")
Back to Journals » Psychology Research and Behavior Management » Volume 14
How Patients with an Uncertain Diagnosis Experience Intolerance of Uncertainty: A Grounded Theory Study
Authors Yang Z , Zhao X, Zhu Z, Fu Y , Hu Y
Received 4 May 2021
Accepted for publication 30 July 2021
Published 12 August 2021 Volume 2021:14 Pages 1269—1279
DOI https://doi.org/10.2147/PRBM.S318263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Zhongfang Yang1,2 *, Xia Zhao3 *, Zheng Zhu,1,2 Yanfen Fu,4 Yan Hu1,2
1School of Nursing, Fudan University, Shanghai, People’s Republic of China; 2Fudan University Centre for Evidence-based Nursing: A Joanna Briggs Institute Centre of Excellence, Shanghai, People’s Republic of China; 3Peking Union Medical College Hospital, Beijing, People’s Republic of China; 4School of Nursing, Dali University, Dali, Yunnan, Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheng Zhu
School of Nursing, Fudan University, Shanghai, China; and Director of Fudan University Centre for Evidence-based Nursing: A Joanna Briggs Institute Centre of Excellence, 305 Fenglin Road, Xuhui District, Shanghai, 200032, People’s Republic of China
Tel +86 21-6443 0093
Email [email protected]
Purpose: To develop a conceptual framework to explain how patients with uncertain diagnoses experience intolerance of uncertainty (IU) in order to achieve an in-depth understanding of the process of facing uncertainty in this population.
Patients and Methods: A grounded theory study using semi-structured interviews was conducted with 21 patients with uncertain diagnoses in China from December 2018 to March 2019. The coding process followed the procedures of Strauss and Corbin: open coding, axial coding, and selective coding.
Results: We developed a conceptual framework called ‘Facing an Uncertain Diagnosis’. This framework considers not only the external and internal context of IU generation but also the ongoing process of how IU impacts patients’ psychological status, cognitive response, behavior, and decision making.
Conclusion: We suggest that healthcare professionals should be aware of the high level of IU and its psychological, cognitive, and behavioral manifestations in patients with uncertain diagnoses. Healthcare professionals should also be more cautious in shared decision making with patients with uncertain diagnoses.
Keywords: decision making, qualitative study, psychology research, behavior management
Introduction
Despite the rapid development of medical diagnosis technology, there are still many complex and rare diseases that cannot be clearly diagnosed. Large numbers of patients are repeatedly hospitalized to obtain a certain diagnosis and treatment.1,2 Uncertainty is inevitable, and dealing with uncertainty is part of daily life. However, a previous study showed that patients who are facing uncertain diagnosis and treatment measures had excessive, uncontrollable worry.3,4 Uncertain diagnoses are given when the clinician feels unable to provide an accurate explanation of a patient’s health condition, which may lead to the patient being unable to acquire a certain diagnosis or treatment activities.5 Regardless of the likelihood and consequences of the situation or event, this population is more likely to be intolerant of uncertainty. They consider uncertainty as unacceptable and seek to avoid it, which may challenge both patients’ and healthcare professionals’ patience, attitude, communication, and decision making.6
Intolerance of uncertainty (IU) is defined as a negative disposition toward uncertainty.7 Individuals with IU tend to react negatively to uncertain situations and the absence of information. IU has received increased attention in recent years.8 It is regarded as a critical construct in generalized anxiety and a causal mechanism of anxiety-related difficulties.9,10 Previous studies sought to examine the indirect and direct effects of IU on anxiety-related symptoms in both the general population and patients with generalized anxiety disorder.9,11 In addition, IU has a close relationship with other psychological symptoms, such as anxiety, worry, and depression.12 Therefore, it can be observed as an indicator across various diagnostic categories, including generalized anxiety disorder, obsessive-compulsive disorder, panic disorder, social phobia, and depressive disorder.13,14
Previous studies explored the levels of IU in various high-risk populations facing uncertainty. Kurita et al study identified a high level of IU in patients with lung cancer and found that a higher level of IU was associated with a higher perception of stress and poorer emotional well-being.15 Donthula et al found that patients with musculoskeletal symptoms had high a level of IU, and greater IU was associated with greater pain intensity.16 Other clinical populations without mental disorders, such as patients with cancer and chronic diseases, also showed severe IU.17–20
However, few studies have explored how IU impacts patients’ process of pursuing medical treatments, which may lead to failure to fundamentally solve the real clinical problems regarding IU. Patients who are repeatedly hospitalized without a certain diagnosis or treatments face uncertainty for a long period. Our previous study found that this population had higher levels of IU than their counterparts with clear diagnoses and treatment plans.21 It remains unknown how they experience IU and how IU impacts the process of their treatment, and data from the patient’s perspective are especially lacking.
Grounded theory is originated from symbolic interactions, which provide a method for researchers to explore how people explain, participate in, and respond to the social environment.22 Grounded theory can be used as a method for generating hypotheses from qualitative data.23,24 This method identifies inter-relationships by merging concepts, which could be useful in describing how patients with an uncertain diagnosis experience IU and how IU impacts their treatment. Therefore, the purpose of this qualitative study was to develop a conceptual framework based on the grounded theory approach to explain how patients with uncertain diagnoses experience IU in order to achieve an in-depth understanding of the process of facing uncertainty in this population.
