")
Back to Journals » Nature and Science of Sleep » Volume 14
Idiopathic Hypersomnia: Historical Account, Critical Review of Current Tests and Criteria, Diagnostic Evaluation in the Absence of Biological Markers and Robust Electrophysiological Diagnostic Criteria
Authors Billiard M, Sonka K
Received 7 November 2021
Accepted for publication 27 January 2022
Published 26 February 2022 Volume 2022:14 Pages 311—322
DOI https://doi.org/10.2147/NSS.S266090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ahmed BaHammam
Michel Billiard,1 Karel Sonka2
1Department of Neurology, Gui de Chauliac Hospital, Montpellier, France; 2Department of Neurology and Center of Clinical Neuroscience, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czech Republic
Correspondence: Michel Billiard, Department of Neurology, Gui de Chauliac Hospital, 80, Avenue Augustin Fliche, Montpellier Cedex 5, 34295, France, Tel +33 6 75 028 364, Email [email protected]
Abstract: Idiopathic hypersomnia was first described in 1976 under two forms: polysymptomatic, characterized by excessive daytime sleepiness, long and unrefreshing naps, nocturnal sleep of abnormally long duration and signs of sleep drunkenness upon awakening; monosymptomatic, manifested by excessive daytime sleepiness only. Yet, after 45 years, this sleep disorder is still poorly delineated and diagnostic criteria produced by successive International Classifications of Sleep Disorders are far from satisfactory. The first part of this review is a historical account of the successive names and descriptions of idiopathic hypersomnia: monosymptomatic and polysymptomatic idiopathic hypersomnia in 1976; central nervous system idiopathic hypersomnia in 1979; idiopathic hypersomnia in 1990; idiopathic hypersomnia with and without long sleep time in 2005; idiopathic hypersomnia again in 2014; and, within the last few years, the proposal of separating idiopathic hypersomnia into a well-defined subtype, idiopathic hypersomnia with long sleep duration, and a more heterogeneous subtype combining idiopathic hypersomnia without long sleep duration and narcolepsy type 2. The second part is a critical review of both current ICSD-3 diagnostic criteria and clinical features, scales and questionnaires, electrophysiological and circadian control tests, research techniques, currently used to diagnose idiopathic hypersomnia. The third part proposes a diagnostic evaluation of idiopathic hypersomnia, in the absence of biologic markers and of robust electrophysiological diagnostic criteria.
Keywords: central disorders of hypersomnolence, idiopathic hypersomnia, idiopathic hypersomnia with long sleep time, idiopathic hypersomnia without long sleep time, idiopathic hypersomnia with long sleep duration, idiopathic hypersomnia without long sleep duration, narcolepsy, narcolepsy type 1 and narcolepsy type 2
Introduction
Idiopathic hypersomnia (IH) is a chronic neurological disorder clinically characterized by excessive daytime sleepiness frequently accompanied by altered wakefulness, long unrefreshing naps, abnormally prolonged nocturnal sleep, sleep drunkenness (a severe manifestation of sleep inertia), autonomic and cognitive symptoms. The condition is a heterogenous entity. Clinical and electrophysiological diagnostic criteria presented in the successive diagnostic classifications of sleep disorders have varied from one classification to the next one and still deserve improvement. IH most often begins during adolescence or young adulthood. Prevalence of IH is unsettled due to the absence of biomarkers and of a clear consensus on the frontiers of the condition. However, cohorts of patients published by different sleep disorders centers suggest a prevalence lower than the one of narcolepsy. In contrast, the prevalence of “excessive quantity of sleep” defined as a night sleep period or a 24h sleep duration higher than or equal to 9 hours, accompanied by complaints of impaired functioning or distress due to excessive sleep, was observed in 1.6% of a large sample of 15.929 non-selected individuals.1 Thus, even if presumably not all of these subjects met diagnostic criteria for IH, it is clear that some symptoms of IH are not uncommon in the general population. According to several cohorts, there is a higher prevalence of IH in women.2 Approximately one-third of the patients have a positive family history of IH in favor of a genetic contribution to IH.3,4 However, no association with HLA has been evidenced. In this article, we will first give a historical account of the successive descriptions of the disorder, then review the current diagnostic criteria and approaches with their strengths and weaknesses, and finally propose a diagnostic evaluation of the condition in the absence of biological markers and of robust electrophysiological criteria.
Historical Account
The knowledge of diseases with excessive daytime sleepiness has a relatively short history. Fifty years ago, the attention was focused mainly on narcolepsy, while other conditions were neglected. Thus, it goes without saying that the classification of hypersomnias including narcolepsy, hypersomnia and the subwakefulness syndrome proposed by the Czechoslovak neurologist Bedrich Roth, in 1976, was of major interest.5 Hypersomnia was recognized as either symptomatic, due to organic affections of the brain, general metabolic affections as well as intoxications, or functional, including IH, neurotic hypersomnia and hypersomnia with disorders of respiration during sleep. IH was in turn subdivided into two forms, a polysymptomatic form characterized by prolonged night sleep of a duration of 12 to 18 hours or even more, diurnal sleep attacks if the patients are left undisturbed, sleep drunkenness occurring at every awakening, and a monosymptomatic form manifested by ”states of excessive diurnal sleep of a duration of one to several hours, not so irresistible as in narcolepsy”. This classification had been heralded by important contributions, description of sleep drunkenness, a major difficulty in awakening, as soon as 19566 and successive clinical and polysomnographic entities suggestive of either IH without affiliation status7–9 or IH polysymptomatic form.10,11 Three years after the initial description of IH with its two forms, the “Diagnostic Classification of Sleep and Arousal Disorders”12 used the term “idiopathic CNS hypersomnia”, merging the two forms of idiopathic hypersomnia and mentioning that symptoms such as total nocturnal sleep time of long duration or great difficulty in awakening affected many of the patients. Importantly, polysomnographic monitoring failed to uncover either sleep onset REM periods (SOREMPs) or excessive apneas. In 1990, the International Classification of Sleep Disorders13 came back to the term IH and recognized alike a single form of the disorder, with a variable frequency of