")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
Hyperlipidemia in COPD is associated with decreased incidence of pneumonia and mortality: a nationwide health insurance data-based retrospective cohort study
Received 17 December 2015
Accepted for publication 14 March 2016
Published 18 May 2016 Volume 2016:11(1) Pages 1053—1059
DOI https://doi.org/10.2147/COPD.S102708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Ming-Chen Chan,1–3 Ching-Heng Lin,4 Yu Ru Kou1
1Institute of Physiology, National Yang-Ming University, Taipei, 2Division of Chest Medicine, Department of Internal Medicine, Taichung Veterans General Hospital, 3College of Nursing, Central Taiwan University of Science and Technology, 4Department of Medical Research, Taichung Veterans General Hospital, Taichung, Taiwan
Purpose: COPD is often associated with various comorbidities that may influence its outcomes. Pneumonia, cardiovascular disease (CVD), and cancer are the major causes of death in COPD patients. The objective of this study is to investigate the influence of comorbidities on COPD by using the Taiwan National Health Insurance database.
Patients and methods: We retrospectively analyzed the database in 2006 of one million sampling cohort. Newly diagnosed patients with COPD with a controlled cohort that was matched by age, sex, and Charlson comorbidity index (CCI) were included for analysis.
Results: In total, 1,491 patients with COPD were included for analysis (61.8% male). Patients with COPD had higher incidences of pneumonia (25.7% vs 10.4%; P<0.0001), CVD (15.1% vs 10.5%; P<0.0001), and mortality rate (26.6% vs 15.8%; P<0.001) compared with the control group in the 4-year follow-up. In patients with COPD, CCI ≥3 have a higher incidence of pneumonia (hazard ratio [HR] 1.61; 95% confidence interval [CI] 1.23–2.09; P<0.0001), CVD (HR 1.73; 95% CI 1.24–2.41; P=0.001), and mortality (HR 1.12; 95% CI 1.12–1.83; P=0.004). Among the major comorbidities of COPD, hyperlipidemia was associated with decreased incidence of pneumonia (HR 0.68; 95% CI 0.5–0.93; P=0.016) and mortality (HR 0.64; 95% CI 0.46–0.90; P=0.009), but was not associated with increased risk of CVD (HR 1.10; 95% CI 0.78–1.55; P=0.588).
Conclusion: Our results demonstrate that COPD is associated with increased incidence of pneumonia, CVD, and mortality. In patients with COPD, higher CCI is associated with increased incidence of pneumonia, CVD, and mortality. However, COPD with hyperlipidemia is associated with decreased incidence of pneumonia and mortality.
Keywords: COPD, hyperlipidemia, pneumonia, mortality
Introduction
COPD is one of the major public health problems in modern society caused mainly by cigarette smoking, and its importance is increasing.1,2 COPD is a complex, heterogeneous, multicomponent disease with great variations in its clinical, radiological, and functional aspects.3 It has a variety of systemic manifestations and thus the current guideline recommends a multidirectional strategy in diagnosis, treatment, and prevention of COPD.4
COPD is often associated with a variety of comorbidities, including cardiovascular disease (CVD), malignancy, anxiety, depression, chronic renal failure, and infection.5–10 Comorbidities of COPD also have important impacts on major outcomes, including quality of life,11 rate of acute exacerbation,12 and mortality.13 Both COPD14,15 and coronary artery disease16 are characterized by low-grade systemic inflammation, which is manifested by increased levels of inflammatory biomarkers. Patients with COPD are at increased risk of hospitalization and mortality due to CVD.17,18 Moreover, patients with more severe COPD have higher cardiovascular mortality and morbidity than those with less severe COPD.19 Although obesity and hyperlipidemia are both risk factors of CVD,20 patients with COPD tend to have lower body mass index (BMI) and are less likely to have hyperlipidemia.21 Most comorbidities are associated with increased risk of mortality in patients with COPD, but in an observational study, the prevalence of hyperlipidemia is higher in survivors than non-survivors.22 Furthermore, as BMI is one of the composite factors of BODE (body mass index, airflow obstruction, dyspnea, and exercise capacity) index score, patients with COPD having lower BMI are associated with increased risk of death.23,24 Thus, the impact of hyperlipidemia on clinical outcomes of patients with COPD is complex and unclear.
The aim of this study is to use nationwide, 5-year population-based data to examine the relationship of major comorbidities on outcomes of COPD, with special interest on hyperlipidemia.
