")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 11
Immunotherapy for HER2-positive breast cancer: recent advances and combination therapeutic approaches
Authors Ayoub NM , Al-Shami KM , Yaghan RJ
Received 6 November 2018
Accepted for publication 12 December 2018
Published 17 January 2019 Volume 2019:11 Pages 53—69
DOI https://doi.org/10.2147/BCTT.S175360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Nehad M Ayoub,1 Kamal M Al-Shami,2 Rami J Yaghan3
1Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology (JUST), Irbid, Jordan; 2Department of Drug Discovery and Development, Harrison School of Pharmacy, Auburn University, Auburn, AL, USA; 3Department of General Surgery and Urology, Faculty of Medicine, Jordan University of Science and Technology (JUST), Irbid, Jordan
Abstract: Cancer immunotherapy has evolved dramatically with improved understanding of immune microenvironment and immunosurveillance. The immunogenicity of breast cancer is rather heterogeneous. Specific subtypes of breast cancer such as estrogen receptor (ER)-negative, human EGF receptor 2 (HER2)-positive, and triple-negative breast cancer (TNBC) have shown evidence of immunogenicity based on tumor–immune interactions. Several preclinical and clinical studies have explored the potential for immunotherapy to improve the clinical outcomes for different subtypes of breast cancer. This review describes the immune microenvironment of HER2-positive breast cancer and summarizes recent clinical advances of immunotherapeutic treatments in this breast cancer subtype. The review provides rationale and ongoing clinical evidence to the use of immune checkpoint inhibitors, therapeutic vaccines, and adoptive T cell immunotherapy in breast cancer. In addition, the present paper describes the most relevant clinical progress of strategies for the combination of immunotherapy with standard treatment modalities in HER2-positive breast cancer including chemotherapy, targeted therapy, and radiotherapy.
Keywords: immunotherapy, breast cancer, HER2, checkpoint inhibitors, vaccines
Background
Role of immune microenvironment in cancer
Immune cells represent a major component of the tumor microenvironment.1 Immune elements infiltrating the tumor microenvironment include macrophages, natural killer (NK) cells, dendritic cells (DCs), and adaptive immune cells.1,2 The role of immune system in cancer development and progression is described through immunoediting.3 The concept of tumor immunoediting is represented by three phases designated as elimination, equilibrium, and escape.3 The elimination phase implies a process known as tumor immune surveillance, whereby immune system identifies cancerous cells and eliminates them preventing tumor growth.3 In the equilibrium phase, sporadic tumor cells that have escaped immune attack during elimination remain dormant and a temporary state of equilibrium develops between immune system and cancer cells. During this period, immune system will exert a selective pressure to eliminate susceptible tumor cells. However, cancer cells that acquire resistance to antitumor immune response enter the escape phase and continue to grow allowing tumors to develop aggressively.3 Host antitumor immune responses are predominantly mediated via cellular immunity in which CD8+ cytotoxic T lymphocytes (CTLs) are considered the cornerstone cellular element in anticancer immunity.4,5 Activated CTLs exert antitumor effects by secreting interferon gamma (IFN-γ) and tumor necrosis factor alpha (TNF-α) along with other cytotoxins.4,6,7 In this regard, prevention of tumor growth and development is determined, in part, by the number of CTLs invading through the tumor microenvironment and the ability of CTLs to recognize tumor-associated antigens (TAAs).4 Other anti-oncogenic effects of immune system have been mediated through the activation of macrophages, NK cells, and CD4+ T helper (Th) 1 cells.2
A hallmark of cancers is the ability to evade the immune system through tumor-mediated immune escape mechanisms.2 Tumors avoid recognition by immune system through multiple mechanisms including the downregulation of components of antigen processing and presentation machinery leading to loss of major histocompatibility complex (MHC) class I protein expression, low human leukocyte antigen (HLA) class I expression, and defects in T cell receptor (TCR) signaling.6,8 In addition, growing tumors can avoid destruction by immune system through recruitment of immunosuppressive elements such as regulatory T cells (Tregs), myeloid-derived suppressor cells (MDSCs), and tumor-associated macrophages.6,8,9 These immune cells can suppress the actions of CTLs promoting tumor growth.10 Furthermore, growing cancer cells have been shown to enhance the production of immunosuppressive cytokines within the tumor microenvironment such as TGF-β and IL-10 to escape immune attack.8,9 Advancements in immunotherapy research have revealed a key immune evasion mechanism through the utilization of immune checkpoints by tumor cells to suppress the cellular immune response and promote immune tolerance.2,8 Therefore, immunotherapeutic interventions are directed to enhance tumor recognition by immune system and augment CTL activity.
Breast cancer is a heterogeneous disease with a high degree of diversity between and within tumors.11 Comprehensive gene expression profiling classifies breast tumors into three major molecular subtypes: luminal, human EGF receptor 2 (HER2)-positive, and basal-like cancers.12,13 Recently, growing evidence is supporting the immunogenic potential of specific breast cancer subtypes.14,15 Immunogenic nature of breast cancer was illustrated by the identification of tumor-infiltrating lymphocytes (TILs) in breast tumors.15,16 Analysis of breast tumor samples had demonstrated higher level of TILs among patients harboring HER2-positive and triple-negative breast cancer (TNBC) than hormone-dependent subtypes.17–19 Analysis of TILs in a large cohort of breast cancer patients indicated that the presence of CD8+ T cells is associated with a lower risk of mortality in estrogen receptor (ER)-negative and ER-positive/HER2-positive tumors.14,20 However, the presence of CD8+ infiltrates was not associated with survival advantage for patients harboring ER-positive tumors. In the same study, Tregs that are characterized by FOXP3-positive expression were not associated with a prognostic impact among the different subsets of breast tumors evaluated.14,20 Intra-tumoral CD4+ T cell number has been found to positively correlate with advanced tumor stages, large tumor size, positive lymph node status, and HER2 expression in breast cancer patients.21 In addition, CD4+ TILs in breast cancer patients were positively correlated with FOXP3-positive Tregs. The CD4/CD8 ratios were negatively correlated with overall survival (OS) and relapse-free survival in breast cancer patients.21
HER2-positive breast cancer and the immune system
HER2 is a transmembrane tyrosine kinase receptor and a member of the ErbB protein family.22 Amplification of the HER2/neu oncogene located on chromosome 17q12 is the primary pathway of HER2 receptor overexpression, which is the hallmark of HER2-positive or enriched breast tumors.23 HER2 is amplified in 20%–30% of invasive breast cancers.22–24 Overexpression of HER2 is an adverse prognostic factor that is associated with breast tumors of aggressive phenotype, poor survival, and increased risk of disease recurrence.23 The introduction of HER2-directed therapy had revolutionized the treatment of HER2-positive breast cancer. Trastuzumab, a humanized monoclonal antibody, is the prototype HER2-directed therapy that was introduced in the late 1990s for the management of HER2-positive breast cancer.25–27 The combination of trastuzumab with chemotherapy is the standard treatment for HER2-positive breast cancer in the current practice.28,29 Trastuzumab binding to the extracellular domain of HER2 has been shown to prevent receptor dimerization, increase receptor degradation, and inhibit receptor shedding.24 Collectively, these actions inhibit RAS-MAPK and PI3K-AKT-mTOR signaling pathways leading to the suppression of cancer cell proliferation and growth.30 In addition, trastuzumab activity has been found to be mediated through antibody-dependent cellular cytotoxicity (ADCC) as demonstrated by the recruitment of immune cells to HER2-overexpressing breast cancers.24,30 Other HER2-directed therapies approved for clinical use include the monoclonal antibody pertuzumab, the small molecule kinase inhibitor lapatinib, and the toxin-carrying antibody trastuzumab emtansine (T-DM1).31–33 Despite the fact that HER2-targeted therapy had improved treatment outcomes in breast cancer patients, several challenges of clinical relevance have been identified. Efficacy of trastuzumab therapy in combination with chemotherapy peaks at 40%–60% of breast cancer patients.34 In addition, disease relapse has been reported in 15%–20% of patients with HER2-positive locoregional breast cancer after adequate treatment in both neoadjuvant and adjuvant settings.35 Furthermore, pharmacological resistance to trastuzumab and other HER2-directed therapies is of particular importance as it adversely affects treatment outcomes.34,36 Therefore, the development of newer therapies and novel approaches is of utmost importance to overcome limitations to targeted therapy and improve treatment outcomes in HER2-overexpressing breast cancer.
Different types of infiltrating immune cells have been clinically identified in HER2-positive breast tumors. Infiltrating immune cells have distinct prognostic and predictive significance. TILs have consistently shown a positive prognostic association in HER2-positive breast cancer patients.17,37,38 Higher levels of TILs were associated with good prognosis in terms of improved survival and response to therapy as well as higher rates of pathological complete response (pCR).17,38,39 The FinHER trial was the first to demonstrate an association between higher levels of TILs and improved response to trastuzumab among HER2-positive breast cancer patients.40 In this regard, Alexe et al41 demonstrated that strong expression of lymphocyte-associated genes was associated with reduced recurrence rates among HER2-positive breast cancer patients. In a retrospective analysis of data generated from CLEOPATRA study, Luen et al42 found that greater TIL infiltration was significantly associated with improved OS among breast cancer patients with advanced HER2-positive disease treated with docetaxel, trastuzumab, and pertuzumab or placebo. These findings were further confirmed by the NeoALTTO trial in which the presence of TILs at diagnosis was associated with higher rates of pCR and event-free survival (EFS) in early-stage HER2-positive patients treated with lapatinib and trastuzumab.37 Alternatively, increased fraction of Tregs in HER2-positive tumors was associated with advanced clinical stages, lower pCR rate, shorter disease-free survival (DFS), and reduced OS.43,44 Furthermore, increased levels of circulating Tregs have been found to contribute to increased metastatic potential of HER2-positive breast cancer through suppressing CTL response.45,46
Collectively, these findings suggest that HER2-positive breast cancer can be targeted by immunotherapeutic interventions. This review discusses the different immunotherapeutic strategies that have been developed or being assessed in clinical trials in breast cancer, particularly the HER2-positive subtype. The review also describes the potentials for combined treatment of immunomodulating agents with other available treatments for HER2-postive breast cancer.
Immunotherapy of HER2-positive breast cancer
The goal of cancer immunotherapy is to restore the ability of the immune system to detect and eliminate cancer cells by overcoming the mechanisms by which tumors escape immune response.47,48 Although the majority of immune-based therapeutic strategies have relied on passive immunity through the administration of antibodies with direct antitumor activity, there is a growing interest in evolving active immunotherapeutic modalities aiming at boosting host immune system ability to detect and destroy cancerous and precancerous cells.47,49 This part discusses recent clinical progress of immune checkpoint blockade therapies, therapeutic cancer vaccines, and adoptive T cell transfer immunotherapy as immunotherapeutic approaches in breast cancer.
