")
Back to Journals » International Journal of General Medicine » Volume 9
Hyponatremia in patients hospitalized with heart failure: a condition often overlooked in low-income settings
Authors Ali K, Workicho A, Gudina EK
Received 19 April 2016
Accepted for publication 19 May 2016
Published 1 August 2016 Volume 2016:9 Pages 267—273
DOI https://doi.org/10.2147/IJGM.S110872
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Khalid Ali,1 Abdulhalik Workicho,2 Esayas Kebede Gudina3
1Department of Internal Medicine, Dire Dawa University, Dire Dawa, 2Department of Epidemiology, 3Department of Internal Medicine, Jimma University, Jimma, Ethiopia
Background: Hyponatremia is a common electrolyte abnormality in patients with heart failure (HF). It is independently associated with increased short-term and long-term morbidity and mortality. The main objective of this study was to assess patterns of hyponatremia and its association with discharge outcomes in patients with HF admitted to a teaching hospital in Ethiopia.
Patients and methods: This is a descriptive, prospective, hospital-based cohort study of patients with HF admitted to Jimma University Hospital, Ethiopia, between November 1, 2013 and July 31, 2014. A structured questionnaire was used to collect information on sociodemographic characteristics, clinical profile at admission, and outcomes at discharge. Plasma sodium concentration was analyzed at admission for all patients. The relationship between hyponatremia at admission and in-hospital mortality, as well as length of hospital stay, was assessed using both bivariate analysis and multivariable logistic regressions. The level of statistical significance was set at P<0.05.
Results: Of 152 participants admitted with HF, 44 (28.9%) had hyponatremia, which is defined as serum sodium level <135 mmol/L. Patients on salt restriction, on chronic diuretic treatment (furosemide and spironolactone), and with impaired renal function at admission were found to be highly affected. Hyponatremia was found to be associated with increased in-hospital mortality (P=0.008) and longer hospital stay (16.6 vs 12 days, P<0.001). Patients with hyponatremia also had lower blood pressure and poor functional status at discharge.
Conclusion: This study demonstrates that hyponatremia is highly prevalent in patients hospitalized with HF and is associated with increased in-hospital mortality and longer hospital stay. Thus, great emphasis should be given to identify high-risk patients, and prevention and early detection of hyponatremia to prevent its deleterious effects. Large-scale national studies are also needed to complement our findings.
Keywords: heart failure, hyponatremia, outcome, Ethiopia, Africa
Introduction
Heart failure (HF) remains a deadly clinical syndrome despite advances in its management.1 It represents a considerable burden to the health care system, responsible for significant health expenditure and high rates of hospitalizations. HF accounts for approximately 5% of all hospital admissions.1–3
Hyponatremia is the most common electrolyte abnormality in patients hospitalized with HF4 with a prevalence of 19%–25%.5–8 Its occurrence often parallels the severity of cardiac dysfunction.9 Hyponatremia in HF is multifactorial in origin, which results from a combination of mechanisms. The reduction in cardiac output and relative arterial underfilling are important mechanisms for the development of hyponatremia through neurohormonal stimulation.9,10 HF therapy is another factor contributing to hyponatremia.9–11 Although thiazide diuretics are most often implicated, nonthiazide agents such as furosemide and spironolactone also have been associated with hyponatremia.11 Hyponatremia in patients with HF may therefore be a marker of increased neurohormonal activation that reflects the severity of HF.9
Hyponatremia is independently associated with increased short-term and long-term morbidity and mortality for both hospitalized and ambulatory HF outpatients, nearly doubling the risk of mortality in this group. Even mild hyponatremia among patients hospitalized with HF, regardless of ventricular function, is associated with increased in-hospital and postdischarge mortality, prolonged hospital stay, and frequent rehospitalization.6–8,12–15
The presence of hyponatremia can also interfere with administration of appropriate therapy; especially limiting options in terms of diuretic management and could potentially alter HF therapy leading to increase in mortality.11
Most cases of hyponatremia among patients hospitalized with HF are usually chronic and asymptomatic, often detected incidentally.7 As a result, patients with preexisting hyponatremia are often untreated and are at higher risk of severe hyponatremia if not recognized early. As the likelihood of implementing standard management of hyponatremia in low-income countries is questionable, earlier recognition, identification of patients at risk, and prevention will be the most effective approach in such patients.16 In addition, making a timely and accurate diagnosis and instituting appropriate therapy is also crucial.17 Therefore, health care professionals should identify patients who are at risk of developing hyponatremia, should have a good understanding of the importance of early diagnosis, and preventive strategy and management of hyponatremia in order to reduce the adverse consequences of this common metabolic disorder.16
Despite a wealth of information in high-income settings regarding prevalence and characteristics of hyponatremia in patients with HF, there is a prominent scarcity of data in developing countries, particularly in resource-limited sub-Saharan Africa. The main aim of this study was thus to assess the prevalence of hyponatremia in patients hospitalized with HF, identify factors associated with its occurrences, and identify its impact on discharge outcome of patients hospitalized with HF admitted to a teaching hospital in Ethiopia.