Materials and methods
Study population and design
The National Health Research Institutes, Taiwan, maintains the National Health Insurance Research Database (NHIRD) and authorizes its use for research purposes. We obtained a subset of the NHIRD with one million random subjects, accounting for ~5% of all subjects enrolled in the National Health Insurance program. There were no statistically significant differences in age, sex, or health care costs between the sample group and all enrollees (data not shown). The database contains medical claims information regarding ambulatory care, inpatient care, dental services, and prescription drugs as well as insurance data from all subjects between January 1996 and December 2009.25 The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding system was incorporated into the data from the beginning of 2000 and was used in this study.
The study was conducted by a retrospective, matched cohort design. Patients with COPD were included if they fulfilled the following criteria: 1) new diagnosis of COPD in the year 2006; 2) older than 40 years of age at the time of diagnosis of COPD; 3) at least three outpatient visits with COPD medication prescription or admission once with main diagnosis of COPD; 4) were prescribed COPD medication, including inhaled short- and long-acting bronchodilators, inhaled corticosteroids or corticosteroid/long-acting β-agonist combination; 5) lack of diagnosis of cancer, CVD, and COPD from 2000 to 2006. The patients were matched to non-COPD patients by age in 2006, sex, and Charlson comorbidity index (CCI) of 2005 in a 1:1 fashion (Figure 1). COPD was defined by ICD-9-CM codes 491 (chronic bronchitis), 492 (emphysema), and 496 (chronic airway obstruction, not elsewhere classified). Major outcomes of COPD, including pneumonia, CVD, cancer, and death were recorded by NHIRD from 2006 to 2009. Cancer was defined by ICD-9-CM codes 140 to 208; pneumonia was defined by ICD-9-CM codes 480 to 486 as the main diagnosis of admission; CVD was defined by ICD-9-CM codes 390 to 438 as the main diagnosis of admission.
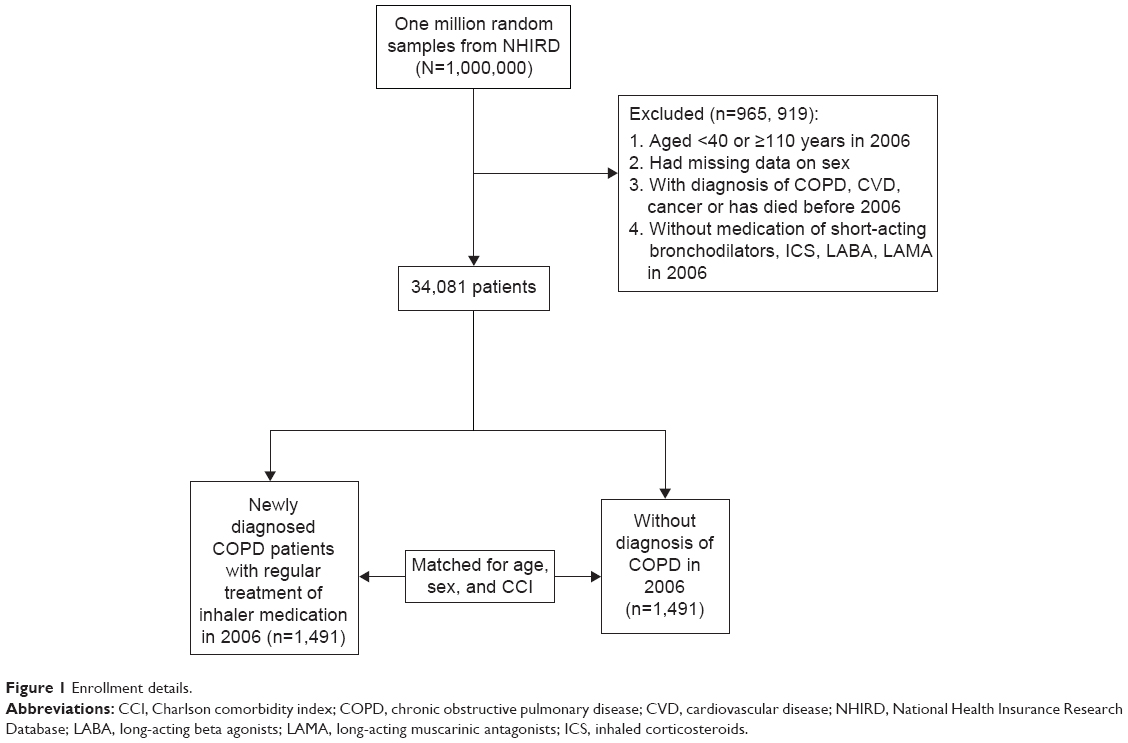 | Figure 1 Enrollment details. |
The major comorbidities, including hypertension (ICD-9- CM codes 401 to 405), hyperlipidemia (ICD-9-CM code 272), diabetes (ICD-9-CM codes 250), chronic renal disease (ICD-9-CM codes 403, 404, 581 to 583, and 585 to 588), and CVD (ICD-9-CM codes 390 to 438) were recorded from inpatient and outpatient database from January 1, 2006 to December 31, 2009. As the NHRI made the claim data available in an anonymous format which provided the individuals cannot be identified individually, retrospective studies do not need ethical approval from ethics committees in Taiwan.