the different symptoms. Polysomnographically, one or more of the following had to be present: 1) A sleep period that is normal or prolonged in duration; 2) Sleep latency less than 10 minutes; 3) Normal REM sleep latency; 4) Multiple sleep latency test (MSLT) that demonstrates a sleep latency less than 10 minutes; 5) Less than two SOREMPs on the MSLT. In 1997, Bassetti and Aldrich,14 on a purely clinical basis, identified three forms of IH, classic, referring to patients who tend to have sleepiness that is not overwhelming, who take long non-refreshing naps up to a several hour duration, who have prolonged night-time sleep and have difficulty in awakening in the morning; narcoleptic-like, referring to patients with overwhelming hypersomnolence, who take short refreshing naps and awake without difficulties; and mixed, referring to patients with clinical features intermediate between the two other groups. One year later, also on a clinical basis, Billiard et al15 suggested returning to Roth’s initial distinction, replacing the terms polysymptomatic and monosymptomatic by the terms complete and incomplete and adding ICSD electrophysiological features. In 2002, a revision of the ICSD was initiated by the board of directors of the American Academy of Sleep Medicine and a Task Force on hypersomnias of central origin, not due to a circadian rhythm sleep disorder, sleep related breathing disorder, or other causes of disturbed nocturnal sleep, was appointed. A large majority of members of the Task Force agreed to separate IH into two subgroups, one characterized by excessive daytime sleepiness, prolonged nocturnal sleep and difficulty in awakening and one remarkable for excessive daytime sleepiness only. Eventually, the two conditions were referred to as idiopathic hypersomnia with long sleep time (IHwLST) and idiopathic hypersomnia without long sleep time (IHwoLST) in the second edition of the International Classification of Sleep Disorders (ICSD-2).16 Polysomnographically, IHwLST should demonstrate a major sleep period longer than 10 hours and, if an MSLT is performed following overnight polysomnography, a mean sleep latency of less than 8 minutes and fewer than two SOREMPs. In the case of IHwoLST, polysomnography should document a major sleep period that is normal (longer than 6 hours but less than 10 hours) and an MSLT demonstrating a mean sleep latency of less than 8 minutes and fewer than two SOREMPS. However, ICSD-2 included shortcomings such as the cut-off of 8 minutes for the mean sleep latency, just a matter of expert opinion.17 Moreover, the distinction between IHwLST and IHwoLST was challenged by the absence of clinical symptoms specific to one subgroup,18,19 and a mean sleep latency on the MSLT of shorter than 8 min in 40 patients with IH and of 8 min or longer in 32 patients with IH, without any difference in the other clinical and polysomnographic parameters in the first study,18 and the normality (> 8 min) of the mean sleep latency in 71% of patients with IHwLST in the second study.19 Thus, the latter released International Classification of Sleep Disorders - 3rd edition (ICSD-3) abandoned the distinction between IHwLST and IHwoLST on clinical and MSLT grounds.20 However, ICSD-3 somewhat neglected the clinical diagnostic criteria of the condition and settled two detailed electrophysiological diagnostic criteria qualified by three electrophysiological notes, the last of which calling for clinical judgment in deciding whether patients with a MSLT mean sleep latency longer than 8 min and total 24-hour sleep time shorter than 660 min should be considered to have IH. Overall, ICSD-3 did not look fully satisfactory, neither from a clinical point of view, clinical diagnostic criteria being reduced to a minimum, nor from an electrophysiological point of view, given the numerous and unsure electrophysiological diagnostic criteria. Last, but not least, IH diagnostic criteria according to ICSD-3 were close to narcolepsy type 2 (NT2) diagnostic criteria and the frontier between the two disorders was fuzzy. Hence, sustained efforts in the last few years to identify better narcolepsy type 1 (NT1), NT2 and IH. The first one was a data-driven cluster analysis based on clinical, polysomnographic and MSLT variables in a population of 96 patients diagnosed with narcolepsy with cataplexy (NwC) (n=23), narcolepsy without cataplexy (NwoC) (n=22), IHwLST (n=26) and IHwoLST (n=25) according to ICSD-2 criteria.21 This study led to the identification of three main clusters of central hypersomnia, namely cluster 1: combined IHwoLST/ NT2 (n=44); cluster 2: IHwLST (n=27) and cluster 3: NT1 (n=23). Following this cluster analysis, at the 7th International Symposium on Narcolepsy held in Massachusetts in the late 2018, a group of specialists gathered to reassess the 2014 ICSD classification of narcolepsy and IH. They proposed, based on available data, that idiopathic hypersomnia with long sleep duration (IHwLSD) should be an identifiable and meaningful sleep disorder, while NT2 and idiopathic hypersomnia without long sleep duration (IHwoLSD) should be merged into a single disorder.22 Besides, a group of European experts published an important “position paper” aimed at discussing shortcomings in the approach and structure of ICSD-3 in general, with subsequent focus on the chapter on “Central disorders of hypersomnolence” in order to improve a future version of ICSD-3.23 Eventually, based on data from the Hypersomnia Foundation Registry, including 563 registry respondents with IH (n=468), NT2 (n=44) and NT1 (n=51), symptoms were compared between IHwLSD and IHwoLSD participants and it was found that “brain fog” and sleep drunkenness were more frequent in those with long sleep duration.24 More recently, with the help of a structured interview completed with information about disease history and a set of questionnaires and scales, a cohort of 43 patients with IH was divided into 25 patients with IHwoLSD and 18 patients with IHwLSD.25 In so doing, the authors could confirm that patients with IHwLSD differed clinically as well as by objective measures from patients with IHwoLSD, at the time of diagnosis and on long-term follow-up. Altogether, the historical account of IH shows a constant oscillation between a presentation of IH under two forms, polysymptomatic with a long night sleep duration and monosymptomatic without a long night sleep duration, or under one form with daytime and nighttime symptoms of variable frequency. It also shows an evolution from purely clinical diagnostic criteria to progressively less clinical diagnostic criteria and more electrophysiological diagnostic criteria in the successive classifications of sleep disorders and, eventually, during these last years, the emergence of a well defined IHwLSD well separated from an IHwoLSD very close or similar to NT2 (Table 1).
