")
Back to Journals » International Journal of General Medicine » Volume 13
Idiopathic Cervical Esophageal Webs: A Case Report and Literature Review
Authors Petrea OC , Stanciu C , Muzica CM , Sfarti CV , Cojocariu C, Girleanu I , Huiban L, Trifan A
Received 28 August 2020
Accepted for publication 16 October 2020
Published 16 November 2020 Volume 2020:13 Pages 1123—1127
DOI https://doi.org/10.2147/IJGM.S278999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Oana Cristina Petrea,1,2 Carol Stanciu,2 Cristina Maria Muzica,1,2 Catalin Victor Sfarti,1,2 Camelia Cojocariu,1,2 Irina Girleanu,1,2 Laura Huiban,1 Anca Trifan1,2
1Department of Gastroenterology, “Grigore T. Popa” University of Medicine and Pharmacy, Iasi, Romania; 2Institute of Gastroenterology and Hepatology, Iasi, Romania
Correspondence: Carol Stanciu
Institute of Gastroenterology and Hepatology, “St Spiridon” Emergency Hospital, Iași 700111, Romania
Tel +40722306020
Email [email protected]
Abstract: An esophageal web is a thin and smooth extension of normal esophageal tissue consisting of mucosa and submucosa that can occur anywhere along the length of the esophagus but is typically located in the cervical segment. The webs can be congenital or acquired, commonly associated with Plummer-Vinson syndrome and rarely with celiac disease, dermatological disorders or graft-versus-host disease. A 54-year-old man was referred to our hospital with a history of high non-progressive dysphagia to solid food, meat impaction and weight loss over last ten months. His medical history and family history were unremarkable nor was the physical examination. Complete blood count and basic biochemical tests were normal. Antigliadin and antiendomysial antibodies for celiac disease were negative. Barium swallow esophagography and upper endoscopy detected cervical esophageal webs. The treatment consisted of endoscopic balloon dilation. The patient’s dysphagia resolved shortly after dilation, and the endoscope passed easily through the esophagus showing normal esophageal, gastric and duodenal mucosa. This report is consistent with a case of esophageal webs rarely documented in males and that is not related with common causes like Plummer-Vinson syndrome. Thus, the pathogenesis and treatment of esophageal webs are evolving.
Keywords: esophageal webs, dysphagia, cervical esophagus, endoscopic dilation
Introduction
An esophageal web is a thin membranous structure which may obstruct the esophageal lumen leading to dysphagia. These webs are typically located in the cervical esophagus, although they can occur anywhere along the length of the esophagus.1 The prevalence of cervical esophageal webs is not known because most of them are asymptomatic. They are seen in 5–15% of patients who had a barium swallow for evaluation of dysphagia.1 Most commonly, the acquired cervical esophageal webs are associated with Plummer-Vinson syndrome (PVs), also known as Paterson–Brown–Kelly syndrome, characterized by the association of dysphagia, iron-deficiency anemia and esophageal webs, affecting mainly women (80%).2 It should be underlined that most proximal webs are considered idiopathic, despite many cases associating other structural lesions such as Zenker diverticulum, heterotopic gastric mucosa, esophageal duplication cyst, and laryngeal carcinoma, as well as dermatological disorders such as epidermolysis bullosa, pemphigus or psoriasis.1
Esophagoscopy proved to be inferior to barium swallow for the diagnosis of esophageal webs. Indeed, upper digestive endoscopy can be a reliable method regarding evaluation of normal mucosa and has a therapeutic advantage. Thus, endoscopy dilation is the method of choice for the treatment of dysphagia due to esophageal webs.
The case described in this report highlights some aspects such as the importance of a differential diagnosis between esophageal webs and other structural lesions or associated conditions that may lead to dysphagia. Likewise, despite the fact that esophageal webs are mostly associated with PVs, this case has allowed us to describe a rare case of idiopathic esophageal webs.
Case Presentation
A 54-year-old man was referred to our hospital with a history of high non-progressive dysphagia to solid food, meat impaction and ~8 kg of weight loss over last ten months because low intake on account of dysphagia as his appetite was normal. He denied heartburn, acute caustic ingestion, any history of chest pain, vomiting or loss of appetite. His medical history and family history (including atopic disease) were unremarkable as well as physical examination; in particular, the patient has no anemia, koilonychia, glossitis or stomatitis.