Statistical methods
Differences in characteristics of subjects with and without COPD according to age, sex and clinical comorbidities, incidence of pneumonia, CVD, cancer, and death were examined using chi-squared tests for categorical variable and Student’s t-test for continuous variables. The Kaplan–Meier curve and log-rank test were used to examine the difference in the mortality between patients with COPD with and without hyperlipidemia. The crude and age-, sex-, and CCI- adjusted hazard ratio (HR) in COPD subjects with pneumonia, acute exacerbation of COPD (AECOPD), CVD, cancer, and mortality were calculated. The rate ratio and 95% confidence interval (CI) were also calculated. Multivariate Cox proportional hazards models were used to explore the relationship between hyperlipidemia and mortality, adjusted for age, sex, and comorbidities. The proportional hazards assumption was tested graphically and by including the interaction of time with each covariate. All statistical tests were two-sided, and a P-value of 0.05 was considered significant. All analyses were performed using SAS software, version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic and clinical characteristics of the study subjects
In total, 2,982 subjects, comprising of 1,491 COPD and 1,491 non-COPD with matched age, sex, and CCI, were included for analysis (Table 1). Patients with COPD had a higher risk of developing pneumonia (25.7% vs 10.4%; P<0.0001), CVD (15.1% vs 10.5%; P<0.0001), and rate of mortality (26.6% vs 15.5%; P<0.0001) over the next 4 years. There was no difference for risk of malignancy.
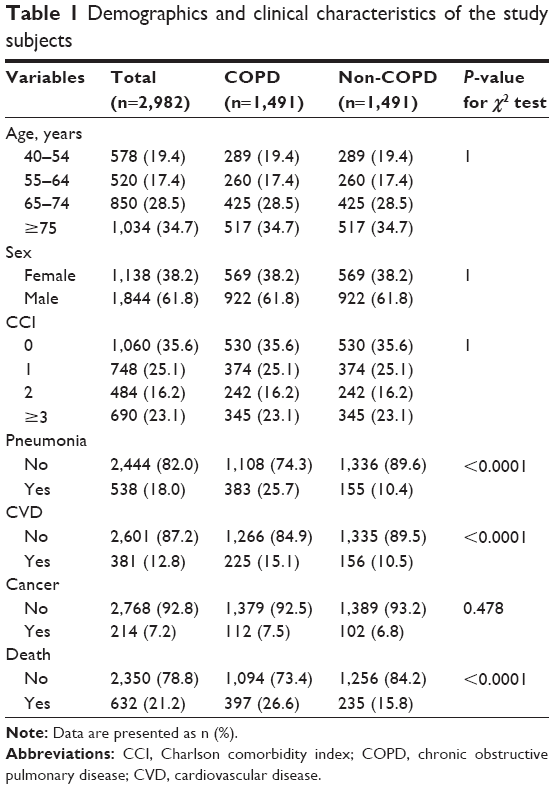 | Table 1 Demographics and clinical characteristics of the study subjects |
Impact of age, sex, and CCI on major outcome of COPD
Age was associated with increased HR of COPD-related outcomes, including pneumonia (HR 1.57; 95% CI 1.44–1.72; P<0.0001), AECOPD (HR 1.34; 95% CI 1.24–1.44; P<0.0001), CVD (HR 1.53; 95% CI 1.45–1.72; P<0.0001), malignancy (HR 1.17; 95% CI 1.00–1.34; P=0.044), and mortality (HR 2.04; 95% CI 1.85–2.24; P<0.0001) (Table 2). Male sex was associated with increased risk of pneumonia (HR 1.56; 95% CI 1.25–1.94; P<0.0001), AECOPD (HR 1.83; 95% CI 1.50–2.24; P<0.0001), malignancy (HR 1.70; 95% CI 1.12–2.53; P=0.013), and mortality (HR 1.46; 95% CI 1.18–1.80; P=0.001) over the next 4 years. CCI >3 was associated with increased risk of pneumonia (HR 1.61; 95% CI 1.23–2.09; P<0.0001), CVD (HR 1.73; 95% CI 1.24–2.41; P=0.001), and mortality (HR 1.43; 95% CI 1.12–1.83; P=0.004) over the next 4 years compared with CCI=0.
