")
Back to Journals » Research Reports in Clinical Cardiology » Volume 9
Hypothesis-generating study on the effect of the ACLS guidelines on the use of atropine in cardiac arrest at a community hospital
Authors Kwok MMK , Stenstrom R, Mak E, Cheung KW
Received 5 March 2018
Accepted for publication 31 May 2018
Published 8 August 2018 Volume 2018:9 Pages 23—25
DOI https://doi.org/10.2147/RRCC.S167289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Kones
Video abstract presented by Matthew Kwok
Views: 6693
Matthew Mo Kin Kwok,1,2 Rob Stenstrom,1 Edward Mak,2 Ka Wai Cheung1
1Department of Emergency Medicine, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada; 2Emergency Department, Richmond Hospital, Vancouver Coastal Health, Richmond, BC, Canada
Background: Barriers exist in translating clinical practice guidelines into medical management of patients. These barriers result in delay in translating the Advanced Cardiac Life Support (ACLS) guidelines into clinical practice. We conducted a pilot study employing the recommendation change in atropine usage in the 2010 ACLS guideline algorithm to examine the time lag in translating guidelines into medical practice.
Methods and results: We completed a retrospective chart review at a community hospital. Study data was derived from cardiac arrest records from the emergency department between January 1, 2009 and December 31, 2013, before and after the publication of the 2010 ACLS guidelines. All cardiac arrests in the form of asystole and/or pulseless electrical activity at some time during resuscitation in patients aged 19 years and older were included in the study. We examined whether atropine was used during the resuscitation. We studied the use of epinephrine as a control. A time versus atropine and a time versus epinephrine usage graphs were generated and examined. Fifty-five resuscitations met inclusion criteria. Although the 2010 ACLS guidelines were first presented in October 2010, we observed that change in atropine use occurred around the summer of 2011. There was no change in the use of epinephrine.
Conclusion: Despite several guideline dissemination strategies, a time lag was found in physicians’ adaptation of the ACLS guidelines.
Keywords: cardiopulmonary resuscitations, resuscitations, Advanced Cardiac Life Support, guidelines translation, guidelines dissemination
Background
The purpose of clinical practice guidelines is to guide physicians in making appropriate decisions in specific clinical circumstances. Their successful implementation should translate research into effective practices and thus improve patient outcomes.1 In particular, the American Heart Association has introduced the Advanced Cardiac Life Support (ACLS) guidelines to improve cardiac arrest quality of care.2 Physicians have to be aware of and utilize these guidelines in order to benefit patients and improve outcomes.
The American Heart Association introduced the ACLS guidelines in 2010. In this update, atropine was removed from the asystole and pulseless electrical activity (PEA) cardiac arrest algorithms.3 Several potential barriers have been identified in physicians’ uptake of the ACLS guidelines.3 These barriers result in delay in translating ACLS guidelines into clinical practice.4–6 The time delay in physicians’ uptake of ACLS guidelines has not been examined, and the time lag in changing medical management after the publication of the guidelines has not been quantified. We conducted a study employing the recommendation change in atropine usage in the ACLS guideline algorithm to examine the time lag in translating guidelines into medical practice.
Methods
We conducted a retrospective chart review at a community hospital after receiving ethics approval from the University of British Columbia Clinical Research Ethics Board. As this is a retrospective observational study meeting the institutional minimal risk standard, consent was not obtained. Study data was derived from cardiac arrest records between January 1, 2009 and December 31, 2013, before and after the publication of the 2010 ACLS guidelines and recorded in an encrypted secured password-protected database. All cardiac arrests in the form of asystole and/or PEA at some time during resuscitation in patients aged 19 years and older were included in the study. This included all prehospital patients presenting to the emergency department and in-hospital emergency department patients with asystole and PEA cardiac arrests. Patients were excluded if they were younger than 19 years of age, the cardiac arrest was not in the form of asystole or PEA, or the patient had a “do not resuscitate” order. For each identified patient, the patient’s age, gender, date of arrest, type(s) of arrest, prehospital vs in-hospital arrest, initials of the emergency physician resuscitation leader, and the medications given during the resuscitation were recorded. We examined whether atropine was used during the resuscitation. We also studied the use of epinephrine as a control. A time versus atropine and a time versus epinephrine usage graph were generated and examined.
