")
Back to Journals » International Journal of Women's Health » Volume 15
How to Support the Referral Towards Group Antenatal Care in Belgian Primary Healthcare Organizations: A Qualitative Study
Authors Talrich F, Van Damme A, Bastiaens HLA , Bergs J , Rijnders MEB , Beeckman K
Received 2 August 2022
Accepted for publication 17 November 2022
Published 6 January 2023 Volume 2023:15 Pages 33—49
DOI https://doi.org/10.2147/IJWH.S384269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Florence Talrich,1,2 Astrid Van Damme,1,2 Hilde LA Bastiaens,3 Jochen Bergs,4 Marlies EB Rijnders,5 Katrien Beeckman1,2,6
1Department of Public Health, Vrije Universiteit Brussel (VUB), Jette, Belgium; 2Departement of Nursing and Midwifery Research Group (NUMID), Universitair Ziekenhuis Brussel (UZ Brussel), Jette, Belgium; 3Department Family Medicine and Population Health, Universiteit Antwerpen, Antwerp, Belgium; 4Department of Healthcare, Universiteit Hasselt, Hasselt, Belgium; 5Department of Child Health, TNO, Leiden, the Netherlands; 6Department Nursing and Midwifery, Universiteit Antwerpen, Antwerp, Belgium
Correspondence: Florence Talrich, Laarbeeklaan 103, Brussel, Jette, 1090, Belgium, Tel +324749853, Email [email protected]
Introduction: Group Antenatal Care (GANC) is an alternative for traditional antenatal care. Despite the model is well accepted among participants and is associated with positive effects on pregnancy outcomes, recruitment of participants can be an ongoing challenge, depending on the structure and financing of the wider health system. This is especially the case for primary care organizations offering GANC, which depend on other health care providers to refer potential participants. The main objective of this study is to understand what determinants are at play for health care providers to refer to GANC facilitators in primary care organizations. Accordingly, we make recommendations for strategies in order to increase the influx of women in GANC.
Methods: Qualitative findings were obtained from 31 interviews with healthcare providers responsible for the referral of women to the GANC facilitators working in primary care organizations, GANC facilitators and stakeholders indirectly involved in the referral. The domains of the Consolidated Framework for Implementation Research (CFIR) and the Theoretical Domains Framework (TDF) helped to develop interview questions and raise awareness of important elements during interviews and thematic analyses.
Results: The findings show that before health care providers decide to refer women, they undergo a complex process that is influenced by characteristics of the potential referrer, GANC facilitator, woman, professional relationship between the potential referrer and the GANC facilitator, organization and broader context.
Discussion: Based on these findings and current literature, we recommend that the GANC team implements strategies that anticipate relevant determinants: identify and select potential referrers based on their likelihood to refer, select champions, invest in communication, concretise the collaboration, provide practical tools, involve in policymaking.
Keywords: antenatal care, CenteringPregnancy, group-based care, recruitment, primary healthcare
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Multazam has been published for this article.
Plain Language Summary
As a care provider, you might encounter challenges regarding the recruitment of participants for a specific program. This is no exception when recruiting for Group Antenatal Care (GANC), an alternative approach to maternity care. Primary care organizations face an even greater challenge in this regard. They have a smaller patient population and therefore depend on other health care providers who refer women. There is potential to optimize regarding the referral of women to GANC. Thus, it is useful to take a closer look at what drives or hinders health care providers to refer women in function of Group Antenatal Care. The researchers tried to answer this question based on interviews with health care providers. From these interviews and after analysis, we found that the decision making process of potential GANC referrers is complex and influenced by an interplay of factors relating to themselves; the GANC facilitators; their relevant organizations; and the potential GANC clients (pregnant women). Based on these findings and current literature, we recommend several strategies that may help to convince health care providers to refer. The team implementing Group Antenatal Care should:
- Identify and select potential referrers based on their likelihood to refer. If GANC facilitators first target potential referrers that are more likely to refer, they will achieve success in the shorter term. Those that are less likely to refer might follow on a longer term.
- Select champions (ie pioneers) within organizations. Champions are care providers who are more inclined towards GANC than other care providers in the organization. Champions can convince their colleagues more easily than GANC facilitators, as they are part of the same organization and may have more prestige.
- Invest in communication. The referral towards GANC facilitators is more appealing if its presentation is adapted to the potential referrer. Good communication throughout the collaboration is essential for the development of a professional relationship, which in turn is a prerequisite for successful referral.
- Solidify the collaboration. The GANC facilitator should identify the needs and protocols of all care providers involved and develop a care pathway in which the responsibilities and roles are clearly defined.
- Increase confidence among referrers by providing tools such as flyers and training.
- Involve in policymaking to remove contextual barriers, such as financial reimbursement of maternity care.
If GANC facilitators apply these strategies, they will improve referral rates and thus increase the chances of implementation-success.
Introduction
Group Antenatal Care (GANC) is a type of antenatal care (ANC) based on the CenteringPregnancy model.1,2 Health assessment, social support, and interactive learning are integrated and are the core of this model. The idea behind this model is that 8 to 12 women, with similar due dates, and optionally their significant others, form a support group attending a series of nine prenatal and one postnatal two-hour-sessions. During these sessions, a healthcare provider (eg, a midwife, general practitioner (GP), or obstetrician) conducts a health assessment, with the women actively participating in their follow-up through self-care (eg, measuring weight and blood pressure themselves). In addition, the group engages in a discussion facilitated by the healthcare provider, referred as GANC facilitator, and a co-facilitator. They encourage the group to share information and experiences on pregnancy-related topics (eg, breastfeeding, mental wellbeing, and family planning) using interactive methods.
Studies in different contexts and target groups have shown neutral or positive effects with regard to maternal and neonatal outcomes, compared to traditional individual ANC.3–5 Regarding satisfaction with care on the other hand, research shows that satisfaction is greater among women who receive GANC.3,6
GANC offers an alternative to traditional individual care, which is still the predominant model in most Western countries.7 Standard antenatal care entails individual visits with a healthcare provider, such as an obstetrician, a midwife, or a GP in a hospital or another clinical setting. On top of the beneficial impact of antenatal care on health outcomes, literature shows that some women desire more involvement, time, and focus on education and psychosocial wellbeing during their pregnancy.8–11 GANC can be an answer covering these demands and is currently offered in high-, middle-, and low-income countries.12–14 In Belgium, GANC is gaining momentum; it is currently being implemented in ten organizations. It is offered in both hospital and primary care settings (eg, independent midwife practices and community health centers). Moreover, the majority of these settings offer GANC primarily to psychosocially vulnerable women or have a patient population with a high degree of vulnerability.
Although the model is well accepted among participants and is associated with positive effects on pregnancy outcomes, a persisting challenge in the implementation of GANC is the recruitment and enrolling of participants.15–18 However, a sufficiently large group is needed for two main reasons: for cost effectiveness19 and to achieve effective group dynamics and cohesion.1
Firstly, while a cost-effectiveness study has not yet been conducted in Belgium, studies in other countries show that a group of 8 or more is necessary to be cost-effective.19 From this, we can conclude a small group implies less revenue for the organization, which may have a financial implication.
Secondly, group cohesion is an essential part and goal of the model.1 It is thought to be one of the psychological mechanisms that explains the improved outcomes and health behaviors among GANC-attendees.
To obtain an appropriate group size, the GANC organization must be able to recruit from a sufficiently large patient population. After all, not all women are willing or able to participate.20–22 In addition, not all women who accept to participate are included in the same group. This is because a group consists of women of similar gestational age, ensuring the topics of the sessions are adapted to the phases and needs of the group.
