")
Back to Journals » Patient Preference and Adherence » Volume 16
Impact of a Dental Storybook on Parents’ Knowledge of Children’s Oral Health: A Randomized Controlled Trial
Authors Alsaadoon AM , Sulimany AM, Hamdan HM , Murshid EZ
Received 21 April 2022
Accepted for publication 12 August 2022
Published 22 August 2022 Volume 2022:16 Pages 2271—2285
DOI https://doi.org/10.2147/PPA.S370430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Alrouh M Alsaadoon,1 Ayman M Sulimany,1 Hebah M Hamdan,2 Ebtissam Z Murshid1
1Department of Pediatric Dentistry and Orthodontics, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; 2Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Correspondence: Alrouh M Alsaadoon, Department of Pediatric Dentistry and Orthodontics, College of Dentistry, King Saud University, Riyadh, 11545, Saudi Arabia, Email [email protected]
Purpose: To evaluate the effectiveness of a dental storybook on parents’ knowledge about oral health of their children and to assess their perception of its effect in reducing dental anxiety levels among their children, as well as improving their oral health knowledge.
Patients and Methods: This was a two-arm parallel, single-blind, randomized controlled trial (RCT) which was performed at the pediatric dental clinics in the Dental University Hospital, King Saud University, Riyadh, Saudi Arabia. Parents of 88 children (6– 8 years old) were included in the present study. Parents and their children were randomly divided into two groups as follows: the intervention group (received the storybook and verbal oral hygiene instructions) and the control group (only received verbal oral hygiene instructions; same information included in the book). Three dental visits, including screening, examination/cleaning and treatment, were provided for each child. In the screening visit, baseline parental oral health knowledge was evaluated for all parents. Afterward, parental oral health knowledge was re-evaluated in the examination visit. In the treatment visit, a parental perception questionnaire was administered to parents following treatment to evaluate their satisfaction regarding the use of the storybook in reducing anxiety levels among their children.
Results: There was a significant improvement in the total knowledge score at the follow-up visit in the intervention group compared to the control group (P< 0.0001). Overall, the majority of parents perceived the storybook as a useful source of information, and they found it to be effective in reducing dental anxiety levels among their children.
Conclusion: The dental storybook is an effective educational tool that can help parents become more knowledgeable about their children’s oral health. Moreover, parents perceived the storybook as an effective tool for enhancing their oral health knowledge and lowering their children’s dental anxiety.
Keywords: oral health, dental health education, parenting education
Introduction
Oral health is a key indicator of overall health, well-being and quality of life. Oral health is multifaceted and includes the ability to speak, smile, taste, chew, swallow and convey a range of emotions through facial expressions with confidence and without pain, discomfort and disease of the craniofacial complex.1 Inadequate oral health care can have significant adverse impacts on children and their families. Therefore, the adoption of proper oral health behaviors in children is critical in maintaining their oral health-related quality of life (OHRQoL),2 which is influenced by several factors, including but not limited to parental oral health knowledge, oral hygiene habits, attitudes and cultural beliefs.3,4
A primary goal of oral health is to ensure that people have adequate knowledge to control the determinants of their health.5 This is known as oral health literacy, which is defined as “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate oral health decisions”.6 Nevertheless, many people lack the adequate knowledge about oral health. Consequently, oral diseases, most predominantly dental caries, have become prevalent in many countries.7,8
It is known that childhood practices determine oral health in adulthood. Thus, dental care must start at an early age. Because most children are unaware of the proper practices to maintain their health, they depend heavily on their guardians to address certain health behaviors and to establish their propensity and ability to achieve daily practices (dietary and hygiene) up to a certain age.9 Such practices are dependent on the parents’ knowledge, and children may suffer if their parents’ information is deficient.10,11
In general, the literature has emphasized that the average knowledge level of oral health among parents and care givers worldwide is unsatisfactorily low.9,10,12–14 Similarly, a considerable percentage of children worldwide have also displayed poor oral health knowledge.15–19
Several tools, ranging from simple and inexpensive measures to sophisticated and expensive measures, have been developed to raise awareness and disseminate knowledge among parents and their children. Among such measures, educational handouts on oral health to parents have successfully raised parental oral health awareness and demonstrated their effectiveness in improving their oral health knowledge.20–22 Moreover, community-oriented programs, internet videos and presentations are also promising methods to promote knowledge on oral health among parents.23–26 Additionally, oral health education among children has resulted in improvement of oral health knowledge and oral health-related behaviors.27–30
Given the pivotal role parents/guardians have on children’s oral health and behaviors, an increasing number of investigations have focused on evaluating the role of parental/guardian literacy on child oral health outcomes.31,32 A systematic review of the literature has shown that poor oral health knowledge of parents is an important indicator of children’s poor oral hygiene.33 Moreover, parents with lower oral health literacy are less likely to seek dental care for their children compared to parents of higher oral health literacy,34,35 which may result in more fearful children in the dental office.36
Overcoming this fear is important to avoid the adverse effects of dental anxiety. Traditionally, there are various approaches to managing dental anxiety and fear ranging from basic to advanced approaches.37 One of the most significant approaches to overcoming dental anxiety is based on the social learning theory by Albert Bandura, which posits that individuals learn certain behaviors through imitation, observation and modeling.38 In the context of overcoming dental anxiety, this would include giving pediatric patients preparatory information before their dental visits, which may, in turn, decrease pain perception and discomfort.39 Additionally, the significance of preparatory information can be explained by the self-regulation theory (SRT), which holds that individuals will attempt to control their behavior based on expectations acquired from prior experience and information available to them.40,41
Given both the social learning theory and SRT, the provision of positive preparatory dental resources about forthcoming procedures can psychologically prepare pediatric patients for their dental visits and lower the disparity between the expected and the actual experience.42 On this basis, Fox and Newton found a reduction in dental fear among British children after exposing them to positive images of dentistry-related materials.42 Another study has reported a considerable reduction of dental anxiety levels after supplying children with audio-visual books prior to their dental appointments.43 As a result, presenting information and explaining procedures to children can be successful in reducing anxiety levels.
The existing literature has highlighted the importance of oral health education for children, reinforcing the need for the acquisition of healthy attitudes and habits in the entire family. However, there is a paucity of literature available regarding the effect of oral health-related information on parental oral health knowledge. To the best of our knowledge, no previous studies have been conducted to evaluate the impact of a dental storybook on the parental knowledge and their perception of such intervention in terms of improving their oral health knowledge and reducing dental anxiety levels among their children.
Thus, the aim of the present study was to determine the effect of a dental storybook on parents’ knowledge about oral health of their children and to assess the parental perception of the storybook in reducing dental anxiety levels among their children, as well as improving their oral health knowledge.
Materials and Methods
Study Design and Setting
This was a two-arm parallel, single-blind, randomized controlled trial (RCT) with an allocation ratio of 1:1. It was performed at the pediatric dental clinics in the Dental University Hospital, King Saud University located in Riyadh, Saudi Arabia. The study was conducted from January 2019 to March 2020.
The present study was the second part of a previously conducted clinical trial. The previous study was a randomized clinical trial that evaluated the effectiveness of a specially designed dental storybook in reducing dental anxiety and improving behavior among children on examination and treatment plan visits followed by a restorative dental visit.44
Study Participants
The research participants of the trial were 6- to 8-year-old children who satisfied all of the following inclusion criteria: children had to be medically fit (classified as ASA I by the American Society of Anesthesiologists Classification);45 children and their parents had to be able to speak and read Arabic (as the storybook is written in Arabic); and children had to require restorative dental treatments (occlusal fillings) requiring a local anesthetic in the upper arch. The exclusion criteria were as follows: children with special needs, including complete audio-visual impairment, learning difficulties and mental retardation; children whose parents were not Arabic speakers; children who had previously been treated with general anesthesia, nitrous or sedation; children with emergency dental needs, such as abscesses and cellulitis; and children suffering from dental phobia (where pharmacological intervention is required for treatment to proceed), as per their baseline anxiety measurements.
Study Procedure
The children attended a screening visit, where recruitment took place based on the inclusion and exclusion criteria. The selected children then attended the following two additional visits: one to complete an examination, and a final visit for restorative dental treatment. All three visits were performed by a senior pediatric dentistry resident (A.M.A.).
Visit 1: Screening
At this visit, the children underwent a basic oral examination to determine their suitability for inclusion in the study. Next, consent was obtained from the selected children’s parents/guardians.
