")
Back to Journals » Cancer Management and Research » Volume 9
Impact of abiraterone on patient-related outcomes in metastatic castration-resistant prostate cancer: current perspectives
Authors El-Amm J, Nassabein R , Aragon-Ching JB
Received 10 April 2017
Accepted for publication 30 May 2017
Published 11 July 2017 Volume 2017:9 Pages 299—306
DOI https://doi.org/10.2147/CMAR.S139305
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Joelle El-Amm,1 Rami Nassabein,1 Jeanny B Aragon-Ching2
1Division of Hematology and Oncology, Department of Internal Medicine, Lebanese American University, Beirut, Lebanon; 2GU Medical Oncology, Inova Schar Cancer Institute, Fairfax, VA, USA
Abstract: Abiraterone acetate has established a major role in the treatment paradigm of metastatic castration-resistant prostate cancer ever since pivotal trials, COU-AA-301 and COU-AA-302, have shown benefit in both the second-line and first-line (post- and pre-chemotherapy) setting, respectively, with improvement in overall survival as well as secondary end points such as prostate-specific antigen (PSA) and radiographic response rates, time to PSA progression, and progression-free survival. There has been a lot of interest and emphasis in the evaluation of patient-related outcomes (PROs) as it relates to quality of life, pain, adverse events, fatigue, and among others, in the use of different agents that have been shown to improve survival. This review examines the companion PROs in conjunction with abiraterone acetate use. This is particularly relevant since PROs are increasingly viewed as a key metric for drug label claims in granting approval across regulatory agencies, including the US Food and Drug Administration and the European Medicines Agency.
Keywords: abiraterone acetate, metastatic castration-resistant prostate cancer, patient-related outcomes, androgen signaling agents
Introduction
Androgen signaling plays a pivotal role in the proliferation of prostate cancer and androgen deprivation therapy (ADT) in the form of either surgical castration or chemical castration through the use of luteinizing hormone releasing hormone (LHRH) agonists or antagonists, which is the mainstay of therapy in metastatic prostate cancer.1–3 ADT elicits a response in majority of patients with metastatic disease. However, resistance develops inevitably leading to metastatic castration-resistant prostate cancer (mCRPC) defined as progression of disease, despite a drop in testosterone level to below 50 ng/dL and recently updated to less than 20 ng/dL.4,5 Progression of disease in patients with mCRPC can lead to development of worsening symptoms and patients may experience decline in their health-related quality of life (HRQoL) with ensuing increased pain.6–8
Prior to 2004, there were few agents available for the treatment of mCRPC and most were used for palliation alone. These included the radiopharmaceuticals samarium and strontium and the chemotherapy mitoxantrone and were US Food and Drug Administration (FDA) approved for their pain palliation properties. Docetaxel became the standard first-line chemotherapy in mCRPC in 2004 based on the two trials SWOG 9916 and TAX-327 that showed survival benefit compared to mitoxantrone.9–11 Although docetaxel and mitoxantrone yielded similar rates of pain relief, there was a notable improvement in the quality of life in patients treated with docetaxel, beyond the improvement in overall survival (OS) alone. Since 2010, the treatment landscape of mCRPC was completely revolutionized with the approval of the first vaccine (sipuleucel-T), drugs targeting the androgen receptor (AR) (enzalutamide and abiraterone), radiopharmaceuticals (radium-223 dichloride), and the cytotoxic drug cabazitaxel, although the majority of these studies evaluated survival as the primary end point and only about 18% analyzed patient-related outcomes (PROs) in their studies.12 It is clear that these newer agents offer not only survival benefits but also improvements in quality of life and pain mitigation.13
mCRPC remains driven by the androgen axis, and despite the use of ADT, almost all men with metastatic prostate cancer can progress to develop castration resistance, which still depends on androgen synthesis and AR signaling for proliferation. In addition, increased intratumoral production of androgens is also thought to result from upregulation of androgen biosynthesis enzymes. Androgens are synthesized from cholesterol through a multistep process using several enzymes, one of which is CYP17A1 which has both a 17 hydroxylase and a 17,20 lyase activity.14,15 CYP17A1 is a key enzyme implicated in the pathogenesis of prostate cancer by sequentially catalyzing the conversion of pregnenolone and progesterone to 17α hydroxypregnenolone and 17α hydroxyprogesterone, which are then converted to dehydroepiandrosterone (DHEA) and androstenedione, respectively. Both DHEA and androstenedione, are eventually transformed into testosterone and dihydroxytestosterone (DHT), the most potent androgen. Abiraterone acetate is a prodrug of abiraterone, which is a selective irreversible steroidal competitive inhibitor of CYP17A1, the critical enzyme in the abovementioned androgen biosynthesis pathway, hence blocking additional intratumoral production of androgens as well as that in the adrenal glands and the testes.16,17 Since abiraterone is an oral nonchemotherapy agent, it has the potential for improving the quality of life while avoiding the toxic side effects of chemotherapy.