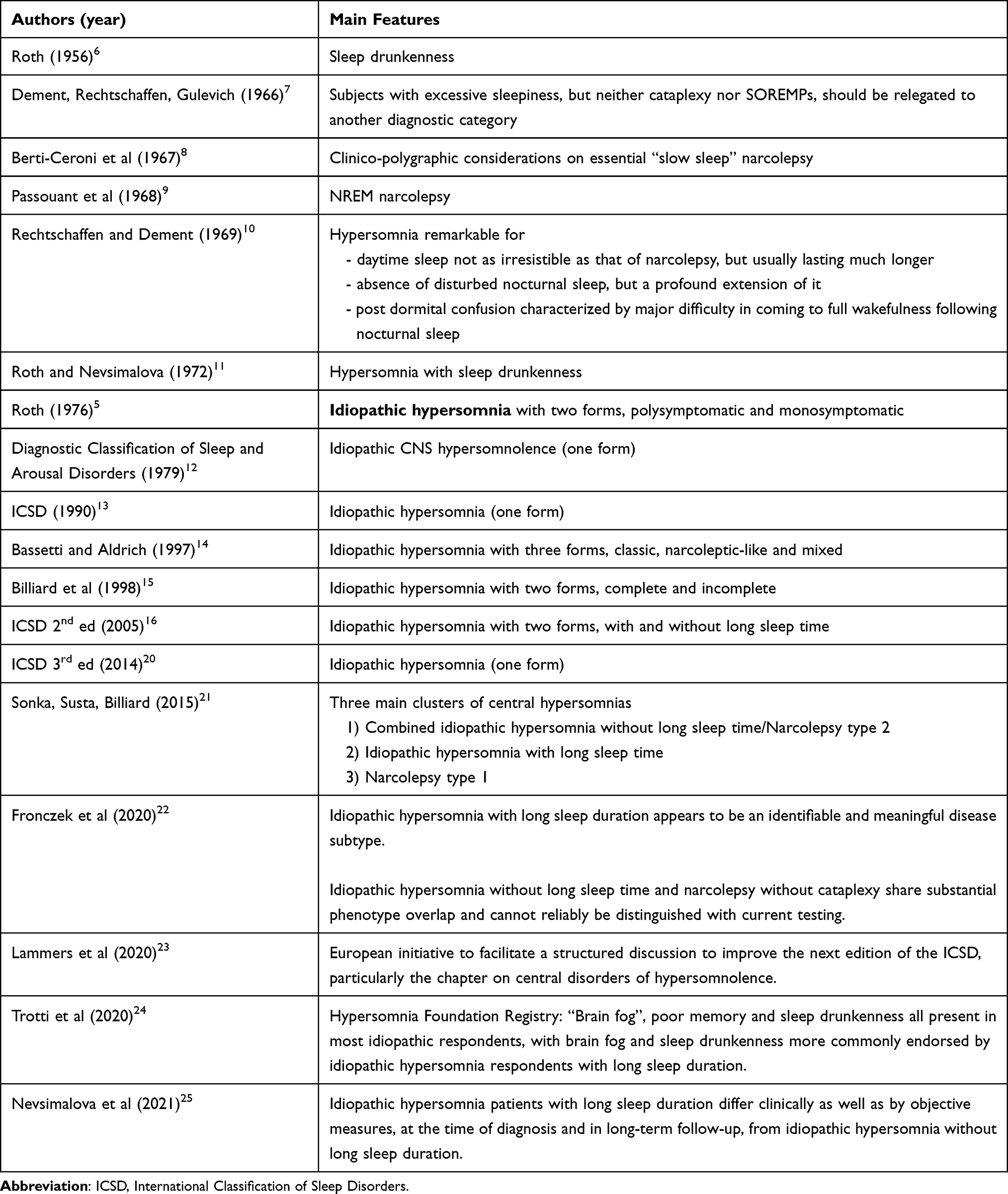 |
Table 1 Idiopathic Hypersomnia: Historical Account |
Critical Review of ICSD-3 Clinical and Electrophysiological Diagnostic Criteria and of Symptoms, Questionnaires and Scales, Electrophysiological and Circadian Control Tests, Research Techniques, Currently Used in Patients Suspected of IH
Symptoms
ICSD-3 clinical diagnostic criteria are clearly insufficient. Diagnostic criterion A for IH patients: “The patient has daily periods of irresistible need to sleep or daytime lapses into sleep occurring for at least 3 months” is the same as for NT1 and NT2 patients, whereas the experience of hypersomnolence may differ qualitatively in IH patients, many of them complaining of a rather continuous, non-imperative hypersomnolence. Second, severe sleep inertia and long unrefreshing naps appear only as notes.20
Questionnaires and Scales
Some questionnaires and scales are of interest whatever the subtype of IH: the Epworth sleepiness scale, a subjective assessment of excessive daytime sleepiness26; the Beck depression inventory questionnaire to exclude depression;27 the idiopathic hypersomnia severity scale, a recently designed scale that has proved to be correlated with daytime sleepiness, depression symptoms and quality of life in patients with IH;28 the composite autonomic symptom score 31 (Compass-31),29 a widely used questionnaire that provides a quantitative assessment of the severity and distribution of autonomic symptoms, which has shown a great symptom burden in the orthostatic and vasomotor domains in IH;30 the section on non-sleep problems containing an auto-questionnaire designed by Vernet et al,31 showing attention deficit, difficulties focusing on their task in a loud environment and memory problems more frequent in patients with IH than in controls; psychomotor vigilance test,32 a reliable and objective measure of sleep inertia showing that sleep inertia is more frequent in patients with IH, 56.5%, than in patients with non IH (patients with narcolepsy, non specified hypersomnolence, obstructive sleep apnea and insomnia), 43.6%.33 Other questionnaires are of more value in as much as they may orient towards IHwLSD: the fatigue severity scale,34 which has shown a higher score in patients with IHwLSD in comparison with patients with IHwoLSD;25 The Horne and Östberg morningness-eveningness questionnaire, the most widely used questionnaire to measure chronotype,35 which has shown a lower score (p=0.001) in patients with IHwLSD in comparison with patients with IHwoLSD;25 and the sleep inertia questionnaire36 showing a higher score in patients with IHwLSD (p=0.007) in comparison with patients with IHwoLSD.25
Electrophysiological Tests
Multiple Sleep Latency Test (MSLT)
The ICSD-3 electrophysiological criteria of IH still rely heavily on the mean sleep latency and the number of SOREMPs on the MSLT, and on the total 24-hour sleep time measured by a 24-hour polysomnographic monitoring or by a wrist actigraphy in association with a sleep log despite the limits of these tests. The MSLT being the gold standard to measure excessive daytime sleepiness, this test was chosen to measure the excessive sleepiness characterizing IH. However, several caveats apply and challenge the relevance of this test in the case of IH. Awakening the patient in the morning in view of the following MSLT sessions precludes documenting a possible prolonged night sleep and the MSLT sessions preclude recording of possible prolonged unrefreshing daytime sleep episodes.37 Some of the IH patients, those affected by the form with long sleep duration, suffer from altered alertness not explored by the MSLT.23 The cut-off used for IH, the 8 min threshold, was copied from narcolepsy diagnostic criteria for reason of simplicity even if not tailored for this condition. As previously indicated, the validity of the mean sleep latency during the MSLT in diagnosing IH was brought into question in two successive studies.18,19 Forty out of 72 patients with IH had a mean sleep latency less than 8 min, but 32 out of the 72 a mean sleep latency of 8 min or more in the first study18 and 46 out of 75 patients with IH a mean sleep latency less than 8 min, but 29 of the 75 a mean sleep latency of 8 min or more in the second study.19 Moreover, as mentioned above, two studies recently questioned the consistency of the MSLT overtime.38,39 The first one included 13 patients with IH, 7 patients with NwoC and 16 subjects with physiological hypersomnia, who underwent MSLT at an interval of 4.2 ± 3.8 years.38 A change in diagnosis occurred in 53% of the patients in relation with a change in the mean sleep latency or in the number of SOREMPs. The second one, included 28 patients with IH, 33 with NT2, 14 with unspecified excessive daytime sleepiness and 22 with NT1, who underwent MSLT at a 1.9-year interval (range 0.02–11.9 years).39 The repeatability in the patients with NT1 (81.3%) was significantly higher than in the patients with NT2 (47.1%), IH (25.0% only) and unspecified excessive daytime sleepines (42.1%). Thus, patients with IH and NT2 show a poor test–retest reliability of the MSLT.