The parents/guardians provided the children’s demographic data and completed a self-administered survey (Appendix 1) to establish their baseline knowledge of their children’s oral health. After that, the main investigator verbally explained to the parents/guardians certain key oral hygiene information and instructions, all of which were provided in the dental storybook. Finally, the independent study investigator randomly allocated the children to one of the two research groups.
The distribution of the dental storybook to the intervention group was performed by the independent study investigator. The investigator was also responsible for instructing the parents/guardians to read the dental storybook for their children once when it was received and one final time the day before the examination visit (twice in total). The independent study investigator played no part in evaluating the outcome measures.
Visit 2: Examination and Cleaning
The examination involved collecting the complete dental and medical history of the children from their parents/guardians. Additionally, intra- and extra-oral exams were conducted on the participating children, and radiographs were taken if required. The children were then subjected to prophylactic and fluoride treatments, and they were each given a tailored treatment plan. Next, to assess the impact of the dental storybook on the parents/guardians’ oral health knowledge, the parents/guardians completed the same knowledge survey to assess whether the storybook influenced their knowledge.
Visit 3: Treatment
At their final visit, the children underwent restorative treatment under local anesthesia. The parents/guardians also completed a survey on parental perception (Appendix 2) to examine the efficacy of the dental storybook in improving their oral health knowledge and in reducing their children’s dental anxiety.
Each of the three visits was conducted one week apart. Parents/guardians were permitted to attend all visits, and basic behavior guidance was followed. Any additional appointments the children required to complete their treatment were booked at the end of the study with the same dentist and dental assistant.
Intervention: Dental Storybook
The purpose of the dental storybook was to prepare the children for their visits to the dental clinic. The book was written in a specific type of simple Arabic, and it featured cartoon characters and a distinct range of colors to create an engaging children’s story. The book described the stages of the first visit and other relevant information as follows: details of the prophylactic and topical fluoride treatments; details of the clinic and dental office waiting area; the roles of the dentist and dental assistant; and details of the dental instruments and what they are used for. Thus, the dental storybook aimed to familiarize the children with the reality of a visit to the dentist. At the end of the book, there was a special page dedicated to give parents even more detailed information as well as dental tips and suggestions.
To optimize the book, experts in childhood education and childhood Arabic reviewed it prior to its approval and registry with the Ministry of Culture and Information of Saudi Arabia (Registration number ISBN: 978–603-02-0122-8) (Figure 1).
 |
Figure 1 The cover of the book entitled, “My First Visit to the Dentist”. |
Outcome Measures
A specially designed self-administered questionnaire about the parents’/guardians’ knowledge and perception regarding the use of a dental storybook for improving their oral health knowledge and reducing dental anxiety levels among their children was completed by one of the parents. The questionnaire contained three sections, namely, background information, parent’s knowledge and parent’s perception, with a total of 36 questions.
The background information questionnaire was administered to all parents/guardians at the screening visit, and it consisted of 25 questions covering demographic information, dental care pattern and behavioral information.
The knowledge questionnaire was administered to all parents/guardians during the screening and examination visits, and it consisted of five questions which were fully covered in the dental storybook. These questions were covering the parental knowledge regarding brushing frequency, the age of first dental visit, frequency of dental visits, the impact of infection in primary teeth and the association between visiting a dentist at a young age with dental anxiety (Appendix 1).
The American Academy of Pediatric Dentistry reference manual was used to determine the correct answers regarding the parental oral health knowledge.46
The perception questionnaire was administered at the treatment visit, and it was administered only to the parents/guardians of the intervention group. This questionnaire consisted of eight questions covering the parental perception of the following aspects: the usefulness of information included in the book; the explanation of the dental visits in a simple manner; the knowledge acquired from the storybook, the ease of following and understanding by the child; the impact of the storybook on the child’s anxiety; and the role of the storybook in fostering acceptance of dental visits (Appendix 2).
Validity and Reliability of the Questionnaires
The questionnaires were developed in the English language, and they were then translated to Arabic by a certified translation agency followed by translation into the English language to test the reliability of the translation.
The content validity of the questionnaire was assessed by three content experts. The primary objectives of the pre-test study were to assess the appropriateness, importance and phrasing of each question. The experts were nominated on the basis of either experience in epidemiological and/or pediatric dentistry research as evidenced by the number of publications in that field or significant clinical work experience. Minor changes were made to the questionnaires in response to the experts’ feedback to increase the comprehensiveness of the questions.
To ensure face validity, a subgroup of ten parents who did not participate in the study were asked to complete the questionnaire to evaluate their understanding and comprehension of the questionnaire. Moreover, after a period of 2 weeks, parents/guardians were asked to complete a second copy of the questionnaire to assess the test-retest reliability. The agreement of the questionnaire results was assessed using Cohen’s kappa statistic, which resulted in an average k of 0.82, indicating good reproducibility and reliability.
Sample Size
The power of the sample was calculated using the G power sample power calculator (University of Kiel, Kiel, Germany).47 A total sample size of 88 was required for an effect size of 0.25 and a power of 0.95 for a two-sided normal distribution with the two groups. Anticipating a possible attrition rate of 20%, the estimated sample size of 105 was required.
Randomization and Blinding
The children were randomly assigned to one of the following two groups according to the block randomization approach: intervention group, children received the dental storybook; and control group, children did not receive the dental storybook. The equal allocation of the children to the two groups was completed by an independent study investigator who used opaque, sealed and sequentially numbered envelopes to conceal the allocations from the main investigator. The main investigator (outcome assessor, A.M.A.) was blinded to the group allocations.
Ethics
The present study was performed in accordance with the Declaration of Helsinki and followed CONSORT guidelines. The study was granted ethical approval by the Institutional Review Board (IRB) at the College of Medicine, King Saud University (research designation E-18-3190), and it was also approved by the Ethics Committee of the College of Dentistry Research Center (CDRC) of King Saud University (research designation No. PR 0104). This study was also registered at the ISRCTN (study ID ISRCTN44193972). Informed consent was obtained from all the subjects involved in the study.
Statistical Analysis
Continuous variables with normal distribution were reported as mean values (standard deviation, SD), and continuous variables with skewed distribution were presented as median values (interquartile range, IQR). Categorical variables were reported as numbers and percentages. Pearson’s Chi-squared test and Fisher’s exact test were used to investigate the differences between the parents’ responses to each knowledge item of the questionnaire at each visit. The McNamara test was used to assess the change in parents’ response with time. We also performed the Mann–Whitney test to calculate the knowledge score and compare it between the study groups at different visits. Moreover, the Wilcoxon test was used to assess the change in the knowledge score within each group. Likert scale responses for both knowledge and perception questionnaires were dichotomized by collapsing strongly agree and agree into one category, “agree”. Strongly disagree, disagree, and neutral were collapsed into the second category “disagree”.
Finally, a multivariate mixed-effects negative binomial regression model was developed to assess the effect of the intervention on the knowledge score after controlling for previous dental visits, parental education, and family income. These factors were chosen based on previous studies related to parental oral health knowledge.
The significance level for all tests was set as p ≤ 0.05, and data were analyzed using SAS 9.4 software (SAS Institute, Inc., Cary, NC, USA).
Results
Figure 2 shows a flowchart of the parents/guardians who participated during each trial phase as follows: enrollment, allocation, follow-up and data analysis.