Compared to a hospital setting, a primary care setting in Belgium has a much smaller patient population. In Belgium pregnant women can freely chose to attend either a midwife, GP or an obstetrician. However, national data indicate that the vast majority of women choose an obstetrician as their main care provider, whether or not in cooperation with a midwife or GP.23 In contrast, only a minority of the Belgian population consults a midwife as their main care provider. Midwifes perform this role mostly in primary care and only for physiological pregnancies. In addition, the current compulsory health and disablement insurance in Belgium reimburses specialist care without preauthorization (including care provided by an obstetrician), regardless of whether it is a pathological or physiological pregnancy. The majority of pregnant women go directly to the obstetrician for ANC.24 Consequently, this specialized care is very accessible. Midwifery care is equally reimbursed by the health insurance, but pregnant woman do not recognize midwives as a primary professional group to provide antenatal care.25 This information is of importance to GANC, given that to our knowledge, each paired team of GANC facilitators consists of at least one midwife. As a result, GANC facilitators working in primary care organizations have a smaller group to recruit participants from. They depend on other organizations and care providers for providing potential participants for this.
Two types of referrers exist: social workers and medical care providers (ie obstetricians, GP’s and midwives). Social workers do not provide antenatal medical care themselves and are therefore obliged to refer women to medical care providers. In contrast, medical care providers do provide antenatal medical care themselves and thus referral is less straightforward. Referral implicates handing over their patients and thus, a loss of source of income. This has to do with the Fee for Service payment system, which is applied in the Belgian health care system, allowing health care providers to be paid for each service performed.
Therefore, primary care organizations face an additional challenge before the actual recruitment of women: the referral of women to their consultation.
The main objective of this study is to understand why care providers refer or do not refer to GANC facilitators in primary care organizations. To our knowledge this is the first study examining this implementation problem. This information contributes to the knowledge about when and how a potential referrer can be involved and influenced. Based on this, strategies can be developed and selected to involve and influence referrers in order to increase the influx of women in antenatal GANC.
Materials and Methods
We adopted a qualitative approach to explore the experiences and perceptions of care providers regarding referral of women to GANC. A predominantly inductive thematic approach to analyse was adopted, considering the predefined constructs of the implementation frameworks the Consolidated Framework for Implementation Research (CFIR)26 and the Theoretical Domains Framework (TDF).27 The frameworks were used as a basis for the interview guides and coding. The CFIR, as well as the TDF are applied to identify barriers and enablers which are operating at multiple levels during implementation of an innovation.28 Although both operate at multiple levels and consist of partially overlapping domains, they place different emphasis. The TDF mainly focuses on individual-level behavior change, which is useful to understand the referral behavior of care providers. It includes constructs such as “skills”, “emotions” and “professional role and identity”. However, behavior is also determined by factors external to the person. In this respect, CFIR has its place to provide a more overarching perspective, comprising elements such as “organizational culture” and “patient needs and resources”. At the start of the interview, the researcher posed open-ended questions which are not based on a construct but allow the phenomenon to be studied in an inductive way. An example is “How do you experience the referral to GANC?” and “Are there any barriers that prevent you from referring women to GANC?”. The larger constructs of the frameworks were used as probes, such as “What characteristics of your organization influence the referral?”. The interviewer was able to explore specific topics in more detail using a printed document containing the constructs of the CFIR and TDF. Thus, the constructs were used both during the development of the interview guide (as probes) and coding, to help awareness of important elements, rather than to cover all the constructs. This flexible approach allowed an inductive examination of the influencing factors that respondents perceive and experience regarding the referral to GANC.
Sample
To select interviewees that are involved in the referral (potential referrals, GANC facilitators, and other stakeholders), we used three primary care organizations offering GANC as a starting point. Two are located in the Brussels Capital Region and one in the province of Antwerp. The GANC facilitators informed the research team about potential care providers, involved in the referral. The GANC facilitators sought participants’ approval before the research team contacted them. We also invited GANC facilitators from four other primary care organizations in Belgium in order to adequately cover this group and their perspective. Important to note is that the selected organizations offer GANC primarily to psychosocially vulnerable women, like most of the GANC organizations in Belgium do. Psychosocially vulnerable pregnant women are defined as such if they meet the criteria determined by the tool developed by Amuli et al29 This tool considers indicators, such as financial situation, housing situation, social support, depression, anxiety, substance use and domestic violence. Organizations do not use general referral criteria. However, given that some GANC organizations offer GANC only to psychosocially vulnerable pregnant women referred, this counts as criteria for the respective organizations. Pathological pregnancies are not excluded, but are jointly followed up with an obstetrician.
To guarantee a diverse sample, we purposively sampled potential respondents. This resulted in a variety of interviewees in terms of organization (primary and secondary care), services (medical and social services), profession (obstetricians, social workers, midwives, heads of midwifery, and general practitioners) and organizations offering GANC or not (internal and external referrals). In addition, GANC facilitators informed us how they experienced the referral of each potential referrer (ie, no, moderate, or good referral to the GANC facilitators).
Data Collection
Data collection took place between January 2021 and February 2022. After the respondents accepted the invitation, the researcher scheduled an appointment. The interviewees could choose between a face-to-face interview and an online interview (through a Teams meeting). The latter was offered as a possibility because of the COVID-19 pandemic. The researcher initiated with a brief recapitulation of the purpose and method of the interview and explanation of confidentiality and then proceeded to the interview. All interviewees provided verbal informed consent for recording and use of anonymized quotations. Semi-structured interviews were used to retrieve the data. The researcher used the topic guide and research question as a reference, but the participants’ responses guided the interview. The topic guide was constructed using manuals offered by the author of the TDF,27 the technical assistance website of CFIR30 and supplemented with additional questions the researchers deemed necessary to explore the research topic. The interview guide was peer reviewed by the research team and ethical committee.
The interviews always started with posing open-ended questions such as “What is your role within GANC?” and “How do you experience the referral to GANC?”. Next, depending on the respondents’ input, specific domains, which are also highlighted by the CFIR and TDF, were explored in more depth.26,27 Examples are “What do you know about GANC?” to investigate the construct knowledge of the CFIR and TDF and “What is your impression about GANC?” to explore their view about GANC. Furthermore, we revisited the initial interview guide as the research progressed, following the answers we received from the respondents, but in consideration of the research question.31 We decided to stop data collection as soon as data saturation was achieved.
Data Analyses
Interviews were audio-recorded and transcribed verbatim. The analysis was conducted based on the steps of thematic analysis recommended by Braun and Clarke.32 Primarily the researcher became familiar with the data by transcribing, reading and re-reading the transcripts, while taking notes of emerging ideas. Next, we assigned codes to fragments, initially closely to what the respondent said. Subsequently, we assessed which codes could be combined to form an overarching theme. We used the domains and constructs of TDF27 and CFIR26 to have a rough structure, but enough flexibility to allow new or additional themes to emerge from the data. The set of themes underwent a successive process of definition, refinement and renaming before finalizing. To support this iterative process, the researcher designed a diagram with the different themes and had a series of discussions with the research team and external advisory committee. In addition, four interviews were conducted and coded by a second researcher, using open codes (independently of the constructs of the CFIR and TDF). In an initial meeting the two researchers compared their codes from the first round. This discussion revealed a clear distinction between referring to and recruiting for GANC. The latter was not the scope of this study and codes were excluded for that reason. Other inconsistencies were not found. However, both researchers agreed which constructs could be merged and which denomination was most accurate. Subsequent discussions with both researchers and a senior researcher on the one hand and the supervisory committee on the other mainly dealt with the merging, splitting, naming and connecting of constructs. Such research triangulation avoids single research bias33 and increases the trustworthiness of the findings.31 In a later phase, the preliminary results were presented to a number of interviewees, which made it possible to verify the interpretation. NVivo software (version 12) was used to assist during data analysis.34
Ethical Statement
We confirm that our study complies with the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of the University Hospital Brussels (Approval number 2019–365) on November 20 2019. All interviewees provided verbal informed consent for recording and use of anonymized quotations, which was approved by the Ethics Committee.