The approval of the new agents in mCRPC was mainly based on their survival benefit. Although OS is the gold standard for showing clinical benefit in prostate cancer clinical trials, HRQoL is increasingly being considered as an important end point of value to patients and health care providers. Quality of life is a complex measure that encompasses physical, social, and emotional well-being.
The US FDA defines a PRO as “any report of the status of a patient’s health condition that comes directly from the patient, without interpretation of the patient’s response by a clinician or anyone else”. The instruments used to assess PRO include information about HRQoL, self-satisfaction with symptoms, compliance with therapy, and perceived value of treatment.18,19 In addition, the PRO claims are important in granting approval across varying agencies such as the US FDA and the European counterpart of the European Medicines Agency (EMA).20 However, the challenge remains in standardizing these methods of qualifying PROs and quantifying and reporting of patients with mCRPC to have a meaningful interpretation in the clinic.13 For instance, the typical use of HRQoL instruments seen in the mCRPC trials was not intended solely for a metastatic prostate cancer population and such relevant issues may not be adequately represented in the questionnaires.
Impact of abiraterone on PROs in clinical trials
The most widely used questionnaires for assessment of PROs are the Functional Assessment of Cancer Therapy-Prostate (FACT-P) questionnaire and the Brief Pain Inventory Short Form (BPI-SF). The FACT-P questionnaire is a validated questionnaire comprising a general function status scale (FACT-G, consisting of four subscales: physical, social/family, emotional, and functional well-being) and a prostate cancer-specific (PCS) subscale that assesses PCS symptoms. The trial outcome index (TOI) represents a composite of the scores on the physical well-being, functional well-being, and PCS scales.21–25 These were considered as secondary outcomes in both the COU-AA-301, the second-line chemotherapy trial, as well as in the COU-AA-302, the first-line chemotherapy trials (Table 1).
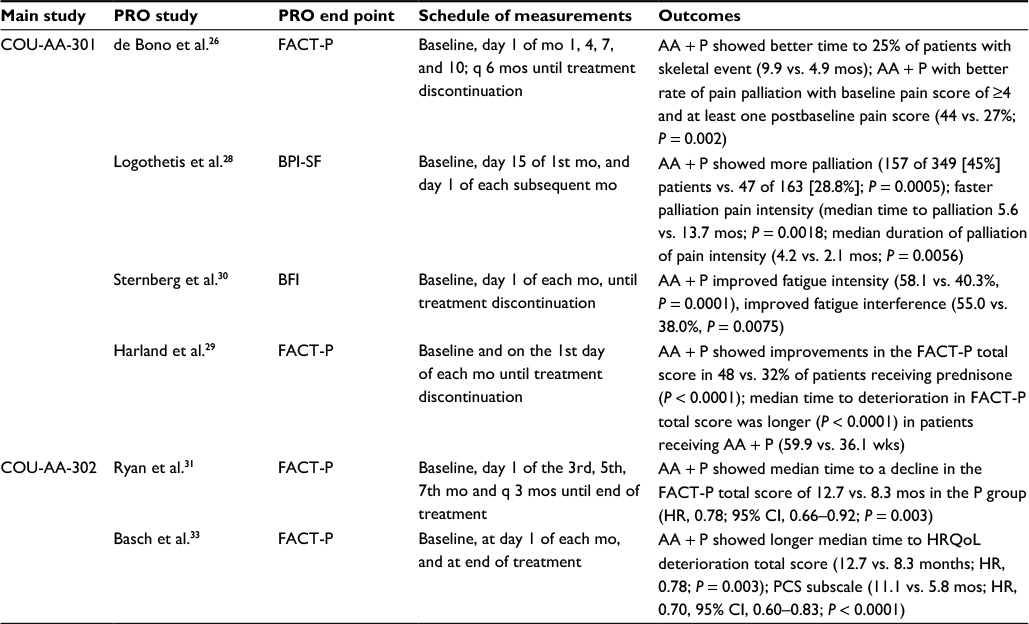 | Table 1 Studies with PROs using abiraterone acetate Note: All comparisons AA + P vs. P alone. Abbreviations: PROs, patient-related outcomes; FACT-P, Functional Assessment of Cancer Therapy-Prostate; mo, month; AA + P, abiraterone acetate + prednisone; BPI-SF, Brief Pain Inventory Short Form; BFI, Brief Fatigue Inventory; P, prednisone; HRQoL, health-related quality of life; HR, hazard ratio; CI, confidence interval; PCS, prostate cancer-specific; q, every. |
The COU-AA-301 (post-chemotherapy) trial
The COU-AA-301 trial included 1,195 patients with mCRPC who progressed on one or more chemotherapy regimens including docetaxel.26,27 Patients who had an Eastern Cooperation Oncology Group performance score of 0 to 2 were randomized in a 2:1 ratio to receive either prednisone and abiraterone or prednisone alone. The primary end point of the study was OS.