Patients and methods
Study setting, and period
The study was conducted at Jimma University Hospital located in Jimma town in Ethiopia. The hospital is the only teaching and referral hospital in southwest Ethiopia. It serves ∼14,000 admissions and 123,000 outpatient visits annually. However, the proportion of HF admissions and its inpatient mortality is unknown. At the time of the study, there were a total of 1,600 patients with HF on follow-up at a cardiac follow-up clinic of the hospital. The study was conducted from November 1, 2013 to July 31, 2014 using hospital-based prospective cohort study.
Study participants
Participants of the study were adult patients ≥18 years of age admitted with clinical diagnosis of HF to the medical wards of the hospital during the study period.
Selection of participants
Patients hospitalized with HF fulfilling the Framingham’s criteria (having two major criteria or one major and two minor criteria)18 for clinical diagnosis and were willing to participate were included in the study.
All study eligible patients admitted during the period of data collection were consecutively recruited based on their consent. A total of 152 patients were included in the study.
Data collection process
All new admissions to medical wards were reviewed daily for eligibility. Patients with admission diagnosis of HF were assessed for inclusion using the Framingham’s criteria for clinical diagnosis.18 Data were collected from eligible patients both at admission and on leaving the hospital. A structured questionnaire was used to collect all the required variables through in-depth interview and physical examination. Demographic characteristics, clinical symptoms at presentation, and previous medical condition (diagnosed diseases, previous therapies, and admissions) were collected at admission through an interview. A physical examination was performed at admission to assess the following: New York Heart Association (NYHA) functional class and noninvasive hemodynamic assessments (evidences of pulmonary congestion, elevation of jugular venous pressure, third heart sound, hepatomegaly, ascites, peripheral edema, coldness of the extremities, blood pressures, and heart rate).
Relevant laboratory data and diagnostic investigations (serum creatinine, blood urea nitrogen, complete blood count, electrocardiography, and echocardiography) and in-hospital management of the patient were collected through chart review. Information regarding in-hospital mortality, cause of death, and date of death were documented from the chart and ward registry. NYHA functional status assessment was also done at discharge for survivors.
The glomerular filtration rate (GFR) was estimated based on serum creatinine and patient’s age, sex, and race. An online-based calculation using Modification of Diet in Renal Disease GFR equation was used for this purpose. The equation can be found at http://www.mdcalc.com/mdrd-gfr-equation/.
Procedures
Electrolytes including serum sodium, potassium, and chloride were determined on the day of admission for all patients. Approximately 5 mL of venous blood was collected by vacuum punctures from each patient into an evacuated tube without any anticoagulant. The blood samples were analyzed within 30 minutes of collection. The tubes were centrifuged unopened to separate the serum. The separated serum was analyzed for the three electrolytes by direction-selective electrolyte analyzer on the HumaLyte Plus 3 (Human Diagnostics GmbH, Wiesbaden, Germany) in the Central Laboratory of the hospital. Quality control of the analyzer (machine) was done routinely with system check cartridge prepared for this purpose each day before the actual sample analysis. The normal range of serum sodium for the machine was calibrated at 135–145 mmol/L (value on the cartridge itself). Hyponatremia was defined as a plasma sodium level of <135 mmol/L based on the threshold used by the laboratory.