Results
Respondents (n= 31) represented a diverse range of care providers, working in different types of organizations and fulfilling a different role within the organization of GANC. The characteristics of the respondents are represented in Table 1. Length of interviews ranged from 17 to 91 minutes (mean length 49 minutes).
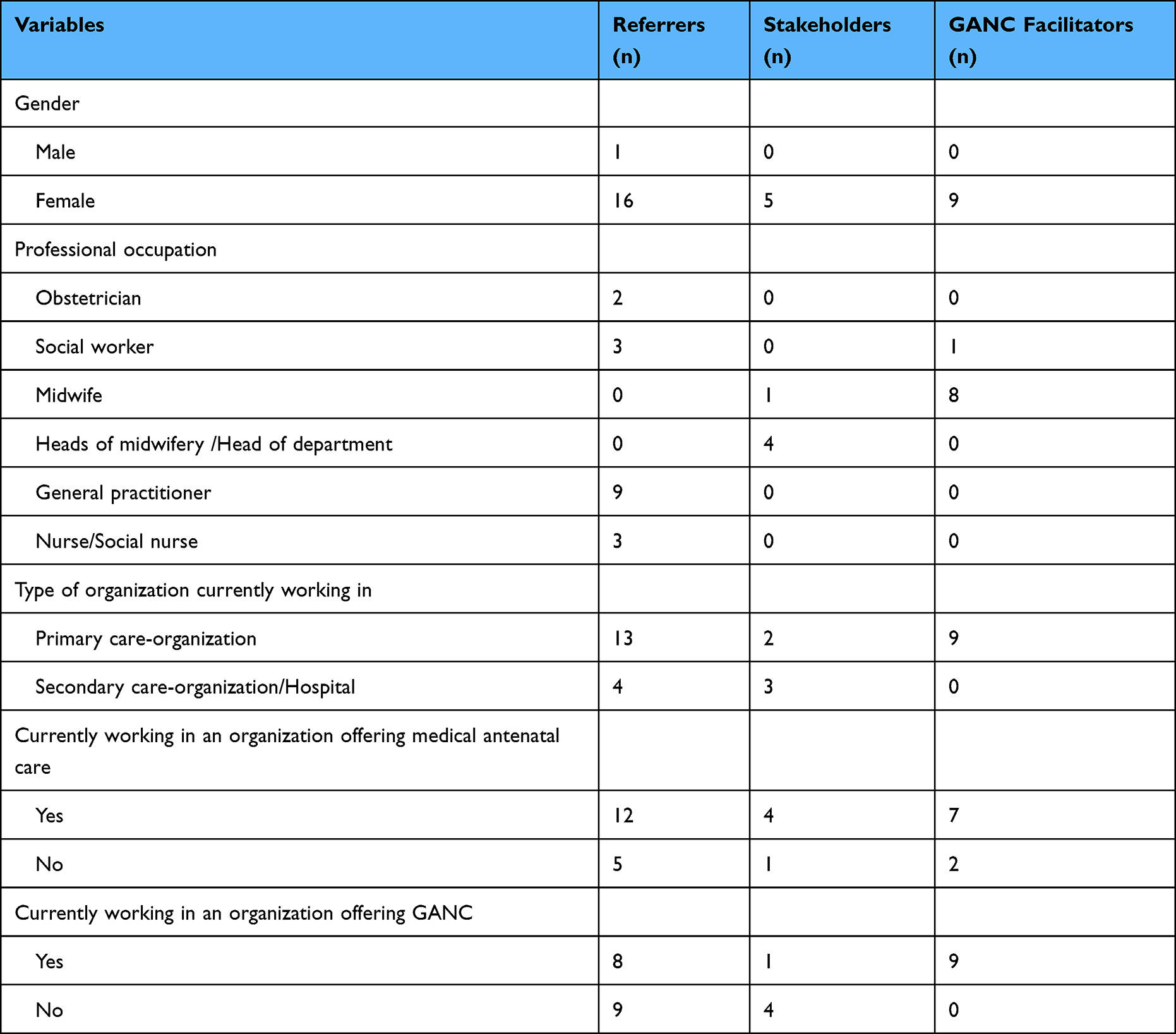 |
Table 1 Characteristics of Respondents (n = 31) (GANC= Group Antenatal Care) |
The results provide an explanation for the variation in referral to GANC facilitators. The findings reflect the perspective of both the (potential) referrers, and the perspective of GANC facilitators and stakeholders indirectly involved in the referrals.
A first observation is that the (potential) referrers undergo a multi-staged decision-making process before they actually refer. While some have completed the process and successfully recruit, others are situated in a previous stage. Thus, the individual stage in which a referrer is situated determines the referral behavior and provides an explanation for the variation in this behavior. Although it was not the purpose of this study to explore the decision making process of (potential) referrers, it emerged from the interviews as an important influencing factor. Even more, it appears to be an impeding factor to which the other determinants are related. This leads us to the second observation: several other enabling factors are at play according to the decision making process-stage. These determinants might explain why an individual may or may not move on to the next stage and in turn affect the referral behavior.
The Decision-Making Process to Refer
Figure 1 illustrates the decision-making process of a potential referrer. The figure includes the constructs and is thus the result of the analysis. Developing the figure helped to structure the constructs, establish and visualize the links between the constructs.
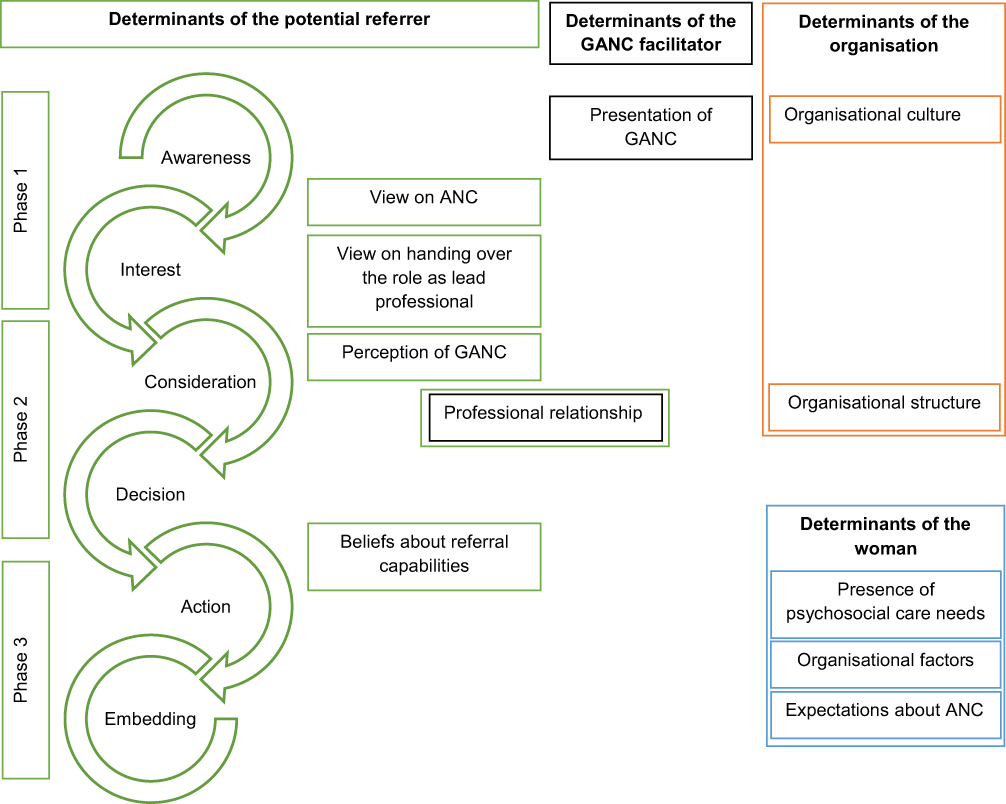 |
Figure 1 Decision-making process of potential referrers for the referral of women to GANC. Abbreviations: ANC, antenatal Care; GANC, Group Antenatal Care. |
The process starts with phase one (upper part of the figure) and consists of “awareness of GANC” and “an interest in GANC”. It proceeds to phase two (middle part of the figure): “consideration to refer”, and the “decision to refer”. Finally, the potential referrer moves to phase three (lower part of the figure): “takes action” (refers) and “embeds the new behavior” (continues referring).