The characteristics of the patients in both groups regarding the baseline pain scores were similar. Baseline pain intensity and pain interference with daily activity were assessed according to the BPI-SF. The majority of patients (89%) had bone metastasis at baseline with a mean baseline analgesic score of 1.2 in the abiraterone group and 1.3 in the placebo group (0 for no analgesic use to 3 for opioids use). The patients who were enrolled in the COU-AA-301 trial were considered mildly symptomatic for pain based on a median BPI-SF score of 3 (range 0–10, with a higher score indicating increased pain severity in the last 24 hours).
The trial measured palliation of worst pain in those with clinically significant worst pain at baseline (score above 4 on the BPI-SF question 3).28 Worst pain intensity palliation was defined as two consecutive follow-up visits (≥4 weeks apart) at which the worst pain intensity score was ≥30% lower than that at baseline without an increase in analgesic use, whereas pain interference palliation was defined as a decrease in mean pain interference score of ≥1.25 points compared with baseline at two consecutive follow-up visits. Median time to palliation in worst pain intensity (5.6 vs. 13.7 months; hazard ratio [HR], 1.68; 95% confidence interval [CI], 1.20–2.34; P = 0.0018) and interference (1.06 vs. 3.7 months; HR, 1.89; 95% CI, 1.31–2.74; P = 0.0004) was shorter in the abiraterone than placebo arm. A total of 157 (45%) patients in the abiraterone group vs. 47 (28.8%) patients in the placebo group had improvement in pain intensity, P = 0.0005. The rate of palliation among patients with a baseline pain score of 4 or more and at least one postbaseline pain score favored patients on abiraterone compared with placebo (44% vs. 27%, P = 0.002). A total of 134 of 223 patients (60.1%) vs. 38 of 100 (38.0%) had palliation of pain interference with daily activity in the abiraterone and placebo groups, respectively, P = 0.0002. Median duration of pain improvement was also significant favoring the abiraterone group at 4.2 vs. 2.1 months for the placebo group, P = 0.005. Median time to skeletal events development was 25 vs. 20.3 months for the abiraterone and placebo group, respectively; HR, 0.615, P = 0.0001. Patients with a baseline BPI level of less than 4 (no clinically significant pain) had an OS of 16.2 and 13.0 months for abiraterone compared with placebo, respectively (HR, 0.64; 95% CI, 0.50–0.82); patients with a baseline BPI of 4 or more (clinically significant pain) had an OS of 12.6 and 8.9 months, respectively (HR, 0.68; 95% CI, 0.53–0.85).