Basic biochemical tests and complete blood count were normal (white blood cell count: 9730/mm3, eosinophils: 70/mm3, hemoglobin level: 14.2 g/dl, mean corpuscular volume: 91.7 fL, serum iron level: 91 mcg/dL and ferritin level: 113 mg/L). Antigliadin and antiendomysial antibodies for celiac disease were negative.
We performed a barium swallow esophagram that showed two linear, circumferential filling defects on the anterior aspect of the cervical esophagus, consisting with the diagnosis of esophageal webs (Figure 1). Likewise, upper gastrointestinal endoscopy confirmed the presence of the cervical webs at 17 cm from the incisors with the endoscope not able to pass through (Figure 2). In order to exclude any other causes of dysphagia, computed tomography was performed. This revealed no abnormality around the esophagus, such as a tumor or swollen lymph nodes, which can cause luminal stenosis.
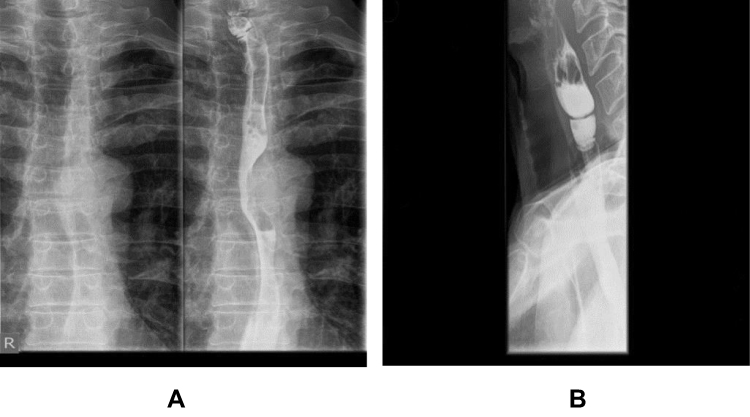 |
Figure 1 Barium swallow esophagram (A). Two cervical esophageal webs (caused by mucosal diaphragm) (B). |
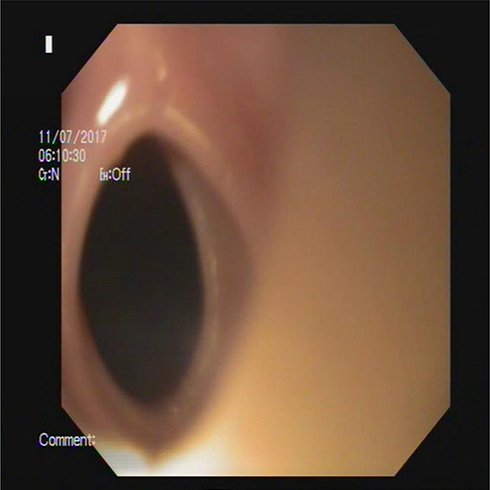 |
Figure 2 Endoscopic view of the cervical esophageal web. |
Thus, other causes of cervical esophageal webs were ruled out, including motility disorders, celiac disease, PVs syndrome, Zenker diverticulum, benign or malignant tumors or extrinsic compression of esophagus.
The treatment consisted of endoscopic balloon dilation without any complications (Figure 3). We used the Boston Scientific CRE Wireguided Balloon Dilation Catheter with the size 15 – 16.5–18 mm, who was inflated to 7 atm, the pressure needed to obtain an 18 mm diameter. Only one dilation was performed with excellent clinical and endoscopic results. After this procedure the patient’s dysphagia resolved immediately and the endoscope passed easily in through the esophagus showing normal esophageal, gastric and duodenal mucosa.
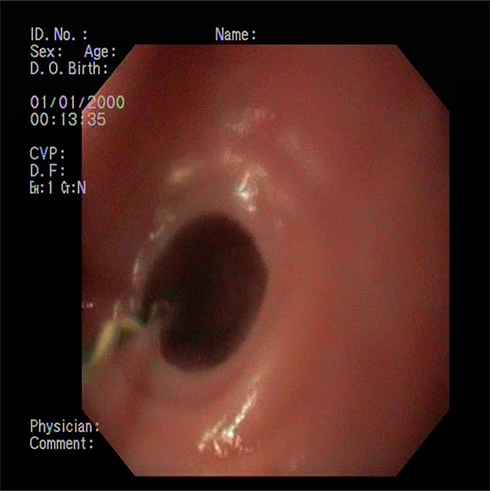 |
Figure 3 Endoscopic dilation of cervical esophageal web. |
At the first follow-up, twelve months after endoscopic ballon dilation, the patient gained weight and he had no complains. Likewise, he remained asymptomatic and did not show any recurrence for three years. A second procedure was not considered necessary by the medical personnel or the patient during the follow-up.