24-Hour and 32-Hour Polysomnographic Monitoring
Several 24-hour ad libitum polysomnographic protocols for capturing excessive sleep duration have been developed.15,19,40 A first protocol including night 1 (10:30 pm–7:30 am) followed by an MSLT (day 1) and then, from 6:30 pm to 6:30 pm the next day (night 2 and day 2) an ad libitum monitoring, was developed by Billiard et al as soon as 1998 and used routinely in Montpellier.15 This protocol was re-used with slight modifications by Vernet and Arnulf in 2009,19 but for the first time, these authors provided normative values for the duration of sleep during an ad libitum 24h continuous monitoring in 35 healthy controls. Compared with controls, the limit of 11 hours of sleep presented the best sensitivity (72%) and the best specificity (97%) to discriminate IH patients from controls. A second protocol including an ad libitum monitoring of sleep during the first 48 hours (day 1, night 1, day 2 and night 2) followed by an MSLT on day 3, was then proposed by Pizza et al.40 However, this protocol did not provide normative values. Each of these two protocols had advantages and disadvantages, but both of them lacked standardization regarding the level of physical and social activity during the ad libitum procedure. Hence, the interest and value of a more recent 32-hour controlled bed rest protocol, including one night polysomnography (11 pm to 7 am) followed by a “modified MSLT” (5 nap opportunities every 2 hours, between 9 am and 5 pm, with the subjects awakened after 1 min of sleep), followed by a 32-hour bed rest protocol (night 1, 11 pm-7 am; daytime, 7 am-11 pm; night 2, 11 pm-7 am), the aim of the bedrest condition being to obtain a maximum amount of sleep in totally standardized conditions, avoiding any form of external influences. This protocol was tested in 37 clear-cut patients with IH, 79 probable patients with IH and 21 controls. Receiver operating characteristic curves were used to find total sleep time cut-off values. The total sleep time cut-off discriminating clear-cut patients with IH from controls was 19 hours for the 32-hour recording (sensitivity 91.9%, specificity 85.7%) and 12 hours (sensitivity 100%, specificity 85.7%) for the first 24 hours. Noteworthy, patients with IH above the 19-hour cut-off had more sleep inertia and had higher total sleep time on all periods compared to patients below 19 hours. However, a limitation of this test is its complexity, making it difficult to be performed in most sleep clinics around the world.
Actigraphic Monitoring
Actigraphic monitoring plays a major role in order to rule out insufficient sleep syndrome and circadian rhythm sleep/wake disorders. In regard, studies using actigraphic monitoring in central disorders of hypersomnolence are scarce. Recently, 33 patients with a diagnosis of IH underwent ad libitum polysomnography with concurrent use of Actiwatch 2.42 Actiwatch 2 sleep–wake activity threshold (SWAT) and sleep immobility onset and offset (SIOO) duration were modified during data processing. Low SWAT + 25 epochs SIOO displayed the least divergent from polysomnographic monitoring (mean difference 3.4 ± 8.72 min). Higher SWAT and lower SIOO increased sensitivity and accuracy, at the expense of reducing specificity and the ability to accurately estimate total sleep time. However, as pointed out by Trotti, only a fraction of these subjects fulfilled the ICSD-3 criteria of IH.43
In-Depth Analyses of Nocturnal Sleep and MSLT
These analyses have been developed to help the diagnosis of central disorders of hypersomnolence. Here we will concentrate on analyses of interest for IH.
Analysis of sleep latencies to the occurrence of the first epoch of sleep stage 1 NREM and of three consecutive sleep stage 1 NREM epochs or any other single epoch was performed in 44 patients with NwC, 7 patients with NwoC and 16 patients with IH.44 IH patients showed significantly longer latencies to the occurrence of three consecutive sleep stage 1 NREM epochs or any other single epoch than to the occurrence of the first epoch of sleep stage 1 NREM compared to patients with NwC and NwoC. Analysis of eleven variables of the nocturnal polysomnography in 101 patients diagnosed with NwC (n=24), NwoC (n=38), IHwLST (n=21) and behavior-induced inadequate sleep syndrome (n=18) showed a higher proportion of sleep stage 3 (p<0.05) in patients with NwoC and IHwLST.45 Pizza et al compared sleep architecture in 19 patients with IHwoLST, 17 patients with NwC and 13 controls.46 Patients with IHwoLST had increased time in bed, sleep period time and total sleep time, and decreased sleep onset latency in comparison with normal controls and increased in number of stage shifts, number of awakenings and sleep stage 1 percentage in comparison with controls and patients with NwC. Comparison of the macro and microstructure of sleep in a sample of NT1 (n=24), NT2 (n=3 and IH (n=25) patients and a snoring reference group of 24 subjects showed a higher sleep efficiency (p < 0.05) and a lower wake after sleep onset (p < 0.01) in patients with IH, but similar arousal indices in comparison with patients with NT1.47 Maski et al checked if patients with NT1 (n=46), NT2 (n=12) and IH (n= 18) had distinct nocturnal sleep stability measures (number of wake and sleep stage bouts) in comparison with subjectively sleepy controls (n=48).48 They found out that patients with IH had a similar number of bouts but better survival of stage N2 bouts (p=0.001) and shorter stage N3 bouts in the first 8 hours of sleep (p=0.003). Altogether, these analyses bring reliable statistics polysomnographic and MSLT features with potential application at the individual level, but only for supportive purpose.
Circadian Control Tests
In a study by Nevsimalova et al salivary samples of melatonin and cortisol were taken over a 24-hour period from 15 patients with IHwLST and sleep drunkenness and from 15 controls, and measured by direct radioimmunoassay.49 Remarkably enough, the melatonin and cortisol rhythms in patients with IHwLST were significantly phase delayed in comparison with those in control subjects. More recently, urine melatonin metabolites were measured in patients with IH.50 A long biological night was demonstrated at 16 ± 1.2 hours. Of note, the biological night was normal at 9 hours or less in 10 patients, possibly in relation with the presence of both patients with IHwLST and with IHwoLST in the sample.
