")
Back to Journals » OncoTargets and Therapy » Volume 12
Immune checkpoint inhibitors for small cell lung cancer: opportunities and challenges
Authors Regzedmaa O , Zhang H, Liu H, Chen J
Received 8 February 2019
Accepted for publication 11 May 2019
Published 13 June 2019 Volume 2019:12 Pages 4605—4620
DOI https://doi.org/10.2147/OTT.S204577
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Carlos E Vigil
Orgilmaa Regzedmaa,1 Hongbing Zhang,1 Hongyu Liu,2 Jun Chen1,2
1Department of Lung Cancer Surgery, Tianjin Lung Cancer Institute, Tianjin Medical University General Hospital, Tianjin 300052, People’s Republic of China; 2Tianjin Key Laboratory of Lung Cancer Metastasis and Tumor Microenvironment, Tianjin Lung Cancer Institute, Tianjin Medical University General Hospital, Tianjin 300052, People’s Republic of China
Abstract: Lung cancer is the most common cancer and the leading cause of cancer death worldwide, with an estimated 2.1 million new cases and 1.8 million deaths in 2018. Although small cell lung cancer (SCLC) is the most aggressive type of lung cancer, it shows high response rates to chemotherapy in early lines of therapy. Unfortunately, it is associated with rapid recurrence and relatively poor prognosis. Over the last few years, considerable progress has been made in cancer immunotherapy. One of the most promising ways to activate therapeutic antitumor immunity is via blockade of immune checkpoints, such as cytotoxic T lymphocyte-associated protein-4 (CTLA-4) and programmed cell death protein-1/programmed cell death ligand-1 (PD-1/PD-L1). Immune checkpoint inhibitors show promise as SCLC therapeutics. The overall expectation for immuno-oncology is high, and the outcomes of trials will hopefully reveal a variety of treatment options for SCLC patients. In this review, we discuss the discovery of new immune inhibitory and stimulatory pathways and rational combination strategies to explain the role of immunotherapy in SCLC and its future opportunities and challenges.
Keywords: small cell lung cancer, immune checkpoint inhibitors, CTLA4, cytotoxic T lymphocyte-associated protein4, PD1, programmed cell death protein1, PDL1, programmed cell death ligand 1, next generation of immune checkpoints
Introduction
Lung cancer is the most common cancer and the leading cause of cancer death worldwide, with an estimated 2.1 million new cases and 1.8 million deaths in 2018.1 Approximately 13% of lung cancer patients have small cell lung cancer (SCLC).2 Although this aggressive tumor shows high response rates to chemotherapy in early lines of therapy, it is associated with rapid recurrence and relatively poor prognosis and is often diagnosed at late stages with systemic metastasis.3,4 Thus, the 5-year survival of SCLC patients is very low and varies according to stage, with 5-year relative survival rates of 31% for limited-stage SCLC (LS-SCLC) but just 2% for extensive-stage SCLC (ES-SCLC).5
Because SCLC is generally highly sensitive to chemotherapy and radiation therapy, combined chemotherapy and radiotherapy has become the accepted standard treatment for all stages of SCLC. The standard chemotherapy regimen of cisplatin or carboplatin plus etoposide used as the first-line treatment of LS-SCLC and ES-SCLC diseases has not changed over the past four decades. Radiotherapy is administered to those patients with LS-SCLC whose cancer is confined to the chest in a single tolerable radiation field.6–8 Recently, the randomized phase III CONVERT trial9 was designed to show the superiority of once-daily concurrent radiotherapy. However, because it was not powered to show equivalence, the standard of care arguably remains twice-daily therapy, although its use is less frequent. These results indicate conventional or hyperfractionated radiotherapy as the potential standard of care in LS-SCLC. Although up to 80% of patients respond to first-line chemotherapy and radiation therapy, most rapidly relapse and show resistance to further therapies.
Recently, many improvements have been made to the fundamentals of SCLC treatment. The results of the CheckMate-032 study contributed to the first Food and Drug Administration (FDA)-accelerated approval for nivolumab (OPDIVO®, anti-programmed cell death protein-1 [PD1]) for the third-line treatment of metastatic SCLC in August 2018. However, the open-label Checkmate-331 study failed to meet the primary endpoint of overall survival (OS) compared with standard of care.10 Recently, the results of the IMpower study contributed to FDA-accelerated approval of the combination of atezolizumab (TECENTRIQ®) with carboplatin and etoposide in the frontline treatment of ES-SCLC in March 2019.11 The study demonstrated an overall survival benefit when the programmed cell death ligand-1 (PD-L1) inhibitor atezolizumab was added to platinum/etoposide chemotherapy for the initial treatment of ES-SCLC (median OS [mOS] of 12.3 months in the atezolizumab group and 10.3 months in the placebo group; hazard ratio [HR] 0.70, 95% confidence interval [CI] 0.54–0.91, p=0.007).12 In Figure 1, we summarize the standard of care therapies and new therapies that have been approved by the FDA.
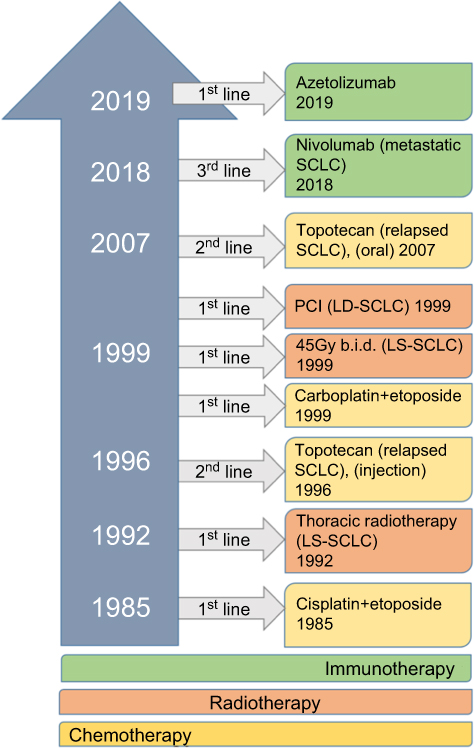 | Figure 1 Timeline of treatment for SCLC. This timeline illustrates the standard of care therapies and new therapies that have been approved by the FDA. |
Additionally, the FDA has granted a priority review designation to a supplemental biologics license application (sBLA) for pembrolizumab (KEYTRUDA®) as a treatment for patients with advanced SCLC whose disease has progressed after two or more prior lines of therapy.13 The application is based on findings from cohorts of the phase II KEYNOTE-158 and phase Ib KEYNOTE-028 studies, in which pembrolizumab elicited 19% and 33% overall response rates (ORRs) in patients with advanced and ES-SCLC, respectively.14,15
The immune system can recognize physiological and pathological changes at the cellular level. After tumorigenesis, tumor-associated antigens can be presented by antigen-presenting cells (APCs) to major histocompatibility complex (MHC) I and then recognized by T cell receptor on CD8 cytotoxic T cells. T cell activation is induced by a secondary co-stimulatory signal, namely, the binding of B7 protein on APCs to CD28 on cytotoxic T cells. Afterward, the activated T cell induces the death of the physiologically and pathologically altered cell. Conversely, the activated T cells are negatively regulated by increased expressed of cytotoxic T lymphocyte-associated protein 4 (CTLA-4), which has a higher affinity for B7 protein of APCs than the CD28 molecule of cytotoxic T cells.16 CTLA-4 is normally expressed in regulatory T cells (Tregs) and acts as a restraint molecule of the activated immune system, suppressing auto-reactivity. Similar to the CTLA-4 molecule, PD-1 is an immune checkpoint inhibitor in activated T cells, peripheral B cells, and myeloid cells. In contrast, the binding of PD-1 to PD-L1 on tissues or hematopoietic cells occurs in the late phase and thereby mainly suppresses activated T cells in peripheral immune effector sites rather than in central lymph systems.17,18 Overexpression of tumor-specific antigens on tumor cells can facilitate their recognition by the host immune system, especially by T cells.19 CTLA-4 and PD-1 are recognized as inhibitors of immune effector cells and they therefore contribute to the rapid development of cancer cells due to inactivation of the immune system during tumorigenesis.
Because SCLC has the highest rate of tumor mutational burden (TMB), the tumor should be sensitive to immune-based therapeutic approaches.20,21 TMB is used as a predictor of immune checkpoint inhibitor efficacy for many cancer types.22 In Helmann et al,23 the objective response rate was 21.3% in the high TMB group (248 mutations on whole-exome sequencing) but just 4.8% in the lower TMB group (0 to 142 mutations). PD-L1 expression has been applied as a biomarker to predict the efficacy of PD-1/PD-L1 inhibitors in relation to the dynamic and heterogeneous expression of PD-L1 in the tumor microenvironment.24 Immune checkpoint molecules are frequently overexpressed in SCLC-associated tumor-infiltrating lymphocytes.25 Figure 2 summarizes the inhibitory and stimulatory molecules and their targets. Cancer immunotherapy research achievements can represent a new hope for SCLC patients and confer them with improved and sustainable survival opportunities. Thus, in this review, we aim to provide an up-to-date overview of recent developments in immune checkpoint therapy and novel immune checkpoint agents and combination therapies in SCLC, focusing on clinical trials.
