")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Identifying Needs and Barriers to Diabetes Dietary Education in Chinese People with Type 2 Diabetes and Their Family Members in Guangzhou: A Qualitative Study
Authors Hu X , Zhang Y, Yao B, Lin B, Yang D, Ling C, Gao L
Received 5 July 2021
Accepted for publication 28 August 2021
Published 15 September 2021 Volume 2021:14 Pages 4005—4014
DOI https://doi.org/10.2147/DMSO.S327988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Xiling Hu,1,* Yao Zhang,2,* Bin Yao,2 Beisi Lin,2 Dan Yang,3 Cong Ling,4,* Lingling Gao3,*
1Department of Medicine, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Endocrinology and Metabolism, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 3School of Nursing, Sun Yat-sen University, Guangzhou, People’s Republic of China; 4Department of Neurosurgery, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Cong Ling
Department of Neurosurgery, The Third Affiliated Hospital of Sun Yat-sen University, No. 600 Tianhe Road, Guangzhou, Guangdong, 510630, People’s Republic of China
Tel +86-13580465121
Email [email protected]
Lingling Gao
School of Nursing, Sun Yat-sen University, No. 74, Zhongshan Er Road, Guangzhou, Guangdong, 510085, People’s Republic of China
Tel +86 13539965693
Email [email protected]
Purpose: The purpose of this exploratory qualitative study was to identify the needs and barriers to diabetes dietary education issues in a Chinese context among people with type 2 diabetes and also their family members.
Patients and Methods: Nineteen patients with type 2 diabetes and 15 family members were randomly selected from a larger study in Guangzhou. Descriptive phenomenological qualitative inquiry guided this study.
Results: Both patients and their family members claimed a variety of needs regarding diabetes dietary information and that it should be patient-centered. In addition, both groups identified the effectiveness and helpfulness of diabetes diet-related health education, but family members reported a lack of professional education. Patients reported that the barriers to diabetes diet-related health education were: 1) patients’ different faculties of memory and acceptance, 2) educators’ methods of explaining the information, 3) lack of advertising and intensity of publicity both inside and outside of the hospital. Family members identified that diabetes diet-related health education assisted them with taking care of patients with diabetes and it was also beneficial for themselves to gain more dietary knowledge and develop healthy dietary habits.
Conclusion: It is necessary to make some adjustment to traditional diabetes dietary education. It may be a good strategy to investigate the needs and faculties of memory and acceptance of people with diabetes before starting a diabetes education program. Hospitals should intensify their publicity of diabetes education and make it more attractive to patients with diabetes and their family members. Educators should add information specifically for family members while conducting diabetes education. Tertiary hospitals could provide standardized training regarding diabetes-related health education to community family physicians; in this way, diabetes education could gradually be transferred to them and both groups of clinicians could share in the education.
Keywords: diabetes, family members, dietary education, needs, barriers, qualitative
Introduction
Diabetes is among the top 10 causes of death in adults; it is a serious long-term condition with poor control leading to several wide-ranging complications and impacts on all aspects of a person’s quality of life, families, and societies worldwide. The incidence of diabetes has increased dramatically over the past decades1 and the International Diabetes Federation (IDF) estimates that a total of 463 million people are living with the disease; this number is expected to increase to 578 million in 2030 and 700 million in 2045.2 China, with 116 million cases, had the highest number of people living with diabetes in 2019, and it is estimated that China will still hold this position in 2030 and 2045. More than 90% of adults with diabetes have type 2 diabetes mellitus (T2DM), which is correlated with increased age, body weight, lifestyle disorders, and family history. It is, therefore, imperative for China to develop and improve the implementation of optimal diabetes management strategies.1
Diabetes dietary self-management education has long been considered a cornerstone of an integral diabetes therapy regimen.3 Health education comprises a set of planned activities that aim to improve people’s knowledge and skills and also help them to take responsibility for maintaining their health, improving engagement in healthy behaviors, and promoting changes in attitudes and perceptions about disease to facilitate adjustments to new situations of daily living.4 Previous meta-analyses of diabetes self-management show that HbA1c reductions ranged from 0.44–0.76% in the general population.5,6 However, other studies confirm that there are still knowledge deficits regarding the diabetic diet among Chinese adults with diabetes.7–9 Furthermore, education regarding diabetes was sometimes not authentic, feasible, or professional, thus contributing to low effectiveness.8,10,11 In Germany, 30–50% of patients do not participate in diabetes education even though it is fully compensated by the German statutory health insurance.12 Similar problems with education attendance are also reported in the United States; ie, that only one third to one half of US patients with diabetes receive diabetes self-management education.13
On the other hand, family members have been increasingly recognized to have an important role in the dietary management of relatives with diabetes and some patients prefer assistance from family members, especially for diet management.16 Some previous studies suggest that the implementation of interventions regarding diabetes information for both patients and their families is helpful in promoting self-care behaviors, following medical diets, decreasing emotional stress, coping with changes in life, enhancing self-efficacy, reducing the frequency of hospitalization, achieving weight loss, better controlling blood sugar levels, and ultimately improving quality of life.14,16 Currently, most diabetes dietary education programs do not include their family members, moreover, most Chinese households traditionally comprise two to three generations. Nevertheless, few studies have assessed family members’ needs and barriers to their diabetes dietary education. Therefore, identifying the underlying needs and barriers to diabetes dietary education among both individuals with diabetes and their family members is considered as an essential element for ameliorating and innovating diabetes dietary education strategies to help improve overall medical outcomes.14–16
Traditional quantitative methods are inappropriate to address questions related to a situation, however, qualitative research studies provide important insights into health-related phenomenon.12 Qualitative research including interviews are valuable complements to quantitative research, helping us to understand individuals and to focus on their thoughts and experiences.17 The purpose of this exploratory qualitative study was to identify the needs and barriers to diabetes dietary education issues in a Chinese context among individuals with type 2 diabetes and their family members.