Research Techniques
Advances in neuroimaging, investigations of the diurnal dynamics of circadian clock gene expression and measure of an endogenous positive allosteric modulator of GABA-A receptors in the cerebrospinal fluid (CSF) open up the possibility for new powerful tools to be applied to clinical populations in order to improve the diagnosis of IH.
Neuroimaging
Boucetta et al used SPECT in 13 patients with IH following ICSD-3 criteria.51 They found two opposite patterns of rCBF perfusion, a lowered rCBF in medial prefrontal cortex, posterior cingulate cortex and putamen and an increased rCBF in the left amygdala and temporo-occipital cortices. Lowered rCBF in the medial prefrontal cortex was associated with higher self-reported daytime sleepiness as reflected by ESS score. Dauvilliers et al used [18F] fludeoxyglucose-PET in 6 patients with NT1, 9 patients with IH according to ICSD-3 and 13 healthy controls.52 They found an increased metabolism in the anterior and middle cingulate and in the insula in the two pathological conditions as compared with healthy controls. Comparisons between patient groups were non-significant. Trotti et al used fluorodeoxyglucose-PET in 14 patients with NT1, 16 patients with IH and 9 controls.53 They found somewhat overlapping, but distinct patterns of regional metabolism. Overall, neuroimaging findings showed inconsistent results likely due to insufficiently defined phenotypes of the patients, that is IH with insufficient affiliation status, and thus, at this point, cannot serve to improve the diagnosis of IH.
Investigation of the Diurnal Dynamic of Circadian Clock Gene Expression
As soon as 2011 an association study was performed in 86 patients suffering from excessive sleepiness to analyze whether there is a genetic predisposition resulting from the involvement of sequence variants in the genes CRY1, CRY2 and BMAL1.54 One polymorphism was detected in CRY1, which was associated with excessive sleepiness regardless of the underlying specific sleep disorder and was not present in the control group. This result suggests that CRY1 could play a role in the complex genetics of hypersomnias of central origin. Later on, dermal fibroblasts have been used and have produced fascinating evidence that key circadian genes are abnormally expressed in IH. Ten patients with IH were chosen after rigorous diagnostic evaluation including clinical, polysomnographic and MSLT criteria.55 Dermal fibroblasts were obtained by skin biopsy. The expression of key circadian proteins was measured over two consecutive 24-hour periods and compared to concentrations in a healthy control group. The circadian amplitudes of the expressed genes BMAL1, PER1 and PER2 were decreased in fibroblasts of patients with IH as compared to those of healthy controls. Posteriorly, Materna et al examined the circadian period length of dermal fibroblasts in 15 patients with IH according to standard criteria of ICSD-3.56 Circadian period length of fibroblasts was measured using a lentiviral bioluminescence assay that transfected a luciferase gene under the control of BMAL1 promoter into human fibroblast cells. Patients with IH had significantly longer circadian period lengths than controls.
Endogenous Positive Allosteric Modulator of GABA-A in the CSF
In 32 subjects presenting for evaluation of a suspected primary hypersomnia including IH, NwC, subjective hypersomnia and long sleeper, Rye et al showed that CSF from these subjects facilitated the binding of GABA-A to the GABA receptor in vitro, which was not the case with CSF from control subjects.57 The bioactive CSF compound had a mass of 500 to 3000 daltons. This finding is of special interest but would benefit from being performed and compared in homogeneous groups of patients with NT2, IHwLSD and IHwoLSD, long sleepers and controls.
Proposal for Diagnostic Evaluation of Idiopathic Hypersomnia in the Absence of Biological Marker and of Robust Electrophysiological Criteria
First Step of the Diagnostic Evaluation: Rule Out Other Causes of Hypersomnolence by Interview, Physical Examination, Questionnaires and Laboratory Tests
Insufficient sleep syndrome by interview and sleep log; circadian rhythm sleep disorder by interview, sleep log, Horne and Östberg morningness-eveningness questionnaire,35 or Munich questionnaire;58 obstructive sleep apnea syndrome by interview, Berlin questionnaire,59 physical examination and home sleep respiration testing/polysomnography; hypersomnolence associated with psychiatric disorders, major depressive disorder, bipolar 1 and 2 disorders, and schizoaffective disorder, by Beck depression inventory27 and evaluation by a psychiatrist involved in sleep medicine; hypersomnolence due to a medical condition such as traumatic brain injury, infectious disease, endocrine disorder, by interview, physical examination and relevant laboratory tests.
Second Step: Diagnosis of IH
In the absence of biological markers and the relative inconsistency of the results of the MSLT, except in the case of NT1, clinical interview should have the first place in the diagnosis of IH, IHwLSD and IHwoLSD. It should include interviewing patients about excessive daytime sleepiness and decreased alertness, duration and refreshing quality of naps, duration and quality of nocturnal sleep, degree of sleep inertia; looking for the presence of cognitive symptoms such as attention and memory deficit, limited mental endurance, inappropriate conversation entries; questioning about autonomic symptoms, particularly in the orthostatic and vasomotor domains; assessing comorbidities and eliminating cataplexy.