Except for serum electrolyte determination, which is not a routine test at the hospital, all the other baseline and diagnostic tests were done as part of routine evaluation for patients hospitalized with HF. Thus, the investigators neither requested nor recommended treating physicians to do these tests. The investigators did not also directly interfere with the treatment plan of the admitted patients. However, abnormal electrolyte results were communicated to treating physician for intervention.
The quality of data was ensured through the training of the data collectors, close supervision, and immediate feedback, reviewing each of the completed data collection tools daily. Data consistency and completeness were checked throughout the data collection and analysis. The electrolyte analyzer machine was calibrated on a daily basis to ensure the accuracy of the result.
Data processing and analysis
The collected data were checked for completeness and consistency prior to entering into the computer for analysis. Data analyses were performed using SPSS version 16 (SPSS Inc., Chicago, IL, USA). Continuous variables were described as mean ± standard deviation (SD). Categorical variables were reported as frequencies and percentages of nonmissing values. Serum sodium concentrations at admission were categorized into two discrete groups: Na <135 mmol/L (hyponatremia) and Na ≥135 mmol/L (normal serum sodium).
Associations between baseline characteristics and hyponatremia were tested using chi-square test. Chi-square test and Fisher’s exact test, for cells with small counts, were also used to assess the association between hyponatremia and outcomes at discharge. Independent sample t-test was used to compare the association between normally distributed continuous and categorical variables. P-values <0.05 were taken as a level of statistical significance.
Operational definitions of terms in the study
- Anemia – It is defined by the criterion established by the World Health Organization (WHO): hemoglobin <13.0 g/dL for men and hemoglobin <12.0 g/dL for women.
- Baseline serum creatinine – the value recorded in the first 3 days of hospitalization.
- Hyponatremia – serum sodium value of <135 mmol/L.
- In-hospital mortality – death from any cause occurring before hospital discharge.
- Length of stay in the hospital – duration from admission to the wards to discharge from the hospital.
- NYHA functional status – refers to patient’s reported symptoms in relation to physical activities.
- Class I: no limitations. Ordinary physical activity does not cause undue fatigue, dyspnea, or palpitations.
- Class II: slight limitation of physical activity. Such patients are comfortable at rest. Ordinary physical activity results in fatigue, palpitations, dyspnea, or angina.
- Class III: marked limitation of physical activity. Although patients are comfortable at rest, less-than-ordinary activity leads to fatigue, dyspnea, palpitations, or angina.
- Class IV: symptomatic at rest. Symptoms of HF are present at rest; discomfort increases with any physical activity.
Ethical consideration
The study was approved by Ethical Review Board of Jimma University College of Health Sciences. An official letter from the board was written to the hospital. Written informed consent was obtained from the study participants or parents/guardians of the participants if the participant was legally unable to make decision. Patient’s confidentiality, equity of services, and interests of patients were ensured during the study period. All data collected during the study were treated with strict confidentiality. This study did not involve any potentially harmful intervention to the patient. Assessment of patient’s serum sodium was done using venous blood and the results were attached to the patient’s clinical records and all findings were communicated to the patients or parents/guardians and the managing physician to make use for intervention in case of abnormality.
Results
Baseline characteristics
During the study period of November 1, 2013 to July 31, 2014, a total of 152 patients admitted with HF were included in the study. Approximately half, 77 (50.7%) of them were males and 96 (63.2%) were older than 45 years with a mean age of 50.9 (SD =18.0) years. A 110 (72.4%) were rural residents and 85 (55.9%) were illiterate.
All patients had exertion-related dyspnea at presentation; most had overt symptoms at rest with orthopnea and paroxysmal nocturnal dyspnea. Approximately 89% presented with Class IV NYHA functional status. Fifty-seven (37.5%) participants were previously diagnosed with HF; 39 (68.4%) among these group had at least one HF-related admission before. Major underlying causes of HF were identified to be ischemic heart disease (40.8%), valvular heart disease (21.1%), and hypertensive heart disease (17.1%; Table 1). Ninety (59.2%) patients had some degree of anemia; 26.3% had high blood pressure and 27.0% had atrial fibrillation at presentation. The mean GFR was 92 mL/minute/1.73 m2 (SD =43) with a range of 8.4–208.5 mL/minute/1.73 m2. Seventy (46.1%) patients had GFR ≥90 mL/minute/1.73 m2, whereas four patients presented with end-stage renal disease.