Materials and Methods
Design
This qualitative study used grounded theory to generate a conceptual model of coping with uncertainty in patients who were repeatedly hospitalized without a definite diagnosis and who were intolerant of uncertainty.25 As a method of analyzing abundant qualitative data, grounded theory provides a set of systematic and flexible criteria for understanding a phenomenon’s real dynamics from the perspective of “duration”, “situation” and “interaction”. Researchers build conceptual frameworks based on semi-structured interviews with open-ended questions. The study goal was to describe how patients who were hospitalized without a definite diagnosis and who were intolerant of uncertainty cope with uncertainty. We followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) to ensure reporting quality.26
Participants
The study was undertaken at B Hospital, which is a tertiary hospital in BJ, China. The inclusion criteria were as follows: 1) age ≥18 years; 2) total number of admissions (including the number of hospital admissions in this institution and other hospitals) ≥ 2; 3) interval between this admission and the last admission less than 30 days; 4) the diagnosis of the disease was uncertain; 5) unable to bear uncertainty in at least one dimension based on the Chinese revised version of the Intolerance of Uncertainty Scale score (more than 21 points);27 and 6) voluntary participation in the study. The exclusion criteria included inability to be interviewed and complete the Intolerance of Uncertainty Scale owing to severe uncertain disease.
In this study, a theoretical sampling strategy was adopted to balance our sampling needs with the emerging theory. We adopted a three-wave scheme to utilize both purposive convenience sampling and homogenous sampling methods. Purposive convenience sampling was conducted to recruit participants according to their sex, age, educational attainment, geographical region, type of insurance, and number of hospitalizations in B and other hospitals. All personal information was collected from the Hospital Information System. Participants were sought until data saturation was achieved. Data saturation was assessed as follows: two researchers collected and analyzed the data at the same time and continuously compared the newly observed data with the results of previous analysis. If there was no new theme was generated from additional data, the saturation point was considered to have been reached.
Ethical Considerations
An informed consent form, which included the risks and benefits explanation, research purpose, research significance, interview duration, methods of data collection, disposal of the research results, and publication of anonymized responses, was provided to the participants. Both the researchers and participants signed the consent form before each interview. To protect the privacy of patients, the results of the study were all anonymous, and the names were replaced by numbers. If the participants did not want to continue the interview for some reason, they could withdraw from the study at any time. This ethical attitude informed the entire research process to ensure that respect, sensitivity and tact were demonstrated toward participants. The informed consent form and protocol for this study were reviewed and approved by the Institutional Review Board of the School of Nursing, Fudan University (IRB#TYSQ20200504). The study was conducted in accordance with the Declaration of Helsinki.
Data Collection
Based on the grounded theory qualitative research method, researchers conducted semi-structured interviews that were carried out in Chinese in a face-to-face manner from December 2018 to March 2019. The interviewers were the healthcare providers of the participants. The close relationships between the interviewer and interviewee enabled researchers to obtain in-depth qualitative data from the participants. Pilot interviews were conducted with five participants to clarify the interview questions based on their feedback. Eventually, we developed five open-ended questions: 1) What are your thoughts when you know the diagnosis is still uncertain? 2) How do you deal with this uncertain diagnosis? 3) How does uncertainty impact your daily life? 4) What is your opinion on your readmission to the hospital? 5) Whether the outcome is good or bad, what are your plans for the future?
The interviews were conducted by two researchers who had rich qualitative research experience. All the interviews were conducted in a quiet location convenient for the participants: two interviews were conducted in their private wards due to their physical condition, and nineteen were conducted in the conversation rooms. The place and time were established with the participants ahead of time. In the formal interviews, one researcher questioned the participants according to the interview outline. The other researcher made notes to supplement the audiotape and asked questions if she felt something had been missed. The whole process was audio-recorded with a recording pen. The length of the interviews ranged from 40 to 60 minutes.
Data Analysis
Recordings were transcribed verbatim in Mandarin by the third researcher (XZ). Two researchers read and checked the accuracy of the transcribed texts and verified the transcriptions with the interviewees to ensure the authenticity of the information. The analysis was conducted using the qualitative software, NVivo, version 11 (QSR International Pty Ltd., Melbourne, VIC, Australia). The coding process followed the procedures of Strauss and Corbin: open coding, axial coding, and selective coding. In the coding stage, two researchers read the data and conducted line-by-line coding individually.21 After all the coauthors reviewed the initial codes, two researchers moved to a more abstract and interpretive coding stage. The data were constantly compared and grouped into the primary and secondary categories. All coauthors reviewed the results and agreed on the final middle-range theory. Selected transcripts along with the initial codes were translated into English by the first author (ZY) and verified by the corresponding author (ZZ).
Measures to Ensure Data Validity
The data in this study mainly came from the semi-structured interviews. To reduce the recall error of the researchers, all recorded materials were transcribed word for word within 24 hours after the end of the interview. To ensure the rigor and trustworthiness of the analysis, the following strategies were adopted in this study: 1) two researchers (ZY & ZZ) extensively read the medical records of the participants to improve their understanding of the participants’ overall living environment and the development context of uncertainty; 2) reflection memos and audit trail were kept as supplementary files as the sources of data triangulation; 3) all the authors discussed categories, and middle-range theory until agreement was reached.
