")
Back to Journals » Clinical Ophthalmology » Volume 14
Hybrid 23/27 Gauge Vitrectomy – Combining the Charm of 27G with the Efficacy of 23G
Authors Garweg JG , Ouassi D, Pfister IB
Received 8 October 2019
Accepted for publication 27 December 2019
Published 31 January 2020 Volume 2020:14 Pages 299—305
DOI https://doi.org/10.2147/OPTH.S233884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Justus G Garweg,1,2 Dean Ouassi,3 Isabel B Pfister1
1Swiss Eye Institute and Berner Augenklinik am Lindenhofspital, Bern, Switzerland; 2Department of Ophthalmology, Inselspital, Bern, Switzerland; 3Medical Faculty, University of Strasbourg, Strasbourg, France
Correspondence: Justus G Garweg
Berner Augenklinik am Lindenhofspital, Bremgartenstrasse 119, Bern CH - 3012, Switzerland
Tel +41 31 311 12 22
Email [email protected]
Background: Minimally invasive transconjunctival sutureless vitrectomy (MIVS) has evolved into the standard of care, smaller incisions thought to result in lower ocular surface trauma and shorter times to recovery. The currently most relevant limitations in macular surgery may be light intensity and 27G instrument stability. Therefore, we thought to compare standard 23 and 27G vitrectomy with a hybrid technique using one 23G and two 27G ports regarding surgical times and short-term outcomes.
Methods: This retrospective comparison included 90 single-center consecutive cases of eyes undergoing elective micro-invasive vitrectomy for epiretinal membranes or idiopathic macular holes between October 2017 and June 2018. The main criteria for the comparison were total surgical time as primary outcome parameter and treatment-demanding intra- and postoperative complications along with recovery of best-corrected visual acuity (BCVA) and central retinal thickness (CRT) from prior to surgery to 1 month thereafter as secondary parameters as independent parameters for the recovery from the pre-existing pathology and the surgical trauma.
Results: Surgical times were shorter with 23G and 23/27G compared to 27G (23G: 38.4± 13.1; 27G: 48.1± 15.3; 23/27G: 34.9± 9 mins; p=0.0005) with no differences in BCVA and CRT outcomes. Switching from 27G to a larger port size was not necessary in any instance. Cryotherapy was applied in 15%, 30%, and 22.5% to suspected retinal pathologies, beyond these, in 5%, 0%, and 7.5% for retinal tears. Four postoperative retinal detachments occurred (4.4%), one in the 23G and three in the 23/27G group requiring re-vitrectomy.
Conclusion: In this exploratory case series, 23/27G hybrid vitrectomy, combining the advantages of 23G and 27G techniques, resulted in shorter surgical times without evident disadvantages. The combination with cataract surgery was unproblematic.
Keywords: vitrectomy, hybrid, 27-gauge, surgical time, epiretinal membrane, inner limiting membrane, peeling
Introduction
Since its first description over a decade ago,1 minimally invasive transconjunctival sutureless vitrectomy (MIVS) has evolved into the standard of care2,3 even in complex retinal pathologies such as tractional diabetic retinal detachment4–8 or advanced proliferative vitreoretinopathy (PVR).9 Meanwhile, the combination of MIVS and small-incision phacoemulsification has become the standard of care in phakic eyes with coexisting cataract and retinal pathology10 allowing better access to the vitreal base and faster visual recovery without requiring a second operation after cataract progression.11,12 The 20-gauge (20G) standard of the 1980s and 1990s has gotten progressively smaller and is now routinely available as 27G mostly due to technical improvements such as the introduction of pneumatically driven single-use continuous flow dual blade cutters and the use of disposable instruments with material properties that allow precise control of shear forces.13 In addition to these technological cornerstones, a further improvement came through the introduction of trocar systems that reduce the risk of entry site breaks.1,14 An increased cutting speed as well as minimized tractional forces to the vitreal base and retinal periphery reduce the risk of postoperative retinal detachment despite shorter surgical times.2,3 As smaller sclerotomy size leads to lower surgical trauma to the ocular surface,15 efforts are underway to further reduce the size beyond 27G.13,16–18