Results
Between January 1, 2009 and December 31, 2013, 64 cardiac arrest records were found. In total, 55 resuscitations met the inclusion criteria. This included 38 prehospital and 17 in-hospital emergency department asystole and/or PEA cardiac arrests. Seventeen emergency physicians were identified to be involved with the resuscitations. The median age of the cardiac arrest patients was 72. There were 22 women and 33 men. Atropine was used in 21 cardiac arrests, while epinephrine was used in 51 cardiac arrests. A time vs atropine use graph and a time vs epinephrine use graph were generated (Figures 1 and 2).
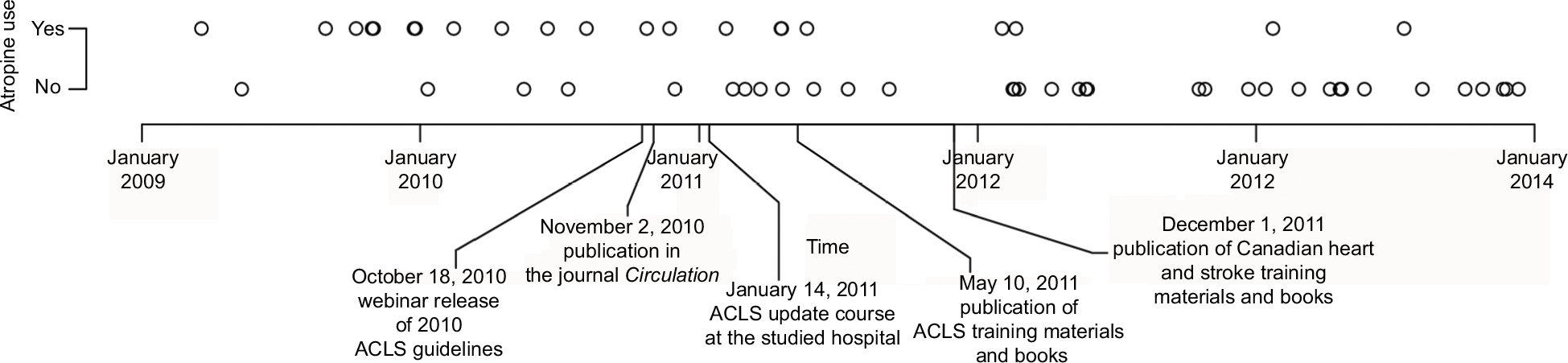 | Figure 1 Atropine use in asystole and/or PEA cardiac arrest. Abbreviations: PEA, pulseless electric activity; ACLS, Advanced Cardiac Life Support. |
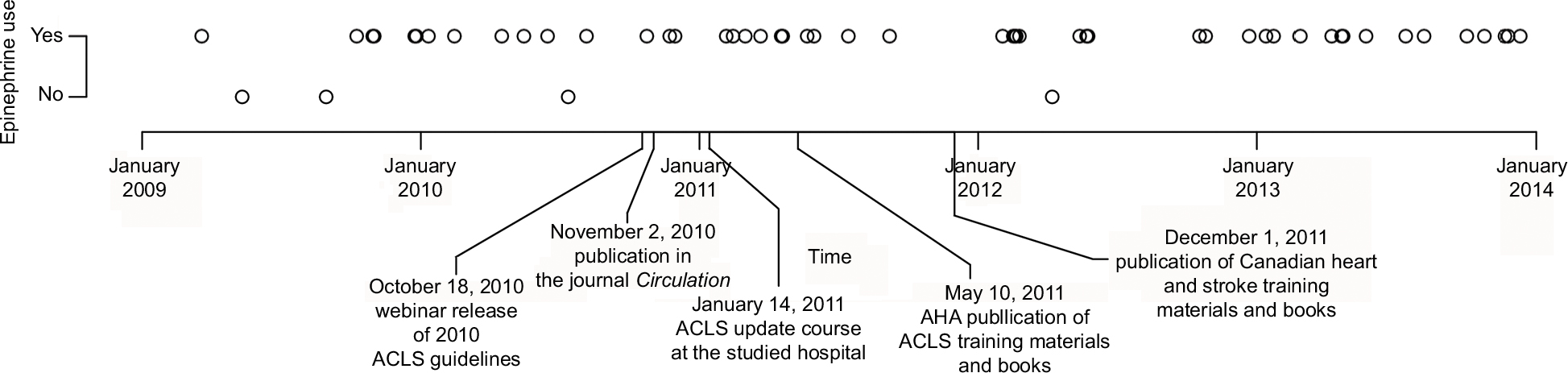 | Figure 2 Epinephrine use in asystole and/or PEA cardiac arrest. Abbreviations: PEA, pulseless electric activity; ACLS, Advanced Cardiac Life Support. |
Discussion
We conducted a hypothesis-generating study on the delay in physicians’ adaptation of clinical practice guidelines by examining the effect of the 2010 ACLS guidelines on the use of atropine in asystole/PEA cardiac arrests. Although the ACLS guidelines were first presented in October 2010 (Box 1), we observed that change in atropine use occurred later around the summer of 2011. These findings elicit 2 questions. First, what guideline dissemination strategies can be used to decrease