Discussion
Esophageal webs are rare structural lesions typically located in the cervical esophagus, but they may, nonetheless, represent a diagnostic and therapeutic challenge in front of a patient presenting with dysphagia and food impaction.
Although most cases of esophageal webs reported in the literature are associated with PVs along with dysphagia and iron-deficiency anemia, there are numerous causes of esophageal webs (Table 1). However, the incidence of PVs has decreased during the last decades probably as the consequence of largely available iron-replacement therapy.23–25
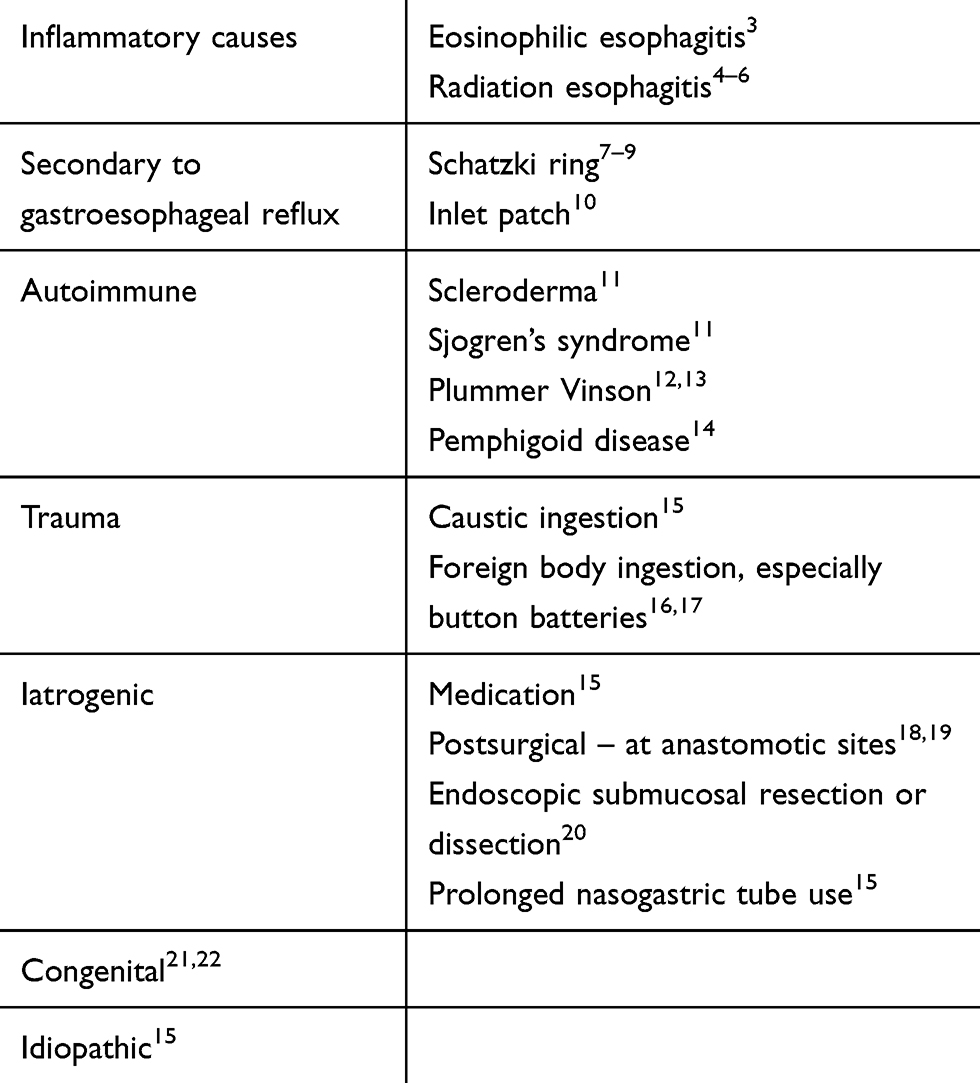 |
Table 1 Causes of Esophageal Webs |
Esophageal webs can also be rarely associated with celiac disease,6,7 where iron-deficiency is usually the cause of anemia, dermatological conditions8–10 or graft-versus-host-disease.11,12 It should be noted that dysphagia associated with iron-deficiency anemia is not always due to PVs. Thus, differential diagnosis is essential and includes several others causes such pharyngeal pouch, Zenker diverticulum, benign esophageal strictures, vascular rings, retained foreign bodies in the esophagus, surgical esophageal anastomosis, benign and malignant esophageal tumors, pernicious anemia, rheumatoid arthritis, epidermolysis bullosa, mucous membrane pemphigoid, and several other esophageal disorders (ie, motility disorders).3,13
In the present case, clinical and laboratory parameters helped us exclude iron-deficiency anemia, PVs and celiac disease. In addition, computed tomography ruled out any possible causes of dysphagia such as esophageal tumors or extrinsic compression of esophagus. Barium swallow esophagram played an important role in diagnosing cervical esophageal webs. Thus, our case emphases the idiopathic etiology of esophageal webs.
