")
Back to Journals » International Medical Case Reports Journal » Volume 13
Hypermature Intumescent Cataract in Advanced Keratoglobus
Authors Singh B, Sharma S, Bharti N, Ranjan R , Bharti S
Received 7 August 2020
Accepted for publication 14 September 2020
Published 12 October 2020 Volume 2020:13 Pages 507—511
DOI https://doi.org/10.2147/IMCRJ.S275335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Hypermature Intumescent cataract in advanced Keratoglobus" [ID 275335].
Views: 362
Bhupesh Singh,1 Sourabh Sharma,2 Neha Bharti,3 Richa Ranjan,3 Sudhank Bharti1
1Cornea Department, Bharti Eye Foundation and Hospital, New Delhi, India; 2Glaucoma Department, Bharti Eye Foundation and Hospital, New Delhi, India; 3Vitreoretina Department, Bharti Eye Foundation and Hospital, New Delhi, India
Correspondence: Sourabh Sharma
Bharti Eye Foundation and Hospital, New Delhi, India
Tel +91-9910790540
Email [email protected]
Abstract: We report a rare case of bilateral keratoglobus with hypermature intumescent cataract in a 55-year-old woman. Clinical examination and corneal topography confirmed generalized corneal bulging and global corneal thinning. A Pentacam® (Oculus Optikgerate, Wetzlar, Germany) demonstrated bilateral diffuse corneal thinning (368 μm in the right eye and 371 μm in the left eye). Phacoemulsification was performed in the right eye after thorough workup and modification of the surgical technique. This case report helps in better understanding of the challenges of cataract surgery and intraocular lens selection in a keratoglobus patient, and stresses the need for both thorough preoperative planning and intraoperative surgical modifications.
Keywords: keratoglobus, intumescent cataract, corneal ectasia
Introduction
Keratoglobus is a rare form of corneal ectasia, which is described as a non-inflammatory corneal disorder characterized by generalized corneal thinning and globular protrusion.1 Both congenital and acquired forms have been reported; the former are usually bilateral and may be associated with various other ocular and systemic syndromes such as Ehlers–Danlos syndrome VI, blue sclera and Leber’s congenital amaurosis.2,3 The acquired forms have been reported to be associated with dysthyroid ophthalmopathy, chronic marginal blepharitis and vernal keratoconjunctivitis.4 There are also cases where keratoglobus has evolved from preexisting pellucid marginal degeneration or advanced keratoconus.5 Keratoglobus patients usually have poor vision and there is no significant improvement with glasses. Contact lens fitting is always a challenge in these eyes because of globular protrusion. Any surgical procedure in these eyes is challenging and can lead to major intraoperative and postoperative complications.6
We report a case of bilateral keratoglobus with cataract in both eyes. We describe the difficulties encountered in intraocular lens (IOL) power calculation, the surgical challenges faced and modification of the surgical techniques to avoid potential complications. Postoperative rehabilitation methods are also discussed.
Case Report
A 55-year-old female came to our ophthalmology department with the main complaint of progressive diminution of vision in the right eye more than the left eye over the past 3 years. She gave a history of enlarged eyes with suboptimal vision since childhood. She had used spectacles since the age of 14 years and the refractive error had never been corrected with contact lenses. There was no significant systemic or family history or any history of trauma.
At the time of the examination at our center, the visual acuity in the right eye was light perception with accurate projection of rays in all quadrants, and that in the left eye was counting fingers at 2 m. Significant globular enlargement of both corneas was apparent to the naked eye. The vertical corneal diameter was 13 mm in both eyes. Her intraocular pressure was 9 mmHg in the right eye and 10 mmHg in the left eye, measured with a non-contact tonometer (NIDEK, Gamagori, Aichi, Japan). On slit-lamp examination, there was a marked protrusion of cornea with thinning as well as arcus senilis-like peripheral scarring. The anterior chambers were very deep, while the iris and pupil were unremarkable. The right eye had intumescent cataract while the left had cataract grade III. The posterior segment was not visible in the right eye and was hazily seen in the left eye.