the lag time in translating ACLS guidelines into practice? Second, what should the timing of these dissemination strategies be to maximize its effect? We believe through quantifying the time lag in translating guidelines into practice, we can better answer these questions by studying whether changes in the type and timing of guideline dissemination strategies will decrease this lag time in the future.
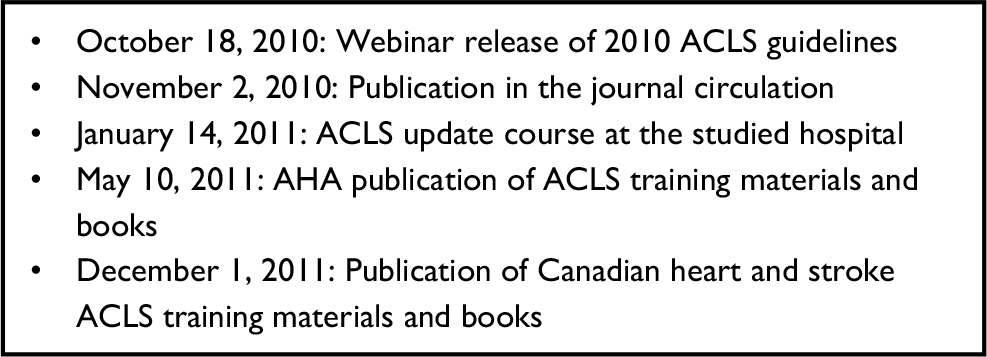 | Box 1 The timeline of the 2010 ACLS guidelines dissemination Abbreviation: ACLS, Advanced Cardiac Life Support. |
Disclosure
The authors report no conflicts of interest in this work.
References
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? JAMA. 1999;282(15):1458–1465. | ||
Carveth S. Standards for cardiopulmonary resuscitation and emergency cardiac care. JAMA. 1974;227(7):796–797. | ||
Field JM, Hazinski MF, Sayre MR, et al. 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(Suppl 3):S640–S946. | ||
Weingarten S. Translating practice guidelines into patient care. Chest. 2000;118(Suppl 2):4S–7S. | ||
Bigham BL, Koprowicz K, Aufderheide TP, et al. Delayed prehospital implementation of the 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiac care. Prehosp Emerg Care. 2010;14(3):355–360. | ||
Govindarajan P, Lin L, Landman A, et al. Practice variability among the EMS systems participating in Cardiac Arrest Registry to Enhance Survival (CARES). Resuscitation. 2012;83(1):76–80. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.