")
Back to Journals » Journal of Inflammation Research » Volume 14
Immune Dysfunction is Associated with Readmission in Survivors of Sepsis Following Infected Pancreatic Necrosis
Authors Yin J, Mao W, Xiao X, Yu X , Li B, Chen F, Lin J, Zhou J, Zhou J, Tong Z, Ke L , Li W
Received 24 May 2021
Accepted for publication 11 October 2021
Published 20 October 2021 Volume 2021:14 Pages 5433—5442
DOI https://doi.org/10.2147/JIR.S321507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Monika Sharma
Jiangtao Yin,1,2,* Wenjian Mao,1,* Xiaojia Xiao,3 Xianqiang Yu,4 Baiqiang Li,5 Faxi Chen,5 Jiajia Lin,5 Jing Zhou,1 Jing Zhou,4 Zhihui Tong,5 Lu Ke,5 Weiqin Li1,5
1Department of Critical Care Medicine, Jinling Hospital, Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Intensive Care Unit, Affiliated Hospital of Jiangsu University, Zhenjiang, People’s Republic of China; 3Department of Critical Care Medicine, Jinling Hospital of Southern Medical University, Nanjing, People’s Republic of China; 4Southeast University School of Medicine, Nanjing, People’s Republic of China; 5Department of Critical Care Medicine, Jinling Hospital, Nanjing University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lu Ke; Weiqin Li
Department of Critical Care Medicine, Jinling Hospital, Medical School of Nanjing University, 305 East Zhongshan Road, Nanjing, 225001, People’s Republic of China
Email [email protected]; [email protected]
Objective: Immunosuppression is common in patients with infected pancreatic necrosis (IPN) and associated with morbidity and mortality. This study aimed to investigate the impact of immune status on mortality and readmission after hospital discharge in patients with IPN-related sepsis.
Methods: In this prospective observational study, eligible adult patients with IPN-related sepsis requiring ICU admission were included. Monocytic human leukocyte antigen DR (mHLA-DR), expression of regulatory T cells (Treg), and neutrophil CD88 (nCD88) were measured on the diagnosis of sepsis, ICU discharge, hospital discharge, and 15, 30, 60 days after hospital discharge. Logistic regression model was used to assess potential risk factors for readmission 60-days within the index discharge.
Results: A total of 53 patients were included, 13 died during hospitalization and one withdrew the consent soon after discharge. Among the survivors, a tendency of immune recovery was observed during the consecutive follow-ups, evidenced by the increased expression of mHLA-DR. Sixteen patients (41.03%) were readmitted within 60 days after the index discharge. In the multivariable regression model, APACHE II score when sepsis was diagnosed > 9 and mHLA-DR at discharged < 14,591 AB/C were found to be independent risk factors affecting readmission.
Conclusion: Immunosuppression is common in patients with IPN-related sepsis and can persist until two months after discharge. The compromised mHLA-DR level at discharge was associated with readmission within two months after discharge.
Keywords: infected pancreatic necrosis, sepsis, immunosuppression, monocyte HLA-DR, readmissions
Introduction
Acute pancreatitis (AP) is a common gastrointestinal disease with clinical features ranging from local pancreatic inflammation to severe systemic complications. Most patients have mild and self-limiting courses with a low risk of death. However, approximately 10–20% of patients have a more severe type of disease characterized by the presence of pancreatic necrosis, and there are about 30% of these patients develop infected pancreatic necrosis (IPN), which carries a mortality of 20–30% due to its related septic complications.1
It is widely accepted that the mononuclear macrophage system, endothelial cells, and neutrophils are activated almost simultaneously in the early phase of AP, promoting the release of inflammatory cytokines and leading to extensive destruction of pancreatic tissue and injury of remote organs.2 Moreover, previous studies showed that immunosuppression illustrated by compromised monocyte function, declined T cell proliferation, and unbalanced T cell subsets could occur very early during the course and persist, being associated with increased disease severity, development of sepsis, or decreased survival.3–9 However, the fluctuation of immune status in the IPN patients after discharge was not studied before.
Unlike other abdominal infections, management of IPN is commonly time-consuming due to its complexity, which means immunosuppression could persist for long once it occurs, potentially leading to secondary infection, persistent inflammation, immunosuppression, and catabolism syndrome (PICS), and hospital readmission.10 Although the development of sepsis-induced immunosuppression during the hospital stay is well documented,11 to date, there are almost no data after hospital discharge in survivors of IPN. It is reported that sepsis patients with immunosuppression have poor long-term outcomes and worse quality of life after hospital discharge, even if they were deemed clinically cured when discharged.12 Readmission is also common in patients with IPN and associated with higher 1-year mortality, as previously reported.13 In previous studies,14,15 immunocompromised status was a positive predictor of late readmission for sepsis patients. However, the association between immunosuppression and readmission in AP has not been studied yet.
The aim of our study was to investigate the impact of immune status on mortality and 60-day readmission in patients with IPN-induced sepsis by measuring the expression of monocytic human leukocyte antigen DR (mHLA-DR), regulatory T cells (Treg), and neutrophil CD88 (nCD88). We chose these three immune markers because they could represent both innate and acquired immunity, and they were reported to be associated with nosocomial infection and immune dysfunction in critically ill patients.16
Materials and Methods
Study Oversight
This is a single-center, prospective, observational cohort study. The protocol was approved by the ethics committee of the Jinling hospital. Besides, written informed consent for this study was obtained from each patient or their next of kin before study commencement.