Immune checkpoint inhibitors
Immune checkpoints represent a plethora of immune system inhibitory pathways.50 Under normal physiological conditions, immune checkpoints regulate immune response to promote self-tolerance and prevent autoimmunity.51 Immunosuppressive pathways are often activated by cancer cells to escape immune detection and subsequent antitumor response and elimination.50 Blockade of these immune checkpoints with monoclonal antibodies has been shown to restore the activity of cell-mediated immunity and promote antitumor response (Figure 1). Immune checkpoint inhibitors have been approved for the treatment of melanoma and renal cell carcinoma.5,7,52,53 Given the immunogenic potential of HER2-positive breast cancer, the role of immune checkpoint inhibitors has been investigated.4,5,7,52,53
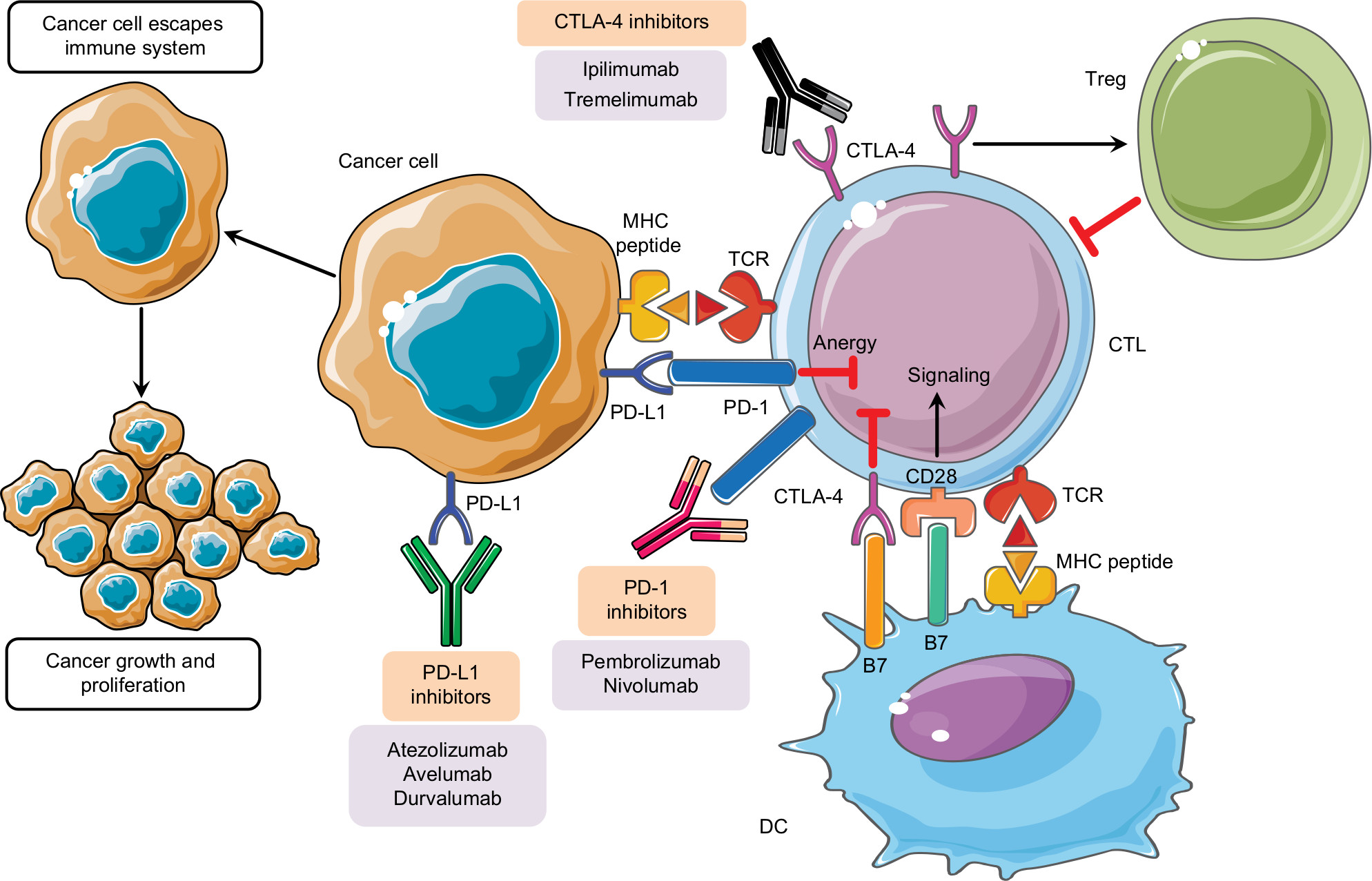 | Figure 1 Immune checkpoint inhibitors in cancer treatment. Notes: Inability to activate CTLs in tumor microenvironment through the suppressive effect of Tregs or through immune checkpoints allows cancer cells to escape immune attack, survive, and grow. B7 ligands expressed on antigen-presenting cells bind to CD28 receptor on CTL leading to T cell amplification and immune response. Alternatively, binding of B7 ligands to CTLA-4 expressed on T cells suppresses their activity. CTLA-4 also enhances the activity of Tregs leading to immunosuppressive activity. PD-1 is expressed on activated T cells. PD-1 binds to its PD-L1 leading to the anergy of CTLs further promoting inhibitory signals. Pharmacological inhibition of immune checkpoints with monoclonal antibodies restores CTL antitumor activity and relieves immunosuppression. Abbreviations: CTLA-4, cytotoxic T-lymphocyte antigen 4; CTLs, cytotoxic T lymphocytes; DC, dendritic cell; MHC, major histocompatibility complex; PD-1, programmed cell death-1; PD-L1, programmed cell death-1 ligand; TCR, T cell receptor; Tregs, regulatory T cells. |
Cytotoxic T-lymphocyte antigen 4 (CTLA-4) blockade
CTLA-4 is a key inhibitory receptor expressed on effector T cells.54 Surface expression of CTLA-4 is upregulated after T cell activation to provide feedback inhibition of the immune response.54 Regularly, the activation and proliferation of T cells are driven by the interaction between the costimulatory receptor CD28 expressed on T cells with its ligands expressed on antigen-presenting cells.55 CTLA-4 and CD28 are highly homologous and compete for the binding to B7 ligands (B7-1 and B7-2) on antigen-presenting cells.56 Binding of B7 ligands to CD28 receptor on effector T cells promotes T cell amplification and immune response mediated by specific cytokines and chemokines essential for T cell activation.54–57 On the contrary, binding of B7 ligands to CTLA-4 suppresses T cell activity and aborts further immune response.54,57 In addition to down-modulating the activity of effector T cells, CTLA-4 has been found to promote the function of Tregs, thus enhancing their immunosuppressive activity.58 Blockade of CTLA-4 with specific antibodies relieves immunosuppression and enhances the antitumor activity of effector T cells (Figure 1).4,59,60 Ipilimumab was the first therapeutic immune checkpoint inhibitor targeting CTLA-4.61 This drug is a human monoclonal antibody approved by the US Food and Drug Administration (US FDA) for the treatment of metastatic melanoma patients.61 Tremelimumab is another CTLA-4 human monoclonal antibody currently under clinical investigations in the management of mesothelioma.62
There are few published reports on the use of CTLA-4 inhibitors in breast cancer. Ipilimumab was evaluated with or without cryoablation in early-stage breast cancer patients.63 Nineteen patients were included in this study in which two patients had HER2-positive disease.63 Findings showed a favorable increase in the proportion of activated effector T cells among patients receiving ipilimumab treatment alone or in combination with cryoablation. The combination treatment also showed a modest increase in the ratio of intratumoral T effector cells relative to Tregs.63 In addition, ipilimumab was well tolerated when administered alone or in combination with cryoablation in which all patients reached the primary end point of the study with no reported grade III or IV adverse events (AEs) associated with treatment.63 Rash, diarrhea, and fatigue were the most frequently reported treatment-related AEs. Tremelimumab was evaluated in combination with exemestane in hormone-dependent breast cancer patients with advanced disease.64 The study included 26 patients who were characterized for the status of hormone receptor expression but not for HER2. Combination treatment stabilized the disease in 42% of patients for a minimum of 12 weeks. Immunologically, tremelimumab and exemestane improved the ratio of effector T cells to Tregs and enhanced T cell activation among patients with advanced breast cancer.64 This combination of tremelimumab and exemestane was tolerable. Most AEs were mild to moderate grade I/II, with no grade IV AEs being reported. Diarrhea was the most frequently reported treatment-related AE. Other AEs were pruritus, constipation, and fatigue.64 Multiple ongoing clinical trials are assessing the therapeutic effect of CTLA-4 inhibitors in different breast cancer subtypes and settings. These trials are summarized in Table 1.