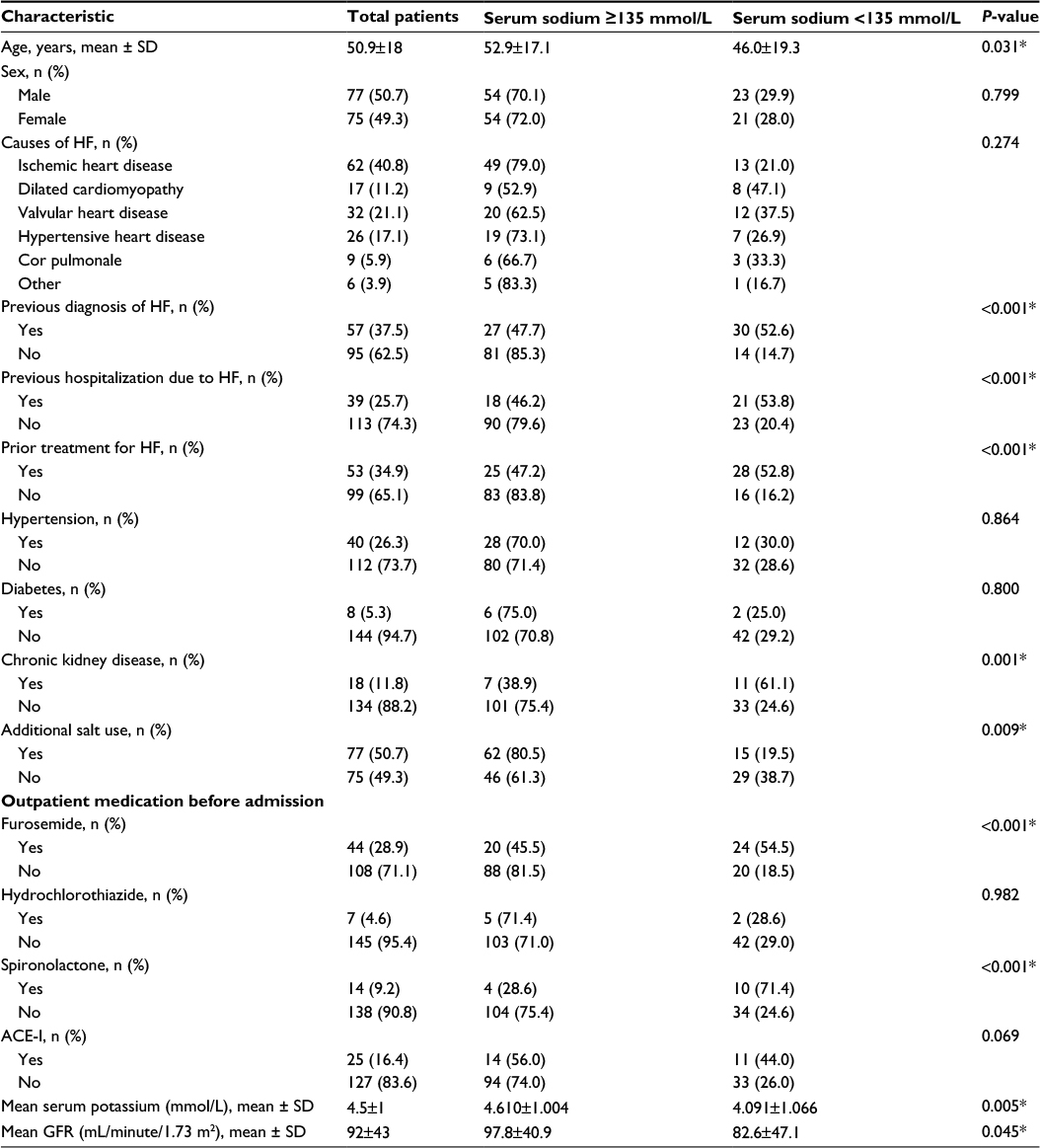 | Table 1 Factors associated with hyponatremia in patients with HF admitted to Jimma University Hospital, Ethiopia (November 1, 2013–July 31, 2014) Note: *Denotes statistically significant P-values. Abbreviations: HF, heart failure; SD, standard deviation; ACE-I, angiotensin-converting enzyme inhibitor; GFR, glomerular filtration rate. |
Patterns of serum sodium
The mean admission serum sodium was 136.9 mmol/L (SD =7.0) with a range of 119.4–157.6 mmol/L. Hyponatremia defined as serum sodium <135 mmol/L was observed in 44 (28.9%) patients.