Despite having theoretical advantages,18 27G vitrectomy has not generally been accepted as the new MIVS standard. This may be related to technical challenges resulting from the small opening of the cutter, namely detaching a strongly adherent vitreous, particularly in younger individuals, and cutting back the vitreal base. Despite recent improvements, the limited instrument stability may interfere with the mechanical force that can be applied to a stretched and adherent epiretinal membrane or to epi- and subretinal proliferations before they tear.7,16,19 From the authors’ own personal experience, the damage to the underlying inner retina appears to correlate – surgeon-related factors apart – with the design of the forceps tip and particularly the sharpness of the tip edges. This increased sharpness may also lead to focal trauma when picking tissue. Generally, the smaller the forceps diameter, the sharper the edges of the branches and the more likely they are to produce a cutting effect. This complicates the picking and lifting of stretched and thickened inner limiting membranes (ILM) from the inner retinal surface without inflicting grip damage and spot bleedings or even tearing the epiretinal membranes and the ILM, in particular, requiring repeated grasping with 27G instruments compared to 23G instrumentation.19 Smaller gauge vitrectomy extends the otherwise short peeling process which may increase surgical trauma to the macula with more spot hemorrhages indicating increased focal inner retinal stretching and damage, even with experienced surgeons. To address these issues, surgeons may need to switch to larger sclerotomy diameters intraoperatively (published values state that this occurs in 25% to 41% of very small incision surgeries).9,20,21 Despite reports that the problem of insufficient illumination, as a result of ever smaller diameters of optical fibers used, has been resolved through technical advances,2,17 others report an increased use of chandelier illumination in bimanual vitrectomy.17,22 To avoid having to switch sclerotomy diameters intraoperatively and optimize outcomes, some authors considered mixing different sizes of small gauge vitrectomy depending on the specific surgical needs.5,6,23
The performance of new developments in vitrectomy, namely smaller gauge instrumentation, must be compared to existing technologies with regard to vitrectomy duration and safety outcomes. The latter are particularly difficult to assess if the outcome affects macular structure rather than retinal stability, but in these cases, early recovery of visual acuity may be a qualified indicator of surgical trauma. In this study, we compare two standard vitrectomy techniques, namely 23 and 27G, to a hybrid technique using one 23G and two 27G ports. Vitrectomy was combined with small incision cataract surgery in phakic instances. The different techniques are compared using surgical times, intraoperative and early postoperative complications, and short-term visual and anatomical outcomes as the main criteria.
Methods
Our dataset consists of 153 consecutive eyes that underwent vitrectomy (MIVS) by the same surgeon in retrobulbar anesthesia in a single-center setting (Berner Augenklinik am Lindenhofspital, Bern, Switzerland) during an 8-month period that ended on June 4th, 2018. In phakic instances, MIVS was combined with small incision (2.2 mm) phacoemulsification and placement of an intraocular lens into a capsular bag.
Out of a total of 153 eyes operated in total during this period, 90 eyes (90 patients) received primary elective vitrectomy for a functionally relevant macular pathology, i.e., epiretinal membrane or macular hole, and were therefore included in this retrospective comparison, assigning them to three different groups based on the technique used in the procedure: (i) 23G (n=20), (ii) 27G (n=30), and (iii) 23/27G hybrid (n=40). These three procedures were combined with phacoemulsification in 13 (65%), 19 (63.3%), and 24 instances (60.0%), respectively. From all eyes, preoperative best-corrected Snellen visual acuity (BCVA) and OCT-quantified central retinal thickness (CRT) were recorded prior to surgery and again 1 month thereafter, along with the surgical time, intraoperative complications, and early postoperative complications during the first 6 months. For the purposes of our analysis, preoperative CRT measurements in eyes with macular holes (MH) were excluded from the analysis.
The remaining 63 eyes from our dataset of 153 cases were operated for retinal detachment (n=27), PVR-associated retinal re-detachment (n=13), silicone oil tamponade after PVR-associated retinal detachment (n=12), as well as PDR with or without vitreal hemorrhage and other retinal pathologies including myopic macular holes, reopened macular holes, non-diabetic vitreous hemorrhage, dropped nucleus and intraocular lens, inflammatory retinovascular proliferation-associated PVR, and subretinal hemorrhage (n=11). While these 63 cases were not included in the primary outcome assessment, they contributed to our overall experience from which we report our insights regarding technical recommendations and potential limitations of each of the three techniques.