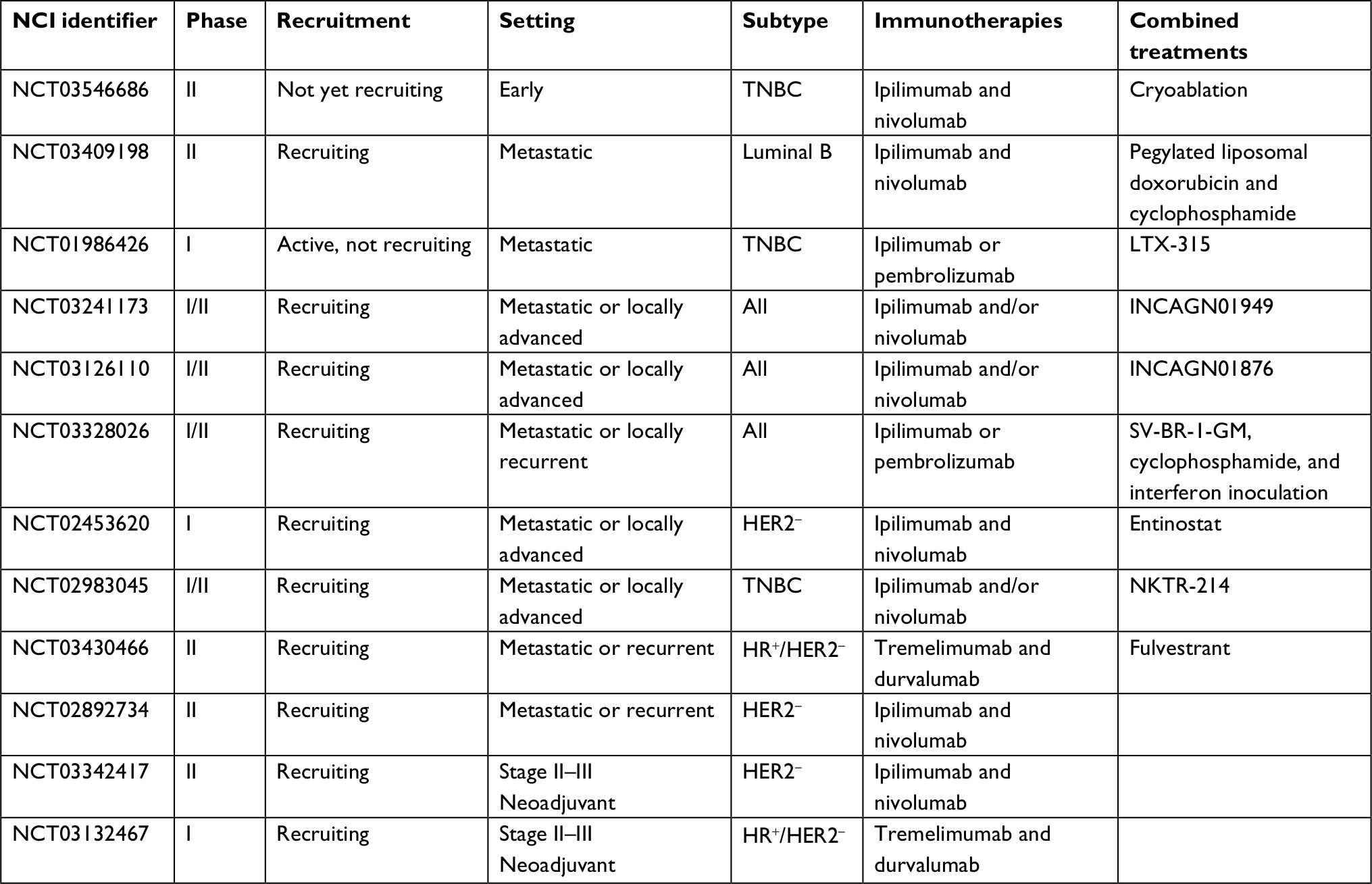 | Table 1 Ongoing clinical trials of CTLA-4 inhibitor immunotherapeutics in breast cancer Abbreviations: CTLA-4, cytotoxic T-lymphocyte antigen 4; HER2, human EGF receptor 2; HR, hormone receptor; TNBC, triple-negative breast cancer. |
Programmed cell death-1 (PD-1)/programmed cell death-1 ligand (PD-L1) blockade
PD-1 is a member of the CD28 superfamily that is expressed on activated T cells.65 PD-1 binds to its ligands, PD-L1 and PD-L2, delivering inhibitory signals leading to decreased cytokine production and cytolytic activity of T cells.65 PD-L1 has wide tissue expression and is the main contributor to the inhibitory signals that attenuate T cell activation leading to immune tolerance.66 As such, multiple immunotherapeutic agents blocking the PD-1/PD-L1 axis have been approved to enhance antitumor immune response (Figure 1). Pembrolizumab and nivolumab are monoclonal antibodies against PD-1 which have been approved by the US FDA in 2014 for the treatment of patients with metastatic melanoma.67,68 Both antibodies inhibit the interaction between PD-1 receptor and its ligand, thus restoring antitumor immunity.67,68 Nivolumab approval has been recently expanded to include metastatic non-small-cell lung cancer (NSCLC), advanced renal cell carcinoma, and classical Hodgkin lymphoma.69–71 PD-L1-targeting antibodies include atezolizumab, avelumab, and durvalumab. Atezolizumab has been approved for the treatment of metastatic NSCLC and advanced urothelial carcinoma, while avelumab has gained recent approval for the treatment of metastatic Merkel cell carcinoma.72 Durvalumab was recently approved for the treatment of patients with locally advanced or metastatic urothelial carcinoma who have disease progression during or following chemotherapy as well as patients with locally advanced, unresectable stage III NSCLC.73,74 Ghebeh et al75 demonstrated the increased expression of PD-L1 in breast cancer specimens as well as TILs. The expression of PD-L1 has been associated with unfavorable clinicopathologic features such as large tumor size, high tumor grade, lack of hormone receptor expression, and HER2-positive status.75 In a Phase Ib study, pembrolizumab was well tolerated and resulted in a modest but durable overall response in a subset of patients with advanced, PD-L1-positive, ER-positive/HER2-negative breast cancer.76 Nausea and fatigue were the most common treatment-related AEs and were mainly grade I/II. In addition, pembrolizumab and atezolizumab had shown acceptable toxicity profile and modest activity among TNBC patients in Phase I clinical trials.77–79 In the JAVELIN Solid Tumor study, avelumab has been tested in 168 patients with metastatic breast cancer; in which 26 patients (15.5%) had HER2-positive breast cancer disease, 72 patients (42.9%) had hormone receptor-positive disease, and 58 patients (34.5%) had TNBC.80 Overall, avelumab was well tolerated in which fatigue, nausea, and infusion-related reactions were most commonly encountered AEs. The overall objective response rate (ORR) was 3%; however, avelumab produces better clinical activity among patients with positive expression of PD-L1 and among patients with TNBC.80 Currently ongoing clinical trials of PD-1/PD-L1 checkpoint inhibitors in breast cancer are summarized in Table 2.
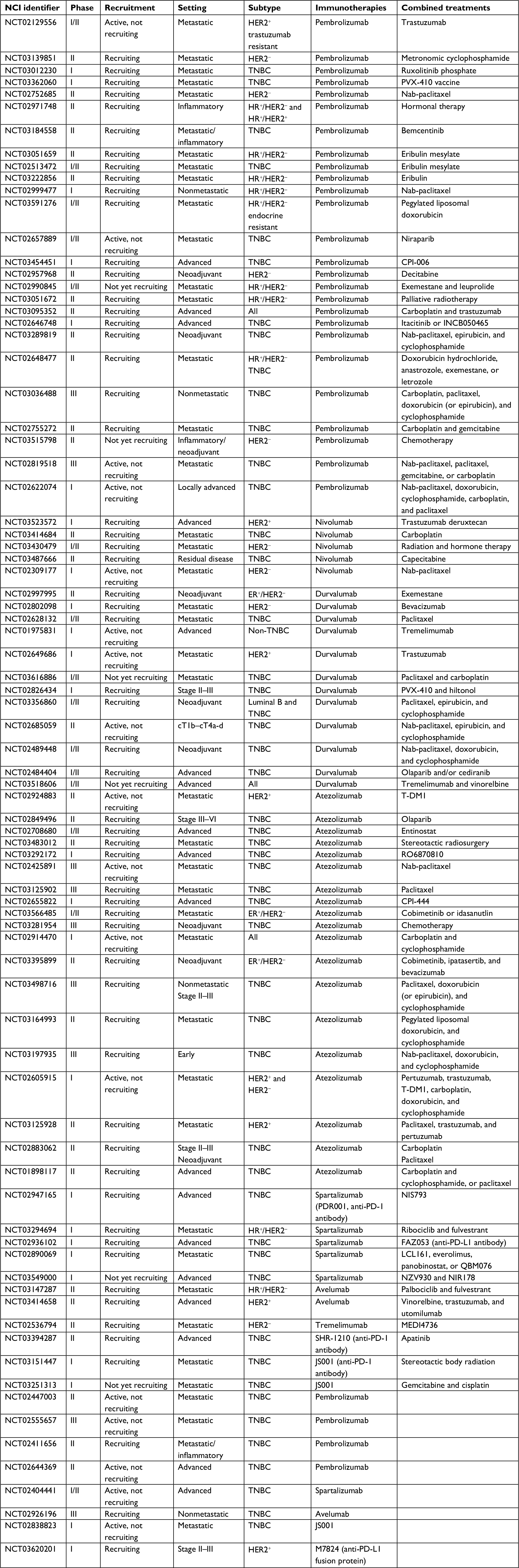 | Table 2 Ongoing clinical trials of PD-1/PD-L1 immunotherapeutics in breast cancer Abbreviations: ER, estrogen receptor; HER2, human EGF receptor 2; HR, hormone receptor; T-DM1, trastuzumab emtansine; TNBC, triple-negative breast cancer. |
Therapeutic cancer vaccines
Therapeutic cancer vaccines are intended to treat existing tumors by enhancing antitumor immune response.81 Cancer vaccine strategies utilize specific tumor antigen-derived peptides, proteins, DNA, RNA, and whole tumor and DC lysates.82,83 Cancer vaccines are expected to induce strong immunity by stimulating immune regulators such as antibodies, Th cells, and CTLs, thus establishing immunological memory and preventing tumor recurrence.10,84 Multiple breast cancer-specific TAAs have been identified including HER2, mucin 1 (MUC1), carcinoembryonic antigen (CEA), human telomerase reverse transcriptase (hTERT), Wilms tumor gene (WT1), and mammaglobin-A (MAM-A).2,85
Nelipepimut-S (E75 peptide)
HER2/nue is a remarkable therapeutic target for peptide-based cancer vaccines. HER2/neu drives oncogenic potential, and its expression on the surface of HER2-overexpressing breast carcinomas can be up to 50-fold higher than its expression on normal cells.85–87 Nelipepimut-S (E75) is a nine amino acid peptide from the extracellular domain of HER2/neu.88 Nelipepimut-S binds HLA-A2 and HLA-A3 molecules on antigen-presenting cells which then stimulate CTLs to recognize and lyse HER2-expressing tumor cells.89 NeuVax™ (Galena Biopharma, Inc., Portland, OR, USA) is a vaccine composed of nelipepimut-S and the hematopoietic growth factor, granulocyte macrophage colony-stimulating factor (GM-CSF).89 GM-CSF is administered as an adjuvant known to induce proliferation, maturation, and migration of DCs to enhance nelipepimut-S-specific immunity through augmentation of antigen presentation to CTLs.89 In addition, E75 vaccination has been shown to decrease circulating levels of Tregs in the majority of vaccinated breast cancer patients.90 Earlier clinical trials showed that nelipepimut-S was immunogenic and of reasonable safety profile and reduced recurrence rate among high-risk breast cancer patients.91–93 Mild pain and erythema at the site of injection were most frequent treatment-related AEs to E75 and GM-CSF vaccine. Other AEs included fever, nausea, and fatigue all of which were grade I/II.91 Interestingly, immunogenic potential of nelipepimut-S was shown in breast cancer patients irrespective of the level of HER2 tumor expression.94 Recently, a multicenter, multinational, prospective, randomized, double-blind, controlled Phase III study (PRESENT trial, NCT01479244) evaluating the efficacy and safety of NeuVax administered with adjuvant Leukine® (sargramostim, GM-CSF) has been completed. The study enrolled breast cancer patients who have node-positive disease and low-to-intermediate expression of HER2. A total of 758 vaccine-treated patients and control patients will be compared for DFS (NCT01479244).