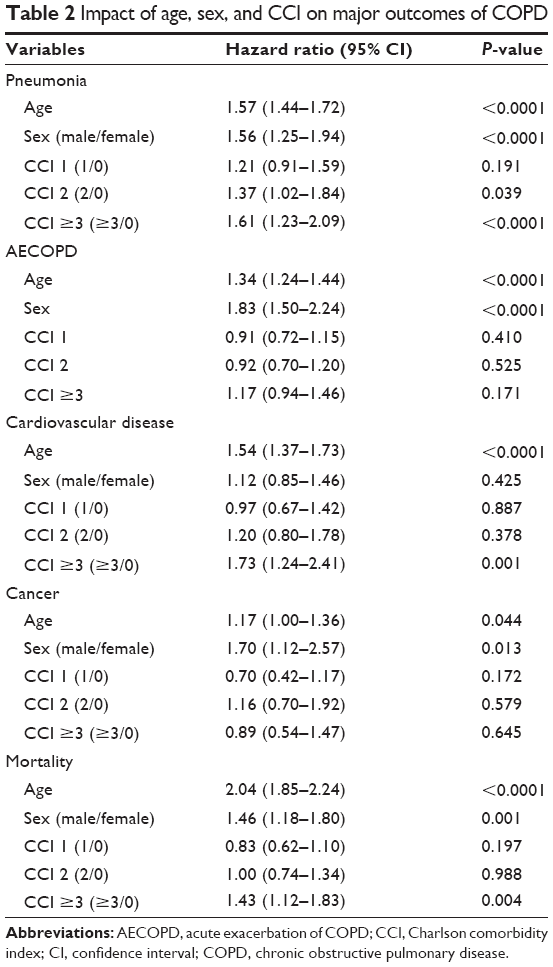 | Table 2 Impact of age, sex, and CCI on major outcomes of COPD |
Impacts of major comorbidities on outcomes of COPD
We further investigated the association between major comorbidities and COPD outcome. Age and sex remained important determinants in developing major comorbidities over the next 4 years (Table 3). Hyperlipidemia was associated with decreased risk of pneumonia (HR 0.68; 95% CI 0.49–0.93; P=0.016), but was not associated with increased risk of CVD (HR 1.09; 95% CI 0.77–1.53; P=0.641). Hyperlipidemia was also associated with decreased risk of mortality (HR 0.62; 95% CI 0.44–0.87; P=0.005). However, diabetes was associated with increased risk of pneumonia (HR 1.37; 95% CI 1.05–1.79; P=0.019), and CVD (HR 1.66; 95% CI 1.20–2.30; P=0.002). Patients with COPD having chronic renal disease (HR 1.66; 95% CI 1.20–2.30; P=0.002) and CVD (HR 1.94; 95% CI 1.23–3.07; P=0.005) were associated with increased mortality.
 | Table 3 Impacts of major comorbidities on outcomes of COPD |
We used Kaplan–Meier survival estimates to compare survival between hyperlipidemia and non-hyperlipidemia in patients with COPD. With regard to the mortality for the 4-year follow-up period, patients with hyperlipidemia were associated with better survival by the log-rank test (Figure 2, P<0.01).