Depending on the phase in the process where the potential referrer is situated, different elements are of influence. In the figure, these are grouped into elements at the level of the potential referrer (in green), the GANC facilitator (in black) the organization (in orange) and the woman (in blue).
Being aware of the existence of GANC is the first obvious step to referring to GANC; without knowing its existence, referrers cannot present it as a possibility for pregnancy monitoring. All of the respondents were familiar with and understood the basic elements of GANC. When asked more specifically what they understood by the concept of GANC, the emphasis was mainly on “sharing information in a group” and “strengthening the social network”. Interestingly, the third core component of GANC, the medical assessment, was less explicitly addressed by the respondents.
Based on the information potential referrers receive about GANC, in combination with other factors discussed below, they gain an interest to refer people to GANC. It is the first reaction to GANC and the idea of collaboration without undertaking specific actions. At this first stage, one could say that the potential referrer has a relatively passive role and should mainly be receptive to the information and the idea of referral.
During this second phase, “consideration and decision to refer”, potential referrers are no longer mere recipients of information but play a more active role. They actively engage in thinking about how to make the referral possible. Whereas in the previous phase it is mainly important that the idea about GANC and the referral is acceptable for the potential referrer, during the second phase, the feasibility of the referral is considered more in detail: what are the advantages and disadvantages, obstacles, and facilitators? After considering all the elements, a decision is made to proceed with the referral.
During the third phase, the actual action takes place; healthcare providers refer women to GANC facilitators. Initially, they try out the new behavior. After a while, this test phase will determine whether they will continue to refer or not. If so, referral to GANC is embedded in routine practice.
The process described here is one with a positive outcome: the healthcare providers refers. However, the process can be interrupted at any time and resumed, depending on perceived barriers or facilitators.
Influencing Elements During the First Phase of the Decision-Making Process: Being Aware of and Getting Interested in GANC
At the very beginning of the process, a potential referrer becomes aware of the existence of GANC and develops an interest in it. This phase in the process is illustrated in the upper part of Figure 1. Two groups of actors play a role: the GANC facilitators as information providers and the potential referrers as information recipients. The latter is driven by their intrinsic vision and the organizational culture.
Presentation of GANC by GANC Facilitators
In the first instance, the GANC facilitators act as the sole and most important source of information on GANC in most cases. All potential referrers indicated that they became acquainted with GANC through GANC facilitators. GANC is still a new concept and poorly known among healthcare providers and women.
In addition, during this first introduction, GANC facilitators do not only promote GANC, but also a potential collaboration. The crucial elements of this first introduction are a clear but concise explanation, emphasizing the added value, motivating the potential referrers and stakeholders, and creating an opening for further collaboration. These elements are best integrated in a person-to-person meeting, and is thus more effective compared to, for example, a mail or leaflet.
They came to the hospital to present the project. And we couldn’t have done it better. (.) They presented it very well, very clearly and concisely. And that really created an opening. Because that way there was also personal contact. - Midwife 1, hospital, stakeholder
A variation on a conventional presentation or meeting to inform about GANC is to simulate a session together with potential referrers. This approach is more concrete and generates additional motivation to refer.
We are now going to (.) conduct a session with them. With the supervisors. So that they understand the concept very well. (.) And we think that once they’ve had a taste of what it’s like, they’ll be able to refer people much better or more enthusiastically. - Midwife 2, primary care-organization, GANC facilitator
Potential Referrer’s View on ANC
This phase of being “aware of and interested in referring to GANC” also depends on the potential referrer’s view on ANC.
Most of the respondents described ANC as an event in which both medical and psychosocial needs must be considered. Some indicate that primary care organizations should be the first point of contact for physiologic pregnancies and that referral to the hospital is only necessary if specialized care is needed.
I am a promoter of primary care. I tend, yes, not to medicalize everything. If everything goes well, you don’t need to go to hospital, you don’t need to see a obstetrician. It’s still performance-oriented medicine. - General Practitioner 1, primary care-organization, referrer
In addition, respondents mentioned this view is not shared by all care providers. The care providers who work in hospitals focus mainly on the medical and technical aspects of a pregnancy follow-up. This “medicalization of the pregnancy” is, according to respondents, the main reason why hospitals are not interested in referring their clients to GANC organizations.
With them (obstetricians) it goes in one ear and out the other. They’re not really interested. (.) A pregnancy is a medical follow-up, but there is also the whole aspect of information. As long as obstetricians don’t see that, don’t realize it. (.) The medical remains their job and their job is the most important thing. - Midwife 3, primary care-organization, stakeholder
Potential Referrer’s View on Handing Over the Role as the Lead Professional
A third theme addressed by most respondents was their view on handing over their role as lead professional towards the GANC facilitator. GANC replaces most of the prenatal consultations, which entails a redistribution of the roles and responsibilities within the pregnancy follow-up. For some, this implies that the role is completely handed over to the GANC facilitator. In this study this is mainly the case for general practitioners. For others (eg obstetricians) it entails shifting to a shared follow-up, dividing both the consultations and the role as lead professional.
Some felt that this is part of interdisciplinary work and benefits women and the quality of care.
I now see it more as a collaboration. It’s not as if we don’t see any pregnant women anymore. The midwife calls from time to time and says: look, for this or that problem, can you help her out? It’s not like: here’s the pregnant woman, there you go, it’s up to you. No, we’re still here. - General Practitioner 1, primary care-organization, referrer
So I think that if you can share the care with each other, you will increase quality. But what I was a bit afraid of is that the doctors don’t realize this. Not like the midwives do. - Midwife 4, hospital, stakeholder
For others, on the contrary, it had a rather negative connotation. Care providers experience the referral to GANC as “handing over” the women and their role within the pregnancy follow-up. The following quote from a general practitioner highlights that being a referral in function of GANC, also implies that she no longer performs pregnancy follow-up.
And so, yes, I’ve let it (the pregnancy follow-up) go. So I refer them all. And I do think that’s a shame. So I think, maybe there are still colleagues who find that a bit unfortunate. – General Practitioner 2, primary care-organization, referrer
Several interviewees even described it as rivalry between healthcare providers and as the primary reason healthcare providers do not refer.
And we also have one of the obstetricians who doesn’t like to share (laughs), if you know what I mean. Who doesn’t like to hand over consultations for example. Who is afraid that it will become a competition instead of a collaboration. - Midwife 4, hospital, stakeholder
We identified several main reasons for this negative connotation with this handing over of the role as lead professional.
When a healthcare provider refers a woman to GANC, they have less or no consultations at all with the referred women. For some this implies a loss of financial income:
Well, on the one hand, I think it’s very understandable that they want to keep their patients. That’s just the commercial side of healthcare. (.) So financially it’s not interesting for them to send patients to us. Erm, because they are losing money. - Midwife 5, primary care-organization, GANC facilitator
I think as a midwife myself, referring women to a midwife is a difficult thing to do, because you are actually handing over work (.) As a self-employed worker, I would think ‘why am I referring them?’. Unless I really see an added value for the women I would ask myself why I didn’t just do it myself and earn my own living from it. - Midwife 6, primary care-organization, GANC facilitator
In addition, some presume that sharing the pregnancy follow-up with another care provider implies for the potential referrer that they no longer have an overview of the needs of the women and the provided care. Also, it might no longer be clear to them which role they will have in the pregnancy follow-up, resulting in role ambiguity.