In addition to assessment of pain, patients in the COU-AA-301 trial were assessed for HRQoL using the FACT-P questionnaire during cycles 1, 4, 7, and 10 then every 6 cycles.29 Baseline subscales were equal in both groups. Enrolled patients had mean baseline FACT-P total scores of 108 (with the trial considering a maximum possible FACT-P score of 156), indicating a moderate level of HRQoL impairment. Abiraterone showed improvement in quality of life compared to placebo, 48.1 vs. 31.9%; P < 0.0001. This significant difference was shown in all subscales of quality of life assessment including: physical well-being (46.6 vs. 28.5%; P < 0.0001), emotional well-being (55.8 vs. 38.7%; P = 0.0241), and functional well-being (44.6 vs. 33.7%; P = 0.0047) except for social and family well-being (57.5 vs. 49.2%; P = 0.1134). As far as deterioration in the quality of life, abiraterone was found to delay the median FACT-P score deterioration of 419 days when compared to placebo of 253 days; HR, 0.6, P < 0.0001. However, similar to the difference observed in subscales of quality of life assessment, the duration of delay was not significantly different between both groups for social and family well-being. It is hypothesized that social and family well-being is a scale that is not affected by the study drug, instead it is dependent on social and family support and interpersonal relations in the surrounding environment or society.
Patients enrolled in the COU-AA-301 trial were also studied for fatigue progression or improvement during treatment.30 Fatigue was assessed and recorded using the Brief Fatigue Inventory (BFI) questionnaire before enrollment and on the first day of each cycle. Baseline fatigue scores were similar between the two groups. A greater percentage of patients in the abiraterone arm showed improvement in their fatigue intensity (58 vs. 40%; P = 0.0001). The median time to improvement in fatigue intensity (59 vs. 194 days; P = 0.0155) was less in the abiraterone arm. Similar results were obtained when comparing fatigue interference of daily activity; 55% in the abiraterone group vs. 38% in the placebo group P = 0.0075. Abiraterone delays time to symptomatic deterioration or progression in the fatigue intensity with a median of 232 days which is about 93 days delay when compared to placebo’s median time to progression, P = 0.005. Fatigue interference progression occurred in 22 and 25% of abiraterone and placebo group, respectively, and time to progression (25th percentile) was 281 days in the abiraterone group and 139 days for the placebo group P = 0.0008. This suggests that abiraterone acetate with prednisone could further improve patients’ report of fatigue, despite failure on prior docetaxel, and reflect an important measure of PRO in patients taking oral abiraterone.
The COU-AA-302 trial (pre-chemotherapy)
The COU-AA-302 trial was a Phase III, multinational, randomized, double-blind study that enrolled asymptomatic (score of 0 or 1 on item 3 of the BPI-SF questionnaire) or mildly symptomatic (score of 2 or 3 on BPI-SF item 3), chemotherapy-naive patients with progressive mCRPC.31,32 A total of 1,088 patients were randomly assigned 1:1 to receive either abiraterone acetate 1 g daily plus prednisone 5 mg twice daily (n = 546) or placebo plus prednisone 5 mg twice daily (n = 542). The primary end point of the trial was both radiographic progression-free survival and OS. While the initial iteration of the trial showed statistically significant radiographic progression-free survival in favor of abiraterone with prednisone, the OS did not initially cross the prespecified efficacy boundary, but it was later shown to be statistically significant in subsequent updated analyses.32 Patient-reported pain and functional status were examined as part of the secondary end points of this trial.33 Pain was recorded using the BPI-SF questionnaire at each cycle and at the end of treatment. HRQoL was assessed using FACT-P questionnaire. Closer scrutiny shows that patients had an overall better quality of life compared to the COU-AA-301 population with better FACT-P total scores averaging around 122. At baseline, 69% of patients in the abiraterone group and 65% of placebo group were asymptomatic, and many of the patients enrolled did not use analgesics. Using data from the second interim analysis, with a median follow-up of 22.2 months, the median time to progression of mean pain intensity (increase by 30% from baseline) was 26.7 vs. 18.4 months for abiraterone and placebo, respectively (HR, 0.82; P = 0.049). The median time to progression of worst pain intensity was 26.7 months for the abiraterone group vs. 19.4 months for the placebo group (HR, 0.85; P = 0.109). Looking at the median time to functional status deterioration according to FACT-P (decrease of three points from baseline), it was 12.7 vs. 8.3 months for the abiraterone group and placebo group, respectively (HR, 0.78; P = 0.003). P value was significant on comparison of both groups using several scales: prostate cancer-specific subscale, general function subscale, physical well-being, functional, and emotional well-being. Therefore, in this trial, the time to progression to worst pain and initiation of cytotoxic chemotherapy was similar in both groups, and the benefit was evident in clinical pain improvement and quality of life. In addition, a consistent pattern in the delay of pain progression as well as pain interference was seen with abiraterone use (P = 0.005) compared to prednisone,13 although the mean pain intensity approached but was short of statistically significant in favor of abiraterone with prednisone (P = 0.061).34