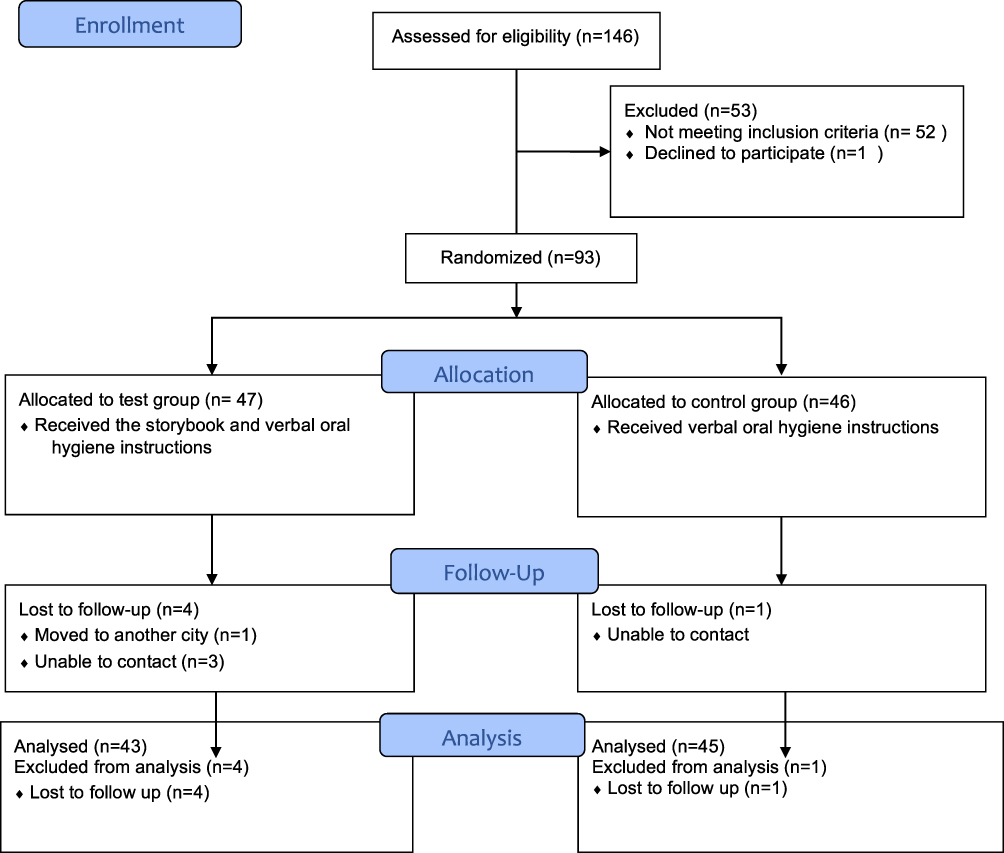 |
Figure 2 CONSORT flow diagram: the flow of participants during each trial phase. Notes: Adapted from: Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3):e1000251.64 Copyright: © 2010 Schulz et al. Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/legalcode). https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000251. |
The demographics of the population are depicted in Table 1. The sample consisted of 88 children aged 6–8 years old (mean age of 7.08 ± 0.76 years) who either received the storybook (n = 43, 48.9%) or did not (n = 45, 51.1%). The children who participated in the study were mostly Saudis (n = 79, 89.8%), and the majority of the families who participated in the study were middle class (n = 47, 53.4%). Many parents (n = 38, 43.2% fathers; n = 42, 47.7% mothers) had a bachelor’s degree. The majority of children were accompanied by their fathers, who were accountable for reading the book to them (n = 46, 52.3%). According to the parents’ responses, 43 of the children had previously visited the dentist (48.9%), whereas 45 children had not previously visited the dentist (51.1%).
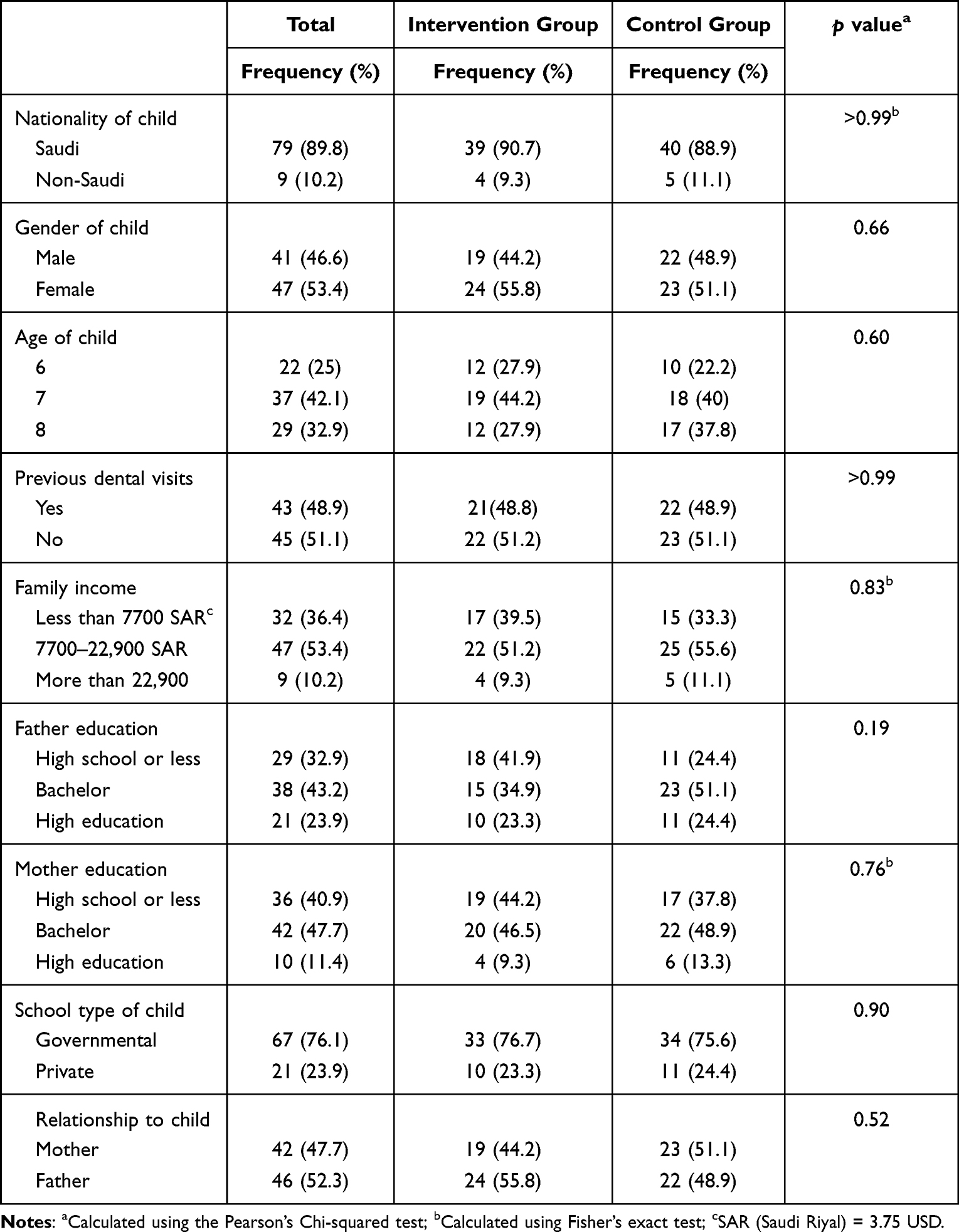 |
Table 1 Background Characteristics According to Study Group |
In general, there were no significant differences in the background characteristics between the two groups.
Table 2 shows the baseline knowledge among the parents of our sample. More than half of the parents in both groups knew about the frequency of brushing and dental visits. Moreover, the majority of the parents knew that infection in primary teeth can harm the permanent teeth. In contrast, most of the parents in both groups were lacking sufficient knowledge regarding the time of the first dental visit and the effect of an early dental visit on the child’s anxiety. However, there was no statistically significant differences between the two study groups regarding the baseline knowledge.