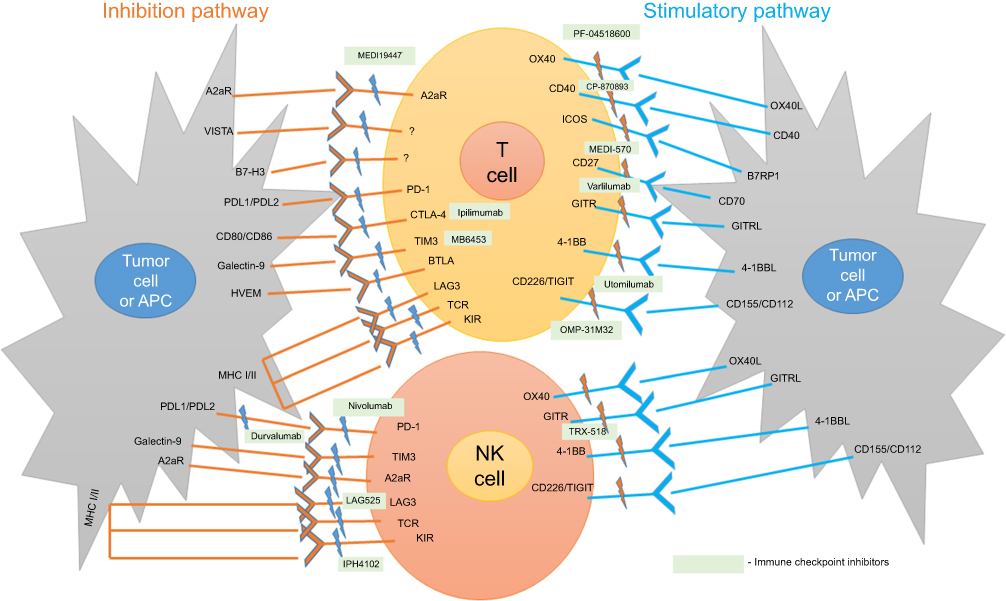 | Figure 2 Immunosuppressive and immunostimulatory checkpoints and their targets. T cells recognize antigens presented by MHC complex on APCs or tumor cells through T cell receptor (TCR). Many of the ligands bind to multiple receptors; some deliver co-stimulatory signals, whereas others deliver inhibitory signals. Full activation of T cells is mediated by binding of CD28 to B7. CTLA-4 competes with CD28 for binding to B7 and transmits an inhibitory signal suppressing T cell activation. PD-1 is expressed on T and NK cells after antigen exposure. Following binding of PD-1 to its ligands, such as PD-L1/PD/L2 (expressed on tumor cells or APCs), an inhibitory signal turns off the immune response mediated by activated T and NK cells. A2aR is expressed on T and NK cells, similar to PD-1. As in CTLA-4 and PD-1 pathways, a significant influence of A2aR signaling on Tregs and effector T cells is likely to be the fundamental driving force behind its immunosuppressive effect. TIM3 is an inhibitory receptor expressed by T and NK cells that interacts with soluble or cell surface galectin 9 to negatively regulate T and NK cell function. BTLA is an inhibitory receptor that is structurally and functionally related to CTLA-4 and PD-1 and expressed by T cells. LAG3 is a receptor that forwards inhibitory signals to activated T and NK cells through LAG3/TCR-MHC interaction, leading to downregulation of immune responses. KIR receptors are expressed on NK cells and to a lesser extent on CD8+ T cells. The binding of inhibitory KIRs (inhKIRS) to their ligands (HLA class I molecule) protects normal cells against the NK cell attack. In contrast, in cancer, higher expression of inhKIRs on the surface of NK and T cells promotes a downregulation of their function. OX40 is a stimulatory receptor, highly expressed by activated T cells and to a lesser degree by NK cells. OX40 and its ligand OX40L play a pivotal role in the activation, potentiation, proliferation, and survival of T cells and in modulating NK cell function. CD40 is a stimulatory receptor expressed on T cells. The interaction between CD40 and CD154 stimulates cytokine secretion by B cells with subsequent T cell activation and tumor cell death. The levels of ICOS, a specific T cell co-stimulatory receptor expressed on T cells, are upregulated in activated T cells, particularly after the use of anti-CTLA-4 therapies. CD27 is a stimulatory receptor expressed on T cells. CD27–CD70 binding results in a potent signal that activates and differentiates T cells into effector and memory cells and boosts the level of B cells. GITR is a co-stimulatory receptor expressed on T and NK cells. 4-1BB is an inducible co-stimulatory receptor expressed on T and NK cells. The interaction between 4-1BB and 4-1BBL triggers subsequent immune cell proliferation and activation, particularly of T and NK cells. TIGIT is a member of CD28 family-like receptors expressed on T and NK cells. It exerts direct immunosuppressive effects on these cells and indirectly increases the release of immunoregulatory cytokines, decreases the production of interferon-γ and IL-7, and prevents maturation of dendritic cells. |
The CTLA-4 pathway and CTLA-4 checkpoint inhibitors
CTLA-4 was the first immune checkpoint receptor to be targeted by a therapeutic agent.26 Monoclonal antibodies against CTLA-4 (ipilimumab and tremelimumab) are designed to prevent the interaction between CTLA-4 and its ligands (CD80/CD86). In this manner, they blockade the inhibitory signal provided by CTLA-4 and enhance the activation and proliferation of tumor-specific T cells, facilitating an effective immune response against tumor cells. In 2011, ipilimumab became the first immune checkpoint inhibitor to be approved by the FDA.27–29 As shown in Table 1, ipilimumab has been investigated in combination with chemotherapy in patients with SCLC.30–32
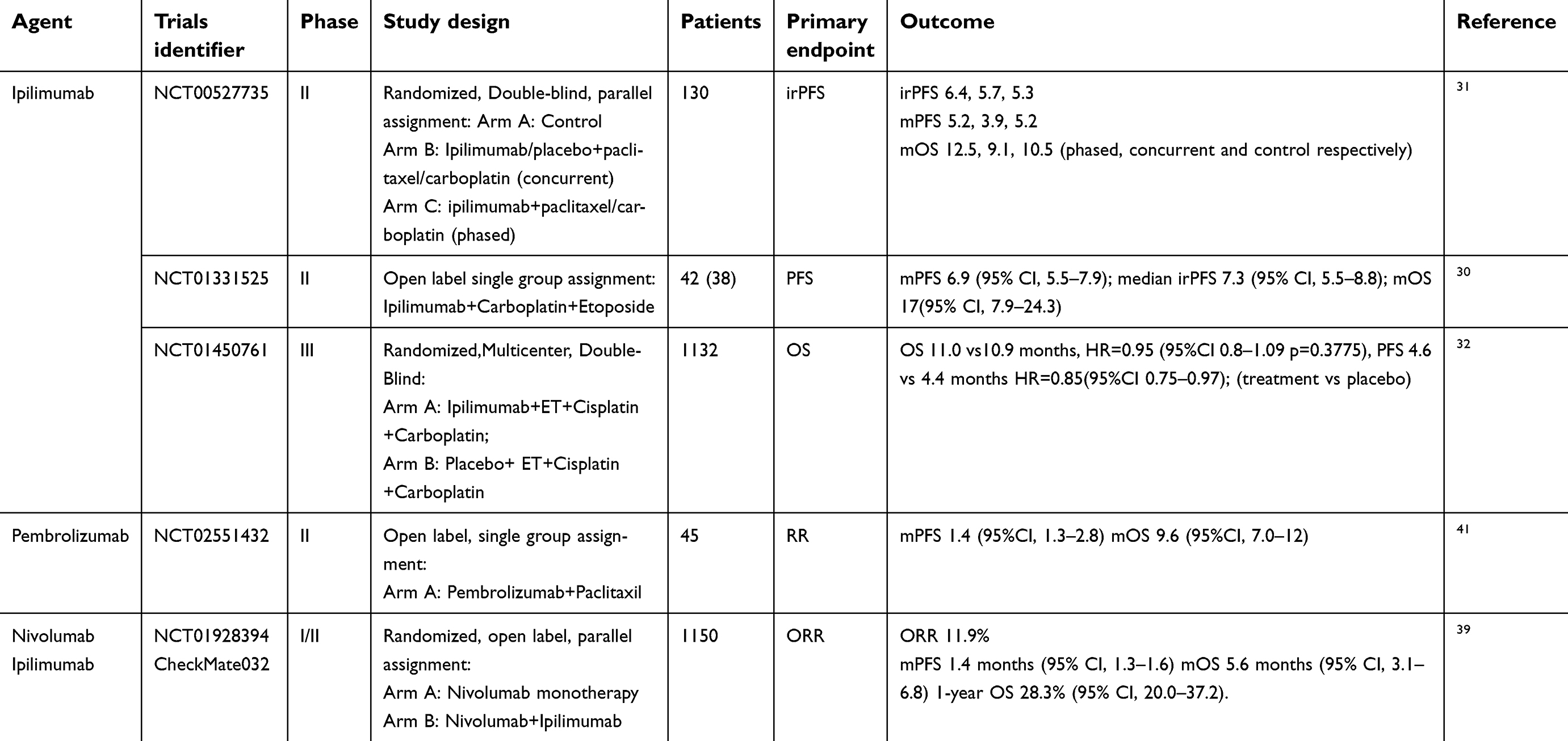 | Table 1 Complete trials of immunotherapy agents in SCLC |
Ipilimumab has achieved promising results in SCLC treatment.33 In a three-arm phase II trial (NCT00527735), patients received either six cycles of carboplatin and paclitaxel with or without ipilimumab or with ipilimumab in a phased schedule.31 The immune-related progression-free survival (irPFS) was significantly prolonged for the phased ipilimumab arm (6.4 vs. 5.3 months, HR 0.64, P=0.03) but was not prolonged for the concurrent arm compared with the control (5.7 vs. 5.3 months, HR 0.75, P=0.11). There was also a nonsignificant trend for improved OS in the phased ipilimumab arm (mOS 12.5 months, 95% CI 7.9–14.9), compared with mOSs of 9.1 months (95% CI 6.7–13.0) for the concurrent arm and 10.5 months (95% CI 8.6–11.7) for the control arm. The HR values relative to control were 0.76 (95% CI 0.48–1.19, P=0.13) for phased ipilimumab and 0.89 (95% CI 0.57–1.39, P=0.41) for concurrent ipilimumab.31 There was also increased toxicity, with grade III and IV toxicities more common in the ipilimumab arms (30% control vs. 43% concurrent vs. 50% phased). The study did not identify any potential biomarkers that could predict the response to ipilimumab treatment in patients with SCLC (Table 1).