We used 23-gauge standard and 27-gauge ultraspeed transformer microincisional vitrectomy surgery systems with a valved cannula,24 as well as commercially available double-cutting probes with constant flow properties25 at standard cutting rates of 2500 cpm (23G) and 8000 cpm (27G and 23/27G). The infusion heights were 80 cm (23G) and 100 cm (27G and 23/27G) while applying suctions of 250 mmHg (23G) and 400 mmHg (27G and 23/27G) using a Venturi pump system in combination with beveled 2-step Trocar systems for the sclerotomies.7 In the hybrid setup, one 23G instrument port was inserted at the right upper sclerotomy and two 27G ports were placed at the superior left and temporal inferior sclerotomies for 27G infusion and illumination. A DORC® Bright Star 27G illumination system was used as the main light source. All eyes received a complete vitrectomy including vitreous base resection under fluid and air, followed by indentation and application of cryotherapy to peripheral sites whenever the possibility of a break could not be fully excluded (suspected retinal break), e.g., in the presence of an intraretinal hemorrhage. Epiretinal membrane (ERM) and inner limiting membrane (ILM) peeling was affected in the area of the optic nerve head and the vessel arcades after staining of the membranes with trypan blue (Membrane Blue, DORC® Instruments, Zuidland, the Netherlands).
The primary endpoint was defined as the duration of MIVS. As there were cases when MIVS was combined with cataract surgery, we calculated the mean duration of these combined procedures and subtracted the mean duration of procedures that did not involve cataract surgery to obtain an estimate for the average surgical time of cataract procedures (8 mins) which could then be subtracted from the surgical time of the combined surgeries to obtain the surgical time of MIVS only. Change in visual acuity and OCT-based central foveal thickness (CRT) were chosen as the secondary endpoint. The intra- and postoperative complications (up to 6 months of follow up) were not compared statistically due to the small event numbers.
Complications arising and being uncovered during the full eye examination on day 1 to 1 month were registered. For the purpose of this study, we recorded any complications requiring treatment.
All patients were above 18 years of age at the time of sampling and had signed informed general consent approving the use of their coded data collected during their therapy at our institution and documented in the institutional eCRF for quality control and scientific purposes which was approved by the institutional ethics committee (Kantonale Ethik-Kommission Bern, registration numbers 152/08 and 2019–00651). The study strictly adhered to the tenets of the Declaration of Helsinki.
Statistics
For statistical purposes, best-corrected Snellen visual acuity (BCVA) was converted into ETDRS letter scores with 85 letters reflecting an angle of 1 arc minute or a BCVA of 20/20. Results are presented as mean values and one standard deviation. Since the data were not normally distributed, we used nonparametric tests for the analyses. The Wilcoxon sign-rank test was used to test for change over time within each group. For inter-group comparisons, we used the Kruskal–Wallis H-test based on a discrimination level of p<0.05 for statistical significance.
Results
All three groups had similar ages (23G: 71.6±8.4 years; 27G: 70.4±8.1 years; 23/27G: 70.3±6.3 years; p=0.68), gender distribution (p=0.84), and percentages of phakic eyes (23G: 65%; 27G: 63.3%; 23/27G: 60.0%; p=0.92). Surgical times were as follows: 23G: 38.4±13.1 (22–70) min; 27G: 48.1±15.3 (26–80) min; 23/27G: 34.9±9.6 (20–66) min (p=0.0005; Figure 1). The 23G and 23/27G groups showed statistically similar surgical times (p=1.0) and surgical times that were significantly shorter compared to the 27G group (23G vs 27G: p=0.047; 23/27G vs 27G; p=0.0005). This difference was not explained by a similar distribution of MH cases between the groups (6 in the 23G group (30.0%), 14 (46.7%) in the 27G group, and 13 (32.5%) in the 23/27G). Neither visual acuity at any point of time (Figure 2), nor visual gain after 1 month (23G: 12.3 letters; 27G: 8.8 letters; 23/27G: 11.6 letters; p=0. 48) differed between the groups. Due to censoring preoperative CRT values in instances with macular holes and an uneven distribution of eyes with macular holes among the groups, the preoperative CRT readings were comparable (p>0.05) but postoperatively they differed significantly 1 month after surgery (p=0.029).