They also do consultation. And I have to say, in the beginning it was quite difficult, because if they do consultation as well, we thought, ‘what will our role be in the long run?’ (.). So (in case of referral to GANC) you cannot know the people very well, because the more they go to different places, the less you know them yourself. (.) Then it would get so fragmented. - Obstetrician 1, hospital, referrer
Organizational Culture
All interviewed healthcare providers work within the context of an organization, which in turn is shaped by its culture and structure. During this first stage of the referral decision-making process, primarily organizational culture has an indirect influence on potential referrers. In the first instance, depending on the culture, an organization is willing to embrace innovation and pass on the information to its employees. Thus, the organization determines whether or not a healthcare provider will receive information about GANC.
In addition, the culture of an organization also affects the views of its employees regarding the pregnancy follow-up and multidisciplinary approach. When interdisciplinary collaboration is part of the values of an organization, referral is encouraged. This is the case for organizations where different type of professionals work in the same organization.
In general, we are working very hard to work interdisciplinary and so on and together and to refer. (.) That certainly helps too. (.) The shared culture ‘together we are stronger’. And we can learn a lot from each other. - General Practitioner 2, primary care-organization, referrer
Influencing Elements During the Second Phase of the Decision-Making Process: Consideration and Decision to Refer
In the second phase of the decision-making process, three main factors will contribute to whether a potential referrer will consider and decide to refer: the perception a potential referrer has regarding GANC, their professional relationship with the GANC facilitators, and the structure of the organization.
Potential Referrer’s Perception of GANC
Almost all interviewees are predominantly positive about GANC and its impact on women’s wellbeing. They believe GANC responds to women’s needs during their pregnancy follow-up. The stated advantages are the strength and psychosocial support the group offers, the increased attention and time for sharing information among peers, more attention to the physiological aspect of pregnancy (de-medicalization of the follow-up) and empowering women to take control over their health and care.
However, when a care provider is not convinced that GANC can add value to the current individual care, neither for one’s organization nor for the women, they will be less likely to decide to act as a referrer. As the following GANC facilitator describes:
I think that if people (care providers) have their own fixed care pathway, they really stick to it and they wouldn’t understand why Group Care is better. Both for them as a hospital and for the women. And I also notice this doubt myself. (.) I don’t know whether I would refer people who I know are getting good and individual support from me. - Midwife 6, primary care-organization, GANC facilitator
In terms of perception about GANC, respondents believe that the compatibility or the fit of the care offered by GANC with the care provided by the referrer is important. If a care provider perceives both as complementary, the threshold for referral is lower. This is certainly the case for social organizations, in which GANC provides the medical services they cannot offer. Some medical professionals also experience the complementarity of care, particularly the extra attention for education and psychosocial support, as a reason to refer women.
The dynamics of a group, of people in the same situation, who can reinforce each other, is something that we cannot offer in this hospitals. And we will be able to offer it when we work together or refer to the project. - Midwife 4, hospital, stakeholder
On the other hand, for some, the medical care offered by GANC overlaps with the care the referrer provides, which makes one’s role in the follow-up of pregnancies uncertain. The response varies for care providers whose roles and services partially or fully overlap. When the benefit for the woman outweighs the benefit for the care provider, they are prepared to adapt their role and care (path) in the referral to GANC.
But I think, it seems to be better for the women. So yeah, it doesn’t have to be better for us. And we are involved. – General Practitioner 1, primary care-organization, referrer
Professional Relationship with GANC Facilitator
The presence of an existing professional relationship between the potential referrer and the group facilitator stimulates the decision to refer. Simply knowing the individual to whom someone refers is a first important step. Group facilitators are aware of this and act on it by visiting potential referrers and getting to know them in person.
Even more crucial is confidence in each other’s expertise, resulting from an already existing and positive collaboration between both parties. The following quote illustrates the importance of mutual trust in expertise:
There is also trust that grows over time in how we (the facilitators) work and how we approach things. (.) If you make use of the other person’s expertise, that trust also grows because he thinks, well, she’ll come to me if she really doesn’t know. And if she really knows, she’ll do it. - Midwife 7, primary care-organization, GANC facilitator
Yes, I think good mutual contact. Mutual contact and trust. You have to have trust. - General Practitioner 3, primary care-organization, referrer
A common view amongst interviewees was that accessibility and availability is an important stimulus for good collaboration. Indeed, if the workplaces are close and the group facilitator is flexible in terms of time and working method, this is less of a barrier than if the opposite is true.
It is never far away, because it happens here. So that’s also something that encourages to refer people. (.) And here you refer, but you stay informed on how it goes. - General Practitioner 4, primary care-organization, referrer
The midwives are also very accessible. (.) When I call the reception, they quickly give me an appointment. They are easy to reach. – Nurse 1, primary care-organization, referrer
Consequently, it is more convenient for internal referrers. They usually are familiar with each other, and already have an existing professional relationship with the group facilitator. There is also no physical barrier, as their workplace is situated in the same building. In addition, they are aware of each other’s expertise: it is “more visible”.
At the doctors’ meeting recently, the midwife came and spoke about medication and breastfeeding for example. And I think, that way the midwife is also visible and we learn things from their expertise and so on. And this reminds us, yes wow, they know so much. And it has such a positive impact. - General Practitioner 5, primary care-organization, referrer
Among external referrers, the opposite is noticeable: more often, they are unfamiliar to each other, each other’s expertise is less visible, and the physical distance is more significant. Especially the physical distance proves to be the most important barrier and challenging to resolve. Group facilitators, however, try to strengthen the professional relationship by physically visiting, maintaining regular contact and relying on the referrer’s expertise.
Organizational Structure
When a potential referrer needs to decide whether or not to refer, the organizational structure and consequently the way decisions are made in an organization have an impact. Organizations with a rather vertical structure can slow down the decision-making process concerning referrals to GANC. In these cases, people from different and higher layers are involved in a decision. According to a number of respondents, these individuals delay or prevent the process and decision to take action. However, the formal approval of the management to collaborate and refer is an important incentive to take action, in this case: refer.
Influencing Elements During the Third Phase of the Decision-Making Process: Action and Embedding
In this phase, the referrer implements the new behavior and anchors it in its daily work (illustrated in the lower part of the figure). The referrers own characteristics still play a major role, especially the belief in one’s own abilities. In addition, it will also depend on the women’s characteristics whether or not the referrer will suggest GANC as a possible option for follow-up.
Beliefs About Referral Capabilities
The lack of belief in one’s own abilities influences whether they refer a woman to GANC, even though they favor GANC. Some indicated that they do not propose GANC or are less likely to propose it if they expect the woman to refuse. Interestingly, it is not the actual reaction of women but rather an anticipation of the reaction that hinders them from introducing GANC.
I don’t know if it’s a kind of resistance on my part or if I think it is on the patients’ side. But, the idea that they would find it strange, like ‘well, there’s a group of pregnant people.’ - General Practitioner 1, primary care-organization, referrer
In addition, feeling insecure about referring women also influences how GANC is presented. It emerged from the interviews that some commented they tend to sell GANC by overwhelming the women with benefits. Several others stick to a concise description, because they believe they have too little affinity with GANC and want to leave the actual recruitment to the facilitators.
For me, it’ s still a bit theoretical. So you explain it a bit, but it’s not really. It’s less inspired I think. - General Practitioner 2, primary care-organization, referrer
When insecure about referring women to GANC, the referral must remain low-threshold by providing support and tools. For example, by letting the GANC facilitator contact the woman after her approval. This way, the GANC facilitator does the actual recruitment.
A frequently cited tool is the use of a flyer intended to convince women to participate in GANC. Opinions on its usefulness are divided. For some, it is a support to explain, and others believe that the effect of a flyer should not be overestimated and that personal contact is the most efficient way to recruit women. Finally, several interviewees favor a training session to learn about recruitment techniques.