Preclinical findings suggest that trastuzumab enhanced breast cancer cell killing by HER2/neu peptide-stimulated CTLs.95 In this context, two clinical trials are assessing the combination of nelipepimut-S with trastuzumab. Both studies will be multicenter, prospective, randomized, single-blind, placebo-controlled Phase II trials of trastuzumab and nelipepimut-S/GM-CSF vs trastuzumab and GM-CSF treatment alone (NCT02297698 and NCT01570036). The first study (NCT02297698) is currently recruiting participants and will include high-risk HER2-positive breast cancer patients with high HER2 expression level. In the second study (NCT01570036), the target population will be node-positive breast cancer patients with low-to-intermediate HER2-expressing tumors. In both studies, the primary end point is to compare DFS between both treatment groups.
GP2
GP2 (HER2/neu 654–662) is a nine amino acid, MHC class I peptide from the transmembrane domain of HER2.81,86 GP2 is immunogenic. The peptide has been shown to stimulate CTLs and has more potential in HER2-overexpressing breast cancer, particularly when combined with trastuzumab.86,96 Results of early Phase I clinical trial revealed safety and tolerability of GP2 peptide vaccine among high-risk, lymph node-negative breast cancer patients.97 No dose-limiting toxicities were reported with the GP2 and GM-CSF vaccine, and local reactions were managed by dose reductions in GM-CSF.97 This was further followed by Phase II trial to assess the efficacy of GP2 vaccine in preventing tumor recurrence among breast cancer patients who were HLA-A2+ with any level of expression of HER2.98 Overall, the vaccinated group did not show a statistically significant difference in the rate of recurrence compared to the control group. However, this trial further confirmed the safety of GP2 vaccine and suggested that vaccination may have clinical benefit, particularly in patients with HER2 overexpression.98
AE37
AE37 is a 15 amino acid MHC class II epitope capable of stimulating CD4+ Th lymphocytes.86 It is the Ii-Key hybrid of the MHC class II peptide, AE36 (HER2/neu 776–790).86 AE37 vaccine has been found to reduce the number of Tregs in peripheral blood from breast cancer patients.99 A Phase I clinical trial showed that AE37 vaccine is safe and well tolerated with minimal toxicity in breast cancer patients. AE37 was shown to induce HER2-specific immune response without the use of an immunoadjuvant.100 A prospective, randomized, multicenter, Phase II adjuvant trial was conducted to evaluate the efficacy of AE37 vaccine among node-positive and high-risk node-negative breast cancer patients with tumors expressing any degree of HER2.101 Results demonstrated similar rate of recurrence among vaccinated and control groups suggesting no benefit of vaccination.101 However, findings confirm the safety of AE37 vaccine suggesting that vaccination may have clinical benefit in patients with low HER2-expressing tumors.101 Patients receiving AE37 and GM-CSF had mild local toxicities which were grade I/II. Maximum systemic toxicities were grade I–III.
Mucin
Mucin glycoproteins are expressed by several epithelial cell types and malignancies.102 MUC-1 is expressed in 90% of human breast cancers.83 Mucin glycoproteins drive tumorigenesis by promoting cell adhesion, enhancing antiapoptotic signaling, and modulating intracellular growth pathways.103 Preliminary MUC-1-directed vaccines have been shown to be safe and occasionally effective at generating antigen-specific T cell and antibody responses.104,105 In a pilot Phase III randomized, double-blind study, patients with stage II breast cancer received subcutaneous injections of either placebo or oxidized mannan-MUC1. The recurrence rate in patients receiving the placebo was 27%, while patients who received immunotherapy had no recurrences, which was statistically significant. Most patients receiving oxidized mannan-MUC1 had measurable antibodies to MUC1 and some reported T cell responses.106 A Phase III trial of oxidized mannan-conjugated MUC-1 peptide vaccine demonstrated a significant reduction in recurrence rate in breast cancer patients receiving conjugated MUC-1 compared to patients receiving placebo.107 After 12–15 years of follow-up period, no signs of toxicity or autoimmunity were developed in patients who administered the vaccine.
MAM-A
MAM-A is a secretory protein that has been found to be overexpressed in 90% of invasive ductal carcinomas of the breast.108 Being a membrane-associated protein that is absent or expressed at very low levels in normal tissues, MAM-A had served as an attractive molecular marker for breast cancer immunotherapy.108,109 Preclinical evidence indicated that MAM-A is highly immunogenic in which MAM-A-expressing cells can be used to generate MAM-A-specific CTLs and CD4+ T cells that are capable of recognizing and destroying MAM-A-expressing breast cancers.109 Interestingly, MAM-A-specific CTLs were detected in breast cancer patients but not in patients without the disease.109 A Phase I clinical trial of an MAM-A DNA vaccine showed that MAM-A was immunogenic through eliciting MAM-A-specific CD8 T cell responses, increased INF-γ levels, and reduced Tregs among patients receiving the vaccine.110,111 Preliminary evidence also suggested the safety of the vaccine and improved progression-free survival (PFS) among treatment groups compared to control patients.111 Malaise/flu-like symptoms were the most common grade I AEs attributed to MAM-A DNA vaccine. No grade III/IV AEs were reported among patients receiving the vaccine.111 In the meantime, a Phase Ib (NCT02204098) randomized clinical trial is undergoing to evaluate the safety and immunogenicity of the MAM-A DNA vaccine in breast cancer patients receiving neoadjuvant endocrine therapy. Another Phase I study (NCT00807781) evaluating safety and immunogenicity of MAM-A DNA vaccine in terms of generating measurable CD8 T cell responses in metastatic breast cancer patients has been completed. These studies would provide further insights into the safety and efficacy profile of MAM-A vaccine in breast cancer.
DCs
The utilization of DCs as a vaccine strategy provides the advantage of presenting vaccine antigens to other cell types of the immune system. Preclinical studies demonstrated the potential for generating HER2-loaded DCs as well as DCs engineered to express HER2 antigen epitopes.87,112,113 The first clinical evidence for the activity of DC vaccine in breast cancer patients was reported by Brossart et al.114 The pilot study revealed the safety and efficacy of DC vaccinations among patients with advanced disease and tumors expressing HLA-A2 and HER2 or MUC1 who administered peptide-pulsed DCs subcutaneously. Immune response was detected by the presence of peptide-specific CTLs suggesting effective antitumor immune response for DC vaccination.114 Czerniecki et al115 conducted a clinical trial using vaccinations of DCs pulsed with HER2/neu HLA class I and II peptides administered to patients with HER2-positive ductal carcinoma in situ (DCIS) before surgical resection. Vaccine DCs were activated in vitro into fully functional DCs with IFN-γ and bacterial lipopolysaccharide to become highly polarized DC1 type secreting high levels of IL-12p70. Thirteen patients received four weekly intranodal doses of DC1 vaccine. The vaccinated subjects showed remarkable accumulation of T and B lymphocytes and induction of complement-dependent, tumor-lytic antibodies in breast tissue. Most patients showed reduced expression of HER2 in surgical tumor specimens. DC vaccine was well tolerated by patients with grade I/II AEs including fever, nausea, fatigue, and injection tenderness. The same strategy was applied by Koski116 et al in another pilot trial of HER2-based DC1 vaccine in a neoadjuvant immunization trial among HER2-postive breast cancer patients with DCIS. Overall, DC vaccine sensitized CD8+ as well as CD4+ T cells against HER2 peptides and enhanced lymphocyte infiltration to breast tumor tissue in a large proportion of immunized patients.116 A clinical trial assessing toxicity of HER2 DC vaccine in patients with HER2-overexpressing DCIS demonstrated tolerability of vaccine treatments with only grade I and II toxicities observed.117 Furthermore, the expression of HER2 has been significantly reduced for most immunized patients suggesting HER2 DC vaccine treatment either promoting destruction of cancer cells or suppressing expression of HER2.117 Recently, HER2 peptide-pulsed DC1 vaccine has been further tested in HER2-positive DCIS breast cancer patients (NCT02061332). In this trial, 54 patients were randomized to receive DC1 vaccine via intralesional, intranodal, or a combination of both routes of administration. In agreement with previous studies, findings confirmed the safety and immunogenicity of neoadjuvant DC1-based vaccination in DCIS HER2-positive patients which was similar among the different vaccination routes indicated.118 Recently, a Phase II clinical trial with autologous DC vaccination in HER2-negative stage II–III breast cancer has been completed and the primary outcome was to assess pCR (NCT01431196). Ongoing clinical trials evaluating peptide-based and DC-based vaccinations in breast cancer are summarized in Table 3.