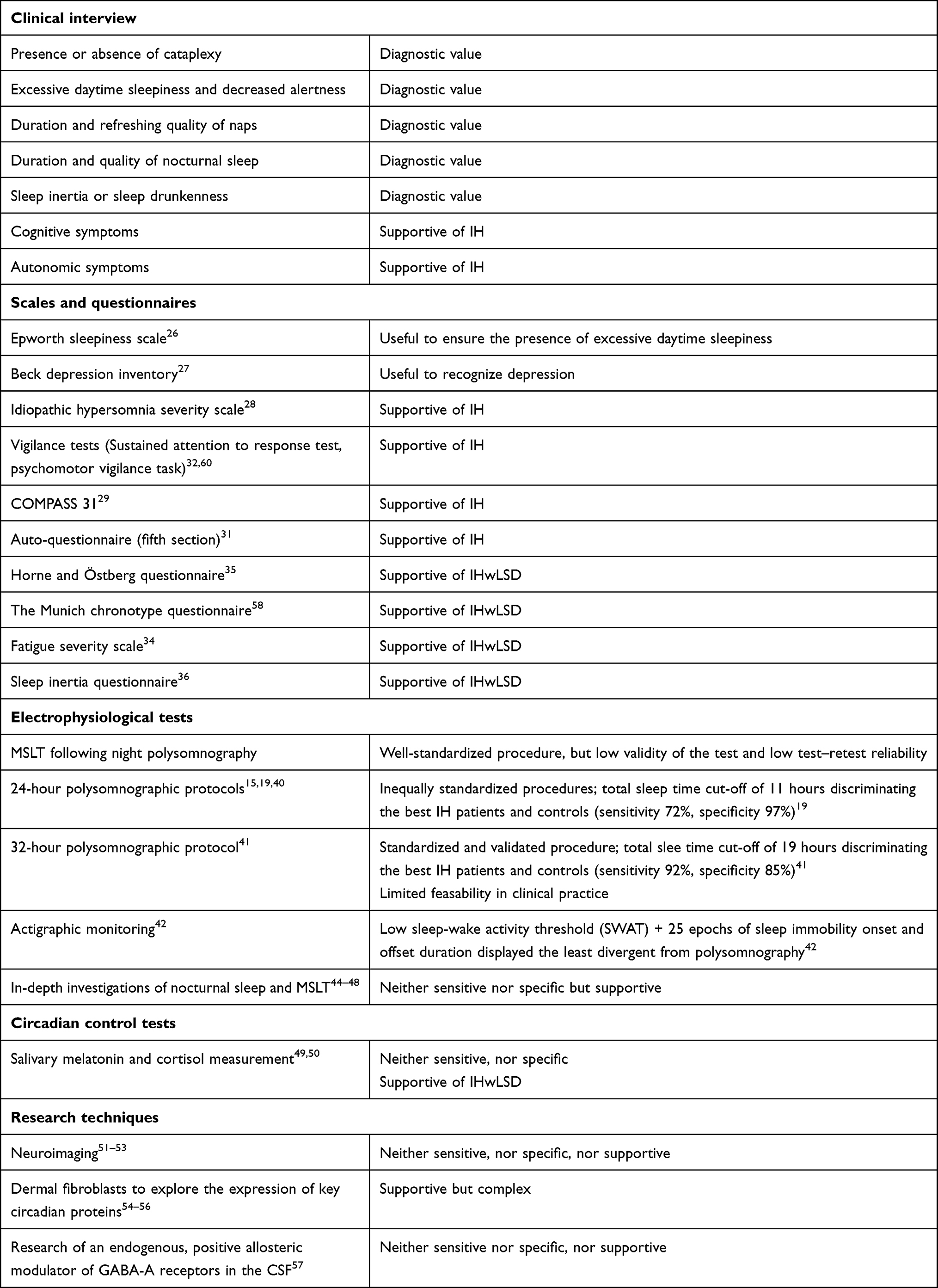 |
Table 2 Diagnostic evaluation of Idiopathic Hypersomnia, in the Absence of Biological Markers and Definite Electrophysiological Criteria |
Questionnaires and scales should include some or all of the following, according to clinical features: Epworth sleepiness scale;26 Beck depression inventory;27 idiopathic hypersomnia severity scale;28 vigilance tests, sustained attention to response task (SART)60 and/or psychomotor vigilance test (PVT) ;32 composite autonomic symptom score (COMPASS 31);29 the section on non-sleep problems of the auto-questionnaire designed by Vernet et al;31 Horne and Östberg morningness-eveningness questionnaire;35 Munich chronotype questionnaire;58 fatigue severity scale;34 and sleep inertia questionnaire.36
Electrophysiological tests remain an important part of the diagnosis in as much as their limitations are taken into consideration. Classical tests include MSLT, 24-hour polysomnographic recording15,19,40 or 32-hour controlled polysomnographic bed rest protocol41 and actigraphic monitoring.42 Lammers et al proposed giving them, particularly the MSLT, a weighting based on their sensitivity and specificity.23 In addition, in-depth analyses of nocturnal sleep may have a supportive value.44–48Circadian control tests, melatonin and cortisol, have value supporting the diagnosis of IHwLSD.49,50 Currently, neuroimaging,51–53 expression of key circadian proteins in dermal fibroblasts54–56 and measure of an endogenous positive allosteric modulator of GABA-A in the CSF57 cannot yet be considered as helpful in the diagnosis of IH (Table 2).
Conclusion
After wavering between one or two forms of IH during 40 years, recent approaches have given credit to a distinction between IHwLSD and a more heterogeneous subtype grouping IHwoLSD and NT2. Different tests currently used in the diagnosis of IH have been reviewed with their strengths and limitations. At present, definite diagnostic criteria of IH are not yet available, but a body of clinical symptoms, relevant scales and questionnaires, electrophysiological tests of various weighted sensitivity and specificity, and circadian control tests, opens the path for a rather reliable diagnosis of IH and of its subtypes, IHwLSD and IHwoLSD, despite the absence of biological markers.
Abbreviations
CNS, central nervous system; CSF, cerebrospinal fluid; ESS, Epworth sleepiness scale; ICSD, International Classification of Sleep Disorders; IH, Idiopathic hypersomnia without affiliation status; IHwLST, idiopathic hypersomnia with long sleep time (from ICSD-2 to 2020); IHwoLST, idiopathic hypersomnia without long sleep time (from ICSD-2 to 2020); IHwLSD, idiopathic hypersomnia with long sleep duration (from 2020 on); IHwoLSD, idiopathic hypersomnia without long sleep duration (from 2020 on); MSLT, multiple sleep latency test; NT1, narcolepsy type 1 (from ICSD-3, 2014, on); NT2, narcolepsy type 2 (from ICSD-3, 2014, on); NwC, narcolepsy with cataplexy (from ICSD-2, 2005, to ICSD-3, 2014); NwoC, narcolepsy without cataplexy (from ICSD-2, 2005, to ICSD-3, 2014); PET, positron emission tomography; rCBF, regional cerebral blood flow; SOREMP, sleep onset REM period; SPECT, single photon emission computed tomography.
Credit Authorship Contribution Statement
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
Dr Sonka is supported by the grant from the Czech Ministry of Health AZV NU20-04-00088 touching idiopathic hypersomnia.
Disclosure
Dr Karel Sonka reports grants from Ministry of Health of the Czech Republic, during the conduct of the study. The authors declared no potential conflicts of interest with respect to authorship and/or publication of the article.