Results
Characteristics of Participants
Table 1 shows the participants’ characteristics. There were 11 (52.4%) women and 10 (47.6%) men. The participants were 38 years old on average, and their ages ranged from 18 to 67 years old. Participants’ level of education ranged from primary school to university degree. The majority of participants had urban employee basic medical insurance (n=14, 66.7%). Four participants (19.0%) paid out-of-pocket health care costs. The average number of inpatient admissions and outpatient visits at PUMCH were 1.9 and 18.1, respectively. The average number of hospital admissions to other hospitals was 1.9. The most common uncertain diagnosis at discharge were abdominal pain of unknown origin, fever of unknown origin, chronic diarrhea of unknown origin, and uncertain gastric cancer diagnosis.
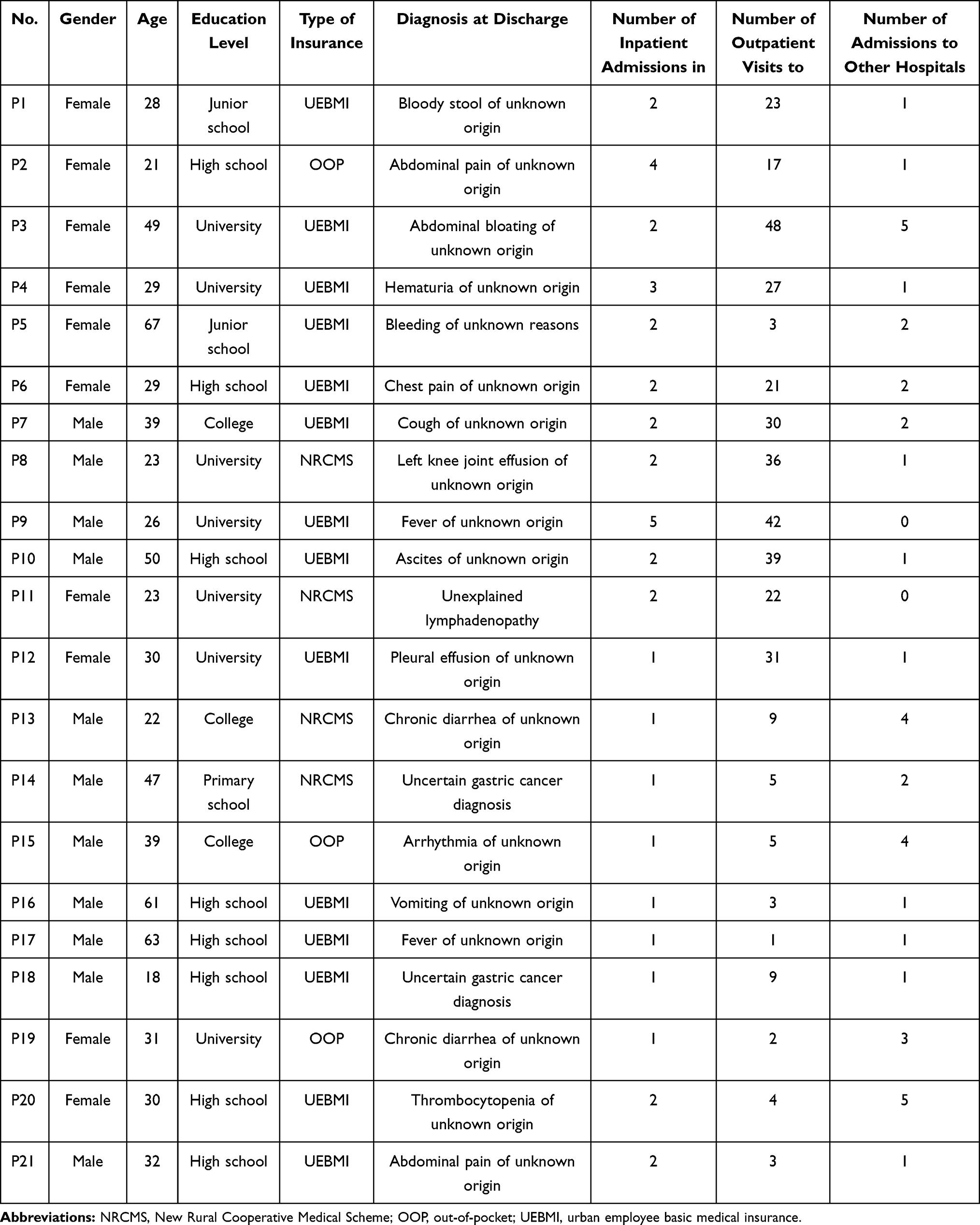 |
Table 1 Characteristics of the Participants (n=21) |
Findings
A middle-range theory, “Facing an Uncertain Diagnosis” (FUD), was derived from the qualitative data (Figure 1). This theory describes the process of how patients interact with their uncertain diagnosis and treatment. FUD has two major components: external context and internal processing. External context comprises the trigger factors generating patients’ IU, and internal processing reflects the psychological process by which patients handle their uncertain diagnosis and treatment. The external context and internal processing interact through complex pathways.