After a detailed explanation had been given to the patient regarding the nature of the disease, written informed consent was taken, and slit-lamp clinical photographs (Figure 1A and B), Scheimflug topography by Pentacam® (Figure 2A and B), specular microscopy (NIDEK CEM-530; Gamagori Aichi, Japan), anterior segment optical coherence tomography (RTVue; Optovue, Fremont, CA) and ultrasound B-scans (US-4000; NIDEK, Japan) were obtained.
 |
Figure 1 Slit-lamp photograph showing bilateral keratoglobus with arcus-like peripheral scarring: (A) right eye with intumescent white cataract; (B) left eye with cataract grade III. |
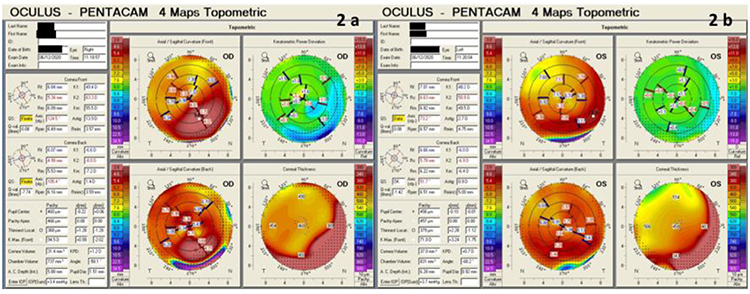 |
Figure 2 Topometric maps on the Pentacam showing diffuse corneal steepening and thinning: (A) right eye; (B) left eye. |
Corneal topography showed marked corneal ectasia. Topometric maps of the right eye showed values of 49.4 D and 63.3 D in the horizontal and vertical meridians, respectively. The respective values for the left eye were 48.2 D and 50.9 D. The pachymetry maps showed the thinnest cornea of 368 μm and 379 μm in the right eye and left eye, respectively. Specular microscopy showed endothelial cell counts of 2074 cells/mm2 in the right eye and 1945 cells/mm2 in the left eye. No morphological anomalies were seen on the endothelium. Anterior chamber depth (internal) was 5.88 mm in the right eye and 6.28 mm in the left eye, while axial length was 27.22 in the right eye and 26.27 mm in the left eye. B-scan ultrasonography showed an unusually large anterior segment and no posterior segment abnormality. The lens was in a normal anatomical relationship with the ciliary body.
After obtaining informed consent and explaining the guarded visual prognosis, phacoemulsification with monofocal IOL was planned in the right eye. The IOL power can be calculated by different formulae, including Holladay, SRK/T, SRK II and Barrett Universal formula II. As it is difficult to reach conclusions regarding the IOL formula in more advanced ectatic corneas, we chose Barrett Universal formula II. The power of the implanted IOL was −7 D (as discussed later, in the Discussion section).7
Surgical Technique with Modifications
The surgery was performed by an experienced surgeon (BS). The surgeon’s usual surgical technique was modified for the case. After instillation of proparacaine eye drops, an equal mixture of bupivacaine 0.5% and lignocaine 2% was injected subconjunctivally with a 25-gauge needle. Because of the thin cornea, a 2.2 mm superior scleral incision was planned. After local conjunctival peritomy and light cautery, a triplanar main port incision was made transsclerally at 120 degrees. The side-port paracentesis incisions were made through the limbal sclera to avoid the thin peripheral cornea with a 20 G MVR knife at 60 degrees. In view of the poor red reflex and visibility, the anterior lens capsule was stained with 0.06% trypan blue dye. The anterior chamber was overfilled with viscoelastic material to create an equilibrium between the anterior chamber pressure and high intralenticular pressure. Capsulorhexis was initiated with the help of cystitome and a white milky secretion was seen oozing out of the capsular bag. A microrhexis forceps was therefore used to complete the rhexis. The chamber depth, scleral incisions and steep cornea caused a lot of difficulties with intraoperative visibility and depth of field. This made control of the capsulorhexis difficult, which led to its radial extension towards the equator but, fortunately, no posterior extension of the capsular tear was noted.