References
1. Ohayon MM, Reynolds III CF, Dauvilliers Y. Excessive sleep duration and quality of life. Ann Neurol. 2013;73(6):785–794. doi:10.1002/ana.23818
2. Dauvilliers Y, Paquereau J, Bastuji H, Drouot J, Weil JS, Viot-Blanc V. Psychological health in central hypersomnias: the French Harmony Study. J Neurol Neurosurg Psychiatry. 2009;80(6):636–641. doi:10.1136/innp.2008.161588
3. Roth B. Idiopathic hypersomnia. In: Roth B, editor. Narcolepsy and Hypersomnia. Basel: Karger; 1980:
4. Billiard M, Sonka K. Idiopathic hypersomnia. Sleep Med Rev. 2016;29(10):23–33. doi:10.1016/j.smrv.2015.08.007
5. Roth B. Narcolepsy and hypersomnia. Review and classification of 642 personally observed cases. Schweiz Arch Neurol Neurochir Psychiat. 1976;119(1):31–41.
6. Roth B. Spankova opilost a spankova obrna [Sleep drunkenness and sleep paralysis]. Cesk Neurol. 1956;19(1):48–58. Czech.
7. Dement WC, Rechtschaffen A, Gulevich G. The nature of the narcoleptic sleep attack. Neurology. 1966;16(1):18–33. doi:10.1212/wnl.16.18
8. Berti-Ceroni G, Coccagna G, Gambi D, Lugaresi E. Considerationi clinico poligrafiche sull narcolessia essenziale “a sonno lento” [Clinico-polygraphic considerations on essential “slow sleep” narcolepsy]. Sist Nerv. 1967;19(2):81–89. Italian.
9. Passouant P, Popoviciu L, Velok G, Baldy-Moulinier M. Etude polygraphique des narcolepsies au cours du nycthémère. [Polygraphic study of narcolepsy during the nycthemeral period]. Rev Neurol. 1968;118(6):431–441. French.
10. Rechtschaffen A, Dement WC. Narcolepsy and hypersomnia. In: Kales A, editor. Sleep: Physiology and Pathology. JB Lippincott Co; 1969:119–130.
11. Roth B, Nevsimalova S, Rechtschaffen A. Hypersomnia with “Sleep drunkenness”. Arch Gen Psychiat. 1972;26(5):456–462. doi:10.1001/archpsyc197201750230066013
12. Association of Sleep Disorders Centers. Diagnostic classification of sleep and arousal disorders. First edition, prepared by the sleep disorders classification committee, HP Roffwarg, Chairman. Sleep. 1979;2(1):1–154. doi:10.1093/sleep/2.1.1
13. Diagnostic Classification Steering Committee, Thorpy MJ, Chairman. International Classification of Sleep Disorders. Diagnostic and Coding Manual. Rochester, Minnesota: American Sleep Disorders Association; 1990.
14. Bassetti C, Aldrich M. Idiopathic hypersomnia. A series of 42 patients. Brain. 1997;120(Pt 8):1423–1435. doi:10.1093/brain/120.8.1423
15. Billiard M, Merle C, Carlander B, Ondze B, Alvarez D, Besset A. Idiopathic hypersomnia. Psychiatry Clin Neurosci. 1998;52(2):125–129. doi:10.1111/j.1440-1819.1998.tb00987.x
16. American Academy of Sleep Medicine. International Classification of Sleep Disorders, 2nd ed.: Diagnostic and Coding Manual. Westchester, Illinois: American Academy of Sleep Medicine; 2005.
17. Billiard M. Diagnosis of narcolepsy and idiopathic hypersomnia. An update based on the International classification of sleep disorders, 2nd ed. Sleep Med Rev. 2007;11(5):377–388. doi:10.1016/j.smrv.2007.04.001
18. Anderson KN, Pilsworth S, Sharples L, Smith I, Shneerson J. Idiopathic hypersomnia: a study of 77 cases. Sleep. 2007;30(10):1274–1281. doi:10.1093/sleep/30.10.1274
19. Vernet C, Arnulf I. Idiopathic hypersomnia with and without long sleep time: a controlled series of 75 patients. Sleep. 2009;32(6):753–759. doi:10.1093/sleep132.6.753
20. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
21. Sonka K, Susta M, Billiard M. Narcolepsy with and without cataplexy, idiopathic hypersomnia with and without long sleep time. A cluster analysis. Sleep Med. 2015;16(2):225–231. doi:10.1016/j.sleep2014.09.016
22. Fronczek R, Arnulf I, Baumann CR, Maski K, Pizza F, Trotti LM. To split or to lump? Classifying the central disorders of hypersomnolence. Sleep. 2020;43(8):1–8. doi:10.1093/sleepzsaa044
23. Lammers GJ, Bassetti CLA, Dolenc-Groselj L, et al. Diagnosis of central disorders of hypersomnolence. A reappraisal by European experts. Sleep Med Rev. 2020;52:101306. doi:10.1016/j.smrv.2020.101306
24. Trotti LM, Ong JC, Plante DT, Friederich MC, King R, Bliwise DL. Disease symptomatology and response to treatment in people with idiopathic hypersomnia: initial data from Hypersomnia Foundation Registry. Sleep Med. 2020;75:343–349. doi:10.1016/j.sleep.2020.08.034
25. Nevsimalova S, Susta M, Prihodova I, Maurovich Horvat E, Milata M, Sonka K. Idiopathic hypersomnia: a homogeneous or heterogeneous disease? Sleep Med. 2021;80:86–91. doi:10.1016/j.sleep.2021.01.031
26. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
27. Beck AT, Ward CH, Mendelson M, Mock JE. An inventory to measuring depression. Arch Gen Psychiatry. 1961;4(6):561–571. doi:10.1001/archpsyc.1961.01710120031004
28. Dauvilliers Y, Evangelista E, Barateau L, et al. Measurement of symptoms in idiopathic hypersomnia: the idiopathic hypersomnia severity scale. Neurology. 2019;92(15):e1754–e1762. doi:10.1212/WNL.0000000000007264
29. Sletten DM, Suarez GA, Low PA, Mandrekar J, Singer W. COMPASS 31: a refined and abbreviated composite autonomic symptom score. Mayo Clin Proc. 2012;87(12):1196–1201. doi:10.1016/j.mayocp.2012.10.013
30. Miglis MG, Schneider L, Kim P, Cheung J, Trotti LM. Frequency and severity of autonomic symptoms in idiopathic hypersomnia. J Clin Sleep Med. 2020;16(5):749–756. doi:10.5664/jcsm.8344
31. Vernet C, Leu-Semenescu S, Buzare M, Arnulf I. Subjective symptoms in idiopathic hypersomnia: beyond excessive sleepiness. J Sleep Res. 2010;19(4):525–534.