Methods
We conducted a qualitative study based on semi-structured interviews during which a set of guidelines containing open questions and topics of needs and barriers to diabetes dietary information and education were raised. Nineteen patients with type 2 diabetes and 15 family members were randomly selected from a larger study focusing on dietary information, behavior, and practices among hospitalized people with type 2 diabetes and their family members in a leading tertiary hospital in Guangzhou from September 2018 to February 2019. Results of the large study have been published as
Dietary Knowledge, Attitude and Practice (KAP) Among the Family Members of Patients with Type 2 Diabetes Mellitus (T2DM) and Its Influence on the KAP of T2DM Patients.
Approval for the study was granted by the Ethics Committee of our hospital. The purpose of this study was explained to participants, with an assurance that participants’ treatment in the hospital would not be affected.
Selection criteria for patients included: diagnosed with type 2 diabetes according to the definition put forward by the World Health Organization (WHO) in 1999; age ≥18 years, illness duration ≥ 3 months; having basic literacy, able to read and understand questions; willing to participate in the study; and provided voluntary informed consent. Exclusion criteria were: diabetes in pregnancy; manage his/her diet totally by himself/herself; not able to complete the survey owing to psychological or physical disorders like acute complications of diabetes and serious heart, brain, lung, kidney illnesses; refused to participate and would not sign the informed consent form; and were ineligible due to other conditions as assessed by the associated researchers.
Selection criteria for family members included: age ≥18 years; designated by the individual with type 2 diabetes; having a major influence on the patient’s diet, including the patient’s spouse, parents, adult children, siblings, or other relatives. Exclusion criteria were: having diabetes of any type; not able to complete the survey owing to psychological disorders or serious heart, brain, lung, kidney, and other illnesses; refused to participate and would not sign the informed consent form.
We arranged the interview times in hospital with each interviewee and sought permission for audio recording and written recording before the in-depth interview took place. In the formal interview, a semi-structured outline (see Appendix) was used; the interview was conducted by two trained researchers and lasted between 30 and 60 min. During recording, suggestive nonverbal behaviors, key words, and temporary comments of the interviewees were briefly recorded. Audio recordings were transcribed verbatim into text data within 48 hours after the interview. Written records were sorted and inserted into transcribed text data, making the interview data as complete as possible.
Content analysis was used to analyze the interview data including designing the classification outline, coding, and refining the topic. The main steps were: (i) read and understand the transcribed data repeatedly, and form a preliminary classification outline in combination with the direction of this study; (ii) open coding: mark key words and sentences for meaningful paragraphs; (iii) axial coding: compare markup content repeatedly, synthesize and generalize, and construct the main concepts; (iv) selective coding: compare the constructed concept with the markup content again, and then present it as one unit with structural meaning; (v) repeatedly analyze and verify the relationships between the code and integrate them into topics; (VI) elaborate the connotation of the theme in combination with written materials.
Results
The sociodemographic characteristics of people with type 2 diabetes and their family members are shown in Tables 1 and 2, respectively.