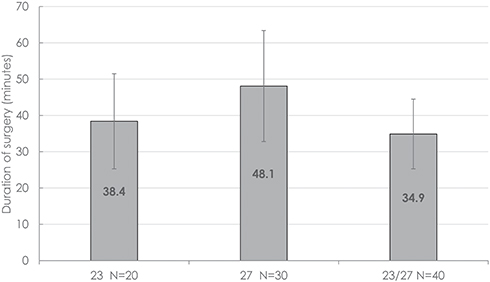 |
Figure 1 23G versus 27G and hybrid 23/27G minimally invasive vitrectomy: surgical times for vitrectomy (those procedures that had been combined with cataract surgery were included after subtracting the estimated average duration of 8 mins for cataract component). |
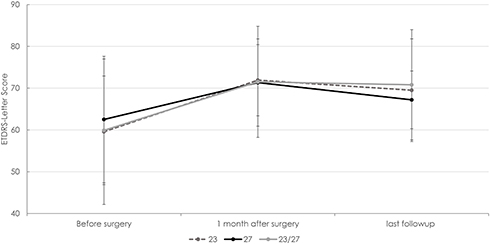 |
Figure 2 23G versus 27G and hybrid 23/27G minimally invasive vitrectomy: evolution of best-corrected visual acuity from before until 1 month after surgery. There were no significant differences between the groups. |
Switching from 27G to a larger port size or suturing of sclerotomies was not necessary in any instance. Seventy percent of 27G and 23/27G as well as 80% of 23G procedures were without complications. Early postoperative hypotony or bleeding or fibrin exudation were never recorded. Of a total of four postoperative retinal detachments (4.4%), two were recurrences of intraoperatively treated beginning detachments in cases of a taut vitreal base in macular holes, one was associated with a capsular rupture during lens replacement, and one newly developed (Table 1). In addition, one persistent macular hole required re-vitrectomy 2 months after the primary surgery (23G group) and one choroidal neovascularisation newly developed 2 months after surgery with preoperative high-risk dry AMD and extensive epiretinal fibrosis.25
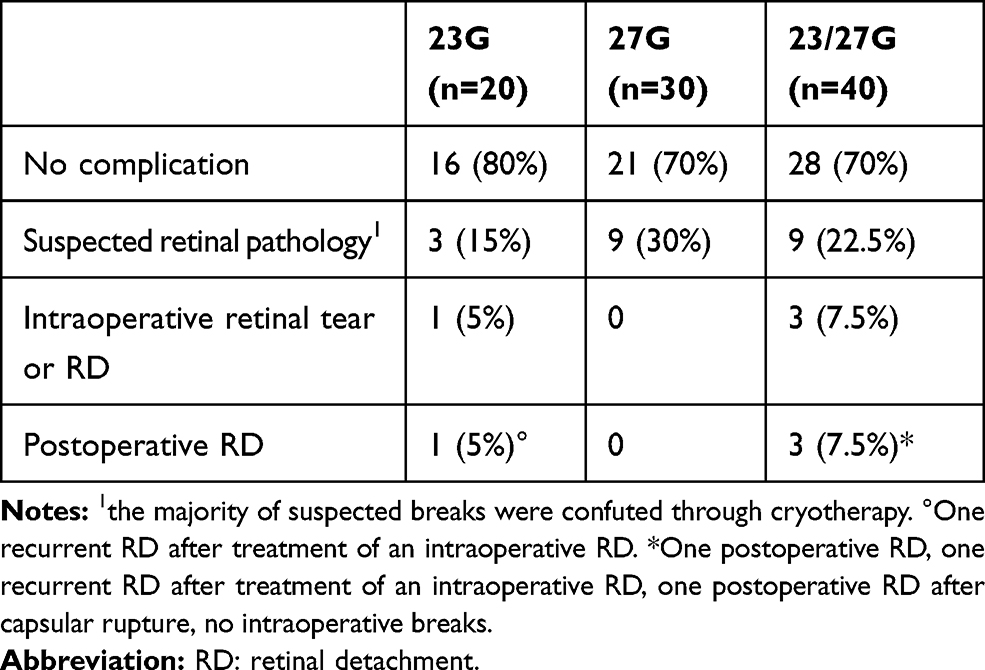 |
Table 1 23G versus 27G and Hybrid 23/27G Minimally Invasive Vitrectomy: Intra- and Early Perioperative Complications |
No severe inflammation was recorded. Sclerotomy leakage was regularly present on day 1, but never required suturing. IOP was usually low but did not need treatment in any instance. No major intraocular hemorrhage (i.e. not spontaneously resolving within 1 week) was noted. The majority of cases were hospitalized for 24 hrs after surgery and received a systematic pain prophylaxis with metamizole 1–2g during the first postoperative hours, but not thereafter, no patient required more than paracetamol 500-mg tablets after discharge from hospital.