Patients
All adult patients (aged ≥18 years) diagnosed with IPN admitted to the Center of Severe Acute Pancreatitis (CSAP) of Jinling Hospital were followed up for potential inclusion from December 2018 to July 2019. They were enrolled when they developed sepsis according to “The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)”.17 Patients who met the following criteria were excluded: (1) were pregnant or lactating; (2) were expected to die within 48 hours: defined as those with norepinephrine usage at a dose of 25 mg/min or more under full-fluid resuscitation, with a systolic blood pressure <90mm Hg and serum pH values <7.0; (3) had a history of immune diseases or long-term administration of immunosuppressive drugs; (4) had preexisting cancer.
Healthy Volunteers
Eligibility criteria: (1) 18 to 70 years of age; (2) able and willing to complete the informed consent process. Exclusion criteria: (1) pregnant or lactating; (2) with a history of immune diseases or long-term administration of immunosuppressive drugs; (3) with a history of cancer.
Diagnosis and Definitions
AP and IPN were defined according to the Determinant-Based Classification of Acute Pancreatitis and the revision of the Atlanta Classification in 2012.1,18 Acute respiratory distress syndrome (ARDS) and acute kidney injury (AKI) were defined according to the Berlin definition and KDIGO Clinical Practice Guideline.19,20 The criteria for PICS were as follows: admission to the ICU >14 days; C-reactive protein (CRP) >50 mg/L; total lymphocyte count (TLC) <0.80×109 cell/L; serum albumin (Alb) <30.0 g/L and weight loss >10% during ICU hospitalization.21 A daily enteral nutrition intake of 70% or more of the target calorie was defined as target reaching of enteral nutrition (EN).22 The primary outcome of the study was readmission, defined as those readmitted to the hospital within 60 days of discharge from the index admission. Readmission within 72 hours of discharge was counted as the same admission.
Management
The treatment of AP and sepsis was carried out according to the international guidelines,23,24 including appropriate fluid resuscitation, early enteral feeding, antibiotics when necessary, and analgesia treatment when necessary, and avoiding surgery in patients with sterile necrosis. We adopted the step-up and delayed approach for IPN management, and intervention could be either endoscopic or surgical based on the location and extent of the collections. An empirical antibiotic regimen was applied for IPN, and aerobic and anaerobic Gram-negative and Gram-positive microorganisms were broadly covered. Targeted anti-infection treatment was based on microbial cultures, such as specimens of sputum, blood, and drain. Transfusion was applied strictly following the guidelines.25
Clinical Data Collection
The following data were collected at enrollment (when IPN-related sepsis was diagnosed): age, gender, body mass index (BMI), etiology, acute physiology and chronic health evaluation (APACHE) II score, blood cells count, the level of albumin, prealbumin, C-reactive protein (CRP), lactic acid and procalcitonin (PCT). Furthermore, the systemic complications, organ support therapy, microorganism culture results from the blood culture or infected pancreatic necrosis, development of PICS, hospital stay, ICU stay, and total cost were documented until hospital discharge or death. All the study patients were followed up until death or for 60 days after the index hospital discharge.
Blood Sampling and Measurements
Blood samples were obtained from all of the enrolled patients at six prospectively designated time points where possible: at enrollment when sepsis was diagnosed (T1), at ICU discharge if available (T2), at hospital discharge (T3), and at 15 (T4), 30 (T5) and 60 (T6) days after discharge. Immune function test included mHLA-DR, expression of Treg, and nCD88. Laboratory results from the blood routines were also obtained at the same time points. All survivors were contacted by telephone and asked to come back to the lab for blood sampling.
All samples were collected using EDTA tubes and tested within an hour after sampling according to the standard procedure. Measurement of the three markers was performed using flow cytometry (NovoCyte, ACEA biosciences, San Diego, CA, USA) according to the recommendations of the manufacturer (Anti-HLA-DR/Anti-Monocyte, BD Biosciences, San Jose, CA, USA; Human Regulatory T Cell Cocktail, BD Biosciences, San Jose, CA, USA; Anti-hC5a R1, R&D systems, Minneapolis, MN, USA). Results were expressed as the number of anti-HLA-DR antibodies per cell (AB/C), and the normal reference is more than 15,000 according to previous studies.12 Expression of Treg was measured based on the expression of CD4, CD25, and CD127 as the proportion of the total number of CD4+ T cells, and the nCD88 was described by expression rate. The median levels of HVs were served as the reference for the latter two parameters. The researchers who performed the immunophenotyping were blinded to the clinical information of the study patients.
Statistical Analysis
Categorical variables were reported as frequencies and proportions. Comparison of categorical data between two groups was performed using the Fisher’s exact test or the Chi-square test as indicated. Student’s t-test or Mann–Whitney’s test was adopted to analyze continuous variables. Two-way repeated measurements of mHLA-DR, Treg, and mCD88 at different time points were analyzed by generalized estimating equations (GEE).26 The association between the potential risk factors and the outcome of interest (readmission within 60 days after the index discharge) was evaluated by univariable logistic regression. Receiver Operating Characteristic (ROC) analysis was used to evaluate the effectiveness of continuous variables in predicting readmission and determine their cutoff value. Only those showing statistical significance (P < 0.10) in the univariable analysis would then enter multivariate regression analysis to determine the independent risk factors for readmission. A P < 0.05 was considered statistically significant. Calculations were performed using SPSS 22.0 (Chicago, IL).
Results
Clinical Characteristics Between Survivors and Non-Survivors
As shown in Figure 1, from December 2018 to July 2019, a total of 53 IPN patients with sepsis were enrolled. The last follow-up was completed in September 2019. Of these study subjects, 40 survived, and 13 (24.5%) died during hospitalization because of sepsis-related multiple organ failures. One survivor withdrew the consent soon after discharge and was therefore excluded in the analysis of readmission. Ten healthy volunteers (HVs) were recruited and sampled as a control group (gender, seven males (70%); mean±SD of age, 38.4±11.4).