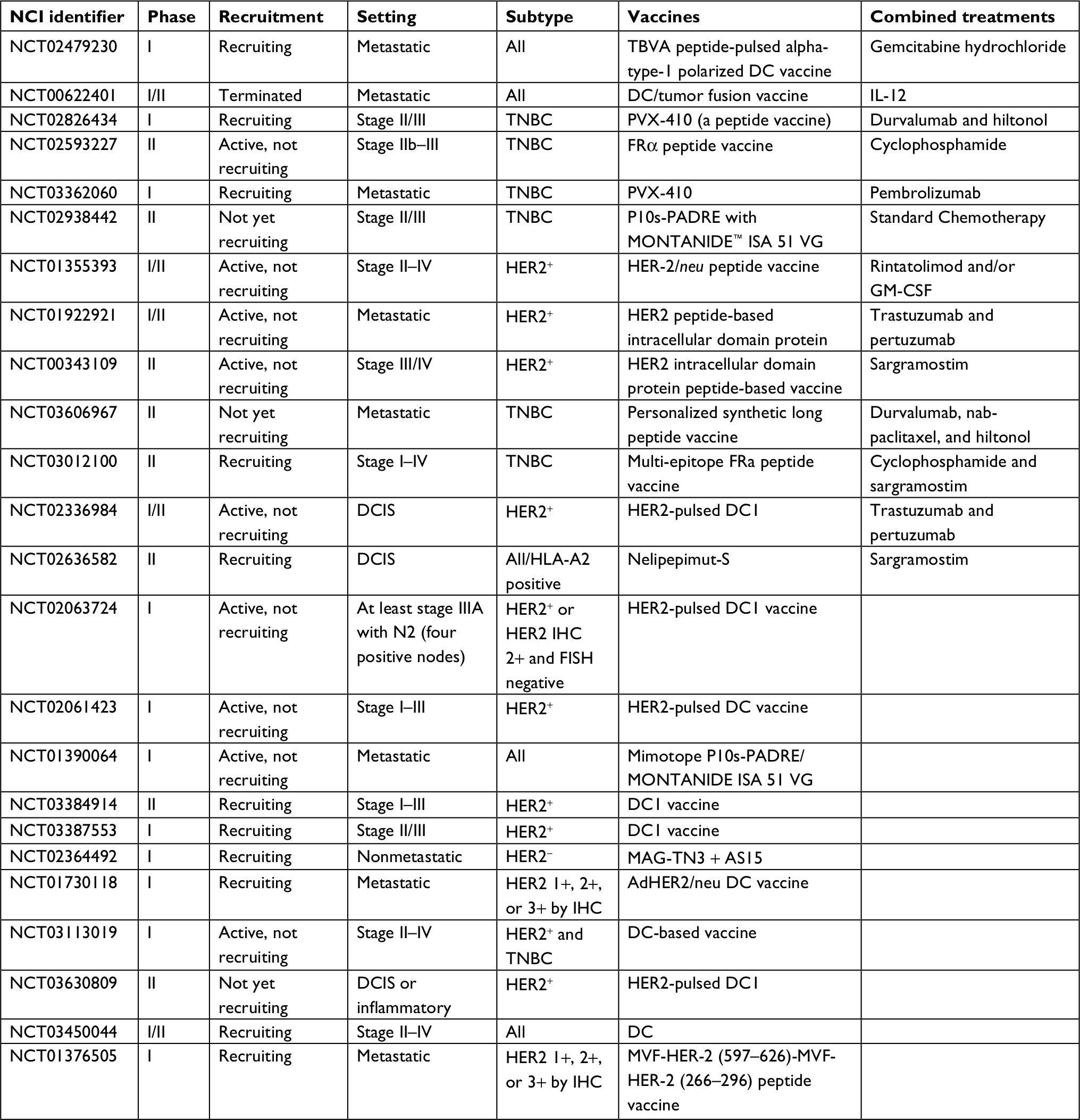 | Table 3 Ongoing clinical trials of peptide- and DC-based vaccine immunotherapeutics in breast cancer Abbreviations: DCIS, ductal carcinoma in situ; DCs, dendritic cells; FISH, fluorescence in situ hybridization; FRa, folate receptor alpha; GM-CSF, granulocyte macrophage colony-stimulating factor; HER2, human EGF receptor 2; HLA, human leukocyte antigen; IHC, immunohistochemistry; TBVA, tumor blood vessel antigen; TNBC, triple-negative breast cancer. |
Adoptive T cell transfer immunotherapy
Adoptive T cell transfer immunotherapy involves the isolation and generation of antitumor T lymphocytes from the primary tumor tissues, further expansion and activation of T cells ex vivo, and subsequently reinfusion of antitumor T cells into cancer patients to cure the disease.83,119 Thus, the ultimate objective of this process is the stimulation and expansion of potent and antigen-specific T cell immunity.119 Chimeric antigen receptor (CAR) technology represents one of the most advanced gene recombination technologies incorporated in adoptive T cell transfer. CAR is a modular fusion protein comprising extracellular target-binding domain usually derived from the single-chain variable fragment (scFv) of antibody, spacer domain, transmembrane domain, and intracellular signaling domain.53 CAR-modified T cells (CAR-T cells) showed remarkable efficacy in B cell malignancies, mostly in anti-CD19 CAR-T cells for B cell acute lymphoblastic leukemia with up to a 90% complete remission rate.120 CAR-T cell technology effectively triggers specific and prolonged T cell-mediated immunity against target antigen.53 Targeting breast cancer using CAR technology has been well documented with preclinical studies reporting the generation of CAR for breast cancer-associated tumor antigens such as mesothelin,121 MAM-A2,122 and MUC-1.123
Multiple preclinical and clinical studies had evaluated adoptive T cell transfer immunotherapy in HER2-overexpressing breast cancer utilizing HER2 as a TAA. In this context, Lanitis et al124 showed that ErbB2-redirected T cells prepared by the isolation of a novel TCR with ErbB2 (369–377) by TCR gene transfer delayed progression of ErbB2-positive HLA-A2+ human tumor in a novel xenograft animal model. Kuznetsova et al87 established a genetically modified T cell-expressing CAR specific for the ErbB2 antigen which was directly transduced into CD3+ cells which were able to specifically target and induce apoptosis in ERbB2-overexpressing breast cancer cells cocultured with CAR-T cells. A dual targeted T cells co-expressing an ErbB2- and MUC-1-specific CAR have been found to effectively kill HER2-positive breast cancer cells which express both targets.123 In addition, adoptive T cell immunotherapy had also demonstrated immune antitumor efficacy in suppressing tumor growth and both micro- and macrometastasis in HER2-overexpressing breast tumors in animal models.125–127
Few clinical studies evaluated adoptive T cell immunotherapy in breast cancer. Bernhard et al128 assessed the impact of the adoptive transfer of autologous HER2-specific T cell clones to patients with HER2-overexpressing metastatic breast cancer refractory to standard regimens. Results indicated the accumulation of the transferred T cells into bone marrow (BM) of breast cancer patients which was further associated with the disappearance of BM-residing disseminated tumor cells.128 A completed Phase I/II clinical trial (NCT00791037) involved autologous ex vivo expanded HER2-specific T cell administration to patients with metastatic HER2-overexpressing breast cancer. The study enrolled 23 patients, and the major outcomes are to evaluate toxicity and immunogenicity of infusing HER2-specific T cells.
Combination of immunotherapeutic strategies in HER2-positive breast cancer
There has been a growing preclinical evidence for the potential synergy of immunotherapy with other treatment modalities in cancer.129,130 Meaningful combinations may enhance immunogenicity by increasing antigen and MHC class I expression on tumor cells, promoting TIL infiltration and vascular permeability, positively modulating CTL antitumor activity, or by relieving immunosuppressive signals within tumors.131 Multiple therapies are currently being investigated in combination with immunotherapy for breast cancer treatment including chemotherapy, targeted therapy, and radiation therapy.52,131,132
Combinations of immunotherapy and chemotherapy
Chemotherapy has been shown to augment antitumor immunogenicity through mediating the activation and functionality of CTLs and NK cells,133–136 enhancing the activity and maturation of DCs,136 and depleting the immunosuppressive Tregs.134,137,138 Collectively, these findings directed the design and evaluation of several combinations of chemotherapeutic agents and immunotherapy in breast cancer. Several groups have evaluated the combinations of chemotherapy and immune checkpoint inhibitors in breast cancer. Multiple ongoing clinical trials combining ipilimumab with liposomal doxorubicin and cyclophosphamide are being conducted in breast cancer patients (Table 1; NCT03409198 and NCT03328026). Pembrolizumab is being currently investigated in advanced breast cancer in combination with carboplatin and trastuzumab in a large Phase II study (Table 2; NCT03095352). Atezolizumab is also being investigated in early Phase I studies with carboplatin, cyclophosphamide, and doxorubicin in metastatic HER2-positive breast cancer patients (Table 2; NCT02914470 and NCT02605915).
Combinations of immunotherapy and targeted therapy
Trastuzumab treatment has been shown to upregulate the levels of PD-L1 in a transgenic mouse model of breast cancer, thus mediating resistance to trastuzumab therapy.139 In line with this, preclinical studies have shown that the combination of PD-L1 and HER2 inhibitors was synergistic against HER2-positive breast cancer in animal models.140 In addition, the presence of TILs was associated with improved outcomes in patients receiving trastuzumab treatment.17,37 Recent evidence also demonstrated increased Tregs in HER2-positive breast cancer patients who failed to achieve pCR suggesting the development of an immunosuppressive phenotype.141 Overall, these findings encouraged clinical trials utilizing checkpoint blocking immunotherapy in combination with anti-HER2 treatments in patients with HER2-positive breast cancer.
The currently ongoing Phase II PANACEA study is investigating pembrolizumab in combination with trastuzumab in HER2-positive metastatic breast cancer patients who progressed while on trastuzumab treatment (Table 2; NCT02129556). Further, pembrolizumab is being evaluated in combination with carboplatin and trastuzumab in advanced breast cancer patients in a Phase II clinical study (Table 2; NCT03095352). A Phase I study is ongoing to evaluate the safety and tolerability of atezolizumab combination with T-DM1 or with trastuzumab plus pertuzumab in HER2-positive disease (Table 2; NCT02605915). Atezolizumab is also being evaluated in combination with paclitaxel, trastuzumab, and pertuzumab in metastatic HER2-positive patients for the assessment of antitumor activity and OS (Table 2; NCT03125928). A Phase II double-blind, randomized, placebo-controlled multicenter study is investigating the efficacy and safety of T-DM1 in combination with atezolizumab in patients with HER2-positive locally advanced or metastatic breast cancer who have progressed on previously received trastuzumab and taxane-based therapy. Almost 200 participants have been enrolled, and the estimated study completion date is by the end of the year 2020 (Table 2; NCT02924883). Durvalumab and nivolumab are also being evaluated among advanced HER2-postive breast cancer patients in combination with trastuzumab (NCT02649686 and NCT03523572, respectively).
Two early Phase I/II clinical trials are currently ongoing to investigate the safety and efficacy of combined vaccine therapy with anti-HER2 treatment among HER2-postive breast cancer patients. The first study is combining HER2 peptide-based intracellular domain protein with trastuzumab and pertuzumab among metastatic HER2-overexpressing patients (Table 3; NCT01922921). The second study is investigating the combination of HER2-pulsed DC1 vaccine with trastuzumab and pertuzumab in DCIS patients with HER2-positive disease (Table 3; NCT02336984). A recently completed Phase II study was conducted among patients with locally recurrent or metastatic HER2-positive disease who received autologous DC vaccine therapy along with trastuzumab and vinorelbine (NCT00266110). Patients were monitored for disease progression and toxicity. In the same context, a completed Phase I study revealed the safety and efficacy for the combination of GP2 peptide and trastuzumab in the treatment of patients with HER2-overexpressing breast cancer in the adjuvant setting (NCT03014076).
Several clinical trials are ongoing to investigate immunotherapy in combination with other targeted treatments among other molecular subtypes of breast cancer; these include poly (ADP-ribose) polymerase (PARP) inhibitors, hormonal treatments, angiogenesis inhibitors, AKT inhibitors, mTOR inhibitors, MEK inhibitors, and other targeted therapies (Tables 1–3).
Combinations of immunotherapy and radiation therapy
Radiation therapy has been recently shown to promote several immunostimulatory effects. Radiation therapy enhances tumor neoantigen presentation, thus improving the recognition of irradiated cells by CTLs.142–144 Although radiation therapy represents an appealing strategy to combine with immunotherapy, limited number of clinical trials is currently investigating the effect of this combination in breast cancer. A recently completed Phase I study (NCT02303366) described the safety and activity of combining ablative body radiosurgery (SABR) treatment and pembrolizumab in 15 patients with oligometastatic breast cancer. Investigators hypothesize that the combination would be tolerable and will result in systemic immune activation.