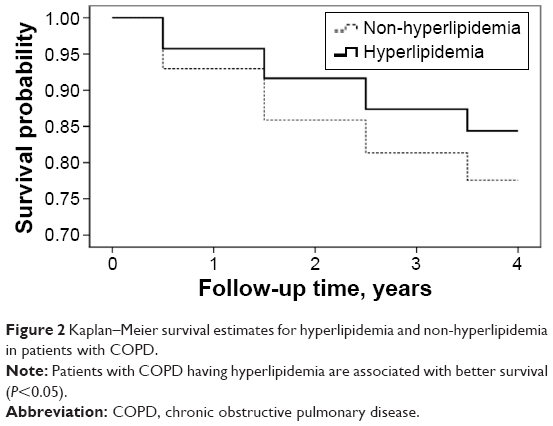 | Figure 2 Kaplan–Meier survival estimates for hyperlipidemia and non-hyperlipidemia in patients with COPD. |
Discussion
Our results demonstrate that COPD was associated with increased incidence of pneumonia, CVD, and mortality compared with matched subjects. CCI >3 was associated with increased risk of pneumonia, CVD, and mortality in patients with COPD. Among these comorbidities, patients with COPD patients having hyperlipidemia had lower incidence of pneumonia and mortality.
COPD continued to be one of the major threats to human health. In a previous analysis of national mortality and population data of Taiwan, it was found that the mortality rate for COPD increased gradually in the 1990s.26 But the mortality rate of COPD is probably underestimated, as COPD is often underreported on death certificates.27 On comparison with matched control subjects, we found that patients with COPD have increased risk of developing pneumonia, CVD, and mortality. Aging is a worldwide health care problem in the modern society and our results show that age is an independent risk factor for comorbidities and major COPD outcomes. COPD is often associated with a variety of comorbidities and its relationship is complex.28 COPD should be considered as a component of multimorbidity and some common pathways of pathogenesis are suggested.29 Current COPD treatments, both pharmacological30 and nonpharmacologial31,32 interventions, can effectively improve lung function, relieve symptoms, prevent exacerbation, and improve quality of life. However, there is an urgent need for treatment to prevent mortality.33,34 Our results once again highlight the association between COPD and comorbidities and thus suggest appropriate managements and prevention of comorbidities that could possibly be the key toward reducing mortality in COPD.
CVD is the leading cause of mortality and hospital admission in COPD patients.35 Long-term use of pharmacological treatment with bronchodilators, including β-2 agonists and anticholinergic agents, may be associated with increased risk to develop cardiovascular complications.23,36–39 Although hyperlipidemia is a well-known risk factor of CVD, our results show that the incidence of CVD was not increased in patients with COPD having hyperlipidemia. On the contrary, the incidence of pneumonia and mortality was lower in patients with COPD having hyperlipidemia. Malnutrition is common in patients with COPD because of increased energy expenditure and decreased intake. The adipose tissue is involved in the development of systemic inflammation of CVD by releasing a wide variety of substances called adipokines.40,41 Dysregulation of adipokines, including leptin and adiponectin with proinflammatory and anti-inflammatory activities, may contribute to the development of systemic inflammation in COPD.42 Since COPD is a heterogeneous disease with different pathogenesis and phenotypes, efforts should be made to clarify the relationship between COPD and hyperlipidemia, from basic science to bedside practice.
Statins are lipid-lowering agents that have been widely used to treat hyperlipidemia and astherosclerotic disease. In addition to lipid-lowering activity, statin has anti-inflammatory, antifibrotic, and immunomodulation effects.43 In an animal study, simvastatin could ameliorate the structural and functional derangements of the lungs caused by cigarette smoking through reduction of chemokines and metalloproteinases.44 Previous studies have also shown that the use of statin has a beneficial impact on improved airflow limitation,45 lower risk of AECOPD,46 and improved survival after exacerbation in patients with COPD.47,48 However, most of these published studies have inherent methodological limitations due to retrospective studies or population-based analyses. So, there is a need for prospective interventional trials designed specifically to assess the impact of statins on clinically relevant outcomes in COPD.
Strengths and limitations
Investigation of clinical problems by using public health data has the following strengths. First, it includes a large population. Second, it is a real-life data without restrictions in age, economic status, races, concomitant drug treatments, comorbidities, and possibly is more clinical relevant. However, our study may have the following limitations. First, the data is primarily based on financial claims and its quality is questionable in some aspects. Social and behavior characteristics (such as smoking status) and COPD severity are not available. In order to assure the accuracy of diagnosis, we included newly diagnosed patients with COPD on regular treatment with inhaler medication because their claims had been carefully inspected and the diagnosis was supported by laboratory data. Second, although a matched control group was selected for comparison, there could still be possible unknown confounding factors. Third, the diagnosis of the comorbidities, including hyperlipidemia, listed in this study was not confirmed by laboratory and image data.