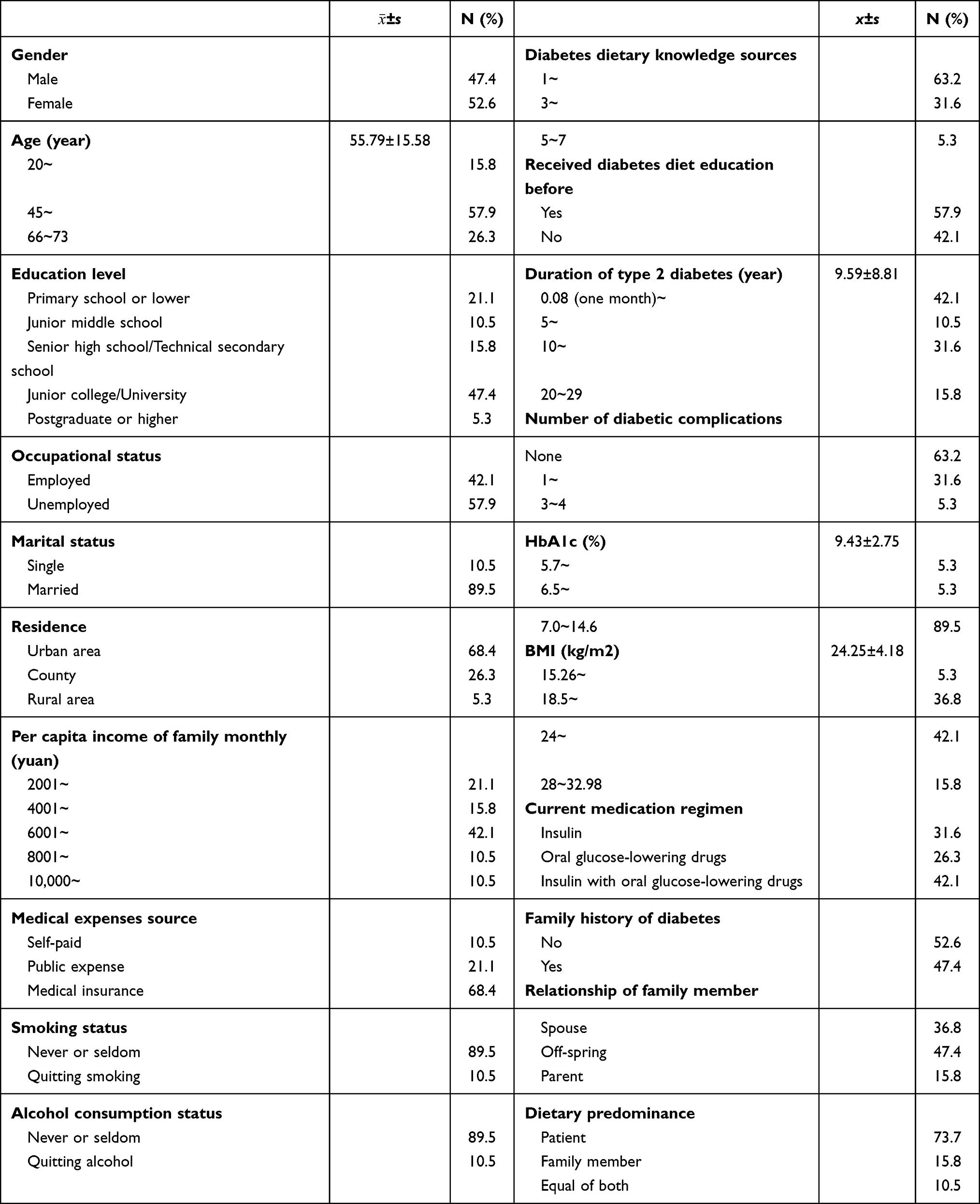 |
Table 1 Sociodemographic and Disease-Related Characteristics of People with Type 2 Diabetes (n=19) |
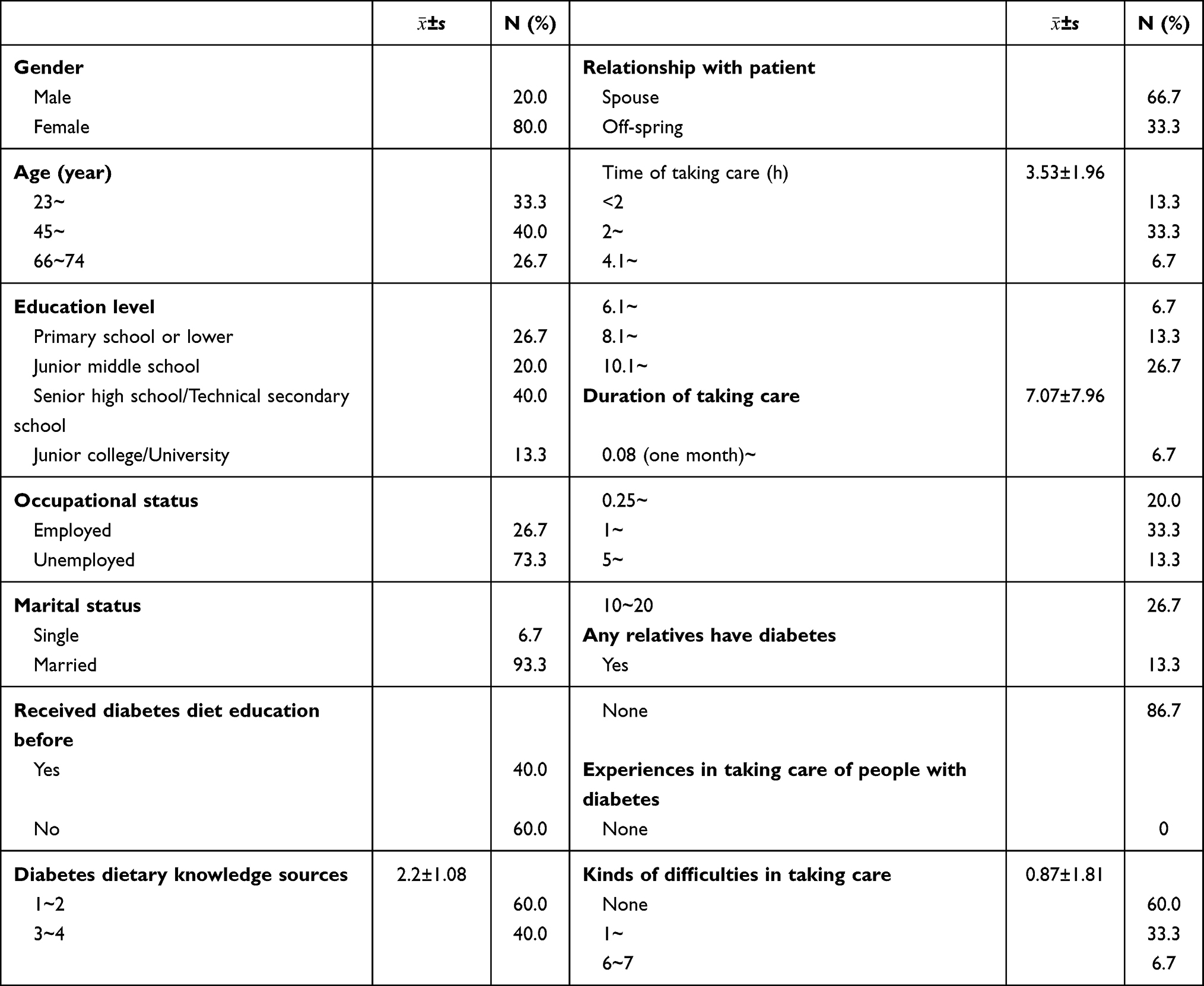 |
Table 2 Sociodemographic and Care-Related Characteristics of Family Members (n=15) |
Results of interviews were analyzed into four themes for patients and three themes for family members, which are shown in Table 3.
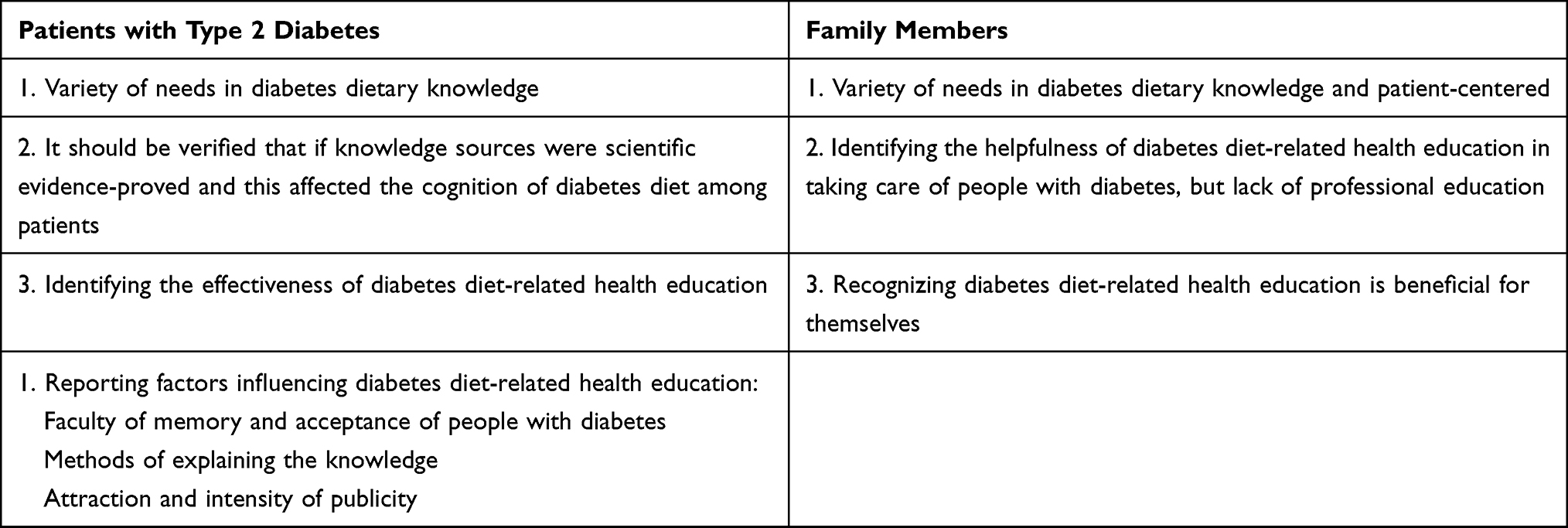 |
Table 3 Themes and Categories of Needs and Barriers to Diabetes Dietary Education |
Patients with Type 2 Diabetes
There Were a Variety of Needs for Diabetes Dietary Information
In general, type 2 diabetes patients had more questions about the diabetes dietary information and different patients had different needs. Patients with short diabetes duration needed more as well as a wider range of information than those with long duration. Patients with long diabetes duration or who were previously well informed preferred dietary information targeted at diabetic individuals as well as information that was adaptable for routine practice. Patients also paid great attention to dietary information for health reasons, for taking control of bad food preferences, and for easily converting dietary information into practical dietary behaviors.
Patient 4 There is one question I still can’t figure out: that if my blood sugar is high due to eating too much today can I balance it with eating less food tomorrow?