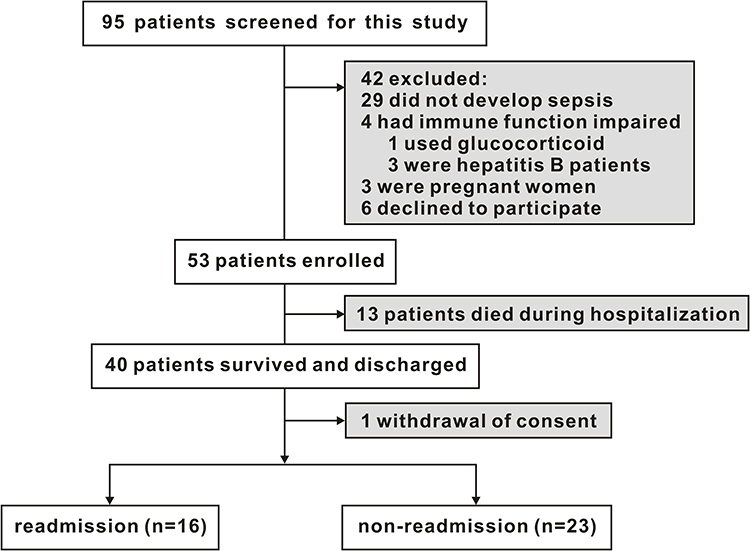 |
Figure 1 Flow chart of the participants. |
The baseline characteristics of these patients are shown in Table 1. The APACHE II score, SOFA score, PCT level, and IL-6 when sepsis was diagnosed were significantly lower in the survivors (both P < 0.05). For the local complications, the extent of necrosis was comparable between groups, while more extrapancreatic collections were seen in the non-survivors group (P < 0.05). The survivors showed higher prealbumin levels when sepsis was diagnosed compared with non-survivors (P = 0.041). For immune status, the survivors showed higher mHLA-DR expression (P = 0.003), and lower Treg expression when sepsis was diagnosed (P = 0.044) (Table 1). The results of microorganisms culture showed that enterococcus faecium was found in 61.5% of the non-survivors compared with 20% in the survivors (p = 0.005) while fungus was found in 46.2% of non-survivors compared with 12.5% in the survivors (p = 0.009) (Table S1).
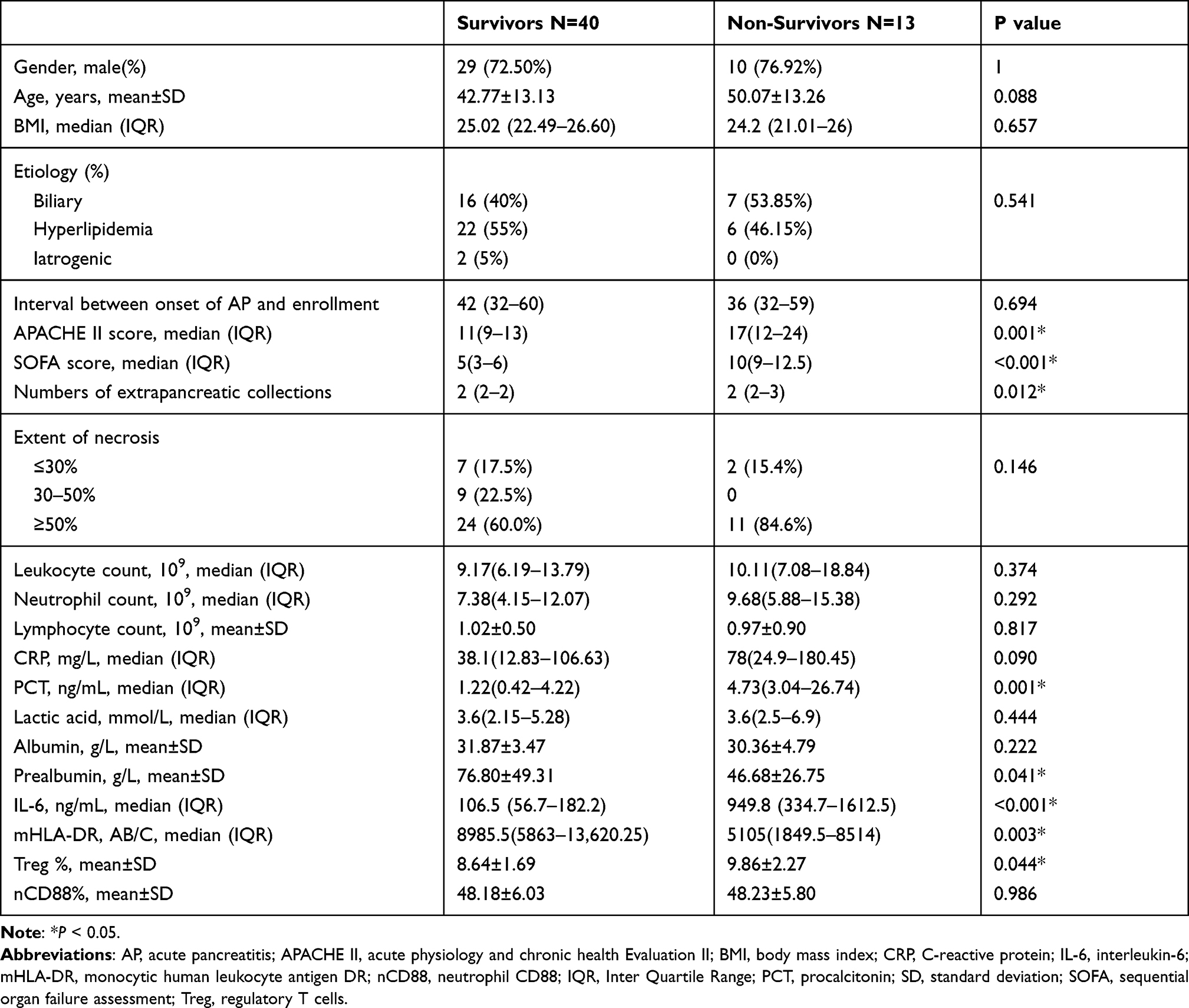 |
Table 1 Baseline Characteristics in Survivors and Non-Survivors |
The Immune Trajectory of the Survivors
Measurements were completed in 39, 39, 39, 38, 36, 37 survivors at T1-T6. For mHLA-DR, an incremental trend was observed among the survivors from enrollment to 60 days post-discharge (Figure 2A). The median level of mHLA-DR was above the normal reference (15,000 AB/C) at T3, which was at hospital discharge and kept above thereafter. Compared with the HVs, the study subjects showed significantly higher Treg levels at T5 (30 days after discharge) (Figure 2B) and lower nCD88 expression at T4 (15 days after discharge) (Figure 2C).