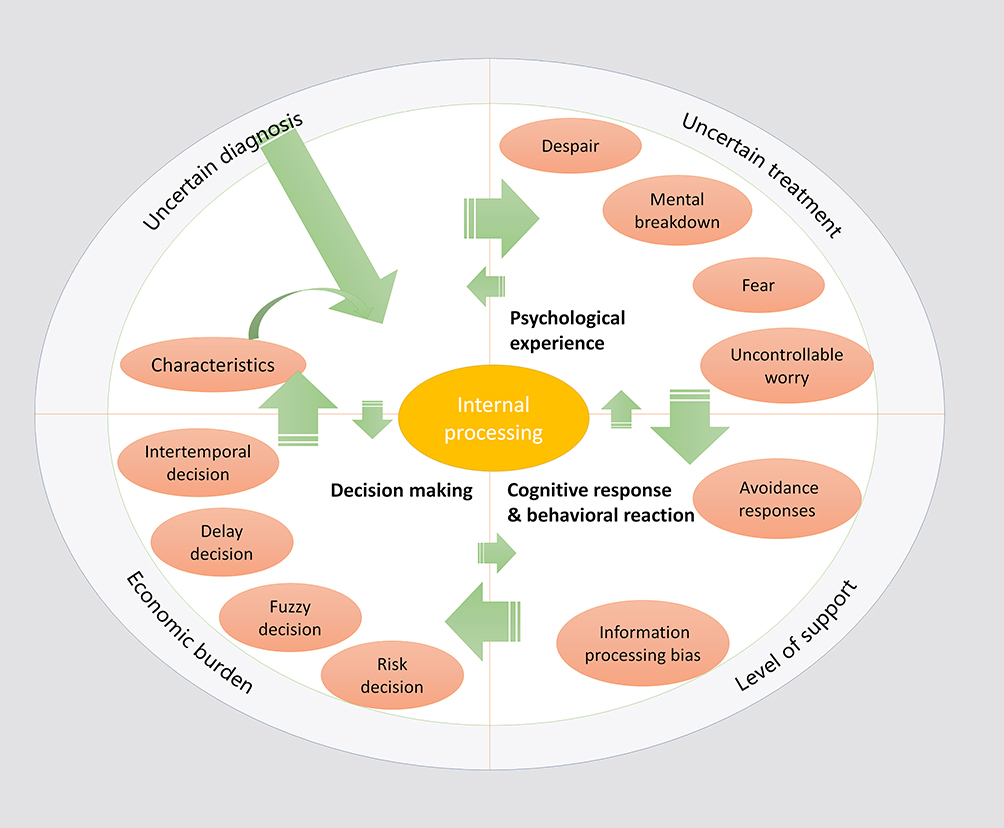 |
Figure 1 The conceptual framework of theory “Facing an Uncertain Diagnosis” (FUD). |
External Context
External context comprises the factors causing uncertainty and patients’ IU during the period of treatment. There were four major components of external context: uncertain diagnosis, uncertain treatment plan, level of support, and economic burden.
Uncertain Diagnosis
Uncertain diagnosis is a situation in which the patients do not receive a certain reply from their doctors about the diagnosis of their disease, which could disrupt the balance between hope and despair in the diagnostic phase. The participants had been repeatedly hospitalized to pursuit a certain diagnosis and treatment measures. They came to the hospital with hope but were discharged with an uncertain diagnosis multiple times. One participant (P16) said,
I came to this hospital from thousands of miles away with hope of receiving a certain diagnosis, but no concrete conclusion had been made at hospital discharge. I was in such despair. I don’t want to talk about this anymore. I don’t know what to do in the future.
They were often bothered by the conflicts between expectation and cold reality. One participant shared (P12),
I was very active in receiving treatment. My mother told me the doctor was specialized in this disease. I thought I would be cured this time, but it failed.
The doctor said I had a relapse. I couldn’t accept it. I don’t even know what’s wrong with my body? (P7)
It was clear across many participants that their emotional reactions were associated with their uncertain diagnosis. Healthcare providers’ words, reactions, and even expressions related to the uncertain diagnosis could be amplified and exaggerated in patients’ mind. For instance, one participant (P6) shared,
I told the doctor that my ejection fraction increased again, but he didn’t give me a clear statement. Their words were all in my head and drove me crazy … Even without a definite diagnosis, I hoped my doctor could give me some advice.
Uncertain Treatment
Patients’ IU could also come from uncertain treatment plans. There were three relevant scenarios. One was when the treatment plan was different from previous experience. Some patients may question the authenticity of a diagnosis and started to find the evidence from other sources to support their original hypothesized diagnosis. As a participant (P8) described,
Doctor A, whom I was seeing in my clinic, advised me to take this medicine, while doctor B advised me not to take this medicine … I believe doctor B is right. He seems to be more professional.
Another case was when the treatment plan was different from what the patient had read on the internet or heard from his or her ward-mates. Health information on the Internet has changed the way patients handle uncertain diagnoses with their healthcare providers. One participant said (P16),
I shared my current health conditions with a doctor on TikTok. He suggested me not to take the pills and start to use traditional Chinese medicine. This doctor had many followers. (what he said must be true)
Suggestions from other patients with similar manifestations could also impact participants’ perspectives on the uncertain disease. As shared by a participant (P21), “The pills my ward-mate took were different from what my doctor prescribed to me. I didn’t want to take it.”