Factors associated with hyponatremia
Hyponatremia was found to be more prevalent in those on chronic salt restriction, those on maintenance of diuretic treatment (furosemide and spironolactone), and those with established chronic kidney disease. Low serum sodium was also associated with impaired renal function at admission (reduced GFR); estimated GFR =82.6±47.1 mL/minute/1.73 m2 in those with hyponatremia compared to 97.8±40.9 mL/minute/1.73 m2 in those with normal sodium, P=0.045. Patients with hyponatremia were also found to be younger, with a mean age of 45.98±19.28 years vs 52.9±17.11 years (Table 1).
On multivariable logistic regression analysis, only low GFR (renal insufficiency) at admission was independently associated with hyponatremia (adjusted OR =4.23, 95% CI =1.20–15.44, P=0.028). However, this association is very weak due to a wide CI. Moreover, no association was found between HF etiology and duration of HF and comorbidities like diabetes, hypertension, and anemia.
Hyponatremia and in-hospital outcomes
Patients with low serum sodium (hyponatremia) had low mean systolic and diastolic blood pressure compared to those with serum sodium of ≥135 mmol/L; on average 11 mmHg less for systolic blood pressure (P=0.031) and 8 mmHg less for diastolic blood pressure (P=0.027).
Overall, the mean length of hospital stay was 13±8 days. Patients with hyponatremia had longer hospital stays, 16.6±9.4 days vs 12±7 days compared to those with serum sodium of ≥135 mmol/L (P<0.001).
The in-hospital mortality rate was also found to be higher in those with hyponatremia than those with normal serum sodium, 11.4% vs 1.0% (P=0.008; Table 2).
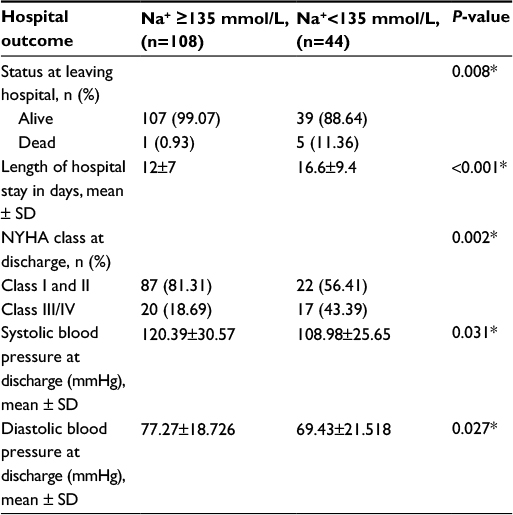 | Table 2 Outcomes of patients with heart failure according to serum sodium status in patients with heart failure admitted to Jimma University Hospital, Ethiopia (November 1, 2013–July 31, 2014) Note: *Denotes statistically significant P-values. Abbreviations: SD, standard deviation; NYHA, New York Heart Association. |
Similar association was seen between hypnatremia and poor functional status at discharge; 43.6% of those with hyponatremia were discharged with NYHA (Class III and IV) compared with 18.7% in the other group (P=0.002; Table 2).
Discussion
The findings of this study demonstrated that hyponatremia was present in 28.9% of patients hospitalized with HF. Patients on long-term diuretic therapy, on salt restriction, and with renal insufficiency were found to be at high risk. Moreover, baseline hyponatremia in patients hospitalized with HF was associated with poor overall discharge outcomes.