Discussion
In this study, we report a direct comparison of surgical times, technical advantages, and challenges associated with the hybrid 23/27G vitrectomy technique compared to standard 23G and 27G procedures. The stiffness of the 23G Tano microforceps clearly facilitated a less traumatic peeling process compared to the more flexible and thus less precise disposable end-gripping 27G forceps, the higher flexibility of its light pipe and vitrectomy cutter may impede access to the vitreal base.
While the 23G vitrectomy technique was rapidly accepted after its introduction,26 25G, which was launched only a few years later, was not met with the same enthusiasm, and 27G, the most recent innovation, found even less approval among vitreoretinal surgeons, possibly due to the inherent limitations associated with this technique (material stability, limited light intensity and access to the vitreal base).27,28 Particularly, the light limitation problem is supported by findings that many surgeons who use the 27G technique still use a twin-light chandelier as an additional light source to achieve sufficient contrast and to allow bimanual working.10
The idea of combining different sclerotomy sizes is not new and was possibly motivated by the fact that small-size high-speed cutters tend to produce less vitreoretinal traction and thus carry a lower risk of inducing retinal breaks while allowing vitreous removal with high efficacy.14 The term “hybrid vitrectomy” was coined for the simultaneous use of sclerotomies of different diameters. This approach can utilize the strengths inherent to each technique while trying to minimize its known limitations. Initially, a combination of 20/23G hybrid technique was used,29 while combinations of 20/23G,23,29,30 20/25G,7,20 23/27G7 and 25/27G10,31 appeared later on for specific surgical situations. Based on our own clinical experience, we would estimate that the 23/27G technique can be used successfully in 90% of routine vitrectomies. To explore its technical advantages and limitations,27 we applied this hybrid technique to uncomplicated and PVR-complicated retinal detachment cases (40 eyes), silicone oil removal combined with membrane peeling (12 instances), and other indications such as retained lens fragment or IOL in combination with secondary IOL placement, tractional diabetic retinal detachment, and others (11 eyes). Compared to 23G, the 23/27G hybrid in our experience presented many advantages, while the presence of a 23G port reduced the limitations inherent in the pure 27G technique as was published before7 (Table 2). By using an external light source (Bright Star), the light was never limiting, and a chandelier illumination not required. Nevertheless, roughly 10% of light ducts had to be replaced due to low output without visible fiber breaks.
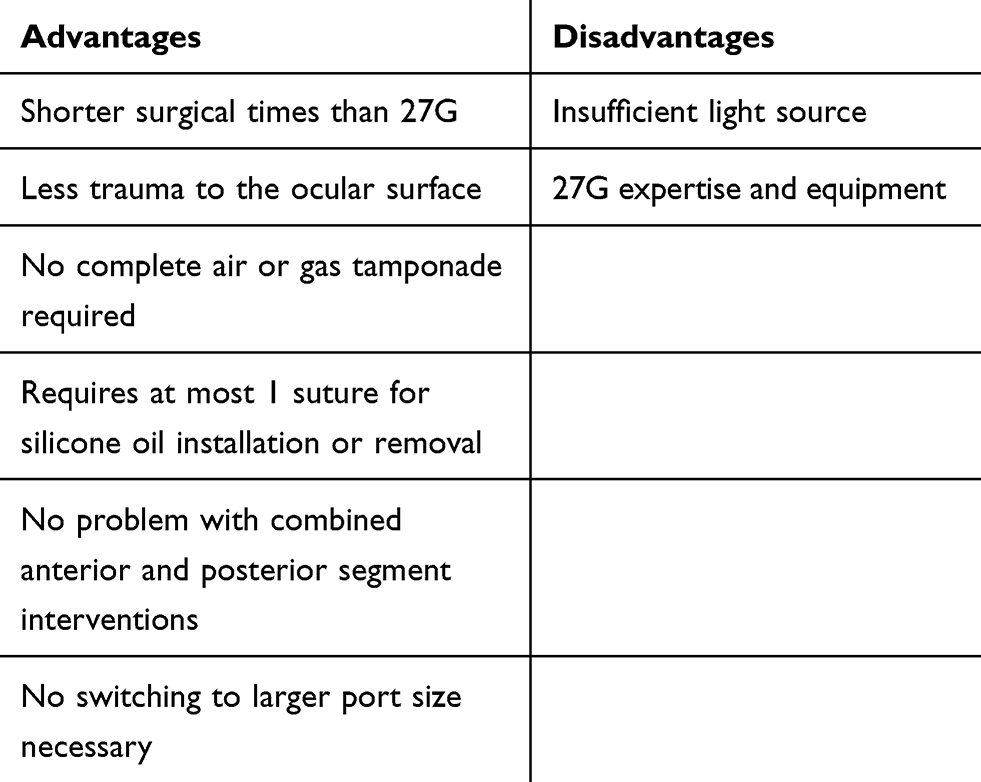 |
Table 2 Advantages Experienced with Hybrid 23/27G Vitrectomy Compared to 23G and 27G |