The third case was when the treatment was not effective. Ineffective treatment may increase patients’ distrust in healthcare providers and enhance the level of uncertainty of future treatment. One participant (P9) stated,
In order to cooperate with the treatment, I dropped out of school for one year. But my disease has not been cured yet … This is the reason why I’m here. The doctors here are famous.
Level of Support
Lack of support can also increase patients’ IU. In this study, participants expressed concern about low levels of support from both health care professionals and family members. As one participant (P2) said, “I asked my doctor what the results meant. He was very impatient with me and urged me to leave soon. I really doubted the doctor’s suggestion.” Most participants living in rural areas had difficulty acquiring support. “I was worried about bleeding again when I got home, and no one could cope with the situation.” One participant (P5) expressed uncontrollable concern when he was informed about his discharge. One participant said (P10), “I don’t have confidence. I only have stress now because no one can help me.”
Economic Burden
Economic burden was another major source of IU. Most participants agreed that the hospitalization and treatment were very expensive. One participant (P14) described his worry about the economic burden caused by rushing from one hospital to another: “It was too expensive to stay in the hospital. If the doctor agreed, I would be discharged. There is no need to stay here anymore if nothing changed.” Another participant (P16) described stress from the same source: “I don’t know what to do next. Almost all the family’s savings were used up for my treatment.”
Internal Processing
Internal processing included four major components: 1) personal characteristics; 2) psychological experience; 3) cognitive response and behavioral reaction; and 4) decision making.
Personal Characteristics
As mentioned above, the external context comprised the trigger factors of IU. Personal characteristics were the most crucial factors determining the occurrence of IU. We found three major relevant characteristics: the gap between expectations and reality, psychological resilience, and levels of health knowledge.
Much of the IU stemmed from the gap between expectations and reality. Patients with uncertain diagnoses had high expectations when they were hospitalized. However, the reality sometimes was not in line with their expectations. In responses in this category, the phrase “I can’t take it” was frequently uttered. One participant (P11) said, “I kept exercising for half a year, but the doctor said I had a relapse and I couldn’t take it.” Another participant (P9) described a similar scenario: “I wished to find out what was wrong with me at that moment. But now it became the same as before. I can’t take it. I could not accept that at all.”
Psychological resilience was highly related to personal control capacity regarding IU. If the participants strengthened their resilience, they would develop a positive subjective state. One participant (P13) stated,
After all, I was not diagnosed with a terminal disease. I would have a good attitude and control myself from thinking about the unknown outcomes and go ahead bravely.
Another patient (P21) said, “I’m not afraid of it. I’m still in a good mood. If it was cancer, it would have been detected.”
As medical knowledge became accessible, patients’ vague knowledge of disease and treatment affected their trust in doctors, which led to uncertainty. As noted by a participant (P6),
I found ejection fraction on the test list. I searched information about ejection fraction on the Internet … Some information was different from what the doctor said. I don’t know which one to believe.
Psychological Experience
We found that four types of psychological experience appeared across participants: uncontrollable worry, fear, mental breakdown, and despair. Uncontrollable worry was the most mentioned emotion. This worry could come from uncertainty caused by financial issues, the recurrence of symptoms, or unknown test results. As stated by one participant (P18),
I am worrying about the money, because I don’t have enough money to cover hospitalization. But if the doctor could clearly identify my disease, I would sell my house.
One participant (P20) said, “I was worried about bleeding again. I couldn’t handle it.” A third participant (P15) said, “I felt like I was preparing for college entrance exam before the heart function test last week. I was worried that the examination result would be poor.”
Facing an uncertain diagnosis, some participants felt a sense of fear. This occurred when participants were hospitalized for the first time and when they thought the disease would make them uncomfortable for a long time in the future. One participant (P2) said, “I am scared. And this feeling is stronger and stronger as time goes on.” Another participant (P7) stated, “When I was hospitalized last time, I had a feeling that my body would become very vulnerable beyond my control. I was scared to death.”
Mental breakdown and despair occurred at the point when the participants were notified that they needed to be hospitalized with no certain diagnosis. As one participant (P1) shared, “I broke down and yelled at him (her husband).” Some participants described the days after they first heard about the uncertainty of the diagnosis. One participant (P17) shared, “When I heard the diagnosis, the feeling was painful. I was almost on the verge of desperation.” Another participant (P6) said, “When the doctor called me that day, he told me I would be hospitalized. I was going crazy. I asked him why I was going to be hospitalized again”.
Cognitive Response and Behavioral Reaction
Participants went through a wide range of cognitive processes in response to their emotional experience. There were two major cognitive responses and behavioral reactions: 1) avoidance responses, such as escapism, reduced compliance, and refusal to communicate, and 2) information processing bias that exaggerated their illness.