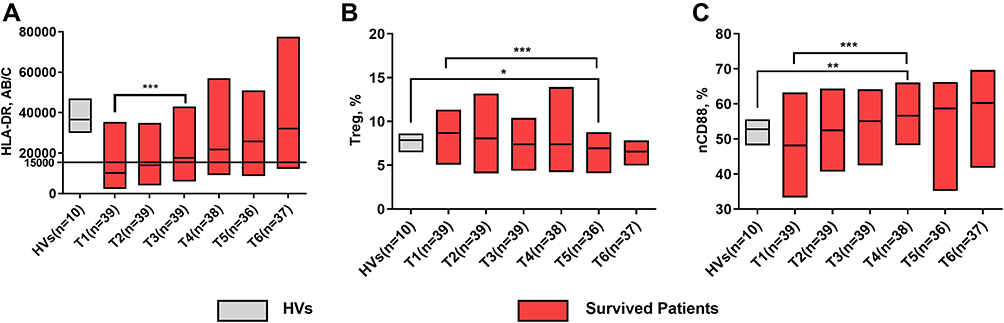 |
Figure 2 The immune trajectory of the survivors. (A) mHLA-DR expression from enrollment to 60 days post hospital discharge. (B) Treg expression from enrollment to 60 days post hospital discharge. (C) nCD88 expression from enrollment to 60 days post hospital discharge. Each band in the figure was shown as median (IQR). *P < 0.05; **P < 0.01; ***P < 0.001. |
The Clinical Implication of Immune Status
A total of 16 patients were readmitted after the index discharge (41.03%). Three were due to the suppressive symptoms resulting from pancreatic pseudocyst or walled-off necrosis, and the remaining 13 patients because of relapse of septic symptoms. The interval between the index discharge and readmission ranged from 14 to 58 days. Analyses for dynamic changes of mHLA-DR, Treg, and nCD88 showed that the mHLA-DR of the readmission group was significantly lower than that of the non-readmission group (P = 0.001) with β of 6120.0 (95% CI 2507.4–9732.6), while no difference was detected for Treg and nCD88 (Figure 3).
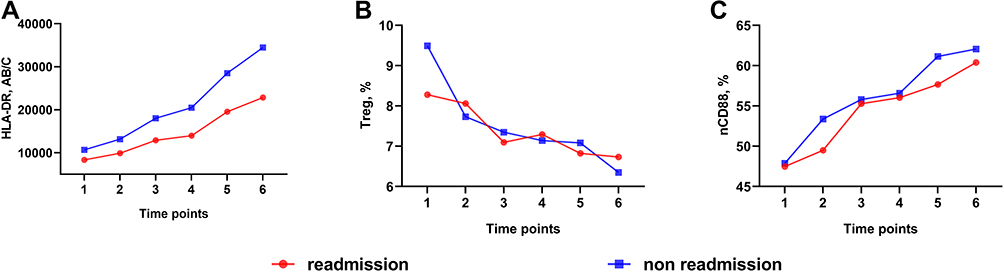 |
Figure 3 Generalized estimating equations of three immune markers between the two groups. (A) The evolution of mHLA-DR was different between the two groups (P = 0.001). (B and C) There was no difference between the two groups of the evolution of Treg and nCD88 (P > 0.05). |
For other clinical parameters, the target-reaching of EN at day 7 after enrollment was significantly lower (43.75% vs 82.61%, P = 0.017) in the readmission group. Furthermore, the APACHE II score when sepsis was diagnosed was also different between groups (Table S2). Besides, the expression of mHLA-DR at T3, T4, and T5 in the readmission group was much lower than the non-readmission group (Table S3).
ROC analysis demonstrated that age (Figure 4A), prealbumin when sepsis was diagnosed (Figure 4B), APACHE II score when sepsis was diagnosed (Figure 4C), and mHLA-DR at discharged (Figure 4D) had optimal predictive value for readmission, with the area under the curve (AUC) of 0.692, 0.711, 0.705 and 0.798, respectively. In the multivariable analysis, APACHE II score when sepsis was diagnosed >9 and mHLA-DR at discharged <14,591 AB/C were found to be independent risk factors affecting readmission (OR = 23.493, 95% CI: 1.111–496.573, P = 0.043 and OR = 22.545, 95% CI: 1.158–438.874, P = 0.040) (Table 2).