The prevalence of hyponatremia in patients hospitalized with HF in this study is within the range reported in other studies: 27% in Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF)8 and 23.8% in the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheter Effectiveness (ESCAPE).7 However, it is higher than findings from Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) with 19.7%,6 the Korean heart failure Registry (KorHF) with 19.1%,19 and Japanese ATTEND registry with 11.6%.20
In addition to neurohormonal mechanisms of HF,9,10 chronic diuretic therapy is now a well-known cause of hyponatremia in such patients.11,21–23 Similarly, in our study, chronic therapy with furosemide and spironolactone were associated with increased risk of hyponatremia even though this association disappeared on multivariable analysis. Renal insufficiency was the only factor independently associated with hyponatremia, a finding consistent with previous studies.24,25 However, this association also looks very weak due to a wide CI. The lack of independent association between these established risk factors and occurrence of hyponatremia in our study is mainly due to small sample size. Nevertheless, the presence of association on univariable analysis is relevant from a clinical point of view.
In-hospital mortality in our study was relatively low; however, the fact that five of the six deaths occurred in those with hyponatremia shows the significance of this association. The increased mortality due to hyponatremia, though the magnitude of this effect varied based on the population studied, is well-documented in multiple large-scale studies from around the globe.6–8,19,20,26,27
The mean hospital stay of patients with HF is approximately 7 days in most of the previous studies.6,8,25 However, the average hospital stay of 13 days in our study was much higher than these findings. Moreover, 71.7% of the patients had at least 8 days of hospital stay. Furthermore, patients with hyponatremia who survived to discharge had longer hospital stays (16.6 days on average). Even though a trend of longer hospital stays among patients hospitalized with HF and who also had hyponatremia has been well-documented in multiple studies in different settings,6,8,19,20,24,25,28 the overall findings in our study may be a reflection of the severity of underlying HF status in our participants. In addition, difference in quality and effectiveness of inpatient management for HF may also be a reason for this difference. The reason for longer hospital stays in the study setting is thus beyond the scope of this study and deserves further scrutiny.
The findings of our study are highly relevant in the light of scarce information in the field in Ethiopia and other similar settings. There is neither routine electrolyte assessment at the hospital nor is there any guideline addressing this issue in high-risk patients. As a result, patients hospitalized with HF who also have hyponatremia remain untreated, which in turn may contribute to poor treatment outcome. Thus, the findings in our study may serve as a wake-up call for further action.
Limitations
However, our study has multiple limitations that deserve listing here. First, the study was limited to only a single teaching hospital with a relatively small sample size. Second, serum sodium was determined at baseline only and the effect of inpatient HF therapy on hyponatremia was not assessed. Furthermore, only outcome at discharge was assessed with little knowledge on immediate postdischarge or long-term outcome. Thus, the finding of our study may not reflect the true burden of the problem.
Conclusion
Hyponatremia was found to be highly prevalent in patients with HF admitted to Jimma University Hospital in Ethiopia and was found to be strongly associated with poor overall discharge outcomes. We thus recommend that all patients hospitalized with HF should have a serum sodium analysis during admission and be serially followed during their hospital stay. At-risk patients (those with impaired renal function test, on absolute salt restriction, and on chronic diuretic therapy) should also be screened during their follow-up. Furthermore, a large-scale national study should be done to complement this study and to outline management of such patients in the country.