In an open-label phase II study30 of ipilimumab with carboplatin/etoposide for use as first-line treatment in previously untreated patients with ES-SCLC, patients received carboplatin and etoposide up to six cycles (3–6) with ipilimumab. The presence of autoantibodies (anti-SOX2, anti-HU, anti-Yo, anti-VGCCA, anti-VGPCA, thyroid peroxidase, rheumatoid factors, anti-muscle antibodies, ANA, and ANCA) was investigated at baseline in 38 patients. Ipilimumab in combination with carboplatin and etoposide might benefit a subgroup of patients with advanced SCLC. A positive autoimmune profile at baseline was associated with improved outcomes, with patients with any positive autoantibodies at baseline having a significantly longer median irPFS (8.8 months [95% CI 5.1–10.7] vs. 7.3 months [95% CI 2.9–7.9], P=0.036). Antinuclear antibody positivity predicted a significantly prolonged irPFS (10.2 months vs. 6.9 months, P=0.032). The mPFS (mPFS) was 6.9 months (95% CI 5.5–7.9), the median irPFS was 7.3 months (95% CI 5.5–8.8), and the mOS was 17 months (95% CI 7.9–24.3). Increased toxicity was detected, with grade III or higher toxicity developing in 90%; 69% of these toxicities were thought to be related to ipilimumab.
Moreover, in a double-blind phase III study of ipilimumab plus etoposide and a platinum agent, OS was not increased compared with chemotherapy alone (mOS of 11.0 vs. 10.9 months, HR 0.94, 95% CI 0.81–1.09, P=0.3775).32 There was also no significant improvement in the mPFS (4.6 vs.4.4 months; HR 0.85, 95% CI 0.75–0.97). Rates of treatment-related adverse events were 48% for grade III to IV events in the ipilimumab arm and 44% in the placebo arm (Table 1).
PD-1 and PD-L1 pathways and PD-1 and PD-L1 checkpoint inhibitors
The PD-1 receptor is another important checkpoint receptor being studied in oncology.34 In contrast to CTLA-4, PD-1 is expressed on a broader range of immune cells besides T lymphocytes (e.g., B lymphocytes and natural killer [NK] cells).34–36 Antibodies designed to inhibit the interaction between PD-1 and its ligands (PD-L1 and PD-L2) have shown promising results in clinical trials of different tumor types, including SCLC. A monoclonal anti-PD-1 antibody (nivolumab) was designated a breakthrough therapy for the treatment of patients with metastatic SCLC on August 17th, 2018.10 The approval was based on the durability of responses in the phase I/II CheckMate-032 trial, in which the objective response rate was 12% (95% CI 6.5–19.5) for nivolumab after platinum-based chemotherapy and one other prior line of therapy in 109 patients, according to the new label. This response rate comprised 11% partial responses and 0.9% complete responses. The median duration of response was 17.9 months (95% CI 7.9–42.1), with 62% of patients continuing to respond at 12 months and 39% still responding at 18 months.37
In the CheckMate-032 study,38 the mOS was 4.4 months (95% CI 3.0–9.3) in the nivolumab monotherapy arm but 6.0 months (95% CI 3.6–11.0) in the nivolumab 3 mg/kg plus ipilimumab 1 mg/kg (N3/I1) arm and 7.7 months (95% CI 3.6–18.0) in the nivolumab 1 mg/kg plus ipilimumab 3 mg/kg (N1/I3) arm. The mPFS was 1.4 months in the nivolumab monotherapy arm (95% CI 1.4–1.9) and 1.4 months (95% CI 1.3–2.2) and 2.6 months (95% CI 1.4–4.1) in the N3/I1 and N1/I3 arms, respectively. The 1-year PFS was 11% (95% CI 5.0–19.0) in the nivolumab monotherapy arm. An updated result of the CheckMate-032 study was recently published.39 Nivolumab monotherapy against SCLC had a strong therapeutic effect and was well tolerated as a third- or later-line treatment for recurrent SCLC. The objective response rate was determined to be 11.9% in the patients with recurrent LS- or ES-SCLC, the mPFS was 1.4 months (95% CI 1.3–1.6), and the mOS was 5.6 months (95% CI 3.1–6.8). Moreover, the 1-year OS was 28.3% (95% CI 20.0–37.2). However, the open-label Checkmate-331 study failed to meet the primary endpoint of OS compared with standard of care.10
A randomized, open-label, phase I/II study comparing nivolumab with 177lu-DOTA0-Tyr3-Octreate radiation therapy, sequentially, in patients with ED-SCLC is currently active and not recruiting patients (NCT03325816).44 The primary endpoints are PFS and the maximum tolerated dose of 177lu-DOTA0-Tyr3-Octreate. Nivolumab 240 mg is being administered every 2 weeks until disease progression, with 177lu-DOTA0-Tyr3-Octreate administered 2 weeks after the first administration of nivolumab. Each dose is infused over 30 minutes. A randomized, open-label, phase II study comparing nivolumab treatment with no treatment after chemotherapy in ED-SCLC is also currently active with the primary endpoint of PFS (NCT03382561).44 In addition, nivolumab clinical trials are ongoing and recruiting patients, including an open-label, phase II study of patients with advanced SCLC treated with gemcitabine (NCT03662074) (Table 2).44
Pembrolizumab
Pembrolizumab (KEYTRUDA®), a fully humanized IgG4 isotype antibody against PD-1, is recognized as an effective immunotherapy for several solid tumors. The FDA initially approved it to treat metastatic melanoma and further approved it in 2017 for any unresectable or metastatic solid tumor with certain genomic anomalies.40 A multicenter phase II trial41 of maintenance pembrolizumab in 45 patients with SCLC showed no improvement in the mPFS (1.4 months, 95% CI 1.3–2.8) when patients received pembrolizumab after completion of 4 to 6 cycles of platinum/etoposide, with a 1-year PFS of 13%. The mOS was 9.6 months (95% CI 7.0–12.0) and the 1-year survival was 37%. Further analysis indicated that the mPFS was 6.5 months (95% CI 1.1–12.8) in the PD-L1–positive group and 1.3 months (95% CI 0.6–2.5) in the PD-L1–negative group, suggesting that this agent only benefits a small subset of PD-L1–expressing patients. The phase 1b basket study KEYNOTE-028 and the phase II basket study KEYNOTE-158 evaluated the antitumor activity of pembrolizumab in patients with advanced SCLC who had received at least two lines of prior therapy,42 with pembrolizumab demonstrating promising antitumor activity. In this exploratory pooled analysis, the mOS was 7.7 months and the 1- and 2-year survival rates were 34.3% and 20.7%, respectively. The mPFS was 2 months, and the 1- and 2-year survival rates were 16.9% and 13.1%, respectively. Moreover, several ongoing clinical trials are evaluating the efficacy and safety of pembrolizumab in SCLC, including a phase III study of patients with ED-SCLC treated with etoposide/platinum (cisplatin or carboplatin) in combination with pembrolizumab (Keynote-604: NCT03066778), as well as in combination with chemotherapy or chemoradiotherapy (Table 2). In addition, the REACTION trial,44 with a primary endpoint of PFS, is evaluating platinum/etoposide in treatment naïve patients with or without pembrolizumab.