Apart from shorter surgical times, the main advantages that we perceived include the availability of optional partial gas or air filling and a smoother ocular surface with less subconjunctival gas and hemorrhaging on the first day, although perioperative patient discomfort and pain have never been an issue with the 23G technique.19 Particularly in cases requiring silicone oil instillation or removal, did we find the hybrid technique easy to use with only a single (23G) sclerotomy requiring suturing (Table 2).21 As a result, the benefit of this technique may, namely, be of interest for outpatient surgery. Based on a partial air or gas filling, none of the self-sealing angulated 27G sclerotomies required any suturing.18 While some authors suggested that air or gas filling may not always be required,32 we used it in all our procedures. We never had to switch to larger port sizes and adopting an infusion height of 100 cm proved to be helpful for achieving a stable intraoperative situation.33
One major disadvantage of the 27G technique is the lower stability of its light pipe and cutter, which limits access to and impedes complete removal of the vitreal basis. It is unclear whether this caused the increased need for cryotherapy in the 27G and 23/27G procedures (30% and 22.5% compared to 15% in the 23G group).34 As the number of confirmed breaks was not recorded, we cannot provide a more conclusive interpretation. Nevertheless, the incidence of anterior retinal pathologies requiring treatment concurs with several other reports using the 20G and 23G vitrectomy. We found two retinal detachments intraoperatively in the 23/27G group and three in the postoperative course (one of which a recurrence of an intraoperative detachment). Our overall rate of postoperative retinal detachments is again in good agreement with earlier reports.28,35 The primary intention of this retrospective pilot study was to assess the surgical efficacy despite complete vitreous removal including its base as far as possible. This retrospective analysis was by far underpowered to allow any comment on differences in the safety between the mentioned techniques.
In conclusion, the hybrid 23/27G vitrectomy technique appears to be a straightforward and highly efficacious technique that should be suitable for the vast majority of standard and complex vitreoretinal situations, including dropped nucleus or luxated intraocular lens and most tractional retinal detachments complicated by PVR and PDR. We found it to be the ideal compromise, facilitating short surgical times that are comparable to the 23G technique without any evident technical disadvantages. We would encourage industry partners to consider providing off-the-shelf mixed 23/27G packages in order to reduce the costs of this high-quality.
Disclosure
JGG is an adviser for several pharmaceutical companies (Alcon, Allergan, Bayer, Novartis) and participates in a number of international multicenter clinical studies in the fields of AMD and diabetic retinopathy that have received sponsors by industry partners (Novartis, Bayer). These activities had no bearing on the study that gave rise to the submitted article, for which JGG received neither direct nor indirect financial support; nor has he conflicts of interest with any of the presented data. The remaining authors report no potential conflicts of interest.