A post hoc analysis of COU-AA-302 trial was designed to investigate the effect of bone-targeted therapy (bisphosphonates or denosumab).35 This third interim analysis of the study confirmed that treatment with abiraterone had improved radiographic progression-free survival significantly (HR, 0.52; P < 0.0001). While bone-targeted therapy has not improved survival, it has shown delayed deterioration in Eastern Cooperative Oncology Group (ECOG) performance status (PS) and prolonged time to opiate use. Upon further analysis of the data, abiraterone with prednisone and bone-targeted therapy delayed the median time to opiate use in cancer-related pain to a not estimable time vs. 26.1 months in prednisone with bone-targeted therapy group (HR, 0.74; P = 0.078). When used in combination with bone-targeted therapy, abiraterone with prednisone delayed the time to ECOG PSdeterioration to 15.7 months compared to 11.8 months for the prednisone only group, with an HR, 0.76; P = 0.026. Thus, abiraterone with bone-targeted therapy added a clinical benefit with acceptable adverse events. Another measure of outcome called TOI using a composite of physical well-being, functional well-being and PCS scores was looked at and statistically significant difference in favor of abiraterone with prednisone was observed.36
Final analysis of the COU-AA-302 trial after a median follow-up of 49.2 months showed that patients in both groups experienced similar percentages of grade 1–2 adverse events including fluid retention and edema (30 vs. 23%), hypokalemia, hypertension (19 vs. 11%), and cardiac events. Median time to opiate use in cancer-related pain was 33.4 months in the abiraterone group vs. 23.4 months in the placebo group (HR, 0.72; P = 0.0001).32 While all the PROs collected, including the TOI, remained significant using a mixed-effects model for repeated measures, further collection of data beyond a year was limited because of attrition beyond a year of treatment.37
Regardless of whether abiraterone was used in the first-line or second-line setting, performance status in and of itself was also found to be a predictor of response to abiraterone acetate. In a pooled analysis from three Canadian centers that examined the differences between patients with ECOG PS of 0–1 vs. PS of 2 or more, patients with PS ≥2 were less likely to achieve prostate-specific antigen (PSA) response, had shorter time to PSA progression and decreased OS,38 suggesting perhaps the use of abiraterone earlier in the disease course, rather than waiting until later on when patients have worse functional status or compromised physical ability, would have better outcomes. The ability to measure these PROs across different studies and different drugs also helps conceptualize to patients what they can expect from each systemic therapy for mCRPC. Even for mCRPC patients who are minimally symptomatic or asymptomatic, there is an expected delay in the deterioration of quality of life or delayed cancer-related symptoms.
Other trials
In a Belgian retrospective study, 368 patients with mCRPC from 23 hospitals who progressed after docetaxel and started on abiraterone and prednisone were analyzed.39 About 75% of patients discontinued abiraterone due to disease progression and 25% due to toxicity. Median OS was 15.1 months, similar to the OS of patients enrolled in COU-AA-301 trial. Anemia grade 3 or more was observed in 13.9% of patients compared to 7.8% of patients patients in the COU-AA-301 trial. Also, hypokalemia ≥grade 3 occurred more in the Belgian patients than in patients COU-AA-301 trial (7.3 vs. 4.4%). Conversely, cardiac disorders ≥grade 3 including ischemic events and arrhythmias were less in the Belgian study (0.8 vs. 5.2% in COU-AA-301 trial). This can be explained by the difference in protocols since Belgian patients underwent cardiac evaluation only upon development of symptoms while the COU-AA-301 trial had patients undergo routine cardiac evaluation. Other side effects were similar between the two studies, such as the rates of nausea, vomiting and fatigue. Another retrospective study observed outcomes of 265 patients from 19 different Italian hospitals who received abiraterone following progression after docetaxel in the context of named patient program.40 Median OS was 17 months in the Italian group compared to 15 months in COU-AA-301 trial. Of those patients, 47.5% had pain at the beginning of treatment with abiraterone. Furthermore, of the patients who had pain at the commencement of their treatment, 29% had improvement of pain only; while 60% of these patients had either no change or even worsening of their pain. But pain assessment was collected based on physician notes not periodically using unified scores. Most common adverse events were fatigue, anemia, and pain followed by edema. Grade 3 or more toxicities were as follows: fatigue (4.2%), anemia (4.2%), and limb pain (0.4%), similar to those reported in COU-AA-301 trial.