The therapeutic method of choice in patients with esophageal webs and dysphagia remains endoscopic balloon dilation, a safe procedure and generally without any risk of web recurrence.1 Our patient was successfully treated with a single session of balloon dilation and remained asymptomatic for more than two years.
Conclusion
Esophageal web is usually seen in women and is rarely documented in males. The pathogenesis and treatment of esophageal webs are expanding. Most of these structural lesions are asymptomatic but can cause dysphagia which requires therapy (commonly endoscopic balloon dilation).
Ethics and Consent Statement
Our institution does not require ethical approval for reporting individual cases or case series (<10 patients).
Consent for Publication
Our patient gave his informed consent regarding publishing personal data in accordance with the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to acquisition of data, or analysis, conception and design, and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. All authors have read and agreed to the published version of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smith MS. Diagnosis and management of esophageal rings and webs. Gastroenterol Hepatol. 2010;6(11):701–704.
2. Hoffman RM, Jaffe PE. Plummer-Vinson syndrome. A case report and literature review. Arch Intern Med. 1995;155:2008–2011. doi:10.1001/archinte.155.18.2008
3. Schoepfer AM, Safroneeva E, Bussmann C, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013;145(6):
4. Guadagnolo BA, Haddad RI, Posner MR, et al. Organ preservation and treatment toxicity with induction chemotherapy followed by radiation therapy or chemoradiation for advanced laryngeal cancer. Am J Clin Oncol. 2005;28(4):371–378. doi:10.1097/01.coc.0000162423.13431.8d
5. Abdel-Wahab M, Abitbol A, Lewin A, et al. Quality-of-life assessment after hyperfractionated radiation therapy and 5-fluorouracil, cisplatin, and paclitaxel (Taxol) in inoperable and/or unresectable head and neck squamous cell carcinoma. Am J Clin Oncol. 2005;28(4):359–366. doi:10.1097/01.coc.0000158837.47450.81
6. Lawson JD, Otto K, Grist W, et al. Frequency of esophageal stenosis after simultaneous modulated accelerated radiation therapy and chemotherapy for head and neck cancer. Am J Otolaryngol. 2008;29(1):13–19. doi:10.1016/j.amjoto.2006.12.002
7. Smith CD. Esophageal strictures and diverticula. Surg Clin North Am. 2015;95(3):669–681. doi:10.1016/j.suc.2015.02.017
8. Ruigómez A, García Rodríguez LA, Wallander MA, et al. Esophageal stricture: incidence, treatment patterns, and recurrence rate. Am J Gastroenterol. 2006;101(12):2685–2692. doi:10.1111/j.1572-0241.2006.00828.x
9. Schatzki R, Gary JE. Dysphagia due to a diaphragm-like localized narrowing in the lower esophagus (lower esophageal ring). Am J Roentgenol Radium Ther Nucl Med. 1953;70(6):911–922.
10. von Rahden BH, Stein HJ, Becker K, et al. Heterotopic gastric mucosa of the esophagus: literature-review and proposal of a clinicopathologic classification. Am J Gastroenterol. 2004;99(3):543–551. doi:10.1111/j.1572-0241.2004.04082.x
11. Sheehan NJ. Dysphagia and other manifestations of oesophageal involvement in the musculoskeletal diseases. Rheumatology (Oxford). 2008;47(6):746–752. doi:10.1093/rheumatology/ken029
12. Kelly AB. Spasm at the entrance to the oesophagus. Proc R Soc Med. 1919;12(LaryngolSect):235.
13. Okamura H, Tsutsumi S, Inaki S, et al. Esophageal web in Plummer-Vinson syndrome. Laryngoscope. 1988;98(9):994–998. doi:10.1288/00005537-198809000-00014
14. Barbosa Ldo N, Silva RS, Verardino GC, et al. Mucous membrane pemphigoid with severe esophageal stricture. An Bras Dermatol. 2011;86(3):565–568. doi:10.1590/s0365-05962011000300023