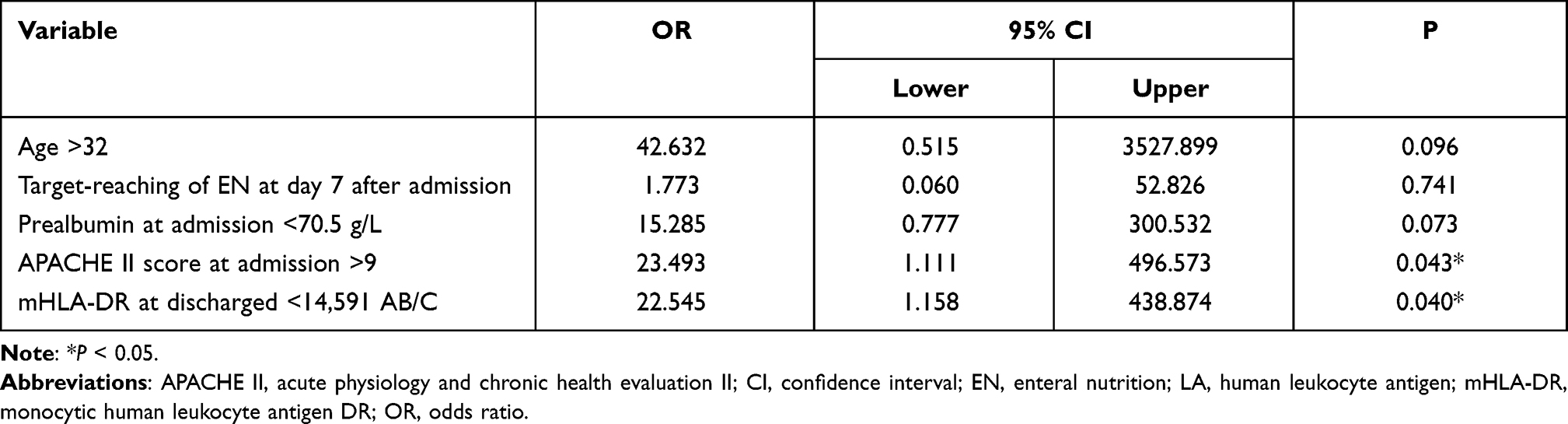 |
Table 2 Independent Risk Factors in a Multivariate Logistic Regression Analysis of Readmission |
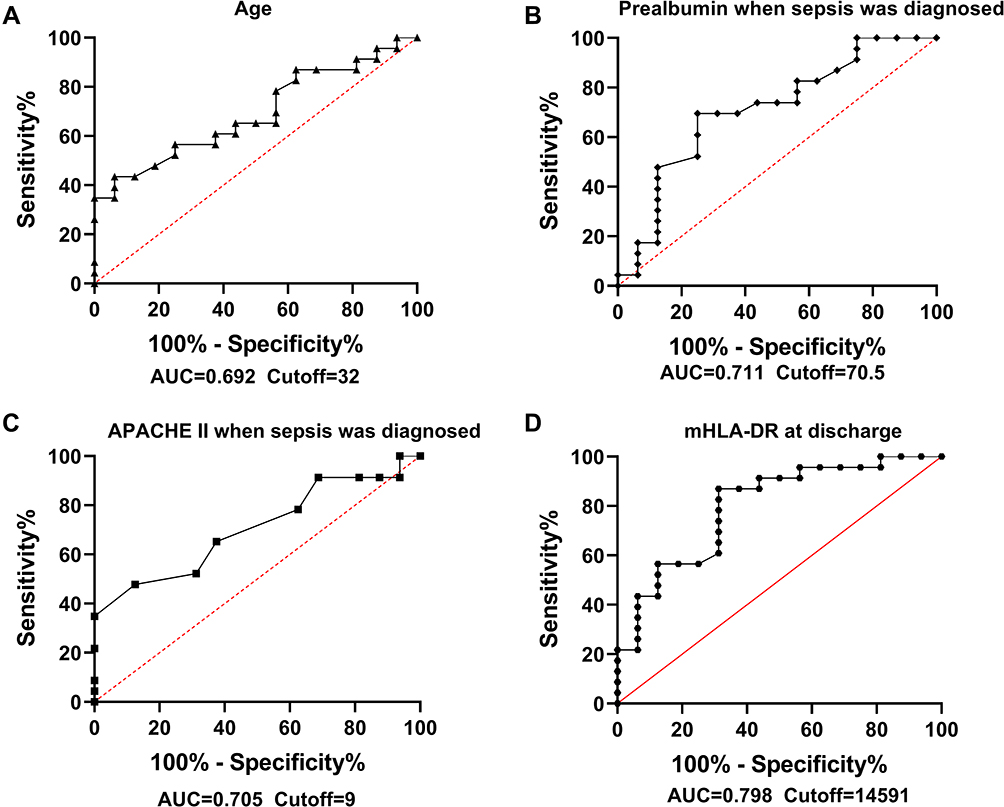 |
Figure 4 Receiver operator characteristic analysis for age (A), prealbumin when sepsis was diagnosed (B), APACHE II score when sepsis was diagnosed (C) and mHLA-DR at discharged (D). |
Discussion
The fluctuation of immune function was rarely studied in AP patients, especially those with IPN, a pivotal complication during the late phase of the disease and was thought to be associated with impaired immune function.27 This study found that cellular immunosuppression developed in patients with IPN-related sepsis during hospitalization and may persist until two months after discharge in some patients. Moreover, the severity and duration of immunosuppression were associated with adverse clinical events like in-hospital death and readmission. The expression of mHLA-DR at hospital discharge, APACHE II score when sepsis was diagnosed were associated with readmission.