A Phase III double-blind trial was held in China to evaluate the safety and tolerance of abiraterone in Asian patients with mCRPC after docetaxel failure.41 A total of 214 patients were randomized 2:1 to receive either abiraterone with prednisone or placebo with prednisone. The median age of patients was 68 years. Regarding the primary end point of the study, abiraterone delayed time to PSA progression by 169 days compared to 84 days in the prednisone-only group (HR, 0.59; P = 0.0001). Abiraterone reduced pain progression by 50% compared to placebo with prednisone (HR, 0.49; P = 0.0014). Quality of life was better with abiraterone using FACT-P scores (median score 110 vs. 31). Less fatigue was observed with abiraterone using BFI score (1.5 vs. 2.8 for the prednisone alone group). Adverse events were comparable between the two groups. Grade 3–4 side effects occurred in 32 and 28% in the abiraterone group and placebo group, respectively. Bone pain was equal in both groups, 2.8%. In a single-arm Phase II study, 82 patients in Taiwan and Korea with mCRPC progressing after docetaxel chemotherapy received abiraterone with prednisone.42 The most common adverse event was bone pain (20%), hypokalemia (7%) followed by fluid retention (5%). A retrospective study was designed to assess the safety of abiraterone in 51 patients with mCRPC with cardiac comorbidities.43 Hypertension occurred in 41% of the patients and 14% had cardiac ischemia. Most of the patients had received two prior hormonal lines of therapy and docetaxel chemotherapy previously. There were no significant variations in left ventricular ejection fraction. Fluid retention and hypertension occurred in 18 and 16% of the patients, respectively, and both were well managed and controlled with medical treatment only. In a large meta-analysis assessing cardiac toxicity of new hormonal agents used in the treatment of mCRPC including abiraterone, it was found that these agents did not significantly increase the risk of high-grade cardiac toxicity.44 However, these agents (including abiraterone) increased the relative risk of all grades of hypertension. In a Phase II study in Japan, 47 patients with mCRPC who progressed after docetaxel received either abiraterone with prednisone or placebo with prednisone. Of 16 patients, nine who had pain at the start of treatment (56%) had a pain palliation response with a median time to pain progression not reached. Seven patients (43%) had improvement in ECOG PS by 1 or more. Abnormal hepatic function and hypertension occurred in 10.6 and 6.4% of patients, respectively, with no treatment discontinuation. There is also an ongoing trial called AQUARiUS (A Study to Investigate the Impact of Abiraterone Acetate and Enzalutamide on Health-related Quality of Life, Participant-Reported Outcomes, and Medical Resource Use in Metastatic Castration-resistant Prostate Cancer Participants) at clinicaltrials.gov (identifier NCT02813408) that serves to examine the different QoL outcomes between the two most commonly used antiandrogen or androgen-targeted signaling agents.
Conclusion
The paradigm of treatment for mCRPC has vastly changed since the approval of abiraterone acetate. However, measures of success using novel drugs rely heavily, not only on the actual as well as perceived improvement in OS, but also in other secondary end points, including quality of life and other measures of PROs. Now that the treatment options for mCRPC have increased, the impact of therapy on quality of life becomes increasingly more important. With the data obtained from the abovementioned clinical trials, it becomes easier to understand and explain to the patient the benefit of abiraterone not only in extending survival and delaying the use of cytotoxic therapy but also in delaying deterioration in HRQoL. Improvement in HRQoL and pain palliation is seen not only with abiraterone but also with other agents including enzalutamide and radium-223. However, there are no head-to-head trials that directly compare the palliative effects of the newly approved agents for mCRPC now, nor will there likely ever be. In addition, it is difficult to compare the results across trials to each other because of lack of consistency in the scales used and the PRO instruments utilized. Standardized PRO instruments will be required to accurately monitor the patient experience with the various treatments. Certainly, given only modest survival benefits at best with some of these agents, and that the use of these drugs is not without toxicity, being cognizant of the ever increasing functional status and quality of life measures while patients are on these life-prolonging medications would be equally as important.33,45
Disclosure
The authors report no conflicts of interest in this work.