Conclusion
In conclusion, by using a nationwide health insurance database, this retrospective analysis demonstrates that patients with COPD with hyperlipidemia is not associated with increased incidence of CVD, but is associated with decreased risk of having pneumonia and death. Further investigation, from basic science to clinical investigation, is warranted to clarify the impact of hyperlipidemia on the outcome of COPD.
Acknowledgments
This study was supported by a grant (MOST 104-2320-B-010-014-MY3) from Ministry of Science and Technology, Taiwan. This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes (registration number 99278). The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
The abstract of this paper was presented at the American Thoracic Society 2013 International Conference, May 17–22, Philadelphia, Pennsylvania, as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in American Journal of Respiratory and Critical Care Medicine, Vol 187, Meeting Abstracts, 2013.
Author contributions
M-CC, C-HL and YRK contributed to conception and design of the study. M-CC and C-HL drafted the manuscript and performed statistical analysis. M-CC, C-HL and YRK made critical revisions to the manuscript and gave final approval of the version to be published.
Disclosure
The authors report no conflicts of interest in this work.
References
Chen JC, Mannino DM. Worldwide epidemiology of chronic obstructive pulmonary disease. Curr Opin Pulm Med. 1999;5:93–99. | ||
Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349:1498–1504. | ||
Shirtcliffe P, Weatherall M, Travers J, Beasley R. The multiple dimensions of airways disease: targeting treatment to clinical phenotypes. Curr Opin Pulm Med. 2011;17:72–78. | ||
Global Strategy for Diagnosis, Management, and Prevention of COPD – 2016. Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2016. Available from: http://www.goldcopd.com/. Accessed Feb 17, 2016. | ||
Tantucci C. COPD and osteoporosis: something more than a comorbidity. Endocrine. 2012;42:5–6. | ||
Sethi S. Infection as a comorbidity of COPD. Eur Respir J. 2010;35:1209–1215. | ||
Incalzi RA, Corsonello A, Pedone C, Battaglia S, Paglino G, Bellia V; Extrapulmonary Consequences of COPD in the Elderly Study Investigators. Chronic renal failure: a neglected comorbidity of COPD. Chest. 2010;137:831–837. | ||
van den Bemt L, Schermer T, Bor H, et al. The risk for depression comorbidity in patients with COPD. Chest. 2009;135:108–114. | ||
Carratu P, Resta O. Is obstructive sleep apnoea a comorbidity of COPD and is it involved in chronic systemic inflammatory syndrome? Eur Respir J. 2008;31:1381–1382. | ||
Mannino DM, Aguayo SM, Petty TL, Redd SC. Low lung function and incident lung cancer in the United States: data from the First National Health and Nutrition Examination Survey follow-up. Arch Intern Med. 2003;163:1475–1480. | ||
van Manen JG, Bindels PJ, Dekker FW, et al. The influence of COPD on health-related quality of life independent of the influence of comorbidity. J Clin Epidemiol. 2003;56:1177–1184. | ||
Terzano C, Conti V, Di Stefano F, et al. Comorbidity, hospitalization, and mortality in COPD: results from a longitudinal study. Lung. 2010;188:321–329. | ||
Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28:1245–1257. | ||
Stolz D, Christ-Crain M, Morgenthaler NG, et al. Copeptin, C-reactive protein, and procalcitonin as prognostic biomarkers in acute exacerbation of COPD. Chest. 2007;131:1058–1067. | ||
Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59: 574–580. | ||
Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med. 2004;350:1387–1397. | ||
Sidney S, Sorel M, Quesenberry CP Jr, DeLuise C, Lanes S, Eisner MD. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente Medical Care Program. Chest. 2005;128:2068–2075. | ||
Curkendall SM, DeLuise C, Jones JK, et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada cardiovascular disease in COPD patients. Ann Epidemiol. 2006;16:63–70. | ||
Curkendall SM, Lanes S, de Luise C, et al. Chronic obstructive pulmonary disease severity and cardiovascular outcomes. Eur J Epidemiol. 2006;21:803–813. | ||
Grundy SM, Cleeman JI, Daniels SR, et al; American Heart Association; National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–2752. | ||