Conclusion
Immunotherapy is evolving dramatically in the treatment of several types of advanced cancers, particularly after the recent success of the use of novel immunotherapy in the treatment of melanoma. Alongside, breast cancer is being recognized as immunogenic as a result of the remarkable progress in understanding the immune landscape of tumor microenvironment for the different subtypes of breast cancer. Accordingly, immunotherapy has emerged as a promising targeted treatment in breast cancer, especially with promising results from clinical trials in patients with TNBC. In this regard, assessing the efficacy of immunotherapeutic treatments based on molecular stratification of breast cancer may allow a greater window of opportunity to individualize breast cancer treatment and drive future research to find the best immunotherapeutic agents for patients. In this review, we have highlighted recent clinical evidence for immunotherapeutic treatments in breast cancer focusing on HER2-overexpressing subtype. Overall, no immunotherapy has been approved so far for preventive or therapeutic treatments in breast cancer. Ongoing clinical trials are investigating immune checkpoint inhibitors, CTLA-4 inhibitors, and anti-PD-1 or anti-PD-L1 antibodies, in early clinical trials for advanced HER2-positive breast cancer. Taking into account the modest benefit for the former immunotherapeutic agents in breast cancer, there is a growing interest in testing activity along with tolerability for the combination treatment of immune checkpoint inhibitors with standard breast cancer treatments such as chemotherapy and targeted and radiation therapy. HER2-specific peptide-based vaccines are most advanced in clinical trials at present. Nelipepimut-S (E75) is currently in Phase III clinical trials and in Phase II trials in combination with trastuzumab. So far, limited data are available for adoptive T cell transfer immunotherapy in clinical breast cancer settings; however, preclinical evidence highlights potentials for this technology.
Future perspective
The combination of immunotherapeutics with established cancer therapies is emerging. Therefore, rational design of combination treatments of immunotherapy with other standard breast cancer treatments requires deep understanding of the effect of each treatment on antitumor immunity utilizing nonredundant mechanisms of actions. In addition, the combination treatment approach requires careful evaluation for issues of treatment cost and toxicity. A major challenge for combination treatments with immunotherapy is the great number of potential combinations which requires crucial selection of breast cancer patients who would benefit most from immunotherapy.
Disclosure
The authors report no conflicts of interest in this work.
References
Chew V, Toh HC, Abastado J-P. Immune microenvironment in tumor progression: characteristics and challenges for therapy. J Oncol. 2012;2012(5):1–10. | ||
Santa-Maria CA, Park SJ, Jain S, Gradishar WJ. Breast cancer and immunology: biomarker and therapeutic developments. Expert Rev Anticancer Ther. 2015;15(10):1215–1222. | ||
Swann JB, Smyth MJ. Immune surveillance of tumors. J Clin Invest. 2007;117(5):1137–1146. | ||
Su M, Huang CX, Dai AP. Immune checkpoint inhibitors: therapeutic tools for breast cancer. Asian Pac J Cancer Prev. 2016;17(3):905–910. | ||
Sugie T, Toi M. Antitumor immunity and advances in cancer immunotherapy. Breast Cancer. 2017;24(1):1–2. | ||
de La Cruz-Merino L, Chiesa M, Caballero R, et al. Breast cancer immunology and immunotherapy: current status and future perspectives. Int Rev Cell Mol Biol. 2017;331:1–53. | ||
Zhang H, Chen J. Current status and future directions of cancer immunotherapy. J Cancer. 2018;9(10):1773–1781. | ||
Yang Y. Cancer immunotherapy: harnessing the immune system to battle cancer. J Clin Invest. 2015;125(9):3335–3337. | ||
Wojtowicz ME, Dunn BK, Umar A. Immunologic approaches to cancer prevention-current status, challenges, and future perspectives. Semin Oncol. 2016;43(1):161–172. | ||
Criscitiello C, Curigliano G. Immunotherapeutics for breast cancer. Curr Opin Oncol. 2013;25(6):602–608. | ||
Polyak K. Heterogeneity in breast cancer. J Clin Invest. 2011;121(10):3786–3788. | ||
Sørlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci U S A. 2001;98(19):10869–10874. | ||
Perou CM, Sørlie T, Eisen MB, et al. Molecular portraits of human breast tumours. Nature. 2000;406(6797):747–752. | ||
Ali HR, Provenzano E, Dawson SJ, et al. Association between CD8+ T-cell infiltration and breast cancer survival in 12,439 patients. Ann Oncol. 2014;25(8):1536–1543. | ||
Miller LD, Chou JA, Black MA, et al. Immunogenic subtypes of breast cancer delineated by gene classifiers of immune responsiveness. Cancer Immunol Res. 2016;4(7):600–610. | ||
Mao Y, Qu Q, Chen X, Huang O, Wu J, Shen K. The prognostic value of tumor-infiltrating lymphocytes in breast cancer: a systematic review and meta-analysis. PLoS One. 2016;11(4):e0152500. | ||
Loi S, Sirtaine N, Piette F, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol. 2013;31(7):860–867. | ||
Stanton SE, Adams S, Disis ML. Variation in the incidence and magnitude of tumor-infiltrating lymphocytes in breast cancer subtypes: a systematic review. JAMA Oncol. 2016;2(10):1354–1360. | ||
Denkert C, von Minckwitz G, Darb-Esfahani S, et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. | ||
Denkert C. The immunogenicity of breast cancer–molecular subtypes matter. Ann Oncol. 2014;25(8):1453–1455. | ||
Huang Y, Ma C, Zhang Q, et al. CD4+ and CD8+ T cells have opposing roles in breast cancer progression and outcome. Oncotarget. 2015;6(19):17462–17478. | ||
Krishnamurti U, Silverman JF. HER2 in breast cancer: a review and update. Adv Anat Pathol. 2014;21(2):100–107. | ||
Burstein HJ. The distinctive nature of HER2-positive breast cancers. N Engl J Med. 2005;353(16):1652–1654. | ||
Hudis CA. Trastuzumab–mechanism of action and use in clinical practice. N Engl J Med. 2007;357(1):39–51. | ||
Ahmed S, Sami A, Xiang J. HER2-directed therapy: current treatment options for HER2-positive breast cancer. Breast Cancer. 2015;22(2):101–116. | ||
Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–792. | ||
Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353(16):1659–1672. | ||
Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353(16):1673–1684. | ||
Viani GA, Afonso SL, Stefano EJ, De Fendi LI, Soares FV. Adjuvant trastuzumab in the treatment of her-2-positive early breast cancer: a meta-analysis of published randomized trials. BMC Cancer. 2007;7(1):153. | ||
Valabrega G, Montemurro F, Aglietta M. Trastuzumab: mechanism of action, resistance and future perspectives in HER2-overexpressing breast cancer. Ann Oncol. 2007;18(6):977–984. | ||
Amiri-Kordestani L, Blumenthal GM, Xu QC, et al. FDA approval: ado-trastuzumab emtansine for the treatment of patients with HER2-positive metastatic breast cancer. Clin Cancer Res. 2014;20(17):4436–4441. | ||
O’Sullivan CC, Connolly RM. Pertuzumab and its accelerated approval: evolving treatment paradigms and new challenges in the management of HER2-positive breast cancer. Oncology. 2014;28(3):186–194. | ||
Ryan Q, Ibrahim A, Cohen MH, et al. FDA drug approval summary: lapatinib in combination with capecitabine for previously treated metastatic breast cancer that overexpresses HER-2. Oncologist. 2008;13(10):1114–1119. | ||
Subbiah IM, Gonzalez-Angulo AM. Advances and future directions in the targeting of HER2-positive breast cancer: implications for the future. Curr Treat Options Oncol. 2014;15(1):41–54. | ||
Martin M, López-Tarruella S. Emerging therapeutic options for HER2-positive breast cancer. Am Soc Clin Oncol Educ Book. 2016;35:e64–e70. | ||
Montemurro F, Donadio M, Clavarezza M, et al. Outcome of patients with HER2-positive advanced breast cancer progressing during trastuzumab-based therapy. Oncologist. 2006;11(4):318–324. | ||
Salgado R, Denkert C, Campbell C, et al. Tumor-infiltrating lymphocytes and associations with pathological complete response and event-free survival in HER2-positive early-stage breast cancer treated with lapatinib and trastuzumab. JAMA Oncology. 2015;1(4):448–454. | ||
Perez EA, Ballman KV, Tenner KS, et al. Association of stromal tumor-infiltrating lymphocytes with recurrence-free survival in the n9831 adjuvant trial in patients with early-stage HER2-positive breast cancer. JAMA Oncol. 2016;2(1):56–64. | ||
Ingold Heppner B, Untch M, Denkert C, et al. Tumor-infiltrating lymphocytes: a predictive and prognostic biomarker in neoadjuvant-treated HER2-positive breast cancer. Clin Cancer Res. 2016;22(23):5747–5754. | ||
Loi S, Michiels S, Salgado R, et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: results from the FinHER trial. Ann Oncol. 2014;25(8):1544–1550. | ||
Alexe G, Dalgin GS, Scanfeld D, et al. High expression of lymphocyte-associated genes in node-negative HER2+ breast cancers correlates with lower recurrence rates. Cancer Res. 2007;67(22):10669–10676. | ||
Luen SJ, Salgado R, Fox S, et al. Tumour-infiltrating lymphocytes in advanced HER2-positive breast cancer treated with pertuzumab or placebo in addition to trastuzumab and docetaxel: a retrospective analysis of the CLEOPATRA study. Lancet Oncol. 2017;18(1):52–62. | ||
Bense RD, Sotiriou C, Piccart-Gebhart MJ, et al. Relevance of tumor-infiltrating immune cell composition and functionality for disease outcome in breast cancer. J Natl Cancer Inst. 2017;109(1):djw192. | ||