Once again, there is a noticeable difference between internal and external referrals. Both the referrer and the woman interpret a referral within the same organization, as a part of the organization’s workflow and as a logical next step in the pregnancy follow-up. Internal referrals usually link a concrete action to the referral, such as a blood test, which simplifies the referral.
In contrast, care providers who refer women externally, perceive it as having to sell GANC. The focus here is much more on GANC. They consider it to be a new service that is not part of the normal routine within their organization, making them feel less comfortable.
Determinants of the Woman
For several respondents, woman’s attributes determine whether a recruiter proposes GANC as a possibility of ANC. Referrers make a selection based on three types of determinants.
First of all, recruiters indicate that they determine on the basis of the woman’s psychosocial characteristics whether they will refer the woman to the GANC facilitator:
I know it’s for everyone but I mainly suggest it to the mums who need a bit more support. So, indeed for the mothers that I think ‘oh, they need a little bit of support’. I will certainly suggest it to them. – Nurse 2, primary care-organization, referrer
A second group of determinants concerns the presence or absence of logistical factors (eg if the woman works, has no childcare for her children or resides too far away). If they feel that these factors will prevent the woman from participating in GANC, they are less inclined to refer them.
I think it is rather based on feeling. There is a difference between patients. (.) Do they have a job, do they not have a job. What is their social background. That determines a little bit who you send there. – Obstetrician, hospital, referrer
A final group of determinants at the woman’s level are the woman’s expectations of ANC. Interviewees indicate that when women have a pre-conceived wish about their pregnancy follow-up, this determines whether they will refer the woman or not. Indeed, referrers are less likely to suggest GANC to women who express wishes that are not in accordance with GANC.
And then there are those who are convinced that it has to be done purely medically. And you can’t get them on board. - General Practitioner 2, primary care-organization, referrer
On the other hand, referrers are much more prone to suggest the option of GANC when women express certain wishes that GANC can offer, such as the wish for more time for education and participation in their pregnancy follow-up.
But I do think that this group of women, who are in any case more interested in a less medical and more inclusive follow-up of the pregnancy, are easier to convince. - General Practitioner 7, primary care-organization, referrer
Discussion
This is the first study to examine the factors that motivate or deter health care providers to refer to GANC facilitators. This research reveals the decision-making process of care providers in the referral of women to primary care organizations for GANC. Understanding the process and their influencing determinants is useful to develop knowledge about when and how a potential referrer can be involved and how to optimize referral. In addition, the study provides key information by generating knowledge about the domains that influence the implementation of GANC, namely the implementation settings, implementation context, implementation agents and implementation strategies.35
According to this study, care providers should be “aware of GANC”, “have an interest in GANC”, “consider to refer” and “decide to refer”. Only then will they “take action” to actually refer and “embed the new behavior” (continues referring).
These stages are similar to the innovation-decision model developed by Rogers,36 which illustrates the process by which individuals adopt innovations. The model describes the following sequential steps: knowledge, persuasion, decision, implementation and confirmation. Whereas Rogers’ stage of persuasion in the present research is divided into 2 steps, namely “gaining interest” and “considering”, the other steps are similar.
Our results allow us to make suggestions about implementation strategies to address specific determinants and decision-making stages. These strategies might ensure that GANC will be adopted and sustained.37 However, GANC organizations still need to explore which strategies are adequate and applicable within their specific context. Consequently, GANC facilitators can and should play an active role within this referral, by implementing specific strategies.
Strategy One: Selecting Referrers
The results show that particular groups of organizations and care providers are more likely to be open to the idea of GANC and to refer than others. Rather than focusing on all care providers, GANC facilitators may prioritize some based on a number of characteristics.
Firstly, facilitators should focus on care providers who can refer within the own organization. Several elements stimulate the acceptance of referral: an existing professional relationship, awareness of the others’ expertise and geographical proximity.
Secondly, it seems easier for social organizations, who do not offer medical antenatal care, to refer to GANC. They do not perceive GANC as a threat, since their services are complementary. Preferably, they are also geographically close to the GANC organization, as a great distance may prevent them from referring.
Lastly, it could be stated that the most challenging types of organizations to convince to refer, are those that offer antenatal care themselves. Their roles overlap.
These findings are comparable to Rogers’ Diffusion of innovations theory.36 This theory states that a population can be divided according to its tendency to accept an innovation: innovators, early adopters, early majority, late majority and laggards. Whereas the first two groups, innovators and early adopters, will accept an innovation relatively easily, the other groups will adopt a wait-and-see attitude. The latter rely on the experience of the first two groups to decide whether or not to accept an innovation. Mirroring this to our findings we can recommend GANC facilitators that they should start to convince the first two groups: within the own organization and organizations offering complementary care. Only after a period of time and after a positive experience of the first two groups, the remaining groups will follow. In this case, the organizations offering antenatal care themselves are part of the latter group. However, GANC-facilitators need to be aware that the diffusion of this new idea is hampered in Belgium due to the current existing pay for service system. The results show that for some external providers who also offer ANC, the added value for women prevails and is therefore sufficient as an incentive to refer women. For others, the loss of the role as main care provider and/or financial loss will outweigh. As a result, many external providers who also offer ANC will be reluctant to refer. Nevertheless, since shared decision making in care is gaining attention, all care providers should inform the pregnant woman about all options of ANC models, allowing her to make an informed choice.
Strategy Two: Selecting Champions
GANC facilitators might identify and target a leader or “champion” in each organization.26 A champion is a person who uses their personal influence to encourage the introduction of an innovation. In addition, a champion can also provide more insight regarding the functioning of the organization and possible barriers and facilitators for the collaboration. The importance of a champion was also demonstrated in interventions including referral to smoking cessation38 and oral health services.39
The results indicate that factors such as the view on ANC and GANC, the view on handing over the role as lead professional and the absence or existence of a professional relationship, affect the tendency to refer. GANC facilitators should select champions within an organization based on these factors. Potential referrers are preferable those who have a positive view on GANC or with whom the facilitator has a pre-existing professional relationship. A champion is meaningful at all stages of the process: from presentation of GANC to continued monitoring during the embedding of referral. While a champion can be helpful in any type of organization to ensure referral, it is most applicable for organizations where most resistance is expected, such as external organizations that also offer ANC. Once again, for most care providers that provide ANC as well, only a financial incentive will suffice to refer towards GANC. In the absence of a financial payment system that encourages referral, we encourage GANC-facilitators to apply a combination of these strategies to increase the likelihood of success.
Strategy Three: Investing in Communication
Throughout the whole process, communication appears to be an important factor. GANC facilitators need to have good communication skills and deploy them to stimulate the different phases of the decision-making process.
At an early stage, GANC facilitators should inform organizations and the potential recruiters to create awareness and interest. This is time-consuming, but of utmost importance in contexts where GANC is not yet widely known.
Our results show that it is important that potential referrers see the added value of GANC, both for the pregnant woman and for the organization. Depending on the type of care provider, GANC facilitators should emphasize the added value for the former (the woman) or the latter (themselves). Indeed, according to Greenhalgh et al,40 an innovation is more likely to be accepted if an individual associates an observable advantage with the innovation compared to what already exists.
Interviewees reported that open communication, regular contact and accessibility are also important in the subsequent phases. These elements strengthen the professional relationship, which is crucial during the second phase, when deciding to collaborate as a referrer.
Finally, when the health care provider eventually progresses to referring women, it is advisable to provide regular feedback about the start of groups, successful referrals and women’s experiences with GANC. This way they are aware of the progress of the groups, remain involved in the project and the women’s care, experience the added value of GANC, and become aware that the referral has been successful.