Joo H, Park J, Lee SD, Oh YM. Comorbidities of chronic obstructive pulmonary disease in Koreans: a population-based study. J Korean Med Sci. 2012;27:901–906. | ||
Divo M, Cote C, de Torres JP, et al. Comorbidities and Risk of Mortality in Patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:155–161. | ||
Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:1005–1012. | ||
Cao C, Wang R, Wang J, Bunjhoo H, Xu Y, Xiong W. Body mass index and mortality in chronic obstructive pulmonary disease: a meta-analysis. PLoS One. 2012;7:e43892. | ||
National Health Insurance Research Database. Available from: http://nhird.nhir.org.tw/en/index/htm. Accessed April 18, 2016. | ||
Kuo LC, Yang PC, Kuo SH. Trends in the mortality of chronic obstructive pulmonary disease in Taiwan, 1981–2002. J Formos Med Assoc. 2005;104:89–93. | ||
Jensen HH, Godtfredsen NS, Lange P, et al. Potential misclassification of causes of death from COPD. Eur Respir J. 2006;28:781–785. | ||
Negewo NA, McDonald VM, Gibson PG. Comorbidity in chronic obstructive pulmonary disease. Respir Investig. 2015;53(6):249–258. | ||
Barnes PJ. Mechanisms of development of multimorbidity in the elderly. Eur Respir J. 2015;45:790–806. | ||
Woodruff PG, Agusti A, Roche N, Singh D, Martinez FJ. Current concepts in targeting chronic obstructive pulmonary disease pharmacotherapy: making progress towards personalized management. Lancet. 2015;385:1789–1798. | ||
Spruit MA, Pitta F, McAuley E, ZuWallack RL, Nici L. Pulmonary rehabilitation and physical activity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192:924–933. | ||
Farver-Vestergaard I, Jacobsen D, Zachariae R. Efficacy of psychosocial intervention on psychological and physical outcomes in chronic obstructive pulmonary disease: a systemic review and mega-analysis. Psychother Psychosom. 2015;84:37–50. | ||
Tashkin DP, Celli B, Senn S, et al; UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359:1543–1554. | ||
Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–789. | ||
Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE; Lung Health Study Research Group. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142:233–239. | ||
Cazzola M, Matera MG, Donner CF. Inhaled beta2-adrenoceptor agonists: cardiovascular safety in patients with obstructive lung disease. Drugs. 2005;65:1595–1610. | ||
Lee TA, Pickard AS, Au DH, Bartle B, Weiss KB. Risk for death associated with medications for recently diagnosed chronic obstructive pulmonary disease. Ann Intern Med. 2008;149:380–390. | ||
Macie C, Wooldrage K, Manfreda J, Anthonisen N. Cardiovascular morbidity and the use of inhaled bronchodilators. Int J Chron Obstruct Pulmon Dis. 2008;3:163–169. | ||
Singh S, Loke YK, Furberg CD. Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300:1439–1450. | ||
Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nat Rev Immunol. 2011;11:85–97. | ||
Ouchi N, Kihara S, Funahashi T, Matsuzawa Y, Walsh K. Obesity, adiponectin and vascular inflammatory disease. Curr Opin Lipidol. 2003;14:561–566. | ||
Breyer MK, Rutten EP, Locantore NW, Watkins ML, Miller BE, Wouters EF; CLIPSE Investigators (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints). Dysregulated adipokine metabolism in chronic obstructive pulmonary disease. Eur J Clin Invest. 2012;42:983–991. | ||
Liao JK, Laufs U. Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol. 2005;45:89–118. | ||
Lee JH, Lee DS, Kim EK, et al. Simvastatin inhibits cigarette smoking-induced emphysema and pulmonary hypertension in rat lungs. Am J Respir Crit Care Med. 2005;172:987–993. | ||
Bando M, Miyazawa T, Shinohara H, Owada T, Terakado M, Sugiyama Y. An epidemiological study of the effects of statin use on airflow limitation in patients with chronic obstructive pulmonary disease. Respirology. 2012;17:493–498. | ||
Blamoun AI, Batty GN, DeBari VA, Rashid AO, Sheikh M, Khan MA. Statins may reduce episodes of exacerbation and the requirement for intubation in patients with COPD: evidence from a retrospective cohort study. Int J Clin Pract. 2008;62:1373–1378. | ||
Soyseth V, Brekke PH, Smith P, Omland T. Statin use is associated with reduced mortality in COPD. Eur Respir J. 2007;29:279–283. | ||
Lawes CM, Thornley S, Young R, et al. Statin use in COPD patients is associated with a reduction in mortality: a national cohort study. Prim Care Respir J. 2012;21:35–40. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.