Currently, few markers could accurately reflect the immune status in critically ill patients. Conway Morris et al found that dysfunction of mHLA-DR, Treg, and nCD88 can predict nosocomial infection and immune dysfunction in critically ill patients.16 The expression of mHLA-DR is a well-established biomarker for immune function, reflecting the ability of antigen presentation and frequently used in previous clinical studies.12,28,29 Furthermore, the reduction of mHLA-DR was demonstrated to be an independent risk factor of nosocomial infection and mortality.30 In previous studies conducted in AP patients, a reduced proportion of mHLA-DR in the early stage was associated with increased disease severity, development of secondary infection, or decreased survival, raising an association between immunosuppression and poor in-hospital prognosis.3–9 Early in 2004, Mentula et al4 have studied 74 patients with acute pancreatitis (AP) admitted within 72 h after symptom onset and found that a reduced proportion of mHLA-DR was associated with secondary infection of pancreatic necrosis. However, no follow-up was arranged after discharge in their study.
In 2005, Wolf-Dietrich Docke et al have proposed a reference value of mHLA-DR using the median level of 100 healthy participants (25,700 AB/C (2.5%–97.5%, 14,100–42,500 AB/C)).12 They also proposed preliminary cutoffs for diagnosis and classification of immunosuppression (15,000 AB/C as indicative of immunocompetence; 5000–15,000 AB/C as indicative of moderate to severe immunodepression; 5000 AB/C as indicative of immunoparalysis). In the present study, only 24 of the 39 (61.54%) survivors were deemed immunocompetent at hospital discharge with mHLA-DR above 15,000 AB/C, suggesting a substantial incidence of persistent immunosuppression in the study population. Moreover, the cutoff values of the study markers were determined by ROC analysis in this study. Interestingly, the optimal cutoff value of the mHLA-DR was almost consistent with the standardized cutoff value of 15,000 AB/C.
Treg is a specialized subpopulation of T lymphocytes that act to suppress immune response.31 A persistent increase in the proportion of Treg suggests immunosuppression and poor prognosis in patients with septic shock.32 The nCD88 is the receptor of C5a, and its reduced expression could represent C5a-mediated neutrophil dysfunction, which was reported to predict the acquisition of nosocomial infection in critically ill patients.33 Therefore, to comprehensively assess different aspects of the immune system, the percentage of Treg and nCD88 were also tested in addition to the mHLA-DR level in this study.
Hospital readmission was reported to be associated with increased mortality in AP.13 As an adverse event, rates of readmission after the resolution of an initial episode of AP ranged from 15% to 29% in previous studies,34,35 which are lower than what we found in our study. That should be due to the study population we chose, which is the most severe type of AP with both organ failure and infection and the relatively long follow-up period we applied (60 days after the index discharge). Previous studies conducted in AP mostly studied the 30-day readmission.36,37 It is true that 60-day readmission may be affected by more confounders, thereby bringing some bias. However, in our cohort, 12 out of the 16 readmissions occurred between 30 and 60 days, since the patients we studied had a higher incidence of PICS, which can persist for months and lead to readmission relatively later.21 Due to similar reasons, follow-up could be up to 90 days to observe readmission in patients with sepsis.38–40
Various risk factors for readmission have been identified before, including the severity of the initial episode of AP, male sex, necrotizing pancreatitis, tobacco smoking, continued alcohol use, idiopathic pancreatitis, and delay in receiving adequate treatment for the underlying cause of AP, such as cholecystectomy in cases of acute biliary pancreatitis.34,35,41–43 However, no studies investigated the impact of immune status on readmission after IPN. Our results showed that mHLA-DR at discharged <14,591 AB/C was associated with readmission, suggesting the clinical implication of persistent decreased mHLA-DR expression. In previous studies, the APACHE II score was frequently used to predicted readmission in sepsis/critical illness patients.44–46 We did not take the SOFA score into the regression model since both SOFA and APACHE II are severity scores with shared underlying data like creatinine, blood pressure, etc. We chose the APACHE II score for the regression model, as it is more sophisticated and comprehensive.
It was reported that immune suppression could persist in post-septic patients, leading to increased susceptibility to secondary infections.47,48 Our results are consistent with previous studies, showing that a significant part of patients with IPN-related sepsis did have long-term post-discharge immunosuppression, and recovery can take more than two months. Unlike other types of sepsis, patients with IPN commonly develop sepsis weeks after the onset of the primary disease.49 That means they can be exhausted both physically and mentally after long-term hospitalization when sepsis occurs, putting them at a higher risk of developing immunosuppression.12,50 However, almost all the enrolled survivors recovered from immunosuppression 60 days after discharge, which might be ascribed to the fact that our study patients were younger than those in the previous studies.
There are several limitations in the present study. First of all, there were some losses of follow-up, which may bring in bias. Moreover, due to the single-center design and small sample size, the clinical implication of this study should be cautiously interpreted. In addition, cytokine profiles and other immune markers, which might be informative, were not measured.
Conclusions
Immunosuppression could occur in patients with IPN-induced sepsis during hospitalization and persist for two months after discharge. The APACHE II score when sepsis was diagnosed and mHLA-DR at discharge were found to be independent risk factors for readmission within two months after discharge, although the predictive capacity of both was relatively low. The persistent immunosuppressive state of sepsis patients following IPN after discharge suggests close monitoring and immune enhancement therapy may be beneficial.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The protocol was approved by the ethics committee of the Jinling hospital (No. 2018NZKY-0020-01). Besides, written informed consent for this study was obtained from each patient or their next of kin before study commencement.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from National Nature Science Foundation of China (No. 81770641) and Zhenjiang Social Development Project (NO. SH2020057).