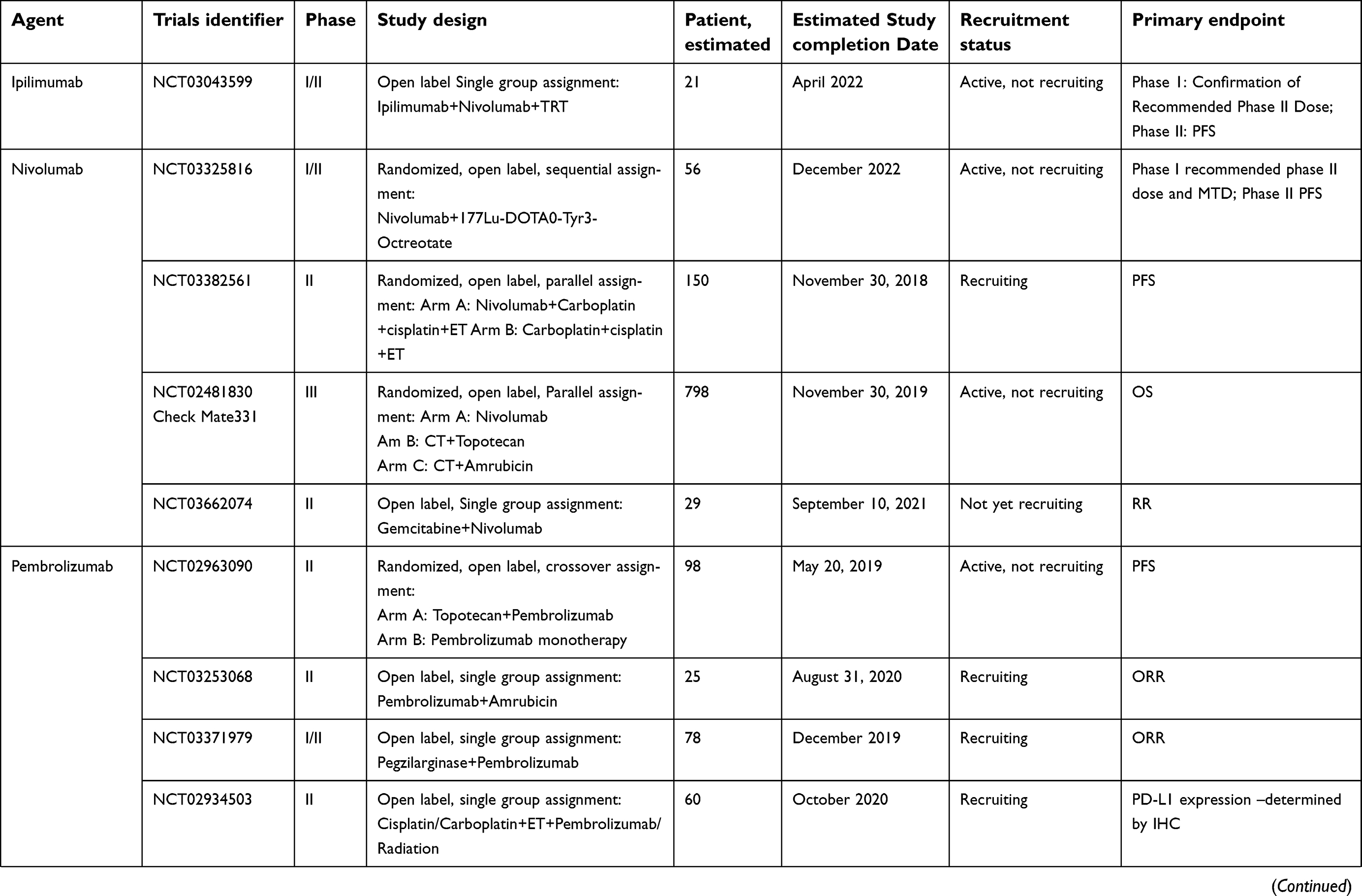 | 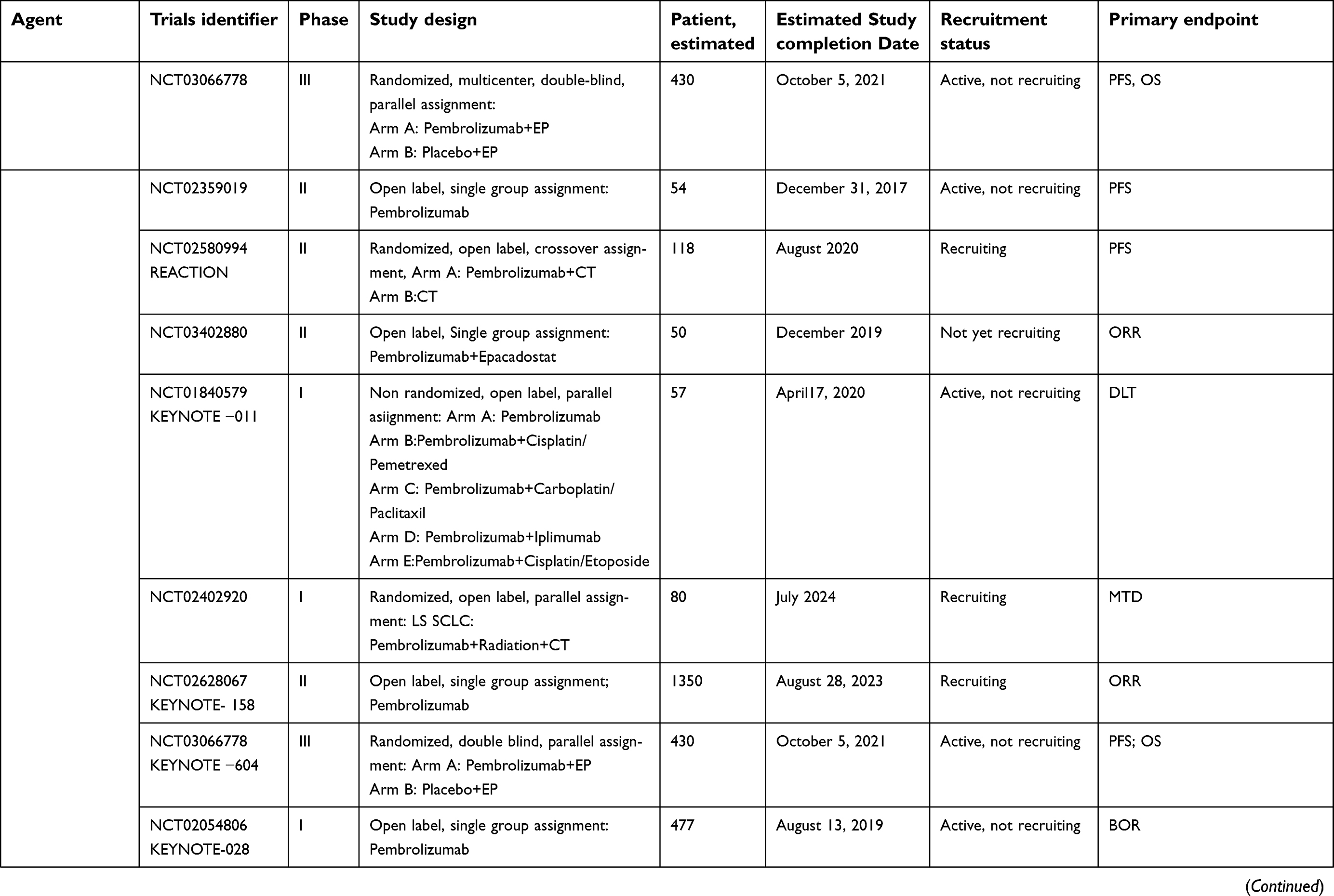 | 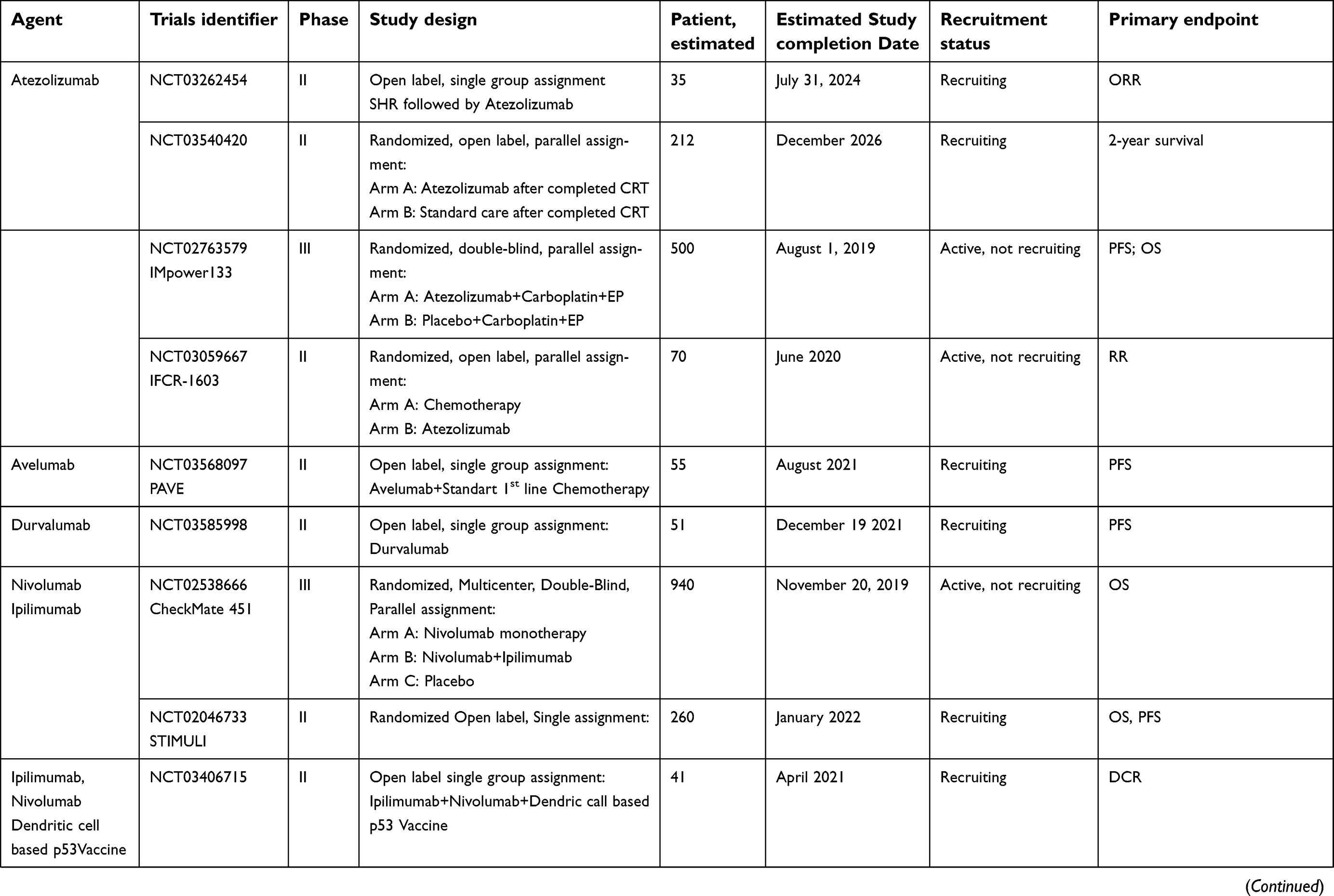 | 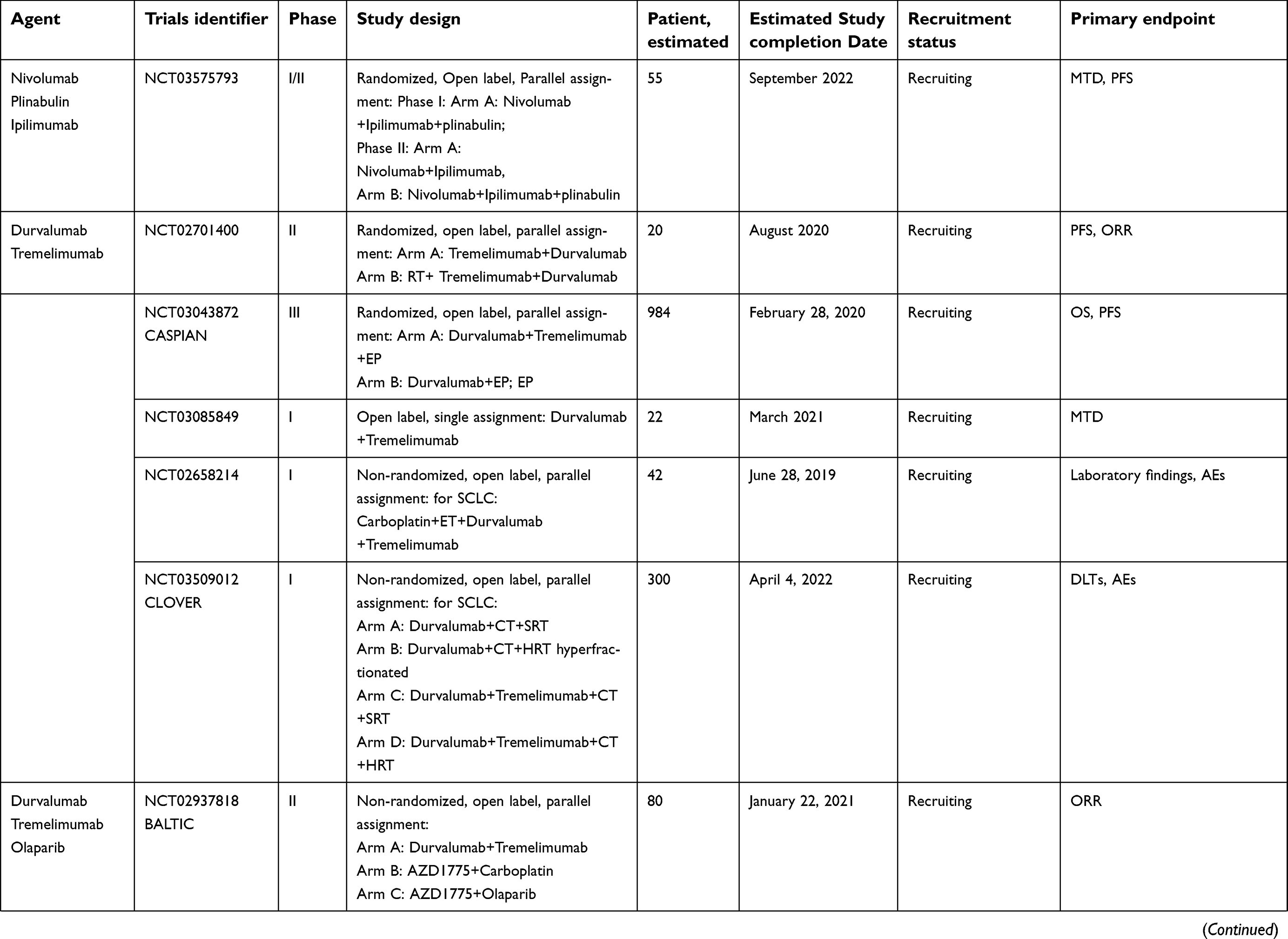 | Table 2 Ongoing trials of immune checkpoint agents in SCLC |
Atezolizumab
Atezolizumab (MPDL3280A), a fully humanized engineered IgG1 monoclonal antibody against PD-L1, is an effective immunotherapy for several solid cancers. Recently, the FDA granted approval to the combination of atezolizumab (TECENTRIQ®) with carboplatin and etoposide for the frontline treatment of patients with ES-SCLC. The approval is based on findings from the phase III IMpower133 study,11 which demonstrated that the addition of atezolizumab to carboplatin and etoposide significantly improved OS in patients with ES-SCLC. The mOS was 12.3 months in the atezolizumab group and 10.3 months in the placebo group (HR 0.70, 95% CI 0.54–0.91, P=0.007. The mPFS was 5.2 months and 4.3 months, respectively (HR 0.77, 95%CI 0.62–0.96, p=0.02).12 However, a randomized phase II trial (IFCT-1603)43 investigating the therapeutic efficacy of single atezolizumab for relapsed SCLC revealed that atezolizumab did not have a significantly better therapeutic efficacy and safety profile. PFS was determined to be 1.4 months in the atezolizumab group (95% CI 1.2–1.5) but 4.2 months in the chemotherapy group (95% CI 1.5–5.9). In this field of study, several clinical trials are still being performed to evaluate the efficacy and safety of atezolizumab for SCLC. In addition, other PD-L1 immune checkpoint inhibitors—durvalumab and avelumab—are also being investigated in clinical trials.44