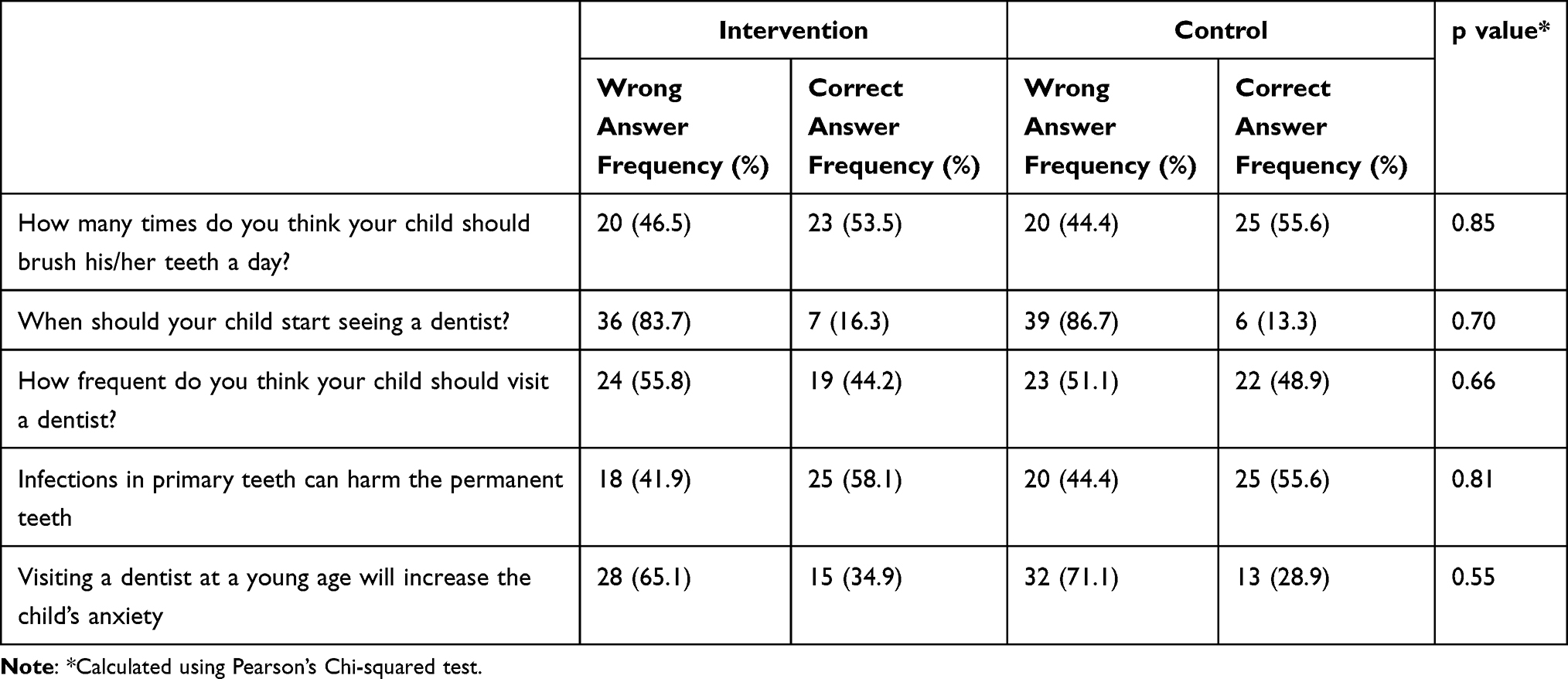 |
Table 2 Parents’ Response to the Knowledge Questions at Baseline |
Table 3 shows the follow-up knowledge of the parents. Regarding the age of the first dental visit, there was a statistically significant difference between the intervention and control group, in which 67.44% of the intervention knew the correct answer compared to only 13.33% of the control group (p < 0.0001). Moreover, almost all the parents (93%) in the intervention group correctly answered the question regarding the frequency of dental visits compared to 60% of the control group (p = 0.0003). Regarding the effect of dental infection of primary teeth on permanent dentition, approximately 84% of the intervention group correctly answered this question compared to 51% in the control group (p = 0.001). Furthermore, the majority of the parents in the intervention group (83.7%) knew the right answer when they were asked about the relationship between visiting the dentist at a young age and dental anxiety compared to 26.7% in the control group (p < 0.0001). In contrast, no statistically significant differences were found between the study groups when parents were asked about the number of times they thought their children should brush their teeth in a day (p = 0.10).
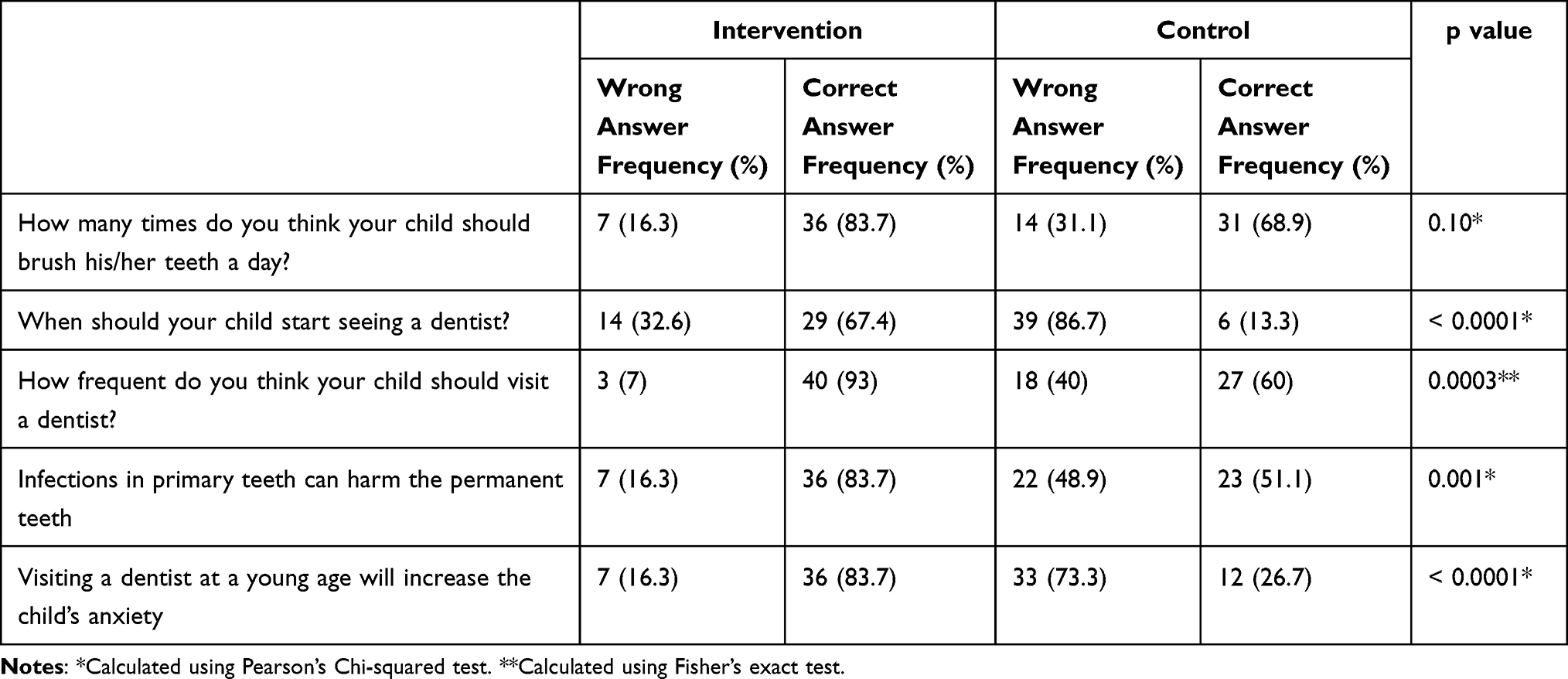 |
Table 3 Parents’ Response to the Knowledge Questions at the Follow-Up |
Tables 4 and 5 illustrate the changes in the parents’ knowledge across time in both groups. There was a significant improvement in the parents’ knowledge in the intervention group in all the items of the knowledge questionnaire. Specifically, 70% of the parents who gave a wrong answer about the frequency of tooth brushing in the first visit knew the correct answer after the intervention (p = 0.0010). Additionally, 66% of the parents who did not know the age of the first dental visit answered it correctly in the second visit (p < 0.0001). Moreover, 87% of parents who gave a wrong answer regarding the frequency of dental visits in the first visit answered it correctly in the second visit (p < 0.000). In addition, 66% of parents who were not aware that infections in the primary teeth can harm the permanent dentition became aware after the intervention (p = 0.0034). Furthermore, 75% of parents who believed that visiting the dentist at a young age would increase their children’s dental anxiety reconsidered their answers in the second visit (p < 0.0001). In contrast, there were no statistically significant improvements in knowledge among parents in the control group (Table 5).
