Chemosphere. 2020;252:126600. doi:10.1016/j.chemosphere.2020.126600
28. Li Y, Ouyang Y, Jiao J, Xu Z, Zhang L. Exposure to environmental black carbon exacerbates nasal epithelial inflammation via the reactive oxygen species (ROS)-nucleotide-binding, oligomerization domain-like receptor family, pyrin domain containing 3 (NLRP3)-caspase-1-interleukin 1beta (IL-1beta) pathway. Int Forum Allergy Rhinol. 2021;11(4):773–783. doi:10.1002/alr.22669
29. Kumagai K, Lewandowski R, Jackson-Humbles DN, et al. Ozone-induced nasal type 2 immunity in mice is dependent on innate lymphoid cells. Am J Respir Cell Mol Biol. 2016;54(6):782–791. doi:10.1165/rcmb.2015-0118OC
30. Sun N, Niu Y, Zhang R, et al. Ozone inhalation induces exacerbation of eosinophilic airway inflammation and Th2-skew immune response in a rat model of AR. Biomed Pharmacother. 2021;137:111261. doi:10.1016/j.biopha.2021.111261
31. Braat JP, Mulder PG, Duivenvoorden HJ, Gerth Van Wijk R, Rijntjes E, Fokkens WJ. Pollutional and meteorological factors are closely related to complaints of non-allergic, non-infectious perennial rhinitis patients: a time series model. Clin Exp Allergy. 2002;32(5):690–697. doi:10.1046/j.1365-2222.2002.01359.x
32. Burte E, Leynaert B, Marcon A, et al. Long-term air pollution exposure is associated with increased severity of rhinitis in 2 European cohorts. J Allergy Clin Immunol. 2020;145(3):834–842e6. doi:10.1016/j.jaci.2019.11.040
33. Segboer CL, Holland CT, Reinartz SM, et al. Nasal hyper-reactivity is a common feature in both allergic and nonallergic rhinitis. Allergy. 2013;68(11):1427–1434. doi:10.1111/all.12255
34. Oteros J, Bartusel E, Alessandrini F, et al. Artemisia pollen is the main vector for airborne endotoxin. J Allergy Clin Immunol. 2019;143(1):369–377 e5. doi:10.1016/j.jaci.2018.05.040
35. Lou H, Huang Y, Ouyang Y, et al. Artemisia annua-sublingual immunotherapy for seasonal allergic rhinitis: a randomized controlled trial. Allergy. 2020;75(8):2026–2036. doi:10.1111/all.14218
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.