Participants described avoidance as a means of reducing their psychological discomfort due to fear, despair, and worry. Avoidance responses, such as escapism, reduced compliance, and refusal to communicate, were used to distract themselves from persistent feelings of psychological discomfort due to their uncertain diagnosis. One participant (P2) said, “I’ve been refusing all medical information from every source. I tried to forget this thing (being ill).” Some patients believed that the diagnosis was not definite and therefore they reduced their treatment compliance. As one participant (P1) shared, “Since I was discharged, I followed doctor’s orders to take medicine every day. But it did not work. I really do not want to do that anymore.” Some participants refused to communicate with their family members and friends when they had an uncertain diagnosis. One participant (P19) said, “Anyway, I just didn’t want to talk to anyone. I don’t know if they really understand me. I think it’s better not to talk.”
Many participants had information processing bias, which, in this case, manifested as exaggerating their illness. For instance, one participant (P9) said, “The doctor said that I couldn’t live the same life after I got sick. I thought I must have some incurable disease.” Another participant (P2) shared,
That day, the doctor said that I had done all kinds of tests (but they did not show concrete results). I think I must have cancer. I was so desperate that I felt I could not fall asleep for two days.
Decision Making
The process of facing uncertainty ultimately leads to four types of decision modes: intertemporal, fuzzy, risk, and delayed. Some participants made intertemporal decisions to acquire the greatest benefits. One participant (P3) shared, “I would not decide what to do until I saw my pathology report. Now I just want to wait in peace.” When the information acquired from the doctor was not clear and incomplete, some participants would not make decisions by themselves anymore and fell into confusion. A participant (P11) shared,
The doctor told me to be discharged and I did as he said. After discharge, I took care of myself and my family. I don’t know which way I should go. It seems what I have done is useless.
Risk decisions emerged when participants developed uncertainty. A participant (P4) shared, “The doctor said I might have cancer and asked me for my thoughts. At that moment, I decided to give up my treatment.” Some participants delayed the decision process to push back uncertainty for a reasonable time. As one participant (P10) shared, “I thought I should calm down first and accepted the situation. It was better to decide what to do later.”
Discussion
In this grounded theory study, we developed a conceptual framework called “Facing an Uncertain Diagnosis” (Figure 1). This framework depicts not only the external and internal context of IU generation but also the ongoing process of how IU impacts patients’ psychological status, cognitive response, behavior, and decision making. The conceptual framework is composed of two sections: external context and internal processing. Although external context and internal processing seem to be separate on the surface, the external and internal factors influence each other to some degree. It is considered that the relationships among an individual’s emotions, cognitions, behaviors and outside environment are mutually influential; thus, the individual and his or her environment constitute a dynamic and constantly changing system. Regarding internal processing, based on external contexts, personal characteristics are a crucial factor determining the occurrence of IU and are regarded as the beginning point of the process of facing an uncertain diagnosis. This cyclical process view is congruent with other IU frameworks, such as the relational map of fearing unknowns and intolerance of uncertainty and the new cognitive-behavioral conceptualization of intolerance of uncertainty and generalized anxiety disorder symptoms, both of which describe the process of facing uncertainty as a cycle in nature.28,29 The occurrence of IU first impacted individuals’ psychological status and then affected their cognition and behaviors. IU finally influenced the style of individuals’ decision making, which was a crucial component of patients receiving healthcare support. The proposed framework can help researchers develop an intervention targeting IU in patients with uncertain diagnoses. To weaken or prevent adverse consequences in the context of an uncertain diagnosis, it is especially important to intervene in the external context, internal processing, and any steps in the internal processing. This framework can also sensitize health care professionals to the identification of IU and its associated factors.
The findings from the study suggested that patients with uncertain diagnoses who have IU show a series of deviations in terms of psychological status, including worry, fear, mental breakdown, and despair. These experiences were widespread across participants. The results were consistent with previous studies showing that IU is directly linked to negative emotions, including anxiety and worry.30,31 IU is regarded as a major factor in the etiology of generalized anxiety disorder and is considered a transdiagnostic mechanism of multiple anxiety-related symptoms based on recent evidence.13 Moreover, we found that some patients with uncertain diagnoses had, in addition to anxiety-related experience, an experience of mental breakdown when they had endured the negative experience for a long period of time. This was possibly due to both the external context and personal characteristics of patients. Patients’ psychological resilience, their level of knowledge, the gap between their expectations and reality, their financial burden, and their subjective social support determined how they handled IU. Therefore, we suggest that healthcare professionals should provide adequate, specific, and targeted information for patients seeking medical treatment with a positive and encouraging attitude. Communicating effectively with patients and developing an optimistic attitude will have a direct effect on improving patients’ IU.
If patients’ deviations in psychological status were not detected and treated, a series of cognitive responses and behavioral reactions would emerge, such as communication refusal, treatment abandonment, communication misunderstandings, and illness exaggeration. These findings were in line with previous studies showing that IU is a vulnerability factor for excessive and inflexible avoidance behaviors.32–34 Our study further indicated that IU could be associated with not only avoidance behaviors but also information processing bias, both manifestations of several mental disorders. We suggest that healthcare professionals need to recognize patients’ avoidance behaviors and be aware of their statements’ authenticity. If necessary, providing patients cognitive-behavioral therapy to alleviate their anxiety symptoms and deviant behaviors is highly recommended in existing guidelines.35,36
Moreover, we found that some patients with uncertain diagnoses tended to avoid making decisions or selected immediately available but high-risk choices, especially patients with a series of negative psychological experiences and avoidance responses. This phenomenon may be due to these populations having high levels of IU. Previous studies stated that individuals with higher levels of IU make poorer decisions and are more behaviorally inhibited in unpredictable situations.37 Poor decision making could be regarded as the behavioral consequence of IU, manifesting as avoidance of potential future threats by making delayed, intertemporal, and fuzzy decisions.37,38 Additionally, such decision making could be described as a method of reducing uncertainty about one’s options. Roughly making quick decisions may reduce uncertainty but never eliminates it.34 Regardless of the decision-making style adopted in this study, they all limit the effectiveness and efficiency of decision-making and create unacceptable dangers for both patients and healthcare professionals. Therefore, we recommend that healthcare professionals exercise caution regarding patients’ decision-making styles when implementing shared decision-making among patients with uncertain diagnoses.