Combination therapy
A number of ongoing trials are focused on combination therapies, such as a phase I/II trial investigating ROVA-T (an anti-DLL3 antibody drug conjugate) with nivolumab and ipilimumab (NCT03026166) and a phase I/II trial investigating olaparib (PARP inhibitor) with durvalumab (anti-PD-L1 antibody) and the anti-VEGF antibody bevacizumab (NCT02734004). A randomized, open-label, phase II study (STIMULI) comparing ipilimumab following chemoradiotherapy alone in LS-SCLC is currently recruiting patients (NCT02046733)44 with primary endpoints of OS and PFS. In the induction phase, nivolumab is to be administered at a dose of 1 mg/kg i.v., followed by ipilimumab 3 mg/kg i.v. once every 3 weeks for four cycles. Nivolumab will be continued as maintenance therapy at a dose of 240 mg i.v. once every 2 weeks for a maximum of 12 months; the results are expected in 2022. Phase III data from the CheckMate-451 trial showed that OPDIVO® (nivolumab) combined with YERVOY® (ipilimumab) missed the primary endpoint of OS.45 Preliminary results from the BALTIC study,46 which evaluated the combination of durvalumab and tremelimumab in 25 patients with platinum-refractory/platinum-resistant ES-SCLC, showed an objective response rate of 9.5%, mPFS of 1.9 months, and mOS of 6.0 months, suggesting improved activity over single-agent anti-PD-L1 therapy (Table 2).