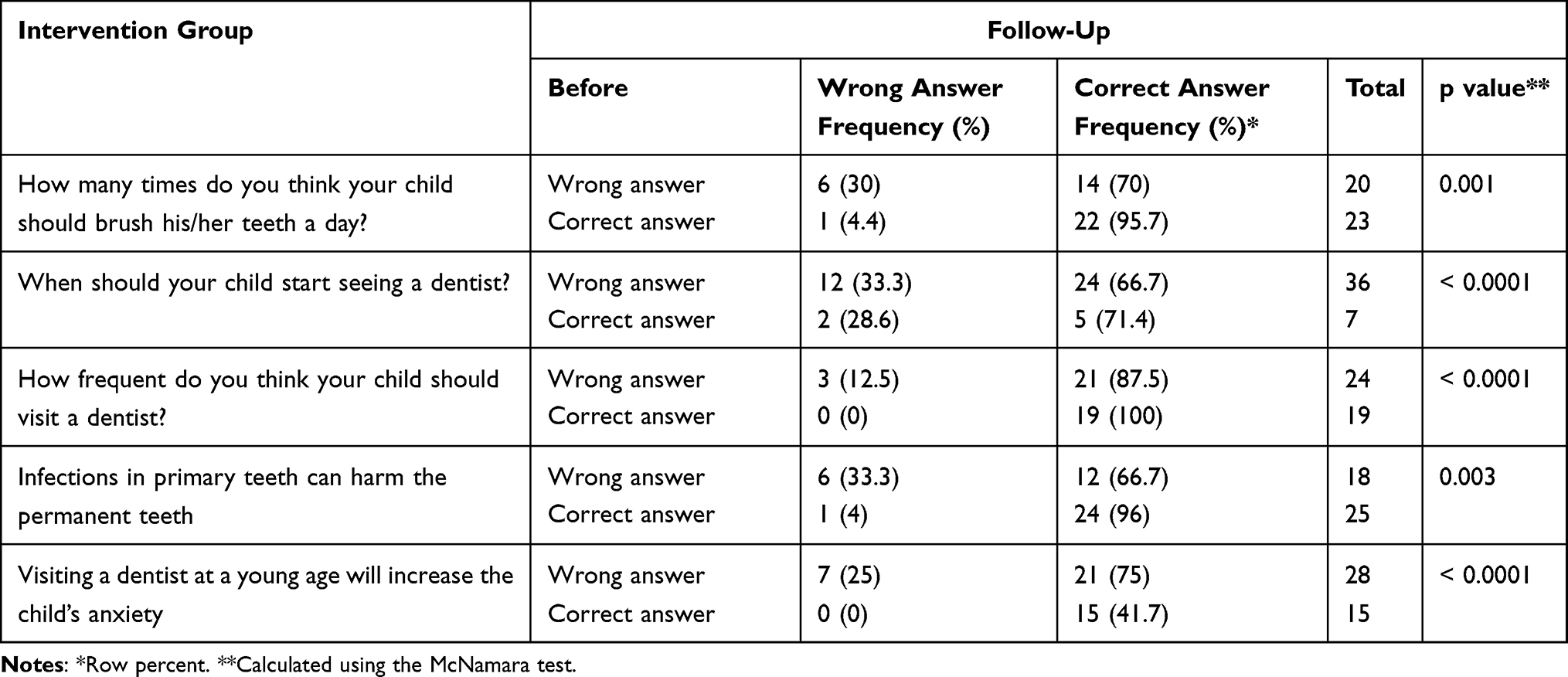 |
Table 4 Changes in the Parents’ Knowledge Across Time in the Intervention Group |
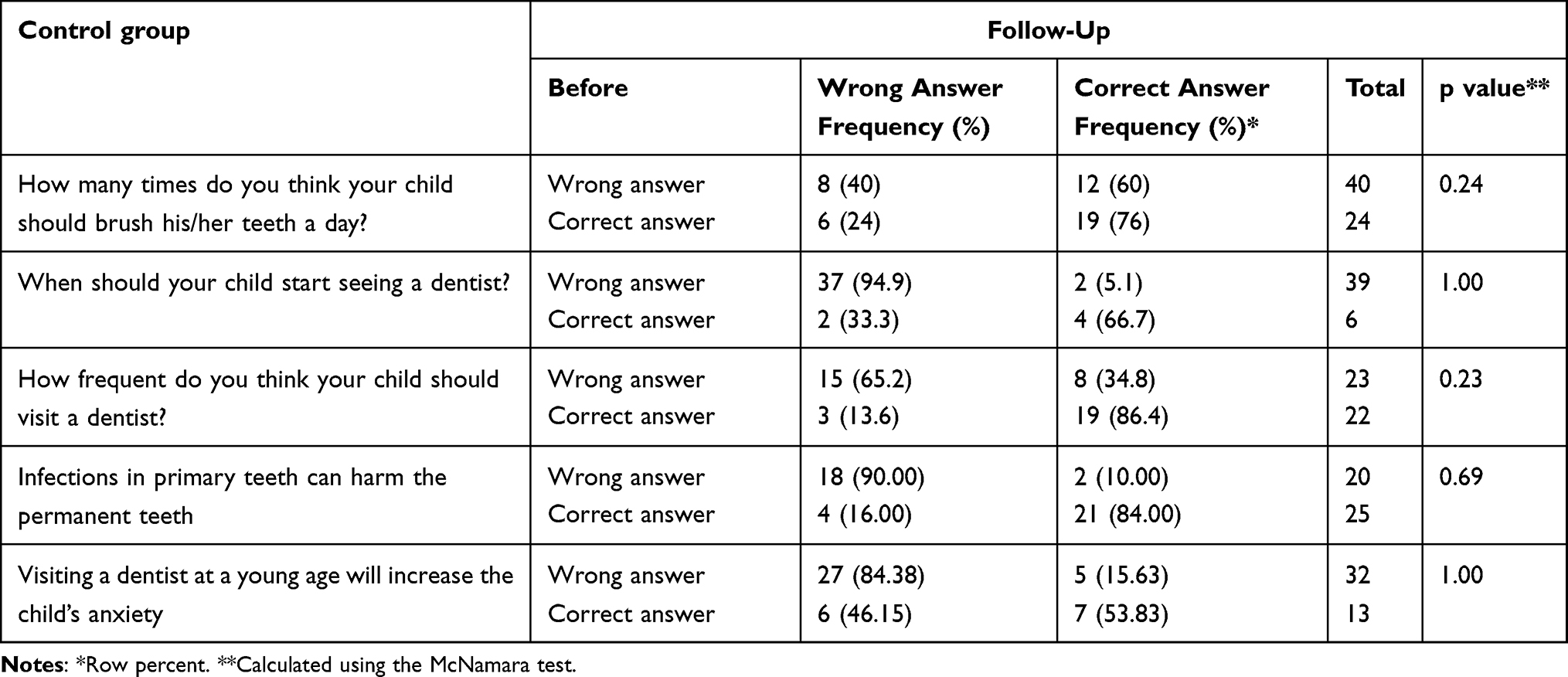 |
Table 5 Changes in the Parents’ Knowledge Across Time in the Control Group |
Table 6 illustrates the differences of the total knowledge score between the study groups during the study period. There was no statistically significant difference in the total knowledge score between the study groups at baseline (p = 0.95). However, we found a significant difference in the total score at the follow-up visit with a median score of 4 (IQR = 1) in the intervention group compared to 2 (IQR = 1) in the control group (p < 0.0001). The within group analysis showed a significant improvement in the total knowledge score among the intervention group, in which the median knowledge score improved from 2 (IQR = 2) at baseline to 4 (IQR = 1) after the intervention (p < 0.0001). However, there was no statistically significant improvement in the total knowledge score among parents in the control group at the follow-up visit (p = 0.36).
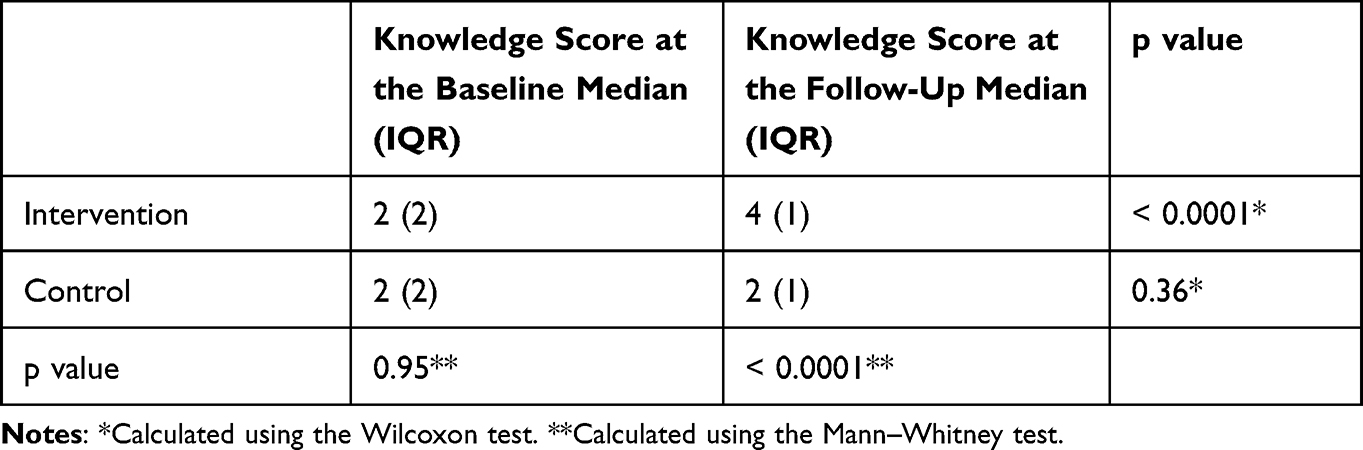 |
Table 6 Difference in the Total Knowledge Score Between the Study Groups |
Furthermore, multivariate mixed-effects negative binomial regression model was to assess the effect of the intervention on the knowledge score after controlling for previous dental visits, parental education, and family income. None of these factors had a significant effect on the relationship between the intervention and the knowledge score.