Patient 5 My husband said I cannot eat rice porridge, sweet potato, and taro, but these are my favorites, so is it true that I cannot eat just a little of them? About an egg, which part is better for me to eat? Yolk or albumin? Also, why can I eat oatmeal despite it being a thin liquid similar to rice porridge?
Patient 10 I am still confused about what we diabetic patients can eat and what we cannot. Is it true that beef is better than pork for us? Then how about seafood or sweet potato? I was told that eating lean meat is better than eating rice; is it true? Can you give me some suggestions on how to choose rice and oil? Can you give me some recommendations in detail; for example, what are the best foods for us to eat and how much we can eat? I am still not clear about these.
Patients Suggested That Sources of Information Should Be Based on Proven Scientific Evidence and This Affected Their Interpretation of a Diabetic Diet
Even though diabetes-related education plays an important role in the prevention and treatment of diabetes, insufficient attention was given by some patients to the scientific basis and professionalism of education. The main sources of diabetes diet information were from relatives, friends, and network media such as television and the official WeChat account owing to easy access; furthermore, some patients believed and followed such information without questioning its authenticity.
Patient 19 I read the newspaper every day, and one day it said that diabetics should not eat tomato because it contains sugar, then I stopped. Actually, I don’t know what I should eat and should not. I hear things about the diabetic diet from my daughter-in-law whose mom also has diabetes; she told me that she obtained the information from her mom.
Patient 18 I watched some short videos about diabetes diets on WeChat and other apps on my phone. They can tell you what you can eat and what you should not eat.
Patient 17 I don’t know much, and also feel confused about dietary information; I followed information from the television. One elderly relative told me that pumpkin was good for people with diabetes and brought some to my home, so I cooked and ate them.
Patient 15 I can get lots of diabetes dietary information from Baidu, so I get all the information I need from Internet……
Identification of the Effectiveness of Diabetes Diet-Related Health Education
Patients with type 2 diabetes identified that diabetes diet-related health education could definitely assist them in controlling their diet, which played a guiding role in both the general direction of the diabetic diet and also in the specific choice of foods. Systematic diabetes dietary education in hospital standardizes patients’ routine dietary management, and enhances patients’ confidence in diet control; this has become the most reliable information source. However, some patients who already have a good grounding in diabetic diets tend to think they will not obtain more information from general diabetes dietary education.
Patient 17 I think the diabetes dietary education courses in this hospital are really good. There are no similar courses in our county and community. Of course, I would like to attend diabetes education courses, but I don’t have access to them in the city where I live. Before taking courses here, I had some knowledge of diabetic diets but was confused. Now standardized learning has clarified my thoughts about the diabetic diet; for example, I know I can eat more food by limiting the amounts of some types of food.
Patient 9 The greatest outcome of diabetes dietary education courses for me is that I have much more confidence in keeping my blood sugar stable.
Patient 4 Information obtained in hospital education classes by professional specialists and educated nurses is based on robust scientific data and thus more reliable. It is like you can see the whole forest not only one tree.
Patient 8 I feel what I was taught in hospital was almost similar to what I already knew because I was a teacher before and now I spend most of my retirement time reading about diabetes.
Patients Report Factors Influencing Diabetes Diet-Related Health Education
Type 2 diabetes patients can indeed obtain effective and helpful information for diabetes diet-related health education; however, conventional large-group classes cannot completely fulfill different patients’ needs; moreover, patients who have poor memories and acceptance learn less. The lack of publicity regarding diabetes-related health education outside of the hospital also impedes their development.
Patient 9 I can clearly remember the diabetes dietary information immediately after taking courses, but after a while I forget again……
Patient 19 It is better to give us some written information or booklets with the content of the course so we can check things we didn’t understand in the class and also review what we learnt. I didn’t know where to learn about diabetes diets as there were no such education classes in the community. I think you should increase the intensity of publicity outside of hospitals to inform more patients with diabetes. I think you should go to communities and housing estates to give lessons on diabetes and appropriate diets because many people do not understand this disease.
Another important factor influencing diabetes diet-related health education is that explanations of information cannot completely meet patients’ characteristics and their needs; for example, they are not concise and explicit, there is a lack of individuation, there is not enough time for interaction.
Patient 9 In my opinion, you can make a list of different food categories such veggies, fruits, and meat and list suitable amounts for patients with diabetes. You can make detailed recipes for us to comply with every day.
Patient 14 I suggest you can tell us what we should eat directly like broccoli, celery, cucumber instead of teaching us every food constituent that we easily forget.
Patient 6 I prefer the one-to-one model of diabetes education as the content is more detailed and I can also ask some questions as well. What’s more, it would be better if you can teach us how to prepare diabetic food.
Patient 8 I suggest there should be some question time in the education classes. The teachers left immediately after each class as they were so busy with their medical work; however, many patients have questions to ask. Most of us need some interaction time in or after class.
Insufficient attention to patients with diabetes is another barrier to diabetes-related education.
Patient 7 There is one issue you should address: that some patients do not accept diabetic education. You should find new ways to attract more patients with diabetes to receive the education.