Disclosure
The authors declare that they have no competing interests.
References
1. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
2. Shrivastava P, Bhatia M. Essential role of monocytes and macrophages in the progression of acute pancreatitis. World J Gastroenterol. 2010;16(32):3995–4002. doi:10.3748/wjg.v16.i32.3995
3. Satoh A, Miura T, Satoh K, et al. Human leukocyte antigen-DR expression on peripheral monocytes as a predictive marker of sepsis during acute pancreatitis. Pancreas. 2002;25(3):245–250. doi:10.1097/00006676-200210000-00006
4. Mentula P, Kylänpää ML, Kemppainen E, et al. Plasma anti-inflammatory cytokines and monocyte human leucocyte antigen-DR expression in patients with acute pancreatitis. Scand J Gastroenterol. 2004;39(2):178–187. doi:10.1080/00365520310008278
5. Ho YP, Sheen IS, Chiu CT, Wu CS, Lin CY. A strong association between down-regulation of HLA-DR expression and the late mortality in patients with severe acute pancreatitis. Am J Gastroenterol. 2006;101(5):1117–1124. doi:10.1111/j.1572-0241.2006.00495.x
6. Chéron A, Monneret G, Landelle C, Floccard B, Allaouchiche B. [Low monocytic HLA-DR expression and risk of secondary infection]. Ann Fr Anesth Reanim. 2010;29(5):368–376. French. doi:10.1016/j.annfar.2010.02.015
7. Thomson JE, Brand M, Fonteh P. The immune imbalance in the second hit of pancreatitis is independent of IL-17A. Pancreatology. 2018;18(3):246–252. doi:10.1016/j.pan.2018.01.007
8. Munir F, Jamshed MB, Shahid N, et al. Advances in immunomodulatory therapy for severe acute pancreatitis. Immunol Lett. 2020;217:72–76. doi:10.1016/j.imlet.2019.11.002
9. Minkov G, Dimitrov E, Yovtchev Y, Enchev E, Lokova R, Halacheva K. Prognostic value of peripheral blood CD14+HLA-DR+ monocytes in patients with acute pancreatitis. J Immunoassay Immunochem. 2021;1–16. doi:10.1080/15321819.2021.1903491
10. Garg PK, Singh VP. Organ failure due to systemic injury in acute pancreatitis. Gastroenterology. 2019;156(7):2008–2023. doi:10.1053/j.gastro.2018.12.041
11. Zorio V, Venet F, Delwarde B, et al. Assessment of sepsis-induced immunosuppression at ICU discharge and 6 months after ICU discharge. Ann Intensive Care. 2017;7(1):80. doi:10.1186/s13613-017-0304-3
12. Döcke WD, Höflich C, Davis KA, et al. Monitoring temporary immunodepression by flow cytometric measurement of monocytic HLA-DR expression: a multicenter standardized study. Clin Chem. 2005;51(12):2341–2347. doi:10.1373/clinchem.2005.052639
13. Lee PJ, Bhatt A, Lopez R, Stevens T. Thirty-day readmission predicts 1-year mortality in acute pancreatitis. Pancreas. 2016;45(4):561–564. doi:10.1097/MPA.0000000000000463
14. Longo M, Pennington Z, Gelfand Y, et al. Readmission after spinal epidural abscess management in urban populations: a bi-institutional study. J Neurosurg Spine. 2019;32465–472.
15. Yende S, Kellum JA, Talisa VB, et al. Long-term host immune response trajectories among hospitalized patients with sepsis. JAMA Network Open. 2019;2(8):e198686. doi:10.1001/jamanetworkopen.2019.8686
16. Conway Morris A, Datta D, Shankar-Hari M, et al. Cell-surface signatures of immune dysfunction risk-stratify critically ill patients: INFECT study. Intensive Care Med. 2018;44(5):627–635. doi:10.1007/s00134-018-5247-0
17. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
18. Choi JH, Kim MH, Cho DH, et al. Revised Atlanta classification and determinant-based classification: which one better at stratifying outcomes of patients with acute pancreatitis? Pancreatology. 2017;17(2):194–200. doi:10.1016/j.pan.2017.01.004
19. Sjoding MW, Hofer TP, Co I, Courey A, Cooke CR, Iwashyna TJ. Interobserver reliability of the Berlin ARDS definition and strategies to improve the reliability of ARDS diagnosis. Chest. 2018;153(2):361–367. doi:10.1016/j.chest.2017.11.037
20. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–c184.
21. Hesselink L, Hoepelman RJ, Spijkerman R, et al. Persistent inflammation, immunosuppression and catabolism syndrome (PICS) after polytrauma: a rare syndrome with major consequences. J Clin Med. 2020;9(1):191. doi:10.3390/jcm9010191
22. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019;38(1):48–79.
23. Besselink M, van Santvoort H, Freeman Met al. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 Suppl 2):e1–e15. doi:10.1016/j.pan.2013.07.063
24. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377.