References
1. Aydin B, Dinç E, Yilmaz SN, et al. Retinal endoilluminator toxicity of xenon and light-emitting diode (LED) light source: rabbit model. Cutan Ocul Toxicol. 2014;33:192–196. doi:10.3109/15569527.2013.832282
2. Barthelmes D, Alexander S, Mitchell P, Chandra J. Hybrid 20/23-gauge pars plana vitrectomy for retained lens fragments after cataract surgery. Retina. 2012;32:1749–1755. doi:10.1097/IAE.0b013e3182453309
3. Cruz-Iñigo YJ, Berrocal MH. Twenty-seven-gauge vitrectomy for combined tractional and rhegmatogenous retinal detachment involving the macula associated with proliferative diabetic retinopathy. Int J Retina Vitreous. 2017;3:38. doi:10.1186/s40942-017-0091-x
4. de Oliveira PR, Berger AR, Chow DR. Vitreoretinal instruments: vitrectomy cutters, endoillumination and wide-angle viewing systems. Int J Retina Vitreous. 2016;2:28. doi:10.1186/s40942-016-0052-9
5. Dikopf MS, Patel KH, Setlur VJ, Lim JI. Surgical outcomes of 25-gauge pars plana vitrectomy for diabetic tractional retinal detachment. Eye (Lond). 2015;29:1213–1219. doi:10.1038/eye.2015.126
6. Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina. 2005;25:208–211. doi:10.1097/00006982-200502000-00015
7. Gozawa M, Takamura Y, Miyake S, et al. Comparison of subconjunctival scarring after microincision vitrectomy surgery using 20-, 23-, 25- and 27-gauge systems in rabbits. Acta Ophthalmol. 2017;95:e602–e609. doi:10.1111/aos.13459
8. Gupta D, Ching J, Tornambe PE. Clinically undetected retinal breaks causing retinal detachment: a review of options for management. Surv Ophthalmol. 2018;63:579–588. doi:10.1016/j.survophthal.2017.08.002
9. Höhn F, Kretz F, Pavlidis M. (2016): surgical and functional results of hybrid 25–27-gauge vitrectomy combined with coaxial 2.2 mm small incision cataract surgery. J Ophthalmol. 2016;2016:9186351. doi:10.1155/2016/9186351
10. Iwahashi-Shima C, Miki A, Hamasaki T, et al. Intraocular pressure elevation is a delayed-onset complication after successful vitrectomy for stages 4 and 5 retinopathy of prematurity. Retina. 2012;32:1636–1642. doi:10.1097/IAE.0b013e3182551c54
11. Khan MA, Kuley A, Riemann CD, et al. Long-term visual outcomes and safety profile of 27-gauge pars plana vitrectomy for posterior segment disease. Ophthalmology. 2018;125:423–431. doi:10.1016/j.ophtha.2017.09.013
12. Khan MA, Samara WA, Hsu J, Garg S. Short-term outcomes of hybrid 23-, 25-, and 27-gauge vitrectomy for complex diabetic tractional retinal detachment repair. Retin Cases Brief Rep. 2017;13:244–247. doi:10.1097/ICB.0000000000000571
13. Khanduja S, Kakkar A, Majumdar S, Vohra R, Garg S. Small gauge vitrectomy: recent update. Oman J Ophthalmol. 2013;6:3–11. doi:10.4103/0974-620X.111893
14. Lin X, Apple D, Hu J, Tewari A. Advancements of vitreoretinal surgical machines. Curr Opin Ophthalmol. 2017;28:242–245. doi:10.1097/ICU.0000000000000369
15. Mitsui K, Kogo J, Takeda H, et al. Comparative study of 27-gauge vs 25-gauge vitrectomy for epiretinal membrane. Eye (Lond). 2016;30:538–544. doi:10.1038/eye.2015.275
16. Mura M, Barca F. 25-Gauge vitrectomy. Dev Ophthalmol. 2014;54:45–53.
17. Oellers P, Stinnett S, Hahn P. Valved versus nonvalved cannula small-gauge pars plana vitrectomy for repair of retinal detachments with Grade C proliferative vitreoretinopathy. Clin Ophthalmol. 2016;10:1001–1006. doi:10.2147/OPTH.S104901
18. Oellers P, Stinnett S, Mruthyunjaya P, Hahn P. Small-gauge valved versus nonvalved cannula pars plana vitrectomy for retinal detachment repair. Retina. 2016;36:744–749. doi:10.1097/IAE.0000000000000762