Family Members
There is a Variety of Needs for Diabetic Dietary Knowledge and Patient-Centered Education
Likewise, family members of people with type 2 diabetes had lots of questions about the diabetic diet. Family members who have less experience in taking care of patients needed more as well as a wider range of information, while experienced family members preferred dietary information more adaptable to routine diet practice and had questions regarding taking practical dietary care of diabetic patients. Family members also paid close attention to balancing food intake to prevent hunger, how to adjust the diet when the patient’s blood glucose was abnormal, and existing difficulties in conversion from dietary information to dietary practice.
Family member 1 Making breakfast is a problem for me as I always make noodles for him to eat for breakfast. Sometimes I make some sweet potatoes or two steamed buns and one egg, but it seems like not enough for him as he feels hungry to the extent of showing hypoglycemic symptoms before lunch. He does not like milk and also is intolerant to it, although I know this is a good choice for a diabetic breakfast.
Family member 3 Can she drink wine? If he eats oatmeal as breakfast, and then eats a bowl or one and half bowls of rice at lunch, can he eat a bowl of rice again at dinner? Will eating a late-night snack affect his blood sugar or not? His blood sugar was 8.2 mmol/L, and then it was 14 mmol/L at over 2 hours after a meal. I was surprised that the blood sugar increased that much as it seemed like he didn’t eat a lot.
Family member 7 You should tell him what as well as how much he should eat and what he should not eat when his blood sugar is high. Are there better diet management programs to help keep blood sugar stable? I think you should write some detailed articles to tell us how people with diabetes should eat; for example, for each type of food how much you should eat.
Family member 9 I know normally Guangdong pork rib soup (boiled for more than 1–2 hours) is not suitable for diabetic patients, but if they really need one kind of soup, what soup can you recommend for me? Then what about fruit? What kind of fruit is more suitable for diabetic patients? What about milk? Can they drink skimmed milk or low-fat milk?
Identifying the Helpfulness of Diabetes Diet-Related Health Education in Taking Care of People with Diabetes, but a Lack of Professional Education
Family members identified the helpfulness of receiving diet-related health education in taking care of patients. However, owing to the lack of resources and time, it is quite difficult for family members to receive professional diabetes-related education.
Family member 5 I make routine meals for him at home, so the diet education class was truly helpful for me. I know I should balance different kinds of food for him and include more veggies, less staple food, and also use less oil and salt while cooking.
Family member 3 I have not attended any diabetes education classes, but I search the Internet for information about the diabetic diet. We do not live in Guangzhou and there are no diabetic education classes in the city where we live. Of course, I would like to attend such education classes.
Family member 7 Before his hospitalization this time, I barely received any diet education because I don’t have spare time. I seldom gained diabetes dietary information on my own because I don’ t like reading or watching TV.
Family member 12 I don’t have spare time to receive diabetes education because I need to make money for our livelihood and her medication. I know it would benefit us if I could go to some professional diabetes diet classes, but I just cannot balance my time. In addition, there is no diabetes education in the place we live so it is impossible educate ourselves there.
Recognizing Diabetes Diet-Related Health Education is Beneficial for Themselves
Family members identified that diabetes diet-related health education can help them with taking care of diabetic patients; they also understood the benefit for themselves to gain more dietary information and develop healthy eating habits. It might help to popularize diabetes-related education among family members of patients with diabetes.
Family member 12 This kind of diabetes dietary education is beneficial to both patients and family members because normally we don’t really pay attention to what we eat. It is easy to buy some snacks to eat without being aware of the large amount of sugar they contain.
Family member 15 There should be dietary education for family members of people with diabetes regarding how to taking care of patients at home.
Discussion
Diabetes self-management dietary education has long been considered a cornerstone of an integral diabetes therapy regimen to assist individuals in achieving glycemic control. There is strong evidence that diabetes education therapy can help improve not only HbA1c but also blood pressure, weight, blood lipids, and overall health outcomes. Quantitative studies using standardized scales and questionnaires cannot explore the needs and barriers to the implementation of diabetic diets and education issues in people with type 2 diabetes and their family members; however, qualitative studies can explore issues in depth and identify new variables and patterns.18
There are indeed some qualitative studies regarding diabetes self-management. Susan et al describe and compare practices reported by patients in good, fair, and poor control to identify successful strategies associated with better glycemic control in patients with type 2 diabetes in a qualitative comparative study.18 Nagelkerk et al completed a qualitative study in which the most commonly reported barriers among patients with diabetes were lack of understanding of the overall plan of care and frustration from inadequate metabolic control and progressive disease despite compliance with the self-care recommendations.19,20 In a qualitative evaluation, Nicole Ide et al identify that patients’ knowledge and self-management behaviors, especially in terms of diet control and exercise, and also lack of social support, can be barriers to diabetes management in Nepal.21 However, there are few qualitative studies regarding the needs and barriers to diabetes dietary education among people with type 2 diabetes in China and also their family members. This qualitative study explored the needs and barriers to diabetes dietary education in people with type 2 diabetes and their family members using in-depth interviews.