The majority of parents (95%) perceived the storybook as an informative source with valuable information, and it increased their knowledge towards routine dental visits. Moreover, all parents agreed that the storybook explained the process of visiting the dentist in a simple manner and that it was easy for their children to follow and understand. Most of the parents (81%) found that the storybook was effective in reducing dental anxiety levels among their children and that it helped them to accept the dental visits (Table 7).
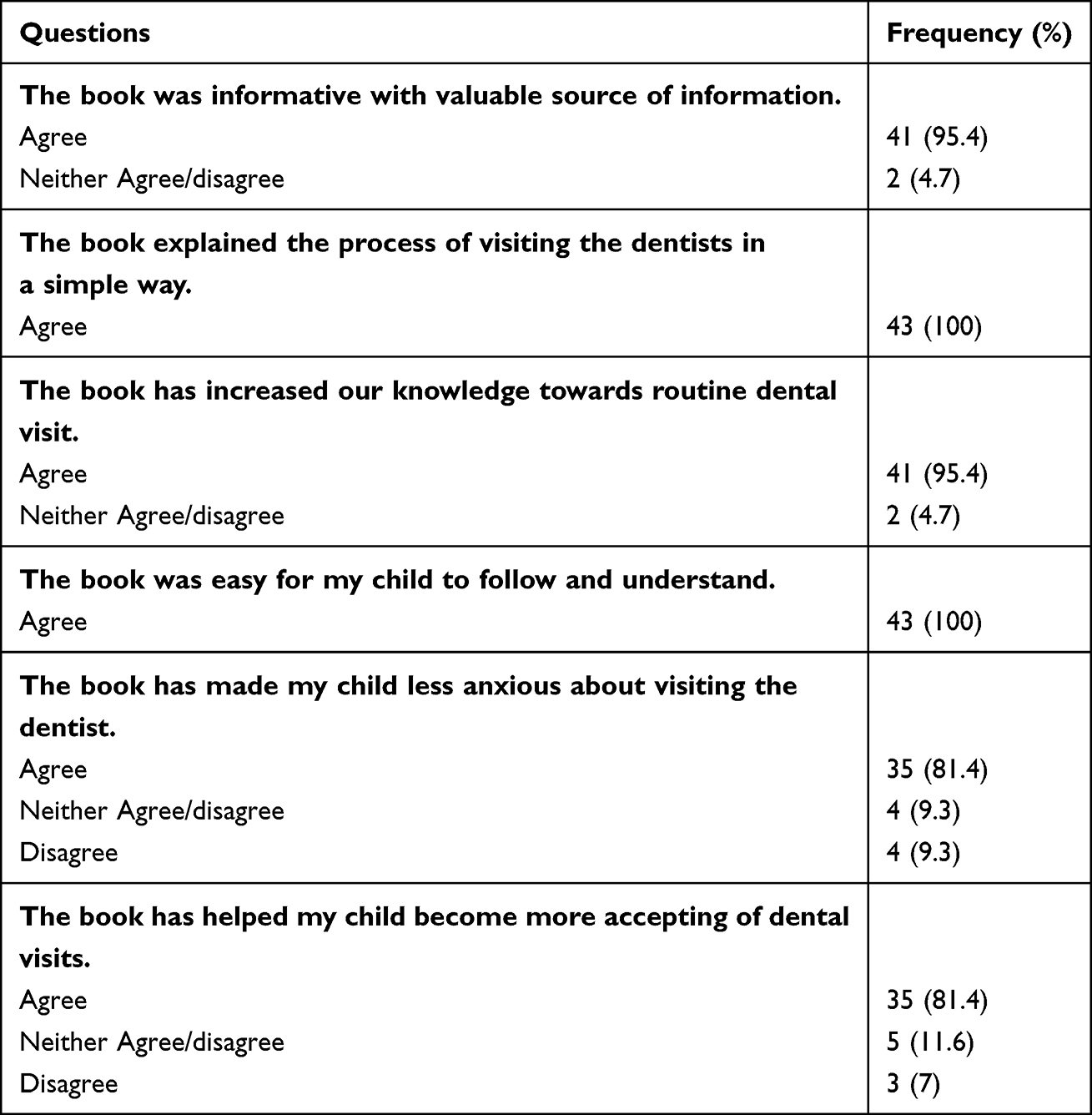 |
Table 7 Parental Perception of the Storybook |
Discussion
Parental oral health education is important to ensure that proper oral health practices are employed for their children. To our knowledge, this is the first study to investigate the role of a dental storybook in improving parental oral health knowledge and assess the parents’ perception regarding the use of the storybook in improving their oral health knowledge and reducing dental anxiety levels among their children. Our findings indicated a significant improvement in parents’ knowledge after using the storybook. The findings of this study were consistent with several randomized controlled trials (RCTs) that have studied information leaflets aimed specifically at parents and claimed that using educational printed materials has a significantly positive effect on the acquisition of information regarding tooth avulsion, orthodontic problems and oral habits.20,21,48 Alsada et al reported an improvement of 32% in knowledge of infant oral health among mothers and early childhood educators after viewing an audio-visual aid.49 Moreover, Kaste et al reported an improvement in oral health knowledge for pregnant women after attending an oral health lecture within a prenatal program.50 Rothe et al found a significant improvement in oral health knowledge among parents after attending an infant oral health education program.24 Furthermore, Bates and Riedy reported improvements in knowledge of oral health among pregnant women and mothers of young children after the women watched an online oral health commercial.51 Additionally, Amin et al reported that a one-time oral health educational workshop was effective in improving parental knowledge with respect to their children’s oral health in African immigrants.25
Nevertheless, none of the abovementioned studies had a control group. One non-blinded quasi-experimental study has been performed using parents and found that a web-based educational film is an effective method to improve parental oral health knowledge, but the parents were not randomly assigned to the control or intervention groups.26
There is increasing awareness among health professionals that health information in a format that the patient can understand needs to be provided to improve their knowledge. Based upon differences in learning styles, various educational methods can be effective in oral health educational programs.52 These formats include verbal information, written information, audiotapes, videotapes, follow-up phone calls, E-mail communication with their doctor and websites to access additional information.53 According to a communication–behavior change model, oral health educational programs based on an information persuasion method have a favorable impact on an individual’s knowledge.54
The findings of the present study demonstrated the power of information disseminated to parents through printed materials. In a written format, material must be eye-catching, concise, contain only the most important details and avoid the use of medical jargon. The effectiveness of the specially designed storybook in the present study may have resulted from its content, simple language and attractive drawings, which corroborated the findings of similar studies, which have reported that educational approaches that are more engaging show more effectiveness in knowledge acquisition and are easily recalled and described in greater detail than those that are less engaging.21,55 Similarly, qualitative studies have indicated that mothers prefer pictorial presentations and simple layouts to improve their understanding of oral health.56,57 These findings are supported by experimental psychology research, indicating that humans prefer visual information over text-based information, which is a phenomenon known as the “picture superiority effect”.58
Importantly, no single instructional method suits all learners. The results of the present study agreed with other studies, which have shown that parents benefit more with verbal and written health information compared to verbal information only.53,59 Lees and Rock determined that there are no significant differences in knowledge scores among written, verbal and video tape methods of oral hygiene instructions for fixed orthodontic patients, and they reported that all methods have equivalent results,60 which contradicted our findings. The differences may be attributed to the time interval for questionnaire administration. The time interval between baseline and the follow-up questionnaire was 8 weeks in their study, and it was only 1 week in our study, which may have affected the ability to recall information. Moreover, we cannot conclusively state that the present findings are applicable to adult patients providing their own care as compared to parents providing care to their children.
Overall, the findings of the present study showed that parents in the intervention group were satisfied about the storybook. Almost all parents found the storybook as an educational resource with useful information that improved their understanding of the importance of regular dental checkups. All parents believed that the storybook explained the procedure of seeing the dentist in a straightforward manner that was easy to follow and comprehend for their children. Furthermore, the majority of parents found that the storybook was useful in lowering dental anxiety in their children and in helping them accept dental visits.