References
Chi KN, Bjartell A, Dearnaley D, et al. Castration-resistant prostate cancer: from new pathophysiology to new treatment targets. Eur Urol. 2009;56(4):594–605. | ||
Hellerstedt BA, Pienta KJ. The current state of hormonal therapy for prostate cancer. CA Cancer J Clin. 2002;52(3):154–179. | ||
Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005;294(2):238–244. | ||
Bubley GJ, Carducci M, Dahut W, et al. Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: recommendations from the Prostate-Specific Antigen Working Group. J Clin Oncol. 1999;17(11):3461–3467. | ||
Scher HI, Halabi S, Tannock I, et al; Prostate Cancer Clinical Trials Working Group. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008;26(7):1148–1159. | ||
Costa L, Badia X, Chow E, Lipton A, Wardley A. Impact of skeletal complications on patients’ quality of life, mobility, and functional independence. Support Care Cancer. 2008;16(8):879–889. | ||
Penson DF, Litwin MS. The physical burden of prostate cancer. Urol Clin North Am. 2003;30(2):305–313. | ||
Sullivan PW, Mulani PM, Fishman M, Sleep D. Quality of life findings from a multicenter, multinational, observational study of patients with metastatic hormone-refractory prostate cancer. Qual Life Res. 2007;16(4):571–575. | ||
Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351(15):1513–1520. | ||
Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351(15):1502–1512. | ||
Berthold DR, Pond GR, Soban F, de Wit R, Eisenberger M, Tannock IF. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: updated survival in the TAX 327 study. J Clin Oncol. 2008;26:242–245. | ||
Seal BS, Asche CV, Puto K, Allen PD. Efficacy, patient-reported outcomes (PROs), and tolerability of the changing therapeutic landscape in patients with metastatic prostate cancer (MPC): a systematic literature review. Value Health. 2013;16(5):872–890. | ||
Nussbaum N, George DJ, Abernethy AP, et al. Patient experience in the treatment of metastatic castration-resistant prostate cancer: state of the science. Prostate Cancer Prostatic Dis. 2016;19:111–121. | ||
Vasaitis TS, Bruno RD, Njar VC. CYP17 inhibitors for prostate cancer therapy. J Steroid Biochem Mol Biol. 2011;125:23–31. | ||
Yap TA, Carden CP, Attard G, de Bono JS. Targeting CYP17: established and novel approaches in prostate cancer. Curr Opin Pharmacol. 2008;8(4):449–457. | ||
Yang LP. Abiraterone acetate: in metastatic castration-resistant prostate cancer. Drugs. 2011;71(15):2067–2077. | ||
Hoy SM. Abiraterone acetate: a review of its use in patients with metastatic castration-resistant prostate cancer. Drugs. 2013;73(18):2077–2091. | ||
U.S. Department of Health and Human Services. Guidance for Industry. Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. Silver Spring, MD: US FDA; 2006. | ||
Calvert M, Blazeby J, Altman DG, et al. Reporting of patient-reported outcomes in randomized trials: the CONSORT PRO extension. JAMA. 2013;309:814–822. | ||
Clark MJ, Harris N, Griebsch I, Kaschinski D, Copley-Merriman C. Patient-reported outcome labeling claims and measurement approach for metastatic castration-resistant prostate cancer treatments in the United States and European Union. Health Qual Life Outcomes. 2014;12:104. | ||
Cella DF, Tulsky DS, Gray G, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11(3):570–579. | ||
Winstead-Fry P, Schultz A. Psychometric analysis of the Functional Assessment of Cancer Therapy-General (FACT-G) scale in a rural sample. Cancer. 1997;79(12):2446–2452. | ||
Overcash J, Extermann M, Parr J, Perry J, Balducci L. Validity and reliability of the FACT-G scale for use in the older person with cancer. Am J Clin Oncol. 2001;24(6):591–596. | ||
Webster K, Cella D, Yost K. The functional assessment of chronic illness therapy (FACIT) measurement system: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1:79. | ||
Esper P, Mo F, Chodak G, Sinner M, Cella D, Pienta KJ. Measuring quality of life in men with prostate cancer using the functional assessment of cancer therapy-prostate instrument. Urology. 1997;50(6):920–928. | ||
de Bono JS, Logothetis CJ, Molina A, et al; COU-AA-301 Investigators. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011;364(21):1995–2005. | ||