19. Osawa S, Oshima Y. (2014): 27-Gauge vitrectomy. Dev Ophthalmol. 2014;54:54–62.
20. Rizzo S, Belting C, Genovesi-Ebert F, Di Bartolo E. Incidence of retinal detachment after small-incision, sutureless pars plana vitrectomy compared with conventional 20-gauge vitrectomy in macular hole and epiretinal membrane surgery. Retina. 2010;30:1065–1071. doi:10.1097/IAE.0b013e3181cd48b0
21. Rizzo S, Polizzi S, Barca F, Caporossi T, Virgili G. (2017): comparative study of 27-gauge versus 25-gauge vitrectomy for the treatment of primary rhegmatogenous retinal detachment. J Ophthalmol. 2017;2017:6384985.
22. Rizzo S, Savastano A, Finocchio L, Savastano MC, Khandelwal N, Agrawal R. Choroidal vascularity index changes after vitreomacular surgery. Acta Ophthalmol. 2018;96:e950–e955. doi:10.1111/aos.13776
23. Sato T, Emi K, Bando H, Ikeda T. Retrospective comparison of 25-gauge vitrectomy with 20-gauge vitrectomy in the repair of retinal detachment complicated with proliferative vitreoretinopathy. Nihon Ganka Gakkai Zasshi. 2012;116:100–107.
24. Shroff D, Gupta P, Gupta C, Atri N, Dutta R, Shroff C. Hybrid 20/23-G pars plana vitrectomy in endophthalmitis and trauma: a strategic approach. Eur J Ophthalmol. 2018;28:94–97. doi:10.5301/ejo.5000988
25. Song Y, Shin YW, Lee BR. Adjunctive use of a novel releasable suture technique in transconjunctival vitrectomy. Retina. 2011;31:243–249. doi:10.1097/IAE.0b013e3181e586ce
26. Stalmans P. 23-gauge vitrectomy. Dev Ophthalmol. 2014;54:38–44.
27. Tarantola RM, Tsui JY, Graff JM, et al. Intraoperative sclerotomy-related retinal breaks during 23-gauge pars plana vitrectomy. Retina. 2013;33:136–142. doi:10.1097/IAE.0b013e31825e1d62
28. Steel DH, Charles S. Vitrectomy fluidics. Ophthalmologica. 2011;226(Suppl 1):27–35. doi:10.1159/000328207
29. Teixeira A, Chong LP, Matsuoka N, et al. Vitreoretinal traction created by conventional cutters during vitrectomy. Ophthalmology. 2010;117(1387–92.e2). doi:10.1016/j.ophtha.2009.11.004
30. Theocharis IP, Alexandridou A, Gili NJ, Tomic Z. Combined phacoemulsification and pars plana vitrectomy for macular hole treatment. Acta Ophthalmol Scand. 2005;83:172–175. doi:10.1111/j.1600-0420.2005.00417.x
31. Thompson JT. Advantages and limitations of small gauge vitrectomy. Surv Ophthalmol. 2011;56:162–172. doi:10.1016/j.survophthal.2010.08.003
32. Tosi GM, Malandrini A, Cevenini G, et al. Vitreous incarceration in sclerotomies after valved 23-, 25-, or 27-gauge and nonvalved 23- or 25-gauge macular surgery. Retina. 2017;37:1948–1955. doi:10.1097/IAE.0000000000001445
33. Yamada K, Maeno T, Yamada M. Hybrid microincision vitrectomy surgery combined with 20-gauge silicone cannulas for use with 20-gauge horizontal scissors in diabetic tractional retinal detachment. Clin Ophthalmol. 2013;7:1559–1563. doi:10.2147/OPTH.S46486
34. Yonekawa Y, Thanos A, Abbey AM, et al. Hybrid 25- and 27-gauge vitrectomy for complex vitreoretinal surgery. Ophthalmic Surg Lasers Imaging Retina. 2016;47:352–355. doi:10.3928/23258160-20160324-08
35. Zehetner C, Moelgg M, Bechrakis E, Linhart C, Bechrakis NE. In vitro flow analysis of novel double-cutting, open-port, ultrahigh-speed vitrectomy systems. Retina. 2018;38:2309–2316. doi:10.1097/IAE.0000000000001882
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.