Acknowledgments
The authors would like to thank Jimma University for funding this project. They would also like to thank Jimma University hospital, particularly, laboratory staff members and clinicians in the medical ward for their support during data collection. This research was funded by Jimma University as part of a postgraduate thesis support.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Bui AL, Horwich TB, Fonarow GC. Epidemiology and risk profile of heart failure. Nat Rev Cardiol. 2011;8(1):30–41. | ||
Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 2008;29(19):2388–2442. | ||
Go AS, Mozaffarian D, Roger VL, et al. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):143–152. | ||
Farmakis D, Filippatos G, Parissis J, Kremastinos DT, Gheorghiade M. Hyponatremia in heart failure. Heart Fail Rev. 2009;14(2):59–63. | ||
Rossi J, Bayram M, Udelson JE, et al. Improvement in hyponatremia during hospitalization for worsening heart failure is associated with improved outcomes: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) trial. Acute Card Care. 2007;9(2):82–86. | ||
Gheorghiade M, Abraham WT, Albert NM, et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur Heart J. 2007;28(8):980–988. | ||
Georghiade M, Rossi JS, Cotts W, et al. Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trial. Arch Intern Med. 2007;167(18):1998–2005. | ||
Klein L, O’Connor CM, Leimberger JD, et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation. 2005;111(19):2454–2460. | ||
Sica DA. Hyponatremia and heart failure--pathophysiology and implications. Congest Heart Fail. 2005;11(5):274–277. | ||
Bettari L, Fiuzat M, Felker GM, O’Connor CM. Significance of hyponatremia in heart failure. Heart Fail Rev. 2012;17(1):17–26. | ||
Oren RM. Hyponatremia in congestive heart failure. Am J Cardiol. 2005;95(9A):2B–7B. | ||
Lee WH, Packer M. Prognostic importance of serum sodium concentration and its modification by converting-enzyme inhibition in patients with severe chronic heart failure. Circulation. 1986;73(2):257–267. | ||
Balling L, Schou M, Videbæk L, Hildebrandt P, Wiggers H, Gustafsson F; Danish Heart Failure Clinics Network. Prevalence and prognostic significance of hyponatraemia in outpatients with chronic heart failure. Eur J Heart Fail. 2011;13(9):968–973. | ||
Milo-Cotter O, Cotter G, Weatherley BD, et al. Hyponatraemia in acute heart failure is a marker of increased mortality but not when associated with hyperglycaemia. Eur J Heart Fail. 2008;10(2):196–200. | ||
Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA. 2003;290(19):2581–2587. | ||
Bissram M, Scott FD, Liu L, Rosner MH. Risk factors for symptomatic hyponatremia: the role of pre-existing asymptomatic hyponatremia. Intern Med J. 2007;37(3):149–155. | ||
Reynolds RM, Seckl JR. Hyponatraemia for the clinical endocrinologist. Clin Endocrinol (Oxf). 2005;63(4):366–374. | ||
Marantz PR, Tobin JN, Wassertheil-Smoller S, et al. The relationship between left ventricular systolic function and congestive heart failure diagnosed by clinical criteria. Circulation. 1988;77(3):607–612. | ||
Lee SE, Choi DJ, Yoon CH, et al. Improvement of hyponatraemia during hospitalisation for acute heart failure is not associated with improvement of prognosis: an analysis from the Korean Heart Failure (KorHF) registry. Heart. 2012;98(24):1798–1804. | ||
Sato N, Gheorghiade M, Kajimoto K, et al. Hyponatremia and in-hospital mortality in patients admitted for heart failure (from the ATTEND registry). Am J Cardiol. 2013;111(7):1019–1025. | ||
Sonnenblick M, Friedlander Y, Rosin AJ. Diuretic-induced severe hyponatremia. Review and analysis of 129 reported patients. Chest. 1993;103(2):601–606. | ||
Brater DC. Diuretic therapy in congestive heart failure. Congest Heart Fail. 2000;6(4):197–201. | ||
Krämer BK, Schweda F, Riegger GA. Diuretic treatment and diuretic resistance in heart failure. Am J Med. 1999;106(1):90–96. | ||
Hoorn EJ, Lindemans J, Zietse R. Acute and concomitant deterioration of hyponatremia and renal dysfunction associated with heart and liver failure. Clin Nephrol. 2006;65(4):248–255. | ||
Saepudin S, Ball PA, Morrissey H. Hyponatremia during hospitalization and in-hospital mortality in patients hospitalized from heart failure. BMC Cardiovasc Disord. 2015;15:88. | ||
Shchekochikhin DY, Schrier RW, Lindenfeld J, Price LL, Jaber BL, Madias NE. Outcome differences in community- versus hospital-acquired hyponatremia in patients with a diagnosis of heart failure. Circ Heart Fail. 2013;6(3):379–386. | ||
Shorr AF, Tabak YP, Johannes RS, Gupta V, Saltzberg MT, Costanzo MR. Burden of sodium abnormalities in patients hospitalized for heart failure. Congest Heart Fail. 2011;17(1):1–7. | ||
Krumholz HM, Chen YT, Bradford WD, Cerese J. Variations in and correlates of length of stay in academic hospitals among patients with heart failure resulting from systolic dysfunction. Am J Manag Care. 1999;5(6):715–723. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.