Limitations
This is the first study to develop a conceptual framework to explain how patients with uncertain diagnoses and who are intolerant of uncertainty face uncertainty. There were some limitations. First, the conclusion of this study was based on interview data from 21 patients who were all recruited from the same hospital, which may limit the external validity of this study. In addition, this study conducts theoretical research from the perspective of patients and lacks diversified explanations of the same issue from other perspectives (medical staff, patients’ families, etc.). Therefore, subsequent studies need to integrate multiple perspectives.
Conclusions
This is the first study to develop a middle-range theory on the process of how patients with uncertain diagnoses and intolerance of uncertainty face uncertainty. The conceptual framework of the theory, “Facing an Uncertain Diagnosis”, showed the external and internal contexts of IU generation and the ongoing process of how IU impacts patients’ psychological status, cognitive response, behavior, and decision making. The proposed framework can sensitize health care professionals to the identification of IU and its associated factors and help researchers develop an intervention targeting IU in the external context, internal processing, and any steps in the internal processing. We suggest that healthcare professionals, including physicians, nurses, and clinical consulting psychologists, should provide adequate, specific, and targeted information for patients seeking medical treatment with a positive and encouraging attitude. Communicating effectively with patients and developing an optimistic attitude would have a direct effect on patients’ negative psychological experiences, cognitive responses, and behavioral reactions. Cognitive-behavioral therapy is recommended for patients with high levels of IU to alleviate their anxiety symptoms and deviant behaviors. Healthcare professionals should also be cautious to shared decision making with patients with uncertain diagnoses due to their avoidant and risky decision style.
Acknowledgment
We thank all participants who were interviewed in this study.
Funding
This work is supported by the Shanghai Soft Science Research Program (20692190300), the Ministry of Education of Humanities and Social Science Project (20YJCZH254), and the Fudan-Fosun Nursing Research Fund (FNF201951). The funders had no involvement in or influence on this study.
Disclosure
All authors declare that they have no competing interests.
References
1. Sump CA, Marshall TL, Ipsaro AJ, et al. Uncertain diagnoses in a children’s hospital: patient characteristics and outcomes. Diagnosis. 2020.
2. Yan C, Lindgren H, Nieves JC. A dialogue-based approach for dealing with uncertain and conflicting information in medical diagnosis. Auton Agent Multi Agent Syst. 2018;32(6):861–885.
3. Counsell A, Furtado M, Iorio C, et al. Intolerance of uncertainty, social anxiety, and generalized anxiety: differences by diagnosis and symptoms. Psychiatry Res. 2017;252:63–69.
4. Wahlund T, Andersson E, Jolstedt M, et al. Intolerance of uncertainty-focused treatment for adolescents with excessive worry: a Pilot Feasibility Study. Cogn Behav Pract. 2020;27(2):215–230.
5. Bhise V, Rajan SS, Sittig DF, Morgan RO, Chaudhary P, Singh H. Defining and measuring diagnostic uncertainty in medicine: a systematic review. J Gen Intern Med. 2018;33(1):103–115.
6. Bhise V, Meyer AND, Menon S, et al. Patient perspectives on how physicians communicate diagnostic uncertainty: an experimental vignette study. Int J Qual Health Care. 2018;30(1):2–8.
7. Buhr K, Dugas MJ. The role of fear of anxiety and intolerance of uncertainty in worry: an experimental manipulation. Behav Res Ther. 2009;47(3):215–223.
8. Bhise V, Rajan SS, Sittig DF, et al. Defining and measuring diagnostic uncertainty in medicine: a systematic review. J Gen Intern Med. 2018;33(1):103–115.
9. Cowie J, Clementi MA, Alfano CA. Examination of the intolerance of uncertainty construct in youth with generalized anxiety disorder. J Clin Child Adolesc Psychol. 2018;47(6):1014–1022.
10. Laposa JM, Fracalanza K. Does intolerance of uncertainty mediate improvement in anger during group CBT for GAD? A preliminary investigation. Behav Cogn Psychother. 2019;47(5):585–593.
11. Kusec A, Tallon K, Koerner N. Intolerance of uncertainty, causal uncertainty, causal importance, self-concept clarity and their relations to generalized anxiety disorder. Cogn Behav Ther. 2016;45(4):307–323.
12. Jensen D, Cohen JN, Mennin DS, Fresco DM, Heimberg RG. Clarifying the unique associations among intolerance of uncertainty, anxiety, and depression. Cogn Behav Ther. 2016;45(6):431–444.