People with type 2 diabetes identified the effectiveness of diabetes diet-related health education; at the same time, they mentioned different needs regarding diabetes dietary education. Deakin et al found that patient-centered, group-based self-management programs showed significant improvements in mean HbA1c, diabetes knowledge, fruit and vegetable intake, enjoyment of food, and treatment satisfaction.22 One study found that patients with a good state of health related to diabetes and those already having sufficient knowledge of diabetes do not participate in diabetic education.12 A systematic review found that the lack of specific details in South Asian tailored diabetic diets and social responsibilities associated with a traditional diet hinder people with diabetes from adopting a diabetic diet. It is necessary to modify diabetes dietary education strategies according to the different needs and requirements of people with diabetes. For instance, we can organize different education classes for retired or working patients, encouraging them to have more social meals with each other. It is important and more effective to separate them to receive specific diabetes dietary education based on their daily life, with the aim of attracting their attention and making it easier to apply to daily life. One barrier to diabetes education mentioned by patients was their different faculties of memory and acceptance, which should be taken into consideration when creating education classes. It may be a good strategy to ask people with diabetes to complete a questionnaire before accepting education to ensure that they receive classes according to their needs. Group diabetes dietary education may be another helpful way to adopted peer support, as individuals can encourage each other and promote perseverance. More research is also needed to compare traditional and new strategies.
A study of more than 5000 adults with diabetes highlights the importance of family, friends, and colleagues in improving well-being and self-management.23 Likewise, a recent study concludes that perceiving family members to be non-supportive is associated with a lower adherence to medication in people with diabetes.14 One systematic review found that the number of trials and statistically significant results in family interventions targeting adults with diabetes is limited; furthermore it is difficult to come to a conclusion on effective approaches in family interventions, though psychosocial and familial dimensions seem sensitive to family-based interventions.9 In the current study, family members of people with diabetes identified the helpfulness of diabetes diet-related health education, but identified a lack of professional education. It is necessary to make some diabetes education classes specifically for family members of patients with diabetes as they can then provide emotional and psychological support to patients and help with behavior change resulting in promoting diabetes self-management. The inclusion of family members in educational interventions may help in the development of healthy family behaviors as they recognized diabetes education is also beneficial to themselves.
We found that lack of sufficient interaction time with educators was a major problem influencing patients’ learning, understanding, and application to routine diet management, which is in agreement with previous studies. One study in Western countries found that patients thought allied healthcare workers were better able to understand their needs and concerns since they had more time available instead of the limited time with a clinician.15,24 Patients in India found it easier to access their family physician versus dietitians, and were highly likely to follow a suggested diet plan.15,25 In Nepal, community- and mid-level health facilities are often ill equipped to provide screening and treatment services for diabetes, thus forcing patients to attend less accessible, higher-level health facilities. Hence one method gaining attention in a growing number of low-resource settings is the use of community-based programs to supplement hospital-based services for chronic diseases such as diabetes. Community-based programs can advance health promotion, improve diabetes awareness and support diabetes patients with their on-going self-management.21 China has been constructing a new community family physician model to address unmet needs in the long-term management of chronic illnesses and relieve the growing burden of patient visits to overloaded physicians in large-scale hospitals; this format can also be applied to diabetes education. Tertiary hospitals could provide standardized training on diabetes related health education to community family physicians, who could then spread the diabetes education or at least both groups of clinicians could share education work. At the same time, owing to greater interaction between patients with diabetes and family physicians, patients learn about diabetes and also build more trust in their educators which accordingly improves patients’ compliance with diet recommendations.
Limitations
This study had a few limitations. Firstly, the study was conducted on hospitalized patients and their family members in a single center; outpatients were not involved in the study. Therefore, the findings may give some directions in diabetic dietary education in hospital, but may not be generalizable to outpatients or even the entire country. Secondly, our sample was not sufficiently large to conclusively determine the needs and barriers of all Chinese patients with diabetes and their family members. We hope to enlarge the sample and include more patients in further research to establish more needs and barriers regarding diabetic diet and education to help improve diabetes-related education in China.
Conclusion
It is necessary to make some adjustments to traditional diabetes dietary education. It may be a good strategy to ask people with diabetes to complete some questionnaires before accepting education and to organize classes based on their needs and faculties of memory and acceptance. The hospitals should intensify their publicity of diabetes education and make it more attractive to patients with diabetes and their family members. Educators should add information specific for family members of people with diabetes while conducting diabetes education. Tertiary hospitals could provide standardized training on diabetes-related health education to community family physicians; such information could gradually be transferred on to patients, or at least both groups of clinicians could share the education work.