A phase I/II study44 comparing nivolumab+ipilimumab±plinabulin in recurrent SCLC is currently recruiting patients (NCT03575793). Primary endpoints include the maximum tolerated dose and PFS. In the phase I trial, nivolumab is to be intravenously administered at a dose of 1 mg/kg i.v., followed by ipilimumab 3 mg/kg i.v. and plinabulin in dose-escalating cohorts (level 1, 13.5 mg/m2; level 1 (start), 20 mg/m2; level 2, 30 mg/m2). After four treatment cycles, ipilimumab will be stopped and patients will be administered nivolumab 240 mg and plinabulin every 2 weeks; the results are due in 2022. A number of ongoing trials are focusing on durvalumab and tremelimumab combination therapies, such as the CASPIAN and CLOVER trials. A phase III study (CASPIAN) comparing durvalumab with or without tremelimumab after chemotherapy alone in ES-SCLC patients is currently active and not recruiting patients (NCT0304872).44 Its results are expected in 2020. The primary endpoints of the clinical trial include OS. The trial is designed as follows. In Arm A, durvalumab and tremelimumab are administered every 3 weeks for 12 weeks and carboplatin/cisplatin and etoposide are administered up to four cycles every 3 weeks. In Arm B, durvalumab is administered every 3 weeks for 12 weeks and carboplatin/cisplatin and etoposide are administered up to four cycles every 3 weeks. In Arm C, carboplatin/cisplatin and etoposide are administered up to six cycles every 3 weeks (Table 2).
Next generation of immune checkpoint targets
Immune checkpoint molecules are important regulators for maintaining immune homeostasis and preventing autoimmunity. These pathways consist of both stimulatory and inhibitory pathways, which are important for maintaining self-tolerance and regulating the type, magnitude, and duration of the immune response,34,47 as shown in Figure 1.
LAG3
Lymphocyte activation gene-3 (LAG3, CD223) is expressed by T cells and NK cells after MHC class II ligation.48,49 LAG3 and PD-1 are frequently co-expressed and upregulated on tumor-infiltrating lymphocytes, leading to immune exhaustion and tumor growth.50 LAG-3 blockade improves tumor immune responses and potentiates a variety of forms of immunotherapy to initiate different mechanisms of action that are mediated by impeding cell cycle progression.51,52 A combinational therapy of PD-1 with anti-LAG3 is an effective tool to treat many cancer types and produces a synergistic effect. However, the combined effects of other immune checkpoint inhibitory molecules and anti-LAG3 antibody are currently under investigation.52,53 LAG525 is an immunoglobulin G4 humanized monoclonal antibody that binds LAG-3 with low nanomolar affinity, inhibiting the LAG-3 interaction with MHC class II and potentially restoring the activity of antitumor effector cells and enhancing anti-PD-1 antitumor activity.52,54 Anti-LAG-3 monoclonal antibody LAG525 is being studied in a phase II clinical trial of patients with advanced solid and hematologic malignancies including SCLC (NCT03365791)44 recruitment is currently underway. The primary endpoint is the clinical benefit rate at 24 weeks of PDR001+LAG525 and the PFS. PDR001and LAG525 will be administered via i.v. infusion over 30 minutes once every 3 weeks. The results should be available in 2021 (Table 3).
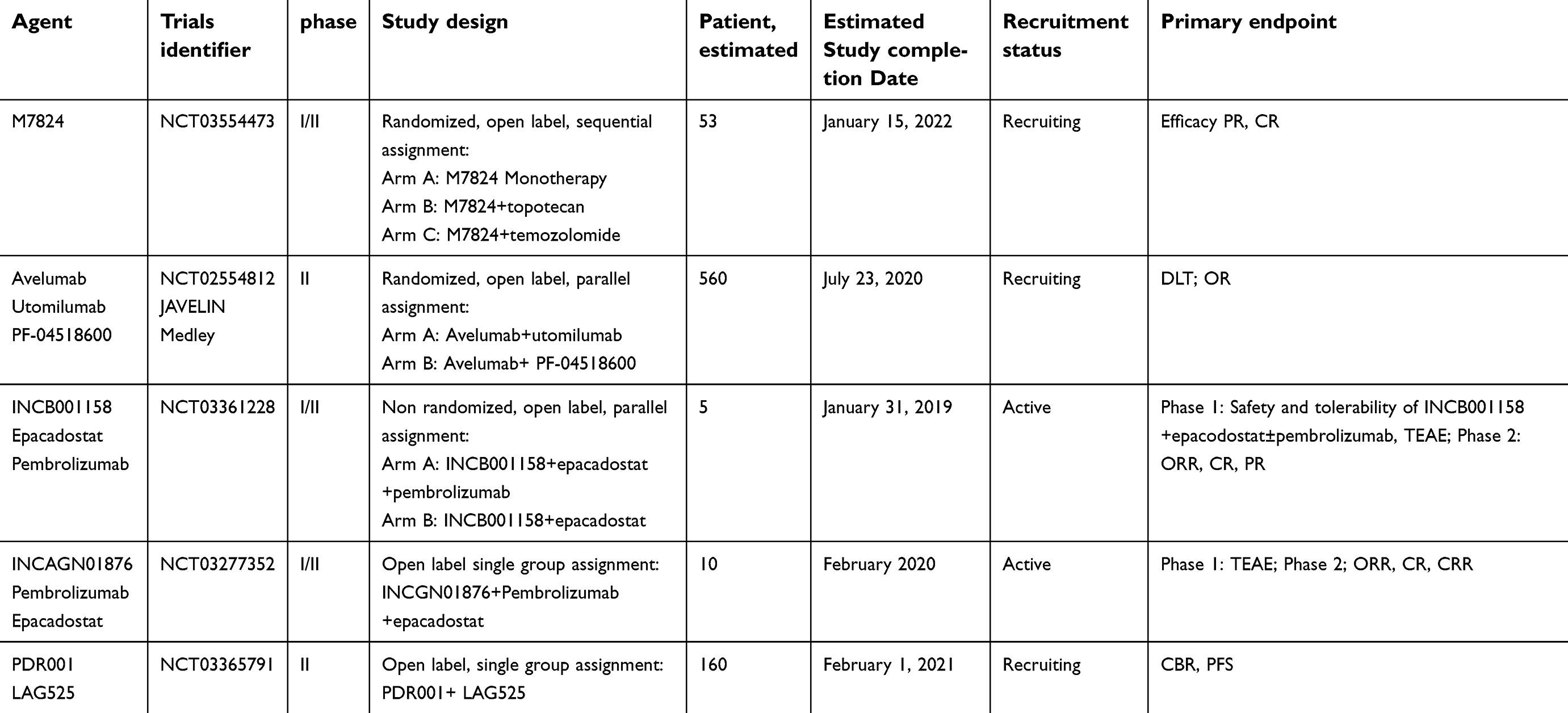 | Table 3 Ongoing trials: next generation of immune checkpoint agents in SCLC |
OX40
OX40 (CD134) is a member of the TNF receptor superfamily that is highly expressed by activated CD4, CD8 T cells, and Tregs and less expressed by neutrophils and NK cells. OX40 is a secondary co-stimulatory immune checkpoint molecule that is expressed for 24 to 72 hours following its activation. Its ligand, OX40L, is also not expressed on resting APCs. OX40 and OX40L play a pivotal role in the activation, potentiation, proliferation, and survival of T cells and in modulating NK cell function.55,56 PF-04518600 (PF-8600) is an IgG2 humanized agonistic monoclonal antibody of OX40 that is being evaluated in the international JAVELIN Medley clinical trial (NCT02554812).44 The primary endpoint is the number of participants with dose-limiting toxicities in the first 8 weeks of treatment and those with an objective response. Currently, no data are unavailable on SCLC (Table 3).
4-1BB
4-1BB, an activation-induced co-stimulatory receptor, is an important regulator of immune responses that is expressed by T cells, NK cells, and APCs. Once expressed, it binds to its ligand (4-1BBL) and triggers the proliferation and activation of immune cells, particularly T and NK cells.57,58 Utomilumab (PF-05082566), a fully human monoclonal antibody that stimulates 4-1BB, is currently being studied in patients with SCLC and in combination with avelumab and PF-04518600 in a phase II clinical trial (JAVELIN Medley).44 The primary endpoint is the number of participants with dose-limiting toxicities in the first 8 weeks of treatment and those with an objective response. Utomilumab is administered to those who have progressed after at least one line of platinum-containing therapy, and one of three dose levels is to be used to optimize the combination with avelumab until disease progression. No preliminary results are available yet (Table 3).