25. Sharma S, Sharma P, Tyler LN. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83(6):719–724.
26. Lee JH, Herzog TA, Meade CD, Webb MS, Brandon TH. The use of GEE for analyzing longitudinal binomial data: a primer using data from a tobacco intervention. Addict Behav. 2007;32(1):187–193. doi:10.1016/j.addbeh.2006.03.030
27. Akinosoglou K, Gogos C. Immune-modulating therapy in acute pancreatitis: fact or fiction. World J Gastroenterol. 2014;20(41):15200–15215. doi:10.3748/wjg.v20.i41.15200
28. Pfortmueller CA, Meisel C, Fux M, Schefold JC. Assessment of immune organ dysfunction in critical illness: utility of innate immune response markers. Intensive Care Med Exp. 2017;5(1):49. doi:10.1186/s40635-017-0163-0
29. Zhuang Y, Peng H, Chen Y, Zhou S, Chen Y. Dynamic monitoring of monocyte HLA-DR expression for the diagnosis, prognosis, and prediction of sepsis. Front Biosci. 2017;22:1344–1354. doi:10.2741/4547
30. Raffray L, Burton RJ, Baker SE, Morgan MP, Eberl M. Zoledronate rescues immunosuppressed monocytes in sepsis patients. Immunology. 2020;159(1):88–95. doi:10.1111/imm.13132
31. Allos H, Al Dulaijan BS, Choi J, Azzi J. Regulatory T cells for more targeted immunosuppressive therapies. Clin Lab Med. 2019;39(1):1–13. doi:10.1016/j.cll.2018.11.001
32. Carvelli J, Piperoglou C, Bourenne J, et al. Imbalance of circulating innate lymphoid cell subpopulations in patients with septic shock. Front Immunol. 2019;10:2179. doi:10.3389/fimmu.2019.02179
33. Jeong JH, Jung JH, Lee JS, et al. Prominent inflammatory features of monocytes/macrophages in acute calcium pyrophosphate crystal arthritis: a comparison with acute gouty arthritis. Immune Netw. 2019;19(3):e21. doi:10.4110/in.2019.19.e21
34. Suchsland T, Aghdassi A, Kühn K, et al. Predictive factors for and incidence of hospital readmissions of patients with acute and chronic pancreatitis. Pancreatology. 2015;15(3):265–270. doi:10.1016/j.pan.2015.03.008
35. Vipperla K, Papachristou GI, Easler J, et al. Risk of and factors associated with readmission after a sentinel attack of acute pancreatitis. Clin Gastroenterol Hepatol. 2014;12(11):1911–1919. doi:10.1016/j.cgh.2014.04.035
36. Bolourani S, Diao L, Thompson DA, et al. Risk factors for early readmission after acute pancreatitis: importance of timely interventions. J Surg Res. 2020;252:96–106. doi:10.1016/j.jss.2020.03.003
37. Argueta PP, Salazar M, Vohra I, et al. Thirty-day readmission among patients with alcoholic acute pancreatitis. Dig Dis Sci. 2021. doi:10.1007/s10620-020-06765-7
38. Wiley MR, Carreon LY, Djurasovic M, et al. Economic analysis of 90-day return to the emergency room and readmission after elective lumbar spine surgery: a single-center analysis of 5444 patients. J Neurosurg Spine. 2020;34:89–95.
39. Stenholt POO, Abdullah S, Sørensen RH, Nielsen FE. Independent predictors for 90-day readmission of emergency department patients admitted with sepsis: a prospective cohort study. BMC Infect Dis. 2021;21(1):315. doi:10.1186/s12879-021-06007-9
40. Guirgis FW, Brakenridge S, Sutchu S, et al. The long-term burden of severe sepsis and septic shock: sepsis recidivism and organ dysfunction. J Trauma Acute Care Surg. 2016;81(3):525–532. doi:10.1097/TA.0000000000001135
41. Yadav D, Lee E, Papachristou GI, O’Connell M. A population-based evaluation of readmissions after first hospitalization for acute pancreatitis. Pancreas. 2014;43(4):630–637. doi:10.1097/MPA.0000000000000078
42. Bejarano González N, Romaguera Monzonís A, García Borobia FJ, et al. Influence of delayed cholecystectomy after acute gallstone pancreatitis on recurrence. Consequences of lack of resources. Rev Esp Enferm Dig. 2016;108(3):117–122.
43. Ahmed Ali U, Issa Y, Hagenaars JC, et al. Risk of recurrent pancreatitis and progression to chronic pancreatitis after a first episode of acute pancreatitis. Clin Gastroenterol Hepatol. 2016;14(5):738–746. doi:10.1016/j.cgh.2015.12.040
44. Rosenberg AL, Watts C. Patients readmitted to ICUs*: a systematic review of risk factors and outcomes. Chest. 2000;118(2):492–502. doi:10.1378/chest.118.2.492
45. Azoulay E, Adrie C, De Lassence A, et al. Determinants of postintensive care unit mortality: a prospective multicenter study. Crit Care Med. 2003;31(2):428–432. doi:10.1097/01.CCM.0000048622.01013.88
46. Campbell AJ, Cook JA, Adey G, Cuthbertson BH. Predicting death and readmission after intensive care discharge. Br J Anaesth. 2008;100(5):656–662. doi:10.1093/bja/aen069
47. Marx G. Incidence of severe sepsis and septic shock in German intensive care units: the prospective, multicentre INSEP study. Intensive Care Med. 2018;44(1):153–156. doi:10.1007/s00134-016-4504-3
48. Delano MJ, Ward PA. Sepsis-induced immune dysfunction: can immune therapies reduce mortality? J Clin Invest. 2016;126(1):23–31. doi:10.1172/JCI82224
49. Jain S, Mahapatra SJ, Gupta S, et al. Infected pancreatic necrosis due to multidrug-resistant organisms and persistent organ failure predict mortality in acute pancreatitis. Clin Transl Gastroenterol. 2018;9(10):190. doi:10.1038/s41424-018-0056-x
50. Gukovskaya AS, Gukovsky I, Algül H, Habtezion A. Autophagy, inflammation, and immune dysfunction in the pathogenesis of pancreatitis. Gastroenterology. 2017;153(5):1212–1226. doi:10.1053/j.gastro.2017.08.071
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.