Fizazi K, Scher HI, Molina A, et al; COU-AA-301 Investigators. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012;13(10):983–992. | ||
Logothetis CJ, Basch E, Molina A, et al. Effect of abiraterone acetate and prednisone compared with placebo and prednisone on pain control and skeletal-related events in patients with metastatic castration-resistant prostate cancer: exploratory analysis of data from the COU-AA-301 randomised trial. Lancet Oncol. 2012;13(12):1210–1217. | ||
Harland S, Staffurth J, Molina A, et al; COU-AA-301 Investigators. Effect of abiraterone acetate treatment on the quality of life of patients with metastatic castration-resistant prostate cancer after failure of docetaxel chemotherapy. Eur J Cancer. 2013;49(17):3648–3657. | ||
Sternberg CN, Molina A, North S, et al. Effect of abiraterone acetate on fatigue in patients with metastatic castration-resistant prostate cancer after docetaxel chemotherapy. Ann Oncol. 2013;24(4):1017–1025. | ||
Ryan CJ, Smith MR, de Bono JS, et al; COU-AA-302 Investigators. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138–148. | ||
Ryan CJ, Smith MR, Fizazi K, et al; COU-AA-302 Investigators. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015;16(2):152–160. | ||
Basch E, Autio K, Ryan CJ, et al. Abiraterone acetate plus prednisone versus prednisone alone in chemotherapy-naive men with metastatic castration-resistant prostate cancer: patient-reported outcome results of a randomised phase 3 trial. Lancet Oncol. 2013;14(12):193–1199. | ||
Rathkopf DE, Smith MR, de Bono JS, et al. Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302). Eur Urol. 2014;66(5):815–825. | ||
Saad F, Shore N, Van Poppel H, et al. Impact of bone-targeted therapies in chemotherapy-naive metastatic castration-resistant prostate cancer patients treated with abiraterone acetate: post hoc analysis of study COU-AA-302. Eur Urol. 2015;68:570–577. | ||
Basch E, Autio KA, Smith MR, et al. Effects of cabozantinib on pain and narcotic use in patients with castration-resistant prostate cancer: results from a phase 2 nonrandomized expansion cohort. Eur Urol. 2015;67(2):310–318. | ||
Cella D, Li S, Li T, Kheoh T, Todd MB, Basch E. Repeated measures analysis of patient-reported outcomes in prostate cancer after abiraterone acetate. J Community Support Oncol. 2016;14(4):148–154. | ||
Azad AA, Eigl BJ, Leibowitz-Amit R, et al. Outcomes with abiraterone acetate in metastatic castration-resistant prostate cancer patients who have poor performance status. Eur Urol. 2015;67(3):441–447. | ||
Van Praet C, Rottey S, Van Hende F, et al. Abiraterone acetate post-docetaxel for metastatic castration-resistant prostate cancer in the Belgian compassionate use program. Urol Oncol. 2016;34(6):254.e7–254.e13. | ||
Caffo O, De Giorgi U, Fratino L, et al. Safety and clinical outcomes of patients treated with abiraterone acetate after docetaxel: results of the Italian Named Patient Programme. BJU Int. 2015;115(5):764–771. | ||
Sun Y, Zou Q, Sun Z, et al. Abiraterone acetate for metastatic castration-resistant prostate cancer after docetaxel failure: a randomized, double-blind, placebo-controlled phase 3 bridging study. Int J Urol. 2016;23(5):404–411. | ||
Kwak C, Wu TT, Lee HM, et al. Abiraterone acetate and prednisolone for metastatic castration-resistant prostate cancer failing androgen deprivation and docetaxel-based chemotherapy: a phase II bridging study in Korean and Taiwanese patients. Int J Urol. 2014;21(12):1239–1244. | ||
Procopio G, Grassi P, Testa I, et al. Safety of abiraterone acetate in castration-resistant prostate cancer patients with concomitant cardiovascular risk factors. Am J Clin Oncol. 2015;38(5):479–482. | ||
Iacovelli R, Verri E, Cossu Rocca M, et al. The incidence and relative risk of cardiovascular toxicity in patients treated with new hormonal agents for castration-resistant prostate cancer. Eur J Cancer. 2015;51(14):1970–1977. | ||
Phillips R. Prostate cancer: patient-reported outcomes of first-line abiraterone therapy. Nat Rev Urol. 2013;10:619. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.