13. Gillett CB, Bilek EL, Hanna GL, Fitzgerald KD. Intolerance of uncertainty in youth with obsessive-compulsive disorder and generalized anxiety disorder: a transdiagnostic construct with implications for phenomenology and treatment. Clin Psychol Rev. 2018;60:100–108.
14. Kim MK, Lee KS, Kim B, Choi TK, Lee SH. Impact of mindfulness-based cognitive therapy on intolerance of uncertainty in patients with panic disorder. Psychiatry Investig. 2016;13(2):196–202.
15. Kurita K, Garon EB, Stanton AL, Meyerowitz BE. Uncertainty and psychological adjustment in patients with lung cancer. Psychooncology. 2013;22(6):1396–1401.
16. Donthula D, Kortlever JTP, Ring D, Donovan E, Reichel LM, Vagner GA. Does intolerance of uncertainty affect the magnitude of limitations or pain intensity? Clin Orthop Relat Res. 2020;478(2):381–388.
17. Eisenberg SA, Kurita K, Taylor-Ford M, Agus DB, Gross ME, Meyerowitz BE. Intolerance of uncertainty, cognitive complaints, and cancer-related distress in prostate cancer survivors. Psychooncology. 2015;24(2):228–235.
18. San Martín C, Jacobs B, Vervliet B. Further characterization of relief dynamics in the conditioning and generalization of avoidance: effects of distress tolerance and intolerance of uncertainty. Behav Res Ther. 2020;124:103526.
19. Alschuler KN, Beier ML. Intolerance of uncertainty: shaping an agenda for research on coping with multiple sclerosis. Int J MS Care. 2015;17(4):153–158.
20. Rasmussen NH, Smith SA, Maxson JA, et al. Association of HbA1c with emotion regulation, intolerance of uncertainty, and purpose in life in type 2 diabetes mellitus. Prim Care Diabetes. 2013;7(3):213–221.
21. Zhao X, Zhu Z, Yu M, et al. The experience of intolerance of uncertainty in patients with no clear diagnosis: a qualitative study. Chinese J Nursx. 2020;55(04):488–493.
22. Blumer H. Symbolic Interactionism: Perspective and Method. University of California Press; 1986.
23. Morse JM, Stern PN, Corbin J, et al. Developing Grounded Theory: The Second Generation. Walnut Creek, Calif: Routledge; 2009.
24. Timonen V, Foley G, Conlon C. Challenges when using grounded theory: a pragmatic introduction to doing GT research. Int J Qualitative Methods. 2018;17(1):16094069–18758086.
25. Strauss AL, Corbin JM. Grounded theory in practice. Contemp Sociol. 1997;28(4):296.
26. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357.
27. Yang Z. Psychometric properties of the Intolerance of Uncertainty Scale (IUS) in a Chinese-speaking population. Behav Cogn Psychother. 2013;41(4):500–504.
28. Carleton RN. Into the unknown: a review and synthesis of contemporary models involving uncertainty. J Anxiety Disord. 2016;39:30–43.
29. Hebert EA, Dugas MJ. Behavioral experiments for intolerance of uncertainty: challenging the unknown in the treatment of generalized anxiety disorder. Cogn Behav Pract. 2019;26(2):421–436.
30. Dar KA, Iqbal N, Mushtaq A. Intolerance of uncertainty, depression, and anxiety: examining the indirect and moderating effects of worry. Asian J Psychiatr. 2017;29:129–133.
31. Wright CJ, Clark GI, Rock AJ, et al. Intolerance of uncertainty mediates the relationship between adult attachment and worry. Pers Individ Dif. 2017;112:97–102.
32. Flores A, López FJ, Vervliet B, et al. Intolerance of uncertainty as a vulnerability factor for excessive and inflexible avoidance behavior. Behav Res Ther. 2018;104:34–43.
33. Neville A, Kopala-Sibley DC, Soltani S, et al. A longitudinal examination of the interpersonal fear avoidance model of pain: the role of intolerance of uncertainty. Pain. 2021;162(1):152–160.
34. Jensen D, Kind AJ, Morrison AS, et al. Intolerance of uncertainty and immediate decision-making in high-risk situations. J Exp Psychopathol. 2014;5(2):178–190.
35. Talkovsky AM, Norton PJ. Negative affect and intolerance of uncertainty as potential mediators of change in comorbid depression in transdiagnostic CBT for anxiety. J Affect Disord. 2018;236:259–265.
36. Torbit L, Laposa JM. Group CBT for GAD: the role of change in intolerance of uncertainty in treatment outcomes. Int J Cogn Ther. 2016;9(4):1–13.
37. Carleton RN, Duranceau S, Shulman EP, Zerff M, Gonzales J, Mishra S. Self-reported intolerance of uncertainty and behavioural decisions. J Behav Ther Exp Psychiatry. 2016;51:58–65.
38. Hunt C, Cooper SE, Hartnell MP, Lissek S. Anxiety sensitivity and intolerance of uncertainty facilitate associations between generalized Pavlovian fear and maladaptive avoidance decisions. J Abnorm Psychol. 2019;128(4):315–326. Available from: https://psycnet.apa.org/record/2019-11183-001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.