Gheybi MK, Farrokhi S, Ravanbod MR, Ostovar A, Mehrzad V, Nematollahi P. The correlation of CD19 + CD24 + CD38 + B cells and other clinicopathological variables with the proportion of circulating Tregs in breast cancer patients. Breast Cancer. 2017;24(6):756–764. | ||
Bailur JK, Gueckel B, Derhovanessian E, Pawelec G. Presence of circulating Her2-reactive CD8 + T-cells is associated with lower frequencies of myeloid-derived suppressor cells and regulatory T cells, and better survival in older breast cancer patients. Breast Cancer Res. 2015;17(1):34. | ||
Decker T, Fischer G, Bücke W, et al. Increased number of regulatory T cells (T-regs) in the peripheral blood of patients with Her-2/neu-positive early breast cancer. J Cancer Res Clin Oncol. 2012;138(11):1945–1950. | ||
Varn FS, Mullins DW, Arias-Pulido H, Fiering S, Cheng C. Adaptive immunity programmes in breast cancer. Immunology. 2017;150(1):25–34. | ||
Disis ML. Mechanism of action of immunotherapy. Semin Oncol. 2014;41(Suppl 5):S3–S13. | ||
Schuster M, Nechansky A, Kircheis R. Cancer immunotherapy. Biotechnol J. 2006;1(2):138–147. | ||
Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12(4):252–264. | ||
Corona SP, Sobhani N, Ianza A, et al. Advances in systemic therapy for metastatic breast cancer: future perspectives. Med Oncol. 2017;34(7):119. | ||
Mansour M, Teo ZL, Luen SJ, Loi S. Advancing immunotherapy in metastatic breast cancer. Curr Treat Options Oncol. 2017;18(6):35. | ||
Hu X, Huang W, Fan M. Emerging therapies for breast cancer. J Hematol Oncol. 2017;10(1):98. | ||
Buchbinder E, Hodi FS. Cytotoxic T lymphocyte antigen-4 and immune checkpoint blockade. J Clin Invest. 2015;125(9):3377–3383. | ||
Bour-Jordan H, Esensten JH, Martinez-Llordella M, Penaranda C, Stumpf M, Bluestone JA. Intrinsic and extrinsic control of peripheral T-cell tolerance by costimulatory molecules of the CD28/ B7 family. Immunol Rev. 2011;241(1):180–205. | ||
Esensten JH, Helou YA, Chopra G, Weiss A, Bluestone JA. CD28 Costimulation: from mechanism to therapy. Immunity. 2016;44(5):973–988. | ||
Mccoy KD, Le Gros G. The role of CTLA-4 in the regulation of T cell immune responses. Immunol Cell Biol. 1999;77(1):1–10. | ||
Karman J, Jiang JL, Gumlaw N, et al. Ligation of cytotoxic T lymphocyte antigen-4 to T cell receptor inhibits T cell activation and directs differentiation into Foxp3+ regulatory T cells. J Biol Chem. 2012;287(14):11098–11107. | ||
Emens LA. Breast cancer immunobiology driving immunotherapy: vaccines and immune checkpoint blockade. Expert Rev Anticancer Ther. 2012;12(12):1597–1611. | ||
Blank CU, Enk A. Therapeutic use of anti-CTLA-4 antibodies. Int Immunol. 2015;27(1):3–10. | ||
Lipson EJ, Drake CG. Ipilimumab: an anti-CTLA-4 antibody for metastatic melanoma. Clin Cancer Res. 2011;17(22):6958–6962. | ||
Guazzelli A, Hussain M, Krstic-Demonacos M, Mutti L. Tremelimumab for the treatment of malignant mesothelioma. Expert Opin Biol Ther. 2015;15(12):1819–1829. | ||
Mcarthur HL, Diab A, Page DB, et al. A pilot study of preoperative single-dose ipilimumab and/or cryoablation in women with early-stage breast cancer with comprehensive immune profiling. Clin Cancer Res. 2016;22(23):5729–5737. | ||
Vonderheide RH, Lorusso PM, Khalil M, et al. Tremelimumab in combination with exemestane in patients with advanced breast cancer and treatment-associated modulation of inducible costimulator expression on patient T cells. Clin Cancer Res. 2010;16(13):3485–3494. | ||
Jin HT, Ahmed R, Okazaki T. Role of PD-1 in regulating T-cell immunity. Curr Top Microbiol Immunol. 2011;350:17–37. | ||
Riley JL. PD-1 signaling in primary T cells. Immunol Rev. 2009;229(1):114–125. | ||
Poole RM. Pembrolizumab: first global approval. Drugs. 2014;74(16):1973–1981. | ||
Raedler LA. Opdivo (Nivolumab): second PD-1 inhibitor receives FDA approval for unresectable or metastatic melanoma. Am Health Drug Benefits. 2015;8(Spec Feature):180–183. | ||
Kasamon YL, de Claro RA, Wang Y, Shen YL, Farrell AT, Pazdur R. FDA approval summary: nivolumab for the treatment of relapsed or progressive classical Hodgkin lymphoma. Oncologist. 2017;22(5):585–591. | ||
Xu JX, Maher VE, Zhang L, et al. FDA approval summary: nivolumab in advanced renal cell carcinoma after anti-angiogenic therapy and exploratory predictive biomarker analysis. Oncologist. 2017;22(3):311–317. | ||
Kazandjian D, Suzman DL, Blumenthal G, et al. FDA approval summary: nivolumab for the treatment of metastatic non-small cell lung cancer with progression on or after platinum-based chemotherapy. Oncologist. 2016;21(5):634–642. | ||
Kim ES. Avelumab: first global approval. Drugs. 2017;77(8):929–937. | ||
Wills S, Hochmuth LK, Bauer Ks Jr, Deshmukh R. Durvalumab: a newly approved checkpoint inhibitor for the treatment of urothelial carcinoma. Curr Probl Cancer. Epub 2018 Sep 18. | ||
Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III Non-Small-Cell Lung Cancer. N Engl J Med. 2017;377(20):1919–1929. | ||
Ghebeh H, Mohammed S, Al-Omair A, et al. The B7-H1 (PD-L1) T lymphocyte-inhibitory molecule is expressed in breast cancer patients with infiltrating ductal carcinoma: correlation with important high-risk prognostic factors. Neoplasia. 2006;8(3):190–198. | ||
Rugo HS, Delord JP, Im SA, et al. Safety and antitumor activity of pembrolizumab in patients with estrogen receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer. Clin Cancer Res. 2018;24(12):2804–2811. | ||
Nanda R, Chow LQ, Dees EC, et al. Pembrolizumab in patients with advanced triple-negative breast cancer: Phase Ib KEYNOTE-012 study. J Clin Oncol. 2016;34(21):2460–2467. | ||
Emens La BF, Cassier P, Delord J, et al. Inhibition of PD-L1 by MPDL3280A leads to clinical activity in patients with metastatic triple-negative breast cancer (TNBC). [abstract]. In: Proceedings of the 106th Annual Meeting of the American Association for Cancer Research; 2015 Apr 18-22; Philadelphia, PA. Philadelphia (PA): AACR. Cancer Res. 2015;75(15 Suppl). Abstract nr 2859. | ||
Schmid PCC, Braiteh FS, Eder JP, et al. Atezolizumab in metastatic TNBC (mTNBC): Long-term clinical outcomes and biomarker analyses [abstract]. In: Proceedings of the American Association for Cancer Research Annual Meeting 2017; 2017 Apr 1–5; Washington, DC. Philadelphia (PA): AACR. Cancer Res. 2017;77(13 Suppl). Abstract nr 2986. | ||
Dirix LY, Takacs I, Jerusalem G, et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: a phase 1b JAVELIN solid tumor study. Breast Cancer Res Treat. 2018;167(3):671–686. | ||
Ladjemi MZ, Jacot W, Chardès T, Pèlegrin A, Navarro-Teulon I. Anti-HER2 vaccines: new prospects for breast cancer therapy. Cancer Immunol Immunother. 2010;59(9):1295–1312. | ||
Page DB, Naidoo J, McArthur HL. Emerging immunotherapy strategies in breast cancer. Immunotherapy. 2014;6(2):195–209. | ||
Zhou J, Zhong Y. Breast cancer immunotherapy. Cell Mol Immunol. 2004;1(4):247–255. | ||
Razazan A, Behravan J, Arab A, et al. Conjugated nanoliposome with the HER2/neu-derived peptide GP2 as an effective vaccine against breast cancer in mice xenograft model. PLoS One. 2017;12(10): e0185099. | ||
Curigliano G, Rescigno M, Goldhirsch A. Immunology and breast cancer: therapeutic cancer vaccines. The Breast. 2007;16(Suppl 2):20–26. | ||
Clifton GT, Mittendorf EA, Peoples GE. Adjuvant HER2/neu peptide cancer vaccines in breast cancer. Immunotherapy. 2015;7(11):1159–1168. | ||
Kuznetsova M, Lopatnikova J, Khantakova J, Maksyutov R, Maksyutov A, Sennikov S. Generation of populations of antigen-specific cytotoxic T cells using DCs transfected with DNA construct encoding HER2/neu tumor antigen epitopes. BMC Immunol. 2017;18(1):31. | ||
Clifton GT, Peoples GE, Mittendorf EA. The development and use of the E75 (HER2 369-377) peptide vaccine. Future Oncol. 2016;12(11):1321–1329. | ||
Schneble EJ, Berry JS, Trappey FA, et al. The HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence: correlation of immunologic data with clinical response. Immunotherapy. 2014;6(5):519–531. | ||
Hueman MT, Stojadinovic A, Storrer CE, et al. Levels of circulating regulatory CD4+CD25+ T cells are decreased in breast cancer patients after vaccination with a HER2/neu peptide (E75) and GM-CSF vaccine. Breast Cancer Res Treat. 2006;98(1):17–29. | ||
Murray JL, Gillogly ME, Przepiorka D, et al. Toxicity, immunogenicity, and induction of E75-specific tumor-lytic CTLs by HER-2 peptide E75 (369-377) combined with granulocyte macrophage colony-stimulating factor in HLA-A2+ patients with metastatic breast and ovarian cancer. Clin Cancer Res. 2002;8(11):3407–3418. | ||
Peoples GE, Gurney JM, Hueman MT, et al. Clinical trial results of a HER2/neu (E75) vaccine to prevent recurrence in high-risk breast cancer patients. J Clin Oncol. 2005;23(30):7536–7545. | ||
Mittendorf EA, Clifton GT, Holmes JP, et al. Final report of the phase I/II clinical trial of the E75 (nelipepimut-S) vaccine with booster inoculations to prevent disease recurrence in high-risk breast cancer patients. Ann Oncol. 2014;25(9):1735–1742. | ||
Benavides LC, Gates JD, Carmichael MG, et al. The impact of HER2/neu expression level on response to the E75 vaccine: from U.S. Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin Cancer Res. 2009;15(8):2895–2904. | ||
Mittendorf EA, Storrer CE, Shriver CD, Ponniah S, Peoples GE. Investigating the combination of trastuzumab and HER2/neu peptide vaccines for the treatment of breast cancer. Ann Surg Oncol. 2006;13(8):1085–1098. | ||
Mittendorf EA, Storrer CE, Foley RJ, et al. Evaluation of the HER2/neu-derived peptide GP2 for use in a peptide-based breast cancer vaccine trial. Cancer. 2006;106(11):2309–2317. | ||