15. O’Rourke A. Benign esophageal webs and strictures. Compr Manage Swallowing Disord. 2016;305.
16. Fuentes S, Cano I, Benavent MI, et al. Severe esophageal injuries caused by accidental button battery ingestion in children. J Emerg Trauma Shock. 2014;7(4):316–321. doi:10.4103/0974-2700.142773
17. Broor SL, Lahoti D, Bose PP, et al. Benign esophageal strictures in children and adolescents: etiology, clinical profile, and results of endoscopic dilation. Gastrointest Endosc. 1996;43(5):474–477. doi:10.1016/s0016-5107(96)70289-4
18. Honkoop P, Siersema PD, Tilanus HW, et al. Benign anastomotic strictures after transhiatal esophagectomy and cervical esophagogastrostomy: risk factors and management. J Thorac Cardiovasc Surg. 1996;111(6):
19. Pierie JP, de Graaf PW, Poen H, et al. Incidence and management of benign anastomotic stricture after cervical oesophagogastrostomy. Br J Surg. 1993;80(4):471–474. doi:10.1002/bjs.1800800422
20. Funakawa K, Uto H, Sasaki F, et al. Effect of endoscopic submucosal dissection for superficial esophageal neoplasms and risk factors for postoperative stricture. Medicine (Baltimore). 2015;94(1):e373. doi:10.1097/MD.0000000000000373
21. Murphy SG, Yazbeck S, Russo P. Isolated congenital esophageal stenosis. J Pediatr Surg. 1995;30(8):1238–1241. doi:10.1016/0022-3468(95)90032-2
22. Bluestone CD, Kerry R, Sieber WK. Congenital esophageal stenosis. Laryngoscope. 1969;79(6):1095–1103. doi:10.1288/00005537-196906000-00004
23. Goel A, Bakshi SS, Soni N, et al. Iron deficiency anemia and Plummer-Vinson syndrome: current insights. J Blood Med. 2017;8:175–184. doi:10.2147/JBM.S127801
24. Hefaiedh R, Boutreaa Y, Ouakaa-Kchaou A, et al. Plummer Vinson syndrome association with coeliac disease. Arab J Gastroenterol. 2013;14(4):183–185. doi:10.1016/j.ajg.2013.10.003
25. Tahara T, Shibata T, Okubo M, et al. A case of Plummer-Vinson syndrome showing rapid improvement of dysphagia and esophageal web after two weeks of iron therapy. Case Rep Gastroenterol. 2014;8(2):211–215. doi:10.1159/000364820
26. Dutta U, Khaliq A, Talha Noor M, et al. Recurrent multiple cervical esophageal webs: an unusual presentation of celiac disease. Gastroenterology Res. 2009;2(6):356–357. doi:10.4021/gr2009.12.1325
27. Sinha SK, Nain CK, Udawat HP, et al. Cervical esophageal web and celiac disease. J Gastroenterol Hepatol. 2008;23:1149–1152. doi:10.1111/j.1440-1746.2008.05452.x
28. Syn WK, Ahmed MM. Esophageal involvement in cicatricial pemphigoid: a rare cause of dysphagia. Dis Esophagus. 2004;17:180–182. doi:10.1111/j.1442-2050.2004.00398.x
29. Fox LP, Lightdale CJ, Grossman ME. Lichen planus of the esophagus: what dermatologists need to know. J Am Acad Dermatol. 2011;65:175–183. doi:10.1016/j.jaad.2010.03.029
30. Djuric Z, Nagorni A, Zivanovic D. Esophagitis and almost complete esophageal occlusion in a girl with epidermolysis bullosa. Turk J Pediatr. 2012;54:301–304. doi:10.2214/AJR.16.16115
31. Watari T, Nagano T, Takinami Y. Graft-versus-host disease – induced esophageal web. J Gen Fam Med. 2019;20:33–34. doi:10.1002/jgf2.215
32. Trabulo D, Ferreira S, Lage P, et al. Esophageal stenosis with sloughing esophagitis: a curious manifestation of graft-vs-host disease. World J Gastroenterol. 2015;21:9217–9222. doi:10.3748/wjg.v21.i30.9217
33. Halland M, Baron TS, Ravi K. Dysphagia in a patient with a Zenker´s diverticulum: there is more to it than meets the eye. Gastroenterology. 2014;146:590–591. doi:10.1053/j.gastro.2013.09.051.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.