Ethics Approval and Informed Consent
We confirm that this study was conducted in accordance with the Declaration of Helsinki. The study was approved by the ethics committee of the Third Affiliated Hospital of Sun Yat-sen University ([2019]02-565-01). All participants signed informed consent before they participated.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vanstone M, Rewegan A, Brundisini F, Giacomini M, Kandasamy S, DeJean D. Diet modification challenges faced by marginalized and nonmarginalized adults with type 2 diabetes: a systematic review and qualitative meta-synthesis. Chronic Illn. 2017;13(3):217–235. doi:10.1177/1742395316675024
2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th)edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
3. Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials. Diabetes Care. 2001;24(3):561–587. doi:10.2337/diacare.24.3.561
4. Gomes LC, Coelho A, Gomides D, Foss-Freitas MC, Foss MC, Pace AE. Contribution of family social support to the metabolic control of people with diabetes mellitus: a randomized controlled clinical trial. Appl Nurs Res. 2017;36:68–76. doi:10.1016/j.apnr.2017.05.009
5. Steinsbekk A, Rygg LØ, Lisulo M, Rise MB, Fretheim A. Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Serv Res. 2012;12:213. doi:10.1186/1472-6963-12-213
6. Norris SL, Lau J, Smith SJ, Schmid CH, Engelgau MM. Self-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care. 2002;25(7):1159–1171. doi:10.2337/diacare.25.7.1159
7. Chen J, Jing X, Liu X, et al. Assessment of factors affecting diabetes management in the City Changing Diabetes (CCD) study in Tianjin. PLoS One. 2019;14(2):e209222.
8. Wang H, Song Z, Ba Y, Zhu L, Wen Y. Nutritional and eating education improves knowledge and practice of patients with type 2 diabetes concerning dietary intake and blood glucose control in an outlying city of China. Public Health Nutr. 2014;17(10):2351–2358. doi:10.1017/S1368980013002735
9. Torenholt R, Schwennesen N, Willaing I. Lost in translation–the role of family in interventions among adults with diabetes: a systematic review. Diabet Med. 2014;31(1):15–23. doi:10.1111/dme.12290
10. Li Z, Jin H, Chen W, et al. Influencing factors of knowledge, attitude, and practice regarding medical nutrition therapy in patients with diabetes: a National Cross-Sectional Study in Urban China. J Diabetes Res. 2017;2017:8948452. doi:10.1155/2017/8948452
11. Jing LL, Chen W, Sun ZL, et al. Investigation into knowledge, attitude, and practice regarding medical nutrition therapy among patients with diabetes in China: results from a national multicenter cross-sectional study. J Diabetes. 2017;9(9):865–873. doi:10.1111/1753-0407.12500
12. Schäfer I, Pawels M, Küver C, et al. Strategies for improving participation in diabetes education. A qualitative study. PLoS One. 2014;9(4):e95035. doi:10.1371/journal.pone.0095035
13. Ruppert K, Uhler A, Siminerio L. Examining patient risk factors, comorbid conditions, participation, and physician referrals to a rural diabetes self-management education program. Diabetes Educ. 2010;36(4):603–612. doi:10.1177/0145721710369705
14. Baig AA, Benitez A, Quinn MT, Burnet DL. Family interventions to improve diabetes outcomes for adults. Ann N Y Acad Sci. 2015;1353(1):89–112. doi:10.1111/nyas.12844
15. Ebrahimi H, Ashrafi Z, Rudsari DM, Parsayekta Z, Haghani H. Effect of family-based education on the quality of life of persons with type 2 diabetes: a Randomized Clinical Trial. J Nurs Res. 2018;26(2):97–103. doi:10.1097/jnr.0000000000000212
16. Mayberry LS, Osborn CY. Family support, medication adherence, and glycemic control among adults with type 2 diabetes. Diabetes Care. 2012;35(6):1239–1245. doi:10.2337/dc11-2103
17. Sohal T, Sohal P, King-Shier KM, Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a Systematic Review. PLoS One. 2015;10(9):e136202. doi:10.1371/journal.pone.0136202
18. K Malterud. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. doi:10.1016/S0140-6736(01)05627-6
19. Susan C Weller SC, Baer R, Nash A, Perez. Discovering successful strategies for diabetic self-management: a qualitative comparative study. BMJ Open Diabetes Res Care. 2017;5(1):e349. doi:10.1136/bmjdrc-2016-000349
20. Rebecca Mathew, Enza Gucciardi, Margaret De Melo and Paula Barata P. Self-management experiences among men and women with type 2 diabetes mellitus: a qualitative analysis. BMC Fam Pract. 2012;13:122. doi:10.1186/1471-2296-13-122
21. Jean Nagelkerk, Kay Reick, Leona Meengs. Perceived barriers and effective strategies to diabetes self-management. J Adv Nurs. 2006;54(2):151–158. doi:10.1111/j.1365-2648.2006.03799.x
22. Nicole Ide, James P LoGerfo and Biraj Karmacharya. Barriers and facilitators of diabetes services in Nepal: a qualitative evaluation. Health Policy Plan. 2018;33(4):474–482. doi:10.1093/heapol/czy011
23. Deakin TA, Cade JE, Williams R, Greenwood DC. Structured patient education: the diabetes X-PERT Programme makes a difference. Diabet Med. 2006;23(9):944–954. doi:10.1111/j.1464-5491.2006.01906.x
24. Rhodes P, Nocon A. A problem of communication? Diabetes care among Bangladeshi people in Bradford. Health Soc Care Community. 2003;11(1):45–54. doi:10.1046/j.1365-2524.2003.00398.x
25. Patel M, Patel IM, Patel YM, Rathi SK. Factors associated with consumption of diabetic diet among type 2 diabetic subjects from Ahmedabad, Western India. J Health Popul Nutr. 2012;30(4):447–455.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.