Carmichael MG, Benavides LC, Holmes JP, et al. Results of the first phase 1 clinical trial of the HER-2/neu peptide (GP2) vaccine in disease-free breast cancer patients: United States Military Cancer Institute Clinical Trials Group Study I-04. Cancer. 2010;116(2):292–301. | ||
Mittendorf EA, Ardavanis A, Litton JK, et al. Primary analysis of a prospective, randomized, single-blinded phase II trial evaluating the HER2 peptide GP2 vaccine in breast cancer patients to prevent recurrence. Oncotarget. 2016;7(40):66192–66201. | ||
Gates JD, Clifton GT, Benavides LC, et al. Circulating regulatory T cells (CD4+CD25+FOXP3+) decrease in breast cancer patients after vaccination with a modified MHC class II HER2/neu (AE37) peptide. Vaccine. 2010;28(47):7476–7482. | ||
Holmes JP, Benavides LC, Gates JD, et al. Results of the first phase I clinical trial of the novel II-key hybrid preventive HER-2/neu peptide (AE37) vaccine. J Clin Oncol. 2008;26(20):3426–3433. | ||
Mittendorf EA, Ardavanis A, Symanowski J, et al. Primary analysis of a prospective, randomized, single-blinded phase II trial evaluating the HER2 peptide AE37 vaccine in breast cancer patients to prevent recurrence. Ann Oncol. 2016;27(7):1241–1248. | ||
Abdel-Aal AB, Lakshminarayanan V, Thompson P, et al. Immune and anticancer responses elicited by fully synthetic aberrantly glycosylated MUC1 tripartite vaccines modified by a TLR2 or TLR9 agonist. Chembiochem. 2014;15(10):1508–1513. | ||
Bafna S, Kaur S, Batra SK. Membrane-bound mucins: the mechanistic basis for alterations in the growth and survival of cancer cells. Oncogene. 2010;29(20):2893–2904. | ||
Kimura T, Finn OJ. MUC1 immunotherapy is here to stay. Expert Opin Biol Ther. 2013;13(1):35–49. | ||
Yuan S, Shi C, Liu L, Han W. MUC1-based recombinant Bacillus Calmette-Guerin vaccines as candidates for breast cancer immunotherapy. Expert Opin Biol Ther. 2010;10(7):1037–1048. | ||
Apostolopoulos V, Pietersz GA, Tsibanis A, et al. Pilot phase III immunotherapy study in early-stage breast cancer patients using oxidized mannan-MUC1 [ISRCTN71711835]. Breast Cancer Res. 2006;8(3):R27. | ||
Vassilaros S, Tsibanis A, Tsikkinis A, Pietersz GA, Mckenzie IF, Apostolopoulos V. Up to 15-year clinical follow-up of a pilot Phase III immunotherapy study in stage II breast cancer patients using oxidized mannan-MUC1. Immunotherapy. 2013;5(11):1177–1182. | ||
Al Joudi FS. Human mammaglobin in breast cancer: a brief review of its clinical utility. Indian J Med Res. 2014;139(5):675–685. | ||
Kim SW, Goedegebuure P, Gillanders WE. Mammaglobin-A is a target for breast cancer vaccination. Oncoimmunology. 2016;5(2):e1069940. | ||
Tiriveedhi V, Fleming TP, Goedegebuure PS, et al. Mammaglobin-A cDNA vaccination of breast cancer patients induces antigen-specific cytotoxic CD4+ICOShi T cells. Breast Cancer Res Treat. 2013;138(1):109–118. | ||
Tiriveedhi V, Tucker N, Herndon J, et al. Safety and preliminary evidence of biologic efficacy of a mammaglobin-a DNA vaccine in patients with stable metastatic breast cancer. Clin Cancer Res. 2014;20(23):5964–5975. | ||
Chen Y, Emtage P, Zhu Q, et al. Induction of ErbB-2/neu-specific protective and therapeutic antitumor immunity using genetically modified dendritic cells: enhanced efficacy by cotransduction of gene encoding IL-12. Gene Ther. 2001;8(4):316–323. | ||
Sas S, Chan T, Sami A, El-Gayed A, Xiang J. Vaccination of fiber-modified adenovirus-transfected dendritic cells to express HER-2/neu stimulates efficient HER-2/neu-specific humoral and CTL responses and reduces breast carcinogenesis in transgenic mice. Cancer Gene Ther. 2008;15(10):655–666. | ||
Brossart P, Wirths S, Stuhler G, Reichardt VL, Kanz L, Brugger W. Induction of cytotoxic T-lymphocyte responses in vivo after vaccinations with peptide-pulsed dendritic cells. Blood. 2000;96(9):3102–3108. | ||
Czerniecki BJ, Koski GK, Koldovsky U, et al. Targeting HER-2/neu in early breast cancer development using dendritic cells with staged interleukin-12 burst secretion. Cancer Res. 2007;67(4):1842–1852. | ||
Koski GK, Koldovsky U, Xu S, et al. A novel dendritic cell-based immunization approach for the induction of durable Th1-polarized anti-HER-2/neu responses in women with early breast cancer. J Immunother. 2012;35(1):54–65. | ||
Sharma A, Koldovsky U, Xu S, et al. HER-2 pulsed dendritic cell vaccine can eliminate HER-2 expression and impact ductal carcinoma in situ. Cancer. 2012;118(17):4354–4362. | ||
Lowenfeld L, Mick R, Datta J, et al. Dendritic cell vaccination enhances immune responses and induces regression of HER2pos DCIS independent of route: results of randomized selection design trial. Clin Cancer Res. 2017;23(12):2961–2971. | ||
Kalos M, June CH. Adoptive T cell transfer for cancer immunotherapy in the era of synthetic biology. Immunity. 2013;39(1):49–60. | ||
Perica K, Varela JC, Oelke M, Schneck J. Adoptive T cell immunotherapy for cancer. Rambam Maimonides Med J. 2015;6(1):e0004. | ||
Tchou J, Wang LC, Selven B, et al. Mesothelin, a novel immunotherapy target for triple negative breast cancer. Breast Cancer Res Treat. 2012;133(2):799–804. | ||
Lerret NM, Rogozinska M, Jaramillo A, Marzo AL. Adoptive transfer of Mammaglobin-A epitope specific CD8 T cells combined with a single low dose of total body irradiation eradicates breast tumors. PLoS One. 2012;7(7):e41240. | ||
Wilkie S, van Schalkwyk MC, Hobbs S, et al. Dual targeting of ErbB2 and MUC1 in breast cancer using chimeric antigen receptors engineered to provide complementary signaling. J Clin Immunol. 2012;32(5):1059–1070. | ||
Lanitis E, Smith JB, Dangaj D, et al. A human ErbB2-specific T-cell receptor confers potent antitumor effector functions in genetically engineered primary cytotoxic lymphocytes. Hum Gene Ther. 2014;25(8):730–739. | ||
Li S, Yang J, Urban FA, et al. Genetically engineered T cells expressing a HER2-specific chimeric receptor mediate antigen-specific tumor regression. Cancer Gene Ther. 2008;15(6):382–392. | ||
Morales JK, Kmieciak M, Graham L, Feldmesser M, Bear HD, Manjili MH. Adoptive transfer of HER2/neu-specific T cells expanded with alternating gamma chain cytokines mediate tumor regression when combined with the depletion of myeloid-derived suppressor cells. Cancer Immunol Immunother. 2009;58(6):941–953. | ||
Wang LX, Plautz GE. T cells sensitized with breast tumor progenitor cell vaccine have therapeutic activity against spontaneous HER2/neu tumors. Breast Cancer Res Treat. 2012;134(1):61–70. | ||
Bernhard H, Neudorfer J, Gebhard K, et al. Adoptive transfer of autologous, HER2-specific, cytotoxic T lymphocytes for the treatment of HER2-overexpressing breast cancer. Cancer Immunol Immunother. 2007;57(2):271–280. | ||
Robert L, Ribas A, Hu-Lieskovan S. Combining targeted therapy with immunotherapy. Can 1+1 equal more than 2? Semin Immunol. 2016;28(1):73–80. | ||
Gotwals P, Cameron S, Cipolletta D, et al. Prospects for combining targeted and conventional cancer therapy with immunotherapy. Nat Rev Cancer. 2017;17(5):286–301. | ||
Wargo JA, Reuben A, Cooper ZA, Oh KS, Sullivan RJ. Immune effects of chemotherapy, radiation, and targeted therapy and opportunities for combination with immunotherapy. Semin Oncol. 2015;42(4):601–616. | ||
Vonderheide RH, Domchek SM, Clark AS. Immunotherapy for Breast Cancer: What Are We Missing? Clin Cancer Res. 2017;23(11):2640–2646. | ||
Xia Q, Zhang FF, Geng F, et al. Improvement of anti-tumor immunity of fibroblast activation protein α based vaccines by combination with cyclophosphamide in a murine model of breast cancer. Cell Immunol. 2016;310:89–98. | ||
Madondo MT, Quinn M, Plebanski M. Low dose cyclophosphamide: mechanisms of T cell modulation. Cancer Treat Rev. 2016;42:3–9. | ||
Kareva I. A Combination of immune checkpoint inhibition with metronomic chemotherapy as a way of targeting therapy-resistant cancer cells. Int J Mol Sci. 2017;18(10):E2134. | ||
Zhu XJ, Yang ZF, Zhou JY, et al. Progression of large lymphoma is significantly impeded with a combination of gemcitabine chemotherapy and dendritic cells intra-tumor vaccination. PLoS One. 2015;10(7):e0132799. | ||
Banissi C, Ghiringhelli F, Chen L, Carpentier AF. Treg depletion with a low-dose metronomic temozolomide regimen in a rat glioma model. Cancer Immunol Immunother. 2009;58(10):1627–1634. | ||
Ghiringhelli F, Menard C, Puig PE, et al. Metronomic cyclophosphamide regimen selectively depletes CD4+CD25+ regulatory T cells and restores T and NK effector functions in end stage cancer patients. Cancer Immunol Immunother. 2007;56(5):641–648. | ||
Chaganty BKR, Qiu S, Gest A, et al. Trastuzumab upregulates PD-L1 as a potential mechanism of trastuzumab resistance through engagement of immune effector cells and stimulation of IFNγ secretion. Cancer Lett. 2018;430:47–56. | ||
Junttila TT, Li J, Johnston J, et al. Antitumor efficacy of a bispecific antibody that targets HER2 and activates T cells. Cancer Res. 2014;74(19):5561–5571. | ||
Force J, Howie LJ, Abbott SE, et al. Early stage HER2-positive breast cancers not achieving a pcr from neoadjuvant trastuzumab- or pertuzumab-based regimens have an immunosuppressive phenotype. Clin Breast Cancer. 2018;18(5):410–417. | ||
Ye JC, Formenti SC. Integration of radiation and immunotherapy in breast cancer – treatment implications. Breast. 2018;38:66–74. | ||
Hu ZI, Ho AY, McArthur HL. Combined radiation therapy and immune checkpoint blockade therapy for breast cancer. Int J Radiat Oncol Biol Phys. 2017;99(1):153–164. | ||
Ishihara D, Pop L, Takeshima T, Iyengar P, Hannan R. Rationale and evidence to combine radiation therapy and immunotherapy for cancer treatment. Cancer Immunol Immunother. 2017;66(3):281–298. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.