Strategy Four: Solidifying the Collaboration
After the potential referrers have been informed and are interested in the referral, it is recommended that the collaboration is further specified and the care pathway for women following GANC is established.
A GANC program ideally is initiated around 12 weeks of gestation. The sessions take place at predetermined stages during pregnancy and with a specific frequency. Medical follow-up and information sharing are incorporated. On the other hand, referrers have their own procedures, care pathways and habits, in their organization. The GANC facilitator should be mindful of these aspects and develop a care pathway in which the responsibilities and roles of all care providers involved are clearly defined. GANC’s care pathway should be flexible and adaptable to a certain extent.
Greenhalgh et al40 believe that innovations that are flexible or can be adapted to the specific needs of an organization are more likely to be accepted. On the other hand, greater fidelity to the GANC model ensures that the positive effects are obtained.41 GANC facilitators must therefore find a balance between the degree of flexibility and fidelity to the model.
Strategy Five: Providing Tools to Increase Confidence Among Referrers
Finally, GANC facilitators can employ strategies to reinforce potential referrer’s belief about their own referral capabilities. Two options are flyers to inform pregnant women and a training for potential recruiters. The latter may include oral or written testimony from women who participated in GANC, whom care providers tend not to refer (eg a working woman or multipara). This may avoid non-referrals based on pre-assumptions. Previous research also provided training to increase self-confidence and motivation to refer towards smoking cessation services among care providers.38
Strategy Six: Change the Policy
While the above elements strongly suggest the importance of individual and organizational elements in referral to GANC, our findings also showed that contextual elements of the broader environment must be considered. Indeed, Pfadenhauer et al35 emphasizes strongly the importance of context and its intertwining with the implementation of interventions.
In Belgium, pregnancy care is strongly focused on the medical aspect, with a central focus on preventing pathology. In addition to the clinical interventions, however, there is also a demand and need for psychosocial support42,43 and a more active role for women in their own trajectory and care.44 GANC can offer an answer to this demand. Despite the tremendous progress of starting-up Group Care in Belgian organizations in recent years, the implementation should be supported by policy and an adapted financing system.24 The referral should not entail a loss in income. In addition, to establish GANC in Belgium, it is necessary to implement GANC in organizations with a larger population and higher prestige (such as hospitals). If key stakeholders within ANC, such as obstetricians, were to implement GANC, this would benefit the acceptance of the model within Belgium. However, we have to bear in mind that this will also include a shift from a focus on medical and technical operations towards including the physiological aspects of pregnancy. In addition, GANC leads to cost neutrality or saving in other countries, depending on the setting.19 A health economics study in Belgium could also be an incentive to engage policy makers.
Limitations and Strengths
A number of limitations need to be pointed out with respect to the study.
As in every study, we should acknowledge that health care providers who agreed to participate in interviews might be more positive towards the topic, in our case GANC and its referral. Also, certain professional groups, such as obstetricians, were underrepresented. We invited several obstetricians of which only two accepted, despite repeated request. Since the central role of obstetricians in pregnancy follow-up in Belgium, we suggest to include them in follow-up research.
Given that the initial goal was not to portray the decision-making process, no framework was used to conduct the interviews and coding around this aspect. For the detection of determinants, the CFIR and TDF were only used to subdivide the data into larger domains. However, this flexible approach allowed us to inductively examine the process and its influencing factors.
In addition, the focus of research was referral to primary care settings, results might have been different when focusing on implementation of GANC in a hospital setting. Furthermore, the results must be seen in the light of the Belgian context, which has a specific healthcare system and funding system. This may influence the transferability of the results to other contexts. Nevertheless, the implementation of any innovation in any context must involve stakeholders at different levels,35 who go through a similar decision-making process. The determinants and strategies described can provide a basis for the implementation of innovations such as Group Care, and applied in a variety of contexts. The strengths of this study are the size of and variation in the research sample, the triangulation with the research team and study participants, and the identification of factors at different levels. In addition, the study provides concrete strategies, which were formulated in such a way that GANC facilitators can easily translate them to their own practice.
Conclusion
In conclusion, we can state that in order to implement GANC in a sustainable way in Belgium, and countries with similar healthcare systems, referrals towards GANC organizations are crucial. This is especially the case in primary care settings. However, mobilizing referrers is a complex process depending on elements at different levels. For Belgium, both the implementation of and referral to GANC would benefit from a change in attitude and financing of ANC. In addition, the implementation of GANC in organizations with a larger population and higher prestige (such as hospitals) would benefit the acceptance of the model. Influencing determinants within the organization and the broader context requires time. However, the implementation of an innovation, such as GANC, initially requires short-term action. In addition, to change determinants at this higher level, policy strategies and political decisions are crucial. In absence of structural support, GANC facilitators in primary care settings should focus on key strategies they can deploy themselves and in a short time frame. In this regard, we advise to identify and select potential referrers based on the criteria found in this study. Following this, they can select a champion within an organization to motivate the other team members. An essential strategy is the presentation of the GANC project, while emphasizing the added value for a specific referrer. Once the collaboration is more concrete, GANC facilitators should work out the care path and referral process together with the potential referrer while respecting the core elements of GANC. In addition, the threshold for referral should be as low as possible by offering tools. And lastly, efforts must be made to build and maintain the professional relationships with the potential referrers.
Abbreviations
GANC, Group Antenatal Care; ANC, Antenatal care; GP, General Practitioner; CFIR, Consolidated Framework of Implementation Research; TDF, Theoretical Domains Framework.
Acknowledgments
We would like to thank all health care providers who participated in this study to make time and to share their experiences for this study. We are grateful to the advisory committee for their guidance and advice throughout the process, with a particular gratitude to Saskia Van Besauw and Katelijne De Koster.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Institute for Health and Disability (CGV 2018/363). This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 848147.
Disclosure
Financial support was obtained from the Belgium National Institute for Health and Disability Insurance (NIHDI) as part of the Federal Public Service Finance and the European Union’s Horizon 2020 research and innovation programme. However, the funders had no role in the study design, data collection, data analysis, interpretation of data or writing of this article. The authors report no other conflicts of interest in this work.
References
1. Rising SS. Centering pregnancy. An interdisciplinary model of empowerment. J Nurse Midwifery. 1998;43(1):46–54. doi:10.1016/S0091-2182(97)00117-1
2. Rising SS, Kennedy HP, Klima CS. Redesigning prenatal care through CenteringPregnancy. J Midwifery Womens Health. 2004;49(5):398–404. doi:10.1111/j.1542-2011.2004.tb04433.x
3. Tubay AT, Mansalis KA, Simpson MJ, Armitage NH, Briscoe G, Potts V. The effects of group prenatal care on infant birthweight and maternal well-being: a randomized controlled trial. Mil Med. 2019;184(5–6):e440–e6. doi:10.1093/milmed/usy361
4. Schellinger MM, Abernathy MP, Amerman B, et al. Improved outcomes for Hispanic women with gestational diabetes using the centering pregnancy© group prenatal care model. Matern Child Health J. 2017;21(2):297–305. doi:10.1007/s10995-016-2114-x
5. Carter EB, Barbier K, Sarabia R, Macones GA, Cahill AG, Tuuli MG. Group versus traditional prenatal care in low-risk women delivering at term: a retrospective cohort study. J Perinatol. 2017;37(7):769–771. doi:10.1038/jp.2017.33
6. Hetherington E, Tough S, McNeil D, Bayrampour H, Metcalfe A. Vulnerable women’s perceptions of individual versus group prenatal care: results of a cross-sectional survey. Matern Child Health J. 2018;22(11):1632–1638. doi:10.1007/s10995-018-2559-1