Hydrodissection was not performed, to avoid any further extension of the rhexis. An excessively deep anterior chamber necessitates holding instruments more vertically and increases the range of focus required. This change in phaco probe orientation distorted the cornea, making the surgical view even poorer. Thus, it was very difficult to reach the cataractous lens with the phaco probe. After a few attempts, the nucleus was successfully cracked and chopped, using a stop-and-chop technique. The nucleus fragments were then luxated to the anterior chamber and emulsified using low phaco and vacuum power to avoid any stress on the zonules. Cortex removal was performed with the help of a bimanual irrigation aspiration cannula. The IOL used was a Sensar monofocal three-piece foldable hydrophobic acrylic (IOL model number AR40M; Johnson & Johnson Vision Care) and was implanted in the sulcus, as there was extension of the anterior capsule. The viscoelastic material was washed and the anterior chamber was formed. The phaco wound was sutured with radial 10–0 nylon suture. The entire surgical procedure was uneventful other than the radial extension of the capsule (see Supplementary Video, which demonstrates the surgical steps).
Postoperatively, prednisolone and moxifloxacin eye drops were prescribed four times per day each for 3 weeks.
The cornea was clear on the first postoperative day with uncorrected visual acuity of 6/60. At 1-month follow-up, the sutures were removed and the best corrected visual acuity (BCVA) was 6/24 with a correction of +1.5 D spherical with −2 D of astigmatism at 120 degrees (+0.5 D spherical equivalent). The corneal endothelial count was 1860 cells/mm2. The IOL was stable and centered.
Discussion
In this article, we report a case of bilateral keratoglobus presenting with hypermature intumescent cataract in one eye, which was managed adequately with phacoemulsification with monofocal IOL implantation, achieving a successful surgical outcome and recovery of the patient’s daily activities.
Keratoglobus is a rare non-inflammatory ectatic corneal disorder with limited literature. It is very important to differentiate keratoglobus from keratoconus. Keratoconus usually starts at puberty and progresses until around 40 years of age, whereas keratoglobus usually presents at birth and is non-progressive or minimally progressive in nature. In keratoconus, corneal thinning is usually paracentral and conical in shape, whereas in keratoglobus, there is a diffuse thinning and globular protrusion.8 Another confusing clinical entity is megalocornea, in which the corneal diameter increases over 12.5 mm with no associated thinning of the cornea, whereas in keratoglobus the corneal diameter is usually unchanged but corneal thinning is the main feature. Keratoglobus also resembles very closely anterior megalophthalmos, in which eyes with enlarged corneas, but with normal axial lengths and corneal curvature, are seen.9
Performing cataract surgery in these eyes is full of challenges, starting from the preoperative work-up, IOL power calculation and selection, intraoperative difficulties owing to the extremely deep anterior chamber making visualization difficult and surgical maneuvers more challenging. The refractive outcomes are also unpredicatable in such cases.
In our case, selecting, calculating and choosing the IOL presented the greatestchallenge. Different methods and instruments, such as corneal topography, manual and optical keratometers, were used to measure the keratometry readings as they showed variability. We decided to take the K-reading from the Pentacam device as it has maximum repeatability in corneal ectasia.10 Because of the enlarged anteroposterior length of the globe, axial length measurement was also tricky. The optical biometer was unable to measure the axial length, so we used ultrasound-based axial length measurement. Regarding the IOL power calculation formula, we subjected these values to different formulae and decided to choose Barrett Universal formula II. The main issue in our case was that none of the formulae accepts keratometry readings greater than 60 D. We kept the 60 D value in one axis (instead of 63 D of our case) and obtained an IOL power of −6 D for emmetropia. Subjecting the formula to 57 D in that axis, with the other parameters kept the same, we obtained an IOL power of −3 D. So, keeping in mind this adjustment, we took an approximate value of −9 D IOL power for emmetropia. But, we also know that in cases of corneal ectasia, there is an inclination to a postoperative hyperopia as biometry usually overestimates the corneal power. Thus, the calculated emmetropic power was increased by 2 D to deliver postoperative myopia. The final power of the IOL implanted in the patient was –7 D. Still, we obtained a postoperative hyperopic shift of +1.5 D. The final refractive result revealed an undercorrection of 2 D, as we aimed for at least 0.5 D myopia postoperatively. We believe that in severe corneal ectasias, such as in our case, there are multiple sources of biometric errors and the IOL calculation can be unpredictable. Nevertheless, the refractive result was acceptable to the patient and she was satisfied with the visual outcome.11
Phacoemulsification surgery too is not straightforward in such cases and intraoperative surgical modifications are essential. Although the surgeon’s preferred practice is clear corneal incision, he chose a superior scleral tunnel to avoid the thin peripheral cornea and intraoperative corneal distortion.12 After the initial chop, the cataractous segments were luxated in the anterior chamber. The bottle height was kept low and emulsification was performed with less phaco power to avoid any damage to the lens zonules and endothelium. To avoid any wound leaks, the main incision was sutured at the end of the surgical procedure.