32. Dinges DF, Powell JW. Microcomputer analysis of performance on a portable, simple visual RT task sustained operation. Behav Res Meth Instrum Comput. 1985;17(6):652–655. doi:10.3758/BF03200977
33. Evangelista E, Rassu AL, Lopez R, et al. Sleep inertia measurement with the psychomotor vigilance task in idiopathic hypersomnia. Sleep. 2021;26:zsab220. doi:10.1093/sleep/zsab.22
34. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46(10):1121–1123. doi:10.1001/archneur.1989.00520460115022
35. Horne JA, Östberg O. A self assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97–110.
36. Kanady JC, Harvey AC. Development and validation of the sleep inertia questionnaire (SIQ) and assessment of sleep inertia in analogue and clinical depression. Cognit Ther Res. 2015;39(5):601–612. doi:10.1007/s10608-015-9686-4
37. Billiard M, Dauviliers Y. Idiopathic hypersomnia. Sleep Med Rev. 2001;5(5):351–360. doi:10.1053/smrv.2001.0168
38. Trotti LM, Staab BA, Rye DB. Test-retest reliability of the multiple sleep latency test in narcolepsy without cataplexy and idiopathic hypersomnia. J Clin Sleep Med. 2013;9(8):789–795. doi:10.5664/jcsm.2922
39. Lopez R, Doukkali A, Barateau L, et al. Test-retest reliability of the multiple sleep latency test in central disorders of hypersomnolence. Sleep. 2017;40:12. doi:10.1093/sleep/zsx164
40. Pizza F, Moghadam KK, Vandi S, et al. Daytime continuous polysomnography predicts multiple sleep latency results in hypersomnias of central origin. J Sleep Res. 2013;22(1):32–40. doi:10.1111/j.1365-2869.2012.01032.x
41. Evangelista E, Lopez R, Barateau L, et al. Alternative diagnostic criteria for idiopathic hypersomnia: a 32-hour protocol. Ann Neurol. 2018;83(2):235–247. doi:10.1002/ana.25141
42. Cook JD, Eftekari SC, Leavitt LA, Prairie LM, Plante DT. Optimizing actigraphic estimation of sleep duration in suspected idiopathic hypersomnia. J Clin Sleep Med. 2019;15(4):597–602. doi:10.5664/jcsm.7722
43. Trotti LM. Are we there yet? Getting closer to certainty in idiopathic hypersomnia diagnosis. J Clin Sleep Med. 2019;15(4):539–540. doi:10.5664/jcsm.7706
44. Pizza F, Vandi S, Detto S, et al. Different sleep onset criteria at the multiple sleep latency test (MSLT): an additional marker to differentiate central nervous system (CNS) hypersomnias. J Sleep Res. 2011;20(ipt2):250–256. doi:10.1111/j.1365-2869.2009.00808.x
45. Drakatos P, Kosky CA, Higgins SE, Muza RT, Williams AJ, Leschziner GD. First rapid eye movement sleep periods and sleep-onset rapid eye movement periods in sleep-stage sequencing of hypersomnias. Sleep Med. 2013;14(9):897–901. doi:10.1016/j.sleep.2013.03.021
46. Pizza F, Ferri R, Poli F, Vandi S, Cosentino FII, Plazzi G. Polysomnographic study of nocturnal sleep in idiopathic hypersomnia without long sleep time. J Sleep Res. 2013;22(2):185–196. doi:10.1111/j.1365-2869.2012.01061.x
47. Cairns A, Bogan R. Comparison of the macro and microstructure of sleep in a sample of sleep clinic hypersomnia cases. Neurobiol Sleep Circadian Rhythms. 2019;6:62–69. doi:10.1016/j.nbscr.2019.02.001
48. Maski KP, Colclasure A, Little E, et al. Stability of nocturnal wake and sleep stages defines central nervous system disorders of hypersomnolence. Sleep. 2021;44(7):zsab021. doi:10.1093/sleep/zsab021
49. Nevsimalova S, Blazejova K, Illnerova H, et al. A contribution to pathophysiology of idiopathic hypersomnia. In: Ambler Z, Nevsimalova S, Kadanka Z, et al. editors. Clinical Neurophysiology at the Beginning of the 21st Century. Suppl Clin Neurophysiol; Vol. 53, 2000:366–370. doi:10.1016/s1567-424x(09)70183-7
50. Thomas RJ, Naik S. The circadian variant of idiopathic hypersomnia. Sleep. 2017;40(Suppl 1):A243. doi:10.1093/sleepj/zsx050.656
51. Boucetta S, Montplaisir J, Zadra A, et al. Altered regional cerebral flow in idiopathic hypersomnia. Sleep. 2017;40(10). doi:10.1093/sleep/zsx140
52. Dauvilliers Y, Evangelista E, de Verbizier D, Barateau L, Peigneux P. [18F] Fludeoxyglucose-positron emission tomography evidence for cerebral hypermetabolism in the awake state in narcolepsy and idiopathic hypersomnia. Front Neurol. 2017;8:350. doi:10.3389/fneur.2017.00350
53. Trotti LM, Saini P, Crosson B, Meltzer CC, Rye DB, Nye JA. Regional brain metabolism differs between narcolepsy type 1 and idiopathic hypersomnia. Sleep. 2021;44(8):zsab050. doi:10.1093/sleep/zsab050
54. Schirmacher AHH, Heidbreder A, Happe S, et al. Sequence variants in circadian rhythmic genes in cohort of patients suffering from hypersomnia of central origin. Biol Rhythm Res. 2011;42(5):407–416. doi:10.1080/09291016.2010.525382
55. Lippert J, Halfter H, Heidbreder A, et al. Altered dynamics in the circadian oscillation of clock genes in dermal fibroblasts of patients suffering from idiopathic hypersomnia. PLoS One. 2014;9(1):e85255. doi:10.1371/journal.pone.0085255
56. Materna I, Halfter H, Heidbreder A, et al. Idiopathic hypersomnia patients revealed longer circadian period length in peripheral skin fibroblasts. Front Neurol. 2018;9:424. doi:10.3389/fneur.2018.00424
57. Rye DB, Bliwise DL, Parker K, et al. Modulation of vigilance in the primary hypersomnias by endogenous enhancement of GABAA receptors. Sci Transl Med. 2012;4(161):161 ra151. doi:10.1126/scitrans/med.3004685
58. Juda M, Vetter C, Roenneberg T. The Munich chronotype questionnaire for shift-workers (MCTQShift). J Biol Rhythms. 2013;28(2):130–140. doi:10.1177/0748730412475041
59. Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Internal Med. 1999;131(7):485–491. doi:10.7326/0003-4819-131-7-199910050-00002
60. Robertson IH, Manly T, Andrade J, Baddeley BT, Yiend J. “Oops!” Performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia. 1997;35(6):747–758. doi:10.1016/s0028-3932(97)00015
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.