Non-t cell-associated inhibitory molecules
TGF-β
Transforming growth factor (TGF)-β is a cytokine that controls multiple cellular processes such as growth suppression of epithelial cells, alveolar epithelial cell differentiation, fibroblast activation, and extracellular matrix organization.59 The TGF-β pathway promotes cancer progression by concomitantly boosting tumor metastasis while inhibiting the host immune response. Although this pathway is able to control early-stage tumors by promoting cell cycle arrest and apoptosis, in advanced stages, it allows for tumor evasion by suppressing cytotoxic T cells and promotes cancer cell proliferation, invasion, and metastasis, a functional switch known as the TGF-β paradox.60,61 M7824 is a monoclonal antibody against PD-L1 linked to the extracellular domain of human TGF-β receptor 2 protein. Upon administration, the PD-L1 monoclonal antibody part of M7824 binds to PD-L1 while the TGF-β part binds to and neutralizes TGF-β receptor 2 protein, which prevents TGF-β– and PD-L1–mediated signaling and promotes CD8+ T cell and NK cell activation, ultimately inhibiting tumor growth.61,62 M7824 is being evaluated in a phase I/II clinical trial (NCT03554473) in patients with relapsed SCLC.43 The primary endpoints include efficacy (after 6 weeks for Arm B and 8 weeks for Arm C), PFS, duration of response, and OS. M7824 is administered at 1800 mg i.v. over 1 hour every 3 weeks on a 3-week cycle (Arm A/B) and at 1200 mg i.v. over 1 hour every 2 weeks on a 4-week cycle (Arm C). Topotecan is administered at 1 mg/m2 i.v. over 30 minutes on days 1–5 on a 3-week cycle. Temozolomide is orally administered at 200 mg/m2 on days 1–5 on a 4-week cycle. The results are expected in 2022 (Table 3).
IDO
Indoleamine 2.3-dioxygenase (IDO) is an intracellular enzyme that converts tryptophan to kynurenines. Kynurenines promote the differentiation and activity of Treg cells and decrease the amount and activity of CD8 T cells, which prompts an immunosuppressive situation that is compounded by the elevated amounts of PD-1/PD-L1 present in this milieu.63,64 Epacadostat is an oral agent that blocks the IDO pathway and is being investigated in a phase I/II clinical trial of advanced and metastatic malignancies including SCLC (NCT03277352).44 The primary endpoints include treatment-emergent adverse events, objective response rate, and the complete response rate. Treatment-emergent adverse events are screened through 60 days after the end of treatment up to 18 months for phase I. The objective response rate and complete response rate are to be assessed every 9 weeks for 12 months, then every 12 weeks up to 18 months for the phase II trial. Moreover, a non-randomized, open-label, phase I/II clinical trial of advanced solid tumors including SCLC (NCT03361228)44 is currently active and not recruiting patients. The primary endpoints include treatment-emergent adverse events and objective response rate, assessed up to approximately 12 months. No preliminary results are available yet (Table 3).
Conclusion
Immune checkpoint inhibitors are showing promise as therapeutic agents for SCLC and are being intensively studied. Thus, numerous trials at all stages and lines of treatment of SCLC are exploring the value of these agents both alone and in combination with chemotherapy or targeted agents. Overall, the expectations for immuno-oncology are high and the outcomes of these trials will hopefully reveal a variety of treatment options for SCLC patients. The discovery of new immune inhibitory and stimulatory pathways and rational combination strategies as discussed in this article is essential and will help to improve SCLC immunotherapy.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (to Jun Chen [No. 81773207] and Hongyu Liu [No. 81372306]), the Tianjin Key Project of the Natural Science Foundation (to Jun Chen [No. 16JCZDJC34200]), the Special Support Program for High Tech Leader & Team of Tianjin (to Jun Chen [No. TJTZJH-GCCCXCYTD-2-6]), the Tianjin Natural Science Foundation (to Hongyu Liu [No. 16PTSYJC00160]), and the China Scholarship Council (to Hongyu Liu [No. 201706940009]).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539–4544. doi:10.1200/JCO.2005.04.4859
3. Rudin CM, Pietanza MC, Bauer TM, et al. Rovalpituzumab tesirine, a DLL3-targeted antibody-drug conjugate, in recurrent small-cell lung cancer: a first-in-human, first-in-class, open-label, phase 1 study. Lancet Oncol. 2017;18(1):42–51. doi:10.1016/S1470-2045(16)30565-4
4. Saito M, Saito K, Shiraishi K, et al. Identification of candidate responders for anti-PD-L1/PD-1 immunotherapy, Rova-T therapy, or EZH2 inhibitory therapy in small-cell lung cancer. Mol Clin Oncol. 2018;8(2):310–314. doi:10.3892/mco.2017.1536
5. Lung Cancer - Small Cell: Statistics [webpage on the Internet]. Alexandria, VA: American Society of Clinical Oncology (ASCO; Cancer.Net); updated 2019. Available from:
6. Amini A, Byers LA, Welsh JW, Komaki RU. Progress in the management of limited‐stage small cell lung cancer. Cancer. 2014;120(6):790–798. doi:10.1002/cncr.28505
7. Spiro SG, James LE, Rudd RM, et al. Early compared with late radiotherapy in combined modality treatment for limited disease small-cell lung cancer: a London lung cancer group multicenter randomized clinical trial and meta-analysis. J Clin Oncol. 2006;24(24):3823–3830. doi:10.1200/JCO.2005.05.3181
8. Pietanza MC, Byers LA, Minna JD, Rudin CM. Small cell lung cancer: will recent progress lead to improved outcomes? Clin Cancer Res. 2015;21(10):2244–2255. doi:10.1158/1078-0432.CCR-14-2958
9. Faivre-Finn C, Snee M, Ashcroft L, et al. Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial. Lancet Oncol. 2017;18(8):1116–1125. doi:10.1016/S1470-2045(17)30318-2
10. Bristol-Myers Squibb. Bristol-Myers Squibb announces Phase 3 CheckMate -331 study does not meet primary endpoint of overall survival with Opdivo versus chemotherapy in patients with previously treated relapsed small cell lung cancer [press release]. New York, NY: Bristol-Myers Squibb; 2018 [October 12]. Available from:
11. FDA Approves Atezolizumab Regimen for Frontline Small Cell Lung Cancer [webpage on the Internet]. Cranbury, NJ: OncLive; 2019. Available from:
12. Horn L, Mansfield AS, Szczęsna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
13. FDA Grants Pembrolizumab Priority Review for Advanced SCLC [webpage on the Internet]. Cranbury, NJ: OncLive; 2019. Available from: https://www.onclive.com/web-exclusives/fda-grants-pembrolizumab-priority-review-for-advanced-sclc. Accessed April 05, 2019.
14. Chung HC, Lopez-Martin JA, Kao SC-H, et al. Phase 2 study of pembrolizumab in advanced small-cell lung cancer (SCLC): KEYNOTE-158. J Clin Oncol. 2018;36(15):8506. doi:10.1200/JCO.2018.36.15_suppl.8506
15. Ott PA, Elez E, Hiret S, et al. Pembrolizumab in patients with extensive-stage small-cell lung cancer: results from the phase Ib KEYNOTE-028 study. J Clin Oncol. 2017;35(34):3823–3829. doi:10.1200/JCO.2017.72.5069
16. Spigel DR, Socinski MA. Rationale for chemotherapy, immunotherapy, and checkpoint blockade in SCLC: beyond traditional treatment approaches. J Thorac Oncol. 2013;8(5):587–598. doi:10.1097/JTO.0b013e318286cf88
17. Buchbinder EI, Desai A. CTLA-4 and PD-1 pathways: similarities, differences, and implications of their inhibition. Am J Clin Oncol. 2016;39(1):98–106. doi:10.1097/COC.0000000000000239
18. Pakkala S, Owonikoko TK. Immune checkpoint inhibitors in small cell lung cancer. J Thorac Dis. 2018;10(Suppl 3):S460–S467. doi:10.21037/jtd.2017.12.51
19. Gajewski TF, Schreiber H, Fu Y-X. Innate and adaptive immune cells in the tumor microenvironment. Nat Immunol. 2013;14(10):1014–1022. doi:10.1038/ni.2703
20. Chalmers ZR, Connelly CF, Fabrizio D, et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017;9(1):34. doi:10.1186/s13073-017-0424-2
21. McGranahan N, Furness AJ, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science. 2016;351(6280):1463–1469. doi:10.1126/science.aaf1490
22. Chan TA, Yarchoan M, Jaffee E, et al. Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic. Ann Oncol. 2018;30(1):44–56. doi:10.1093/annonc/mdy495
23. Hellmann MD, Ciuleanu T-E, Pluzanski A, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med. 2018;378(22):2093–2104. doi:10.1056/NEJMoa1801946
24. McLaughlin J, Han G, Schalper KA, et al. Quantitative assessment of the heterogeneity of PD-L1 expression in non–small-cell lung cancer. JAMA Oncol. 2016;2(1):46–54. doi:10.1001/jamaoncol.2015.3638
25. Rivalland G, Walkiewicz M, Wright GM, John T. Small cell lung cancer: the immune microenvironment and prognostic impact of checkpoint expression. J Clin Oncol. 2017;35(15):8569. doi:10.1200/JCO.2017.35.15_suppl.8569
26. Paglialunga L, Salih Z, Ricciuti B, Califano R. Immune checkpoint blockade in small cell lung cancer: is there a light at the end of the tunnel? ESMO Open. 2016;1(4):e000022. doi:10.1136/esmoopen-2015-000022
27. Graziani G, Tentori L, Navarra P. Monoclonal Antibodies to CTLA-4 with Focus on Ipilimumab. In: Klink M, editor. Interaction of Immune and Cancer Cells. Vienna: Springer; 2014: 233–258.