7. World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. World Health Organization; 2016.
8. Galle A, Van Parys A-S, Roelens K, Keygnaert I. Expectations and satisfaction with antenatal care among pregnant women with a focus on vulnerable groups: a descriptive study in Ghent. BMC Women’s Health. 2015;15(1):1–12. doi:10.1186/s12905-015-0266-2
9. Hildingsson I, Rådestad I. Swedish women’s satisfaction with medical and emotional aspects of antenatal care. J Adv Nurs. 2005;52(3):239–249. doi:10.1111/j.1365-2648.2005.03584.x
10. Sword W, Heaman MI, Brooks S, et al. Women’s and care providers’ perspectives of quality prenatal care: a qualitative descriptive study. BMC Pregnancy Childbirth. 2012;12(1):1–18. doi:10.1186/1471-2393-12-29
11. Docherty A, Bugge C, Watterson A. Engagement: an indicator of difference in the perceptions of antenatal care for pregnant women from diverse socioeconomic backgrounds. Health Expect. 2012;15(2):126–138. doi:10.1111/j.1369-7625.2011.00684.x
12. Harsha Bangura A, Nirola I, Thapa P, et al. Measuring fidelity, feasibility, costs: an implementation evaluation of a cluster-controlled trial of group antenatal care in rural Nepal. Reprod Health. 2020;17(1):1–12. doi:10.1186/s12978-019-0840-4
13. Sultana M, Mahumud RA, Ali N, et al. The effectiveness of introducing Group Prenatal Care (GPC) in selected health facilities in a district of Bangladesh: study protocol. BMC Pregnancy Childbirth. 2017;17(1):1–7. doi:10.1186/s12884-017-1227-6
14. Lundeen T, Musange S, Azman H, et al. Nurses’ and midwives’ experiences of providing group antenatal and postnatal care at 18 health centers in Rwanda: a mixed methods study. PLoS One. 2019;14(7):e0219471. doi:10.1371/journal.pone.0219471
15. Francis E, Johnstone MB, Convington-Kolb S, et al. Group prenatal care attendance and women’s characteristics associated with low attendance: results from Centering and Racial Disparities (CRADLE Study). Matern Child Health J. 2019;23(10):1371–1381. doi:10.1007/s10995-019-02784-7
16. Hackley B, Applebaum J, Wilcox WC, Arevalo S. Impact of two scheduling systems on early enrollment in a group prenatal care program. J Midwifery Womens Healt. 2009;54(3):168–175. doi:10.1016/j.jmwh.2009.01.007
17. Phillippi JC, Myers CR. Reasons women in Appalachia decline CenteringPregnancy care. J Midwifery Womens Healt. 2013;58(5):516–522. doi:10.1111/jmwh.12033
18. Yorga KDW, Sheeder JL. Which pregnant adolescents would be interested in group-based care, and why? J Pediatr Adolesc Gynecol. 2015;28(6):508–515. doi:10.1016/j.jpag.2015.03.006
19. Mooney SE, Russell MA, Prairie B, Savage C, Weeks WB. Group prenatal care: an analysis of cost. J Health Care Finance. 2008;34(4):31–41.
20. Wagijo MAR, Crone MR, van Zwicht BS, et al. CenteringPregnancy in the Netherlands: who engages, who doesn’t, and why. Birth. 2022;49:329–340. doi:10.1111/birt.12610
21. Berman R, Weber Yorga K, Sheeder J. Intention to participate in group prenatal care: moving beyond yes or no. Health Promot Pract. 2020;21(1):123–132. doi:10.1177/1524839918784943
22. McDonald SD, Sword W, Eryuzlu LN, Neupane B, Beyene J, Biringer AB. Why are half of women interested in participating in group prenatal care? Matern Child Health J. 2016;20(1):97–105. doi:10.1007/s10995-015-1807-x
23. Benahmed N, Lefevre M, Christiaens W, Devos C, Stordeur S Towards integrated antenatal care for low-risk pregnancy. Brussels: Health Services Research (HSR). Belgian Health Care Knowledge Centre (KCE); 2019.
24. Mattison CA, Lavis JN, Wilson MG, Hutton EK, Dion ML. A critical interpretive synthesis of the roles of midwives in health systems. Health Res Policy Syst. 2020;18(1):1–16. doi:10.1186/s12961-020-00590-0
25. Vermeulen J, Luyben A, Buyl R, et al. The state of professionalisation of midwifery in Belgium: a discussion paper. Women Birth. 2021;34(1):7–13. doi:10.1016/j.wombi.2020.09.012
26. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sc. 2009;4(1):1–15. doi:10.1186/1748-5908-4-50
27. Atkins L, Francis J, Islam R, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sc. 2017;12(1):1–18. doi:10.1186/s13012-017-0605-9
28. Birken SA, Powell BJ, Presseau J, et al. Combined use of the Consolidated Framework for Implementation Research (CFIR) and the Theoretical Domains Framework (TDF): a systematic review. Implement Sc. 2017;12(1):1–14. doi:10.1186/s13012-016-0534-z
29. Amuli K, Decabooter K, Talrich F, Renders A, Beeckman K. Born in Brussels screening tool: the development of a screening tool measuring antenatal psychosocial vulnerability. BMC Public Health. 2021;21(1):1–13. doi:10.1186/s12889-021-11463-8
30. Consolidated Framework for Implementation Research. Available from: https://cfirguide.org/2022.
31. Gioia DA, Corley KG, Hamilton AL. Seeking qualitative rigor in inductive research: notes on the Gioia methodology. Organ Res Methods. 2013;16(1):15–31. doi:10.1177/1094428112452151
32. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
33. Curtin M, Fossey E. Appraising the trustworthiness of qualitative studies: guidelines for occupational therapists. Aust Occup Ther J. 2007;54(2):88–94. doi:10.1111/j.1440-1630.2007.00661.x
34. QSR International. Invivo qualitative data analysis software (released in March 2020); 2020.
35. Pfadenhauer LM, Gerhardus A, Mozygemba K, et al. Making sense of complexity in context and implementation: the Context and Implementation of Complex Interventions (CICI) framework. Implement Sc. 2017;12(1):1–17. doi:10.1186/s13012-017-0552-5
36. Rogers E. Diffusion of Innovations.
37. Pfadenhauer LM, Mozygemba K, Gerhardus A, et al. Context and implementation: a concept analysis towards conceptual maturity. Z Evid Fortbild Qual Gesundhwes. 2015;109(2):103–114. doi:10.1016/j.zefq.2015.01.004
38. Jones S, Hamilton S, Bell R, et al. What helped and hindered implementation of an intervention package to reduce smoking in pregnancy: process evaluation guided by normalization process theory. BMC Health Serv Res. 2019;19(1):1–13. doi:10.1186/s12913-019-4122-1
39. Jackson JT, Quinonez RB, Kerns AK, et al. Implementing a prenatal oral health program through interprofessional collaboration. J Dent Educ. 2015;79(3):241–248. doi:10.1002/j.0022-0337.2015.79.3.tb05878.x
40. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581–629. doi:10.1111/j.0887-378X.2004.00325.x
41. Novick G, Reid AE, Lewis J, Kershaw TS, Rising SS, Ickovics JR. Group prenatal care: model fidelity and outcomes. Am J Obstet Gynecol. 2013;209(2):112. doi:10.1016/j.ajog.2013.03.026
42. Pampaka D, Papatheodorou SI, AlSeaidan M, et al. Depressive symptoms and comorbid problems in pregnancy-results from a population based study. J Psychosom Res. 2018;112:53–58. doi:10.1016/j.jpsychores.2018.06.011
43. Tani F, Castagna V. Maternal social support, quality of birth experience, and post-partum depression in primiparous women. J Matern-Fetal Neonatal Med. 2017;30(6):689–692. doi:10.1080/14767058.2016.1182980
44. Baas CI, Wiegers TA, de Cock TP, et al. Client‐related factors associated with a “less than Good” experience of midwifery care during childbirth in the Netherlands. Birth. 2017;44(1):58–67. doi:10.1111/birt.12266
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.