Postoperatively, glasses were prescribed as visual aids as well as for protection of the cornea. Even if a patient is emmetropic, protective glasses are advisable as the corneas of these eyes usually run the risk of corneal perforation or rupture due to trivial trauma. Counseling of these patients is very important regarding the use of protective glasses and avoidance of contact sports and trauma to the eye.
Value Statement
What Was Known
- Keratoglobus is an extreme form of corneal ectasia that is rarely seen.
- Cataract surgery in such cases is quite challenging. However, there is a paucity of literature regarding the same, particularly in cases of advanced ectasias.
What This Paper Adds
- This case helps in understanding the challenges of cataract surgery and intraocular lens selection in advanced keratoglobus.
- Preoperative planning, intraoperative surgical modifications and postoperative rehabilitation are the keys to achieving an optimal outcome while avoiding complications and refractive surprises.
Ethics and Consent
The patient has provided informed consent and has given consent to publish. Bharti Eye Foundation ethics board committee reviewed and approved the study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Cavara V. Keratoglobus and keratoconus: a contribution to the nosological interpretation of keratoglobus. Br J Ophthalmol. 1950;34(10):621–626. doi:10.1136/bjo.34.10.621
2. Nelson ME, Talbot JF. Keratoglobus in Rubinstein-Taybi syndrome. Br J Ophthalmol. 1989;73(5):385–387. doi:10.1136/bjo.73.5.385
3. Koenekoop RK. An overview of leber congenital amaurosis: a model to understand human retinal development. Surv Ophthalmol. 2004;49(4):379–398. doi:10.1016/j.survophthal.2004.04.003
4. Jacobs DS, Green WR, Maumenee AE. Acquired keratoglobus. Am J Ophthalmol. 1974;77(3):393–399. doi:10.1016/0002-9394(74)90747-8
5. Karabatsas CH, Cook SD. Topographic analysis in pellucid marginal corneal degeneration and keratoglobus. Eye. 1996;10(4):451–455. doi:10.1038/eye.1996.99
6. Bromley JG, Randleman JB. Treatment strategies for corneal ectasias. Curr Opin Ophthalmol. 2010;21(4):255–258.
7. Ghiasian L, Abolfathzadeh N, Manafi N, Hadavandkhani A. Intraocular lens power calculation in keratoconus; a review of literature. J Curr Ophthalmol. 2019;31(2):127–134. doi:10.1016/j.joco.2019.01.011
8. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/S0039-6257(97)00119-7
9. Gupta N, Ganger A. Keratoglobus: a close entity to megalophthalmos. SpringerPlus. 2016;5(1):634. doi:10.1186/s40064-016-2307-1
10. Hashemi H, Yekta A, Khabazkhoob M. Effect of keratoconus grades on repeatability of keratometry readings: comparison of 5 devices. J Cataract Refract Surg. 2015;41(5):1065–1072. doi:10.1016/j.jcrs.2014.08.043
11. Watson MP, Anand S, Bhogal M, et al. Cataract surgery outcome in eyes with keratoconus. Br J Ophthalmol. 2014;98(3):361e364. doi:10.1136/bjophthalmol-2013-303829
12. Ku JY, Grupcheva CN, Fisk MJ, McGhee CN. Keratoglobus and posterior subcapsular cataract: surgical considerations and in vivo microstructural analysis. J Cataract Refract Surg. 2004;30(1):237–242. doi:10.1016/S0886-3350(03)00644-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.