Parental oral health knowledge has been reported by many authors to be considerably affected by sociodemographic characteristics.61–63 However, in the present study, there were no differences in the total knowledge score across parents with various background characteristics, which may have been attributed to the homogenous sample in the present study because we recruited parents seeking dental treatment for their children at a governmental hospital. Moreover, our findings were consistent with other studies that did not find any relationships between parental sociodemographic characteristics and levels of oral health knowledge.24,26,51
The present study had several limitations. First, the short interval time between the storybook administration and the follow-up questionnaires may have affected the retention of information. It would be interesting to study the knowledge level over a longer period of time. However, due to the COVID-19 pandemic, long-term retention of information was unattainable. Moreover, we were unable to assess whether the storybook improves the oral health practices of parents and children. Thus, a long-term follow-up should be completed to determine permanent changes in practice habits. Finally, because the cohort of the present study consisted of parents who could speak Arabic and were seeking dental treatment at King Saud University, our results cannot be generalized to other populations.
Despite the abovementioned limitations, the present study also had strengths. To the best of our knowledge, this is the first study to determine the effect of a dental storybook on parents’ knowledge about oral health and to assess the parental perception of the storybook in improving their oral health knowledge and in reducing dental anxiety levels among their children in the form of a RCT with blinding, which made the study groups more comparable and minimized bias and confounding. Moreover, the design and simple language used in the storybook fulfilled its value as a valuable information tool regarding parental oral health education.
Further research is needed to elucidate the long-term effects of various tools of information and to determine whether the improved oral health knowledge contributes to better oral health outcomes.
Conclusion
The dental storybook is a suitable tool to impart oral health information and is considerably effective for short-term improvement of parental oral health knowledge.
Additionally, parents perceived it as a useful source of information, and an effective tool in improving their oral health knowledge and reducing dental anxiety levels among their children.
Data Sharing Statement
The datasets used and analysed during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The present study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board (E-18-3190). The study protocol received institutional approval from the Ethics Committee of the College of Dentistry Research Center (CDRC) of King Saud University in Riyadh, Saudi Arabia (number PR 0104). Informed consent was obtained from all the subjects involved in the study.
Acknowledgments
The authors would like to express their gratitude to the children and their families who participated in this research. We would also like to thank the staff at the Department of Pediatric Dentistry for their assistance and contributions.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. Br Dent J. 2016;221(12):792–793. doi:10.1038/sj.bdj.2016.953
2. BaniHani A, Deery C, Toumba J, Munyombwe T, Duggal M. The impact of dental caries and its treatment by conventional or biological approaches on the oral health-related quality of life of children and carers. Int J Paediatr Dent. 2018;28(2):266–276. doi:10.1111/ipd.12350
3. Okada M, Kawamura M, Kaihara Y, et al. Influence of parents’ oral health behaviour on oral health status of their school children: an exploratory study employing a causal modelling technique. Int J Paediatr Dent. 2002;12(2):101–108. doi:10.1046/j.1365-263X.2002.00338.x
4. Wong D, Perez-Spiess S, Julliard K. Attitudes of Chinese parents toward the oral health of their children with caries: a qualitative study. Pediatr Dent. 2005;27(6):505–512.
5. Hobdell M, Petersen PE, Clarkson J, Johnson N. Global goals for oral health 2020. Int Dent J. 2003;53(5):285–288. doi:10.1111/j.1875-595X.2003.tb00761.x
6. Dye Bruce A, Xianfen L, Thornton-Evans G. Oral health disparities as determined by selected healthy people 2020 oral health objectives for the United States, 2009–2010. No. 100. US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2012.
7. Anil S, Anand PS. Early childhood caries: prevalence, risk factors, and prevention. Front Pediatr. 2017;5:157. doi:10.3389/fped.2017.00157
8. Lewis CW. Teeth: small but mighty and mighty important. A comprehensive review of children’s dental health for primary care clinicians. Curr Pediatr Rev. 2020;16(3):215–231. doi:10.2174/1573396316666200228093248
9. Prabhu A, Rao AP, Reddy V, Ahamed SS, Muhammad S, Thayumanavan S. Parental knowledge of pre-school child oral health. J Community Health. 2013;38(5):880–884. doi:10.1007/s10900-013-9693-x
10. ElKarmi R, Shore E, O’Connell A. Knowledge and behaviour of parents in relation to the oral and dental health of children aged 4–6 years. Eur Arch Paediatr Dent. 2015;16(2):199–204. doi:10.1007/s40368-014-0155-7
11. Johnston R, Fowler C, Wilson V, Kelly M. Opportunities for nurses to increase parental health literacy: a discussion paper. Issues Compr Pediatr Nurs. 2015;38(4):266–281. doi:10.3109/01460862.2015.1074318
12. Gussy MG, Waters EB, Riggs EM, Lo SK, Kilpatrick NM. Parental knowledge, beliefs and behaviours for oral health of toddlers residing in rural Victoria. Aust Dent J. 2008;53(1):52–60. doi:10.1111/j.1834-7819.2007.00010.x
13. Ashkanani F, Al-Sane M. Knowledge, attitudes and practices of caregivers in relation to oral health of preschool children. Med Princ Pract. 2013;22(2):167–172. doi:10.1159/000341764
14. Chala S, Houzmali S, Abouqal R, Abdallaoui F. Knowledge, attitudes and self-reported practices toward children oral health among mother’s attending maternal and child’s units, Salé, Morocco. BMC Public Health. 2018;18(1):1–8. doi:10.1186/s12889-018-5542-2
15. Al-Tamimi S, Petersen PE. Oral health situation of schoolchildren, mothers and schoolteachers in Saudi Arabia. Int Dent J. 1998;48(3):180–186. doi:10.1111/j.1875-595X.1998.tb00475.x
16. Oliveira ER, Narendran S, Williamson D. Oral health knowledge, attitudes and preventive practices of third grade school children. Pediatr Dent. 2000;22(5):395–400.
17. Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX. Oral health knowledge, attitudes and behaviour of children and adolescents in China. Int Dent J. 2003;53(5):289–298. doi:10.1111/j.1875-595X.2003.tb00762.x
18. Prasai Dixit L, Shakya A, Shrestha M, Shrestha A. Dental caries prevalence, oral health knowledge and practice among indigenous Chepang school children of Nepal. BMC Oral Health. 2013;13(1):1–5. doi:10.1186/1472-6831-13-20
19. Al-Darwish MS. Oral health knowledge, behaviour and practices among school children in Qatar. Dent Res J (Isfahan). 2016;13(4):342. doi:10.4103/1735-3327.187885
20. Al-Asfour A, Andersson L. The effect of a leaflet given to parents for first aid measures after tooth avulsion. Dent Traumatol. 2008;24(5):515–521. doi:10.1111/j.1600-9657.2008.00651.x
21. Oshagh M, Danoei SM, Ghahremoni Y, Pojuhi N, Boushehri SG. Impact of an educational leaflet on parents’ knowledge and awareness of children’s orthodontic problems in Shiraz. problems in Shiraz. EMHJ. 2011;17(2):121–125. doi:10.26719/2011.17.2.121
22. Danaei SM, Faghihi F, Golkari A, Saki M. The impact of an educational pamphlet on the awareness of parents about 4–6-year-old children’s oral habits and dentofacial discrepancies. J Dent Res Dent Clin Dent Prospects. 2016;10(1):57. doi:10.15171/joddd.2016.009
23. Brown RM, Canham D, Cureton VY. An oral health education program for Latino immigrant parents. J Sch Nurs. 2005;21(5):266–271. doi:10.1177/10598405050210050401
24. Rothe V, Kebriaei A, Pitner S, Balluff M, Salama F. Effectiveness of a presentation on infant oral health care for parents. Int J Paediatr Dent. 2010;20(1):37–42. doi:10.1111/j.1365-263X.2009.01018.x
25. Amin M, Nyachhyon P, Elyasi M, Al-Nuaimi M. Impact of an oral health education workshop on parents’ oral health knowledge, attitude, and perceived behavioral control among African immigrants. J Oral Dis. 2014;2014:1–7. doi:10.1155/2014/986745
26. Verlinden DA, Schuller AA, Verrips GH, Reijneveld SA. Effectiveness of a short web-based film targeting parental oral health knowledge in a well-child care setting. Eur J Oral Sci. 2020;128(3):226–232. doi:10.1111/eos.12700
27. Halawany HS, Al Badr A, Al Sadhan S, et al. Effectiveness of oral health education intervention among female primary school children in Riyadh, Saudi Arabia. Saudi Dent J. 2018;30(3):190–196. doi:10.1016/j.sdentj.2018.04.001
28. Reinhardt CH, Löpker N, Noack MJ, Rosen E, Klein K. Peer teaching pilot programme for caries prevention in underprivileged and migrant populations. Int J Paediatr Dent. 2009;19(5):354–359. doi:10.1111/j.1365-263X.2009.00982.x
29. Tolvanen M, Lahti S, Poutanen R, Seppä L, Pohjola V, Hausen H. Changes in children’s oral health-related behavior, knowledge and attitudes during a 3.4-yr randomized clinical trial and oral health-promotion program. Eur J Oral Sci. 2009;117(4):390–397. doi:10.1111/j.1600-0722.2009.00640.x
30. Yazdani R, Vehkalahti MM, Nouri M, Murtomaa H. School-based education to improve oral cleanliness and gingival health in adolescents in Tehran, Iran. Int J Paediatr Dent. 2009;19(4):274–281. doi:10.1111/j.1365-263X.2009.00972.x
31. Poutanen R, Lahti S, Tolvanen M, Hausen H. Parental influence on children’s oral health-related behavior. Acta Odontol Scand. 2006;64(5):286–292. doi:10.1080/00016350600714498
32. Salama F, Alwohaibi A, Alabdullatif A, Alnasser A, Hafiz Z. Knowledge, behaviours and beliefs of parents regarding the oral health of their children. Eur Arch Paediatr Dent. 2020;21(2):103–109. doi:10.23804/ejpd.2020.21.02.03
33. Firmino RT, Ferreira FM, Martins CC, Granville-Garcia AF, Fraiz FC, Paiva SM. Is parental oral health literacy a predictor of children’s oral health outcomes? Systematic review of the literature. Int J Paediatr Dent. 2018;28(5):459–471. doi:10.1111/ipd.12378
34. Jones M, Lee JY, Rozier RG. Oral health literacy among adult patients seeking dental care. J Am Dent Assoc. 2007;138(9):1199–1208. doi:10.14219/jada.archive.2007.0344
35. Miller E, Lee JY, DeWalt DA, Vann WF. Impact of caregiver literacy on children’s oral health outcomes. Pediatrics. 2010;126(1):107–114. doi:10.1542/peds.2009-2887
36. Merdad L, El-Housseiny AA. Do children’s previous dental experience and fear affect their perceived oral health-related quality of life (OHRQoL)? BMC Oral Health. 2017;17(1):47. doi:10.1186/s12903-017-0338-9
37. AAPD 2021. American academy of pediatric dentistry. Behavior guidance for the pediatric dental patient. In: The Reference Manual of Pediatric Dentistry. Chicago, Ill: American Academy of Pediatric Dentistry; 2021:306–324.
38. Bandura A. Social learning theory of aggression. J Comm. 1978;28(3):12–29. doi:10.1111/j.1460-2466.1978.tb01621.x
39. Olumide F, Newton JT, Dunne S, Gilbert DB. Anticipatory anxiety in children visiting the dentist: lack of effect of preparatory information. Int J Paediatr Dent. 2009;19(5):338–342. doi:10.1111/j.1365-263X.2009.00980.x
40. Leventhal H, Johnson JE. Laboratory and field experimentation: development of a theory of self-regulation. Behav Sci Nurs Theor. 1983;1983:189–262.
41. Johnson JE. Self-regulation theory and coping with physical illness. Res Nurs Health. 1999;22(6):435–448. doi:10.1002/(SICI)1098-240X(199912)22:6<435::AID-NUR2>3.0.CO;2-Q
42. Fox C, Newton JT. A controlled trial of the impact of exposure to positive images of dentistry on anticipatory dental fear in children. Community Dent Oral Epidemiol. 2006;34(6):455–459. doi:10.1111/j.1600-0528.2006.00303.x
43. Moura B, Imparato JCP, Parisotto T, Benedetto M. Child’s anxiety preceding the dental appointment: evaluation through a playful tool as a conditioning feature. RGO-Revista Gaúcha de Odontologia. 2015;63(4):455–460. doi:10.1590/1981-863720150003000122848
44. Alsaadoon AM, Sulimany AM, Hamdan HM, Murshid EZ. The use of a dental storybook as a dental anxiety reduction medium among pediatric patients: a randomized controlled clinical trial. Children. 2022;9(3):328. doi:10.3390/children9030328
45. Daabiss M. American Society of Anaesthesiologists physical status classification. Indian J Anaesth. 2011;55(2):111. doi:10.4103/0019-5049.79879
46. American Academy of Pediatric Dentistry. Periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. Pediatr Dent. 2018;40(6):194–204.
47. Faul F, Erdfelder E, Lang AG, Buchner A. G* Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
48. Ghaderi F, Adl A, Ranjbar Z. Effect of a leaflet given to parents on knowledge of tooth avulsion. Eur J Paediatr Dent. 2013;14(1):13–16.
49. Alsada LH, Sigal MJ, Limeback H, Fiege J, Kulkarni GV. Development and testing of an audio-visual aid for improving infant oral health through primary caregiver education. J Can Dent Assoc. 2005;71(4):241.
50. Kaste LM, Sreenivasan D, Koerber A, Punwani I, Fadavi S. Pediatric oral health knowledge of African American and Hispanic of Mexican origin expectant mothers. Pediatr Dent. 2007;29(4):287–292.
51. Bates SB, Riedy CA. Changing knowledge and beliefs through an oral health pregnancy message. J Public Health Dent. 2012;72(2):104–111. doi:10.1111/j.1752-7325.2011.00289.x
52. Dickinson AO. Concepts in dental public health; 2005.
53. Johnson A, Sandford J. Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home: systematic review. Health Educ Res. 2005;20(4):423–429. doi:10.1093/her/cyg141
54. McGuire WJ. Public communication as a strategy for inducing health-promoting behavioral change. Prev Med. 1984;13(3):299–319. doi:10.1016/0091-7435(84)90086-0
55. Dowse R, Ehlers MS. Pictograms in pharmacy. Int J Pharm Pract. 1998;6(2):109–118. doi:10.1111/j.2042-7174.1998.tb00924.x
56. Arora A, McNab MA, Lewis MW, Hilton G, Blinkhorn AS, Schwarz E. ‘I can’t relate it to teeth’: a qualitative approach to evaluate oral health education materials for preschool children in New South Wales, Australia. Int J Paediatr Dent. 2012;22(4):302–309. doi:10.1111/j.1365-263X.2011.01195.x
57. Arora A, Al-Salti I, Murad H, et al. Adaptation of child oral health education leaflets for Arabic migrants in Australia: a qualitative study. BMC Oral Health. 2018;18(1):1–10. doi:10.1186/s12903-017-0469-z
58. Sansgiry SS, Cady PS, Adamcik BA. Consumer comprehension of information on over-the-counter medication labels: effects of picture superiority and individual differences based on age. J Pharm Mark Manage. 1997;11(3):63–76.
59. Cohen G, Forbes J, Garraway M. Can different patient satisfaction survey methods yield consistent results? Comparison of three surveys. BMJ. 1996;313(7061):841–844. doi:10.1136/bmj.313.7061.841
60. Lees A, Rock WP. A comparison between written, verbal, and videotape oral hygiene instruction for patients with fixed appliances. J Orthod. 2014;27:323–328.
61. Williams NJ, Whittle JG, Gatrell AC. The relationship between socio-demographic characteristics and dental health knowledge and attitudes of parents with young children. Br Dent J. 2002;193(11):651–654. doi:10.1038/sj.bdj.4801652
62. Llena C, Nakdali T, Sanz JL, Forner L. Oral health knowledge and related factors among pregnant women attending to a primary care center in Spain. Int J Environ Res Public Health. 2019;16(24):5049. doi:10.3390/ijerph16245049
63. Alshammari FS, Alshammari RA, Alshammari MH, Alshammari MF, Alibrahim AK. Parental awareness and knowledge toward their children’s oral health in the city of Dammam, Saudi Arabia. J Clin Pediatr Dent. 2021;14(1):100. doi:10.5005/jp-journals-10005-1894
64. Schulz KF, Altman DG, Moher D; CONSORT Group. Statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251. doi:10.1371/journal.pmed.1000251
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.