28. Tanvetyanon T, Gray JE, Antonia SJ. PD-1 checkpoint blockade alone or combined PD-1 and CTLA-4 blockade as immunotherapy for lung cancer? Expert Opin Biol Ther. 2017;17(3):305–312. doi:10.1080/14712598.2017.1280454
29. Ledford H. Melanoma drug wins US approval. Nature. 2011;471:
30. Arriola E, Wheater M, Galea I, et al. Outcome and biomarker analysis from a multicenter phase 2 study of ipilimumab in combination with carboplatin and etoposide as first-line therapy for extensive-stage SCLC. J Thorac Oncol. 2016;11(9):1511–1521. doi:10.1016/j.jtho.2016.05.028
31. Reck M, Bondarenko I, Luft A, et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line therapy in extensive-disease-small-cell lung cancer: results from a randomized, double-blind, multicenter phase 2 trial. Ann Oncol. 2012;24(1):75–83. doi:10.1093/annonc/mds213
32. Reck M, Luft A, Szczesna A, et al. Phase III randomized trial of ipilimumab plus etoposide and platinum versus placebo plus etoposide and platinum in extensive-stage small-cell lung cancer. J Clin Oncol. 2016;34(31):3740–3748. doi:10.1200/JCO.2016.67.6601
33. Reck M, Heigener D, Reinmuth N. Immunotherapy for small-cell lung cancer: emerging evidence. Future Oncol. 2016;12(7):931–943. doi:10.2217/fon-2015-0012
34. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12(4):252–264. doi:10.1038/nrc3239
35. Topalian SL, Weiner GJ, Pardoll DM. Cancer immunotherapy comes of age. J Clin Oncol. 2011;29(36):4828–4836. doi:10.1200/JCO.2011.38.0899
36. Henick BS, Herbst RS, Goldberg SB. The PD-1 pathway as a therapeutic target to overcome immune escape mechanisms in cancer. Expert Opin Ther Targets. 2014;18(12):1407–1420. doi:10.1517/14728222.2014.955794
37. US Food and Drug Administration. FDA grants nivolumab accelerated approval for third-line treatment of metastatic small cell lung cancer [webpage on the Internet]. Silver Spring, MD: US Food and Drug Administration; 2018. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-nivolumab-accelerated-approval-third-line-treatment-metastatic-small-cell-lung-cancer. Accessed September 11, 2018.
38. Antonia SJ, López-Martin JA, Bendell J, et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016;17(7):883–895. doi:10.1016/S1470-2045(16)30098-5
39. Ready N, Farago AF, de Braud F, et al. Third-line nivolumab monotherapy in recurrent SCLC: checkMate 032. J Thorac Oncol. 2019;14(2):237–244. doi:10.1016/j.jtho.2018.10.003
40. Syn NL, Teng MW, Mok TS, Soo RA. De-novo and acquired resistance to immune checkpoint targeting. J Thor Oncol. 2017;18(12):e731–e741.
41. Gadgeel SM, Ventimiglia J, Kalemkerian GP, et al. Phase II study of maintenance pembrolizumab (pembro) in extensive stage small cell lung cancer (ES-SCLC) patients (pts). J Clin Oncol. 2017;35:
42. Chung HC, Piha-Paul SA, Lopez-Martin J, et al. CT073 - Pembrolizumab after two or more lines of prior therapy in patients with advanced small-cell lung cancer (SCLC): Results from the KEYNOTE-028 and KEYNOTE-158 studies. Proceedings of the 110th Annual Meeting of the American Association for Cancer Research, Atlanta, GA, March 29 - April 3 2019. Philadelphia, PA: AACR; 2019.
43. Pujol J-L, Greillier L, Audigier-Valette C, et al. A randomized non-comparative phase 2 study of anti-programmed cell death-ligand 1 atezolizumab or chemotherapy as second-line therapy in patients with small cell lung cancer: results from the IFCT-1603 Trial. J Thorac Oncol. 2019;S1556-0864(19):30025.
44. National Cancer Institute (NCI). Cisplatin/carboplatin and etoposide with or without nivolumab in treating patients with extensive stage small cell lung cancer. Available from:
45. Bristol-Myers Squibb. Bristol-Myers Squibb announces CheckMate -451 study did not meet primary endpoint of overall survival with Opdivo plus Yervoy Vs. placebo as a maintenance therapy in patients with extensive-stage small cell lung cancer after completion of first-line... [press release]. New York, NY: Bristol-Myers Squibb; 2018 [November 26]. Available from:
46. Bondarenko I, Juan-Vidal O, Pajkos G, et al. 1665PD Preliminary efficacy of durvalumab plus tremelimumab in platinum-refractory/resistant ED-SCLC from arm A of the phase II BALTIC study. Ann Oncol. 2018;29(suppl8):
47. Chen L, Flies DB. Molecular mechanisms of T cell co-stimulation and co-inhibition. Nat Rev Immunol. 2013;13(4):227–242. doi:10.1038/nri3405
48. Workman CJ, Dugger KJ, Vignali DA. Cutting edge: molecular analysis of the negative regulatory function of lymphocyte activation gene-3. J Immunol. 2002;169(10):5392–5395. doi:10.4049/jimmunol.169.10.5392
49. Dholaria B, Hammond W, Shreders A, Lou Y. Emerging therapeutic agents for lung cancer. J Hematol Oncol. 2016;9(1):138. doi:10.1186/s13045-016-0365-z
50. Anderson AC, Joller N, Kuchroo VK. Lag-3, Tim-3, and TIGIT: co-inhibitory receptors with specialized functions in immune regulation. Immunity. 2016;44(5):989–1004. doi:10.1016/j.immuni.2016.05.001
51. He Y, Rivard CJ, Rozeboom L, et al. Lymphocyte‐activation gene‐3, an important immune checkpoint in cancer. Cancer Sci. 2016;107(9):1193–1197. doi:10.1111/cas.12986
52. Woo S-R, Turnis ME, Goldberg MV, et al. Immune inhibitory molecules LAG-3 and PD-1 synergistically regulate T-cell function to promote tumoral immune escape. Cancer Res. 2012;72(4):917–927. doi:10.1158/0008-5472.CAN-11-1620
53. Andrews LP, Marciscano AE, Drake CG, Vignali DA. LAG 3 (CD 223) as a cancer immunotherapy target. Immunol Rev. 2017;276(1):80–96. doi:10.1111/imr.12519
54. Piha-Paul SA, Amin A, Kovacs C, Magley A, Purkayastha DD, Zhuo Y. A phase 2, open-label study of the combination of spartalizumab (PDR001) and LAG525 for patients with advanced solid tumors and hematologic malignancies. Journal of Clinical Oncology. 2018;36(15):Abstract TPS2616.
55. Dempke WCM, Fenchel K, Uciechowski P, et al. Second- and third-generation drugs for immune-oncology treatment-The more the better? Eur J Cancer. 2017;74:55–72. doi:10.1016/j.ejca.2017.01.001
56. Sagiv-Barfi I, Czerwinski DK, Levy S, et al. Eradication of spontaneous malignancy by local immunotherapy. Sci Transl Med. 2018;10(426):eaan4488. doi:10.1126/scitranslmed.aao4496
57. Chester C, Ambulkar S, Kohrt HE. 4-1BB agonism: adding the accelerator to cancer immunotherapy. Cancer Immunol Immunother. 2016;65(10):1243–1248. doi:10.1007/s00262-016-1829-2
58. Vinay DS, Kwon BS. 4-1BB (CD137), an inducible costimulatory receptor, as a specific target for cancer therapy. BMB Rep. 2014;47(3):122–129.
59. Massagué J. TGFβ in cancer. Cell. 2008;134(2):215–230. doi:10.1016/j.cell.2008.07.001
60. Wendt MK, Tian M, Schiemann WP. Deconstructing the mechanisms and consequences of TGF-β-induced EMT during cancer progression. Cell Tissue Res. 2012;347(1):85–101. doi:10.1007/s00441-011-1199-1
61. Thomas DA, Massagué J. TGF-β directly targets cytotoxic T cell functions during tumor evasion of immune surveillance. Cancer Cell. 2005;8(5):369–380. doi:10.1016/j.ccr.2005.10.012
62. Knudson KM, Hicks KC, Luo X, Chen J-Q, Schlom J, Gameiro SR. M7824, a novel bifunctional anti-PD-L1/TGFβ Trap fusion protein, promotes anti-tumor efficacy as monotherapy and in combination with vaccine. Oncoimmunology. 2018;7(5):e1426519. doi:10.1080/2162402X.2018.1490854
63. Lan Y, Zhang D, Xu C, et al. Enhanced preclinical antitumor activity of M7824, a bifunctional fusion protein simultaneously targeting PD-L1 and TGF-β. Sci Transl Med. 2018;10(424):eaan5488. doi:10.1126/scitranslmed.aao4496
64. Platten M, Wick W, Van Den Eynde BJ. Tryptophan catabolism in cancer: beyond IDO and tryptophan depletion. Cancer Res. 2012;72(21):5435–5440. doi:10.1158/0008-5472.CAN-12-0569
65. Moon YW, Hajjar J, Hwu P, Naing A. Targeting the indoleamine 2, 3-dioxygenase pathway in cancer. J Immunother Cancer. 2015;3(1):51. doi:10.1186/s40425-015-0094-9
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.