")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
How Employees in a Comprehensive Public Hospital Perceive Corruption Risks: A Survey Study in China
Authors Chen Y , Cui X, Zhuoma J, Zhu F, Luo L, Xie J, Cheng Y
Received 16 October 2021
Accepted for publication 29 January 2022
Published 23 February 2022 Volume 2022:15 Pages 299—309
DOI https://doi.org/10.2147/RMHP.S344782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Video abstract presented by Yan Chen.
Views: 295
Yan Chen,1,2 Xinyu Cui,2 Jiahuan Zhuoma,2 Fang Zhu,2 Li Luo,3 Juan Xie,2 Yongzhong Cheng2
1Institute of Hospital Management, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 2The Commission for Discipline Inspection, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 3Industrial Engineering and Engineering Management Department, College of Business of Sichuan University, Chengdu, People’s Republic of China
Correspondence: Li Luo; Juan Xie, Industrial Engineering and Engineering Management Department, Business School of Sichuan University, Chengdu, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To examine how employees perceive corruption risks in their hospital and to provide recommendations for good governance in that hospital.
Methods: The “Questionnaire of Corruption Risk Perception Index in Public Hospitals” was designed and a questionnaire survey was conducted online from April 17 to 30, 2020 in West China Hospital of Sichuan University, to explore employees’ assessment of corruption risk. Employees were asked to evaluate the likelihood and impact of corruption risk to form a corruption risk perception index (CRPI). Related factors were examined in multifactor analysis.
Results: A total of 5525 employees participated in the survey. Among all 15 kinds of risks, unreasonable personnel changes (CRPI=8.24), no collective discussion about important issues (CRPI=7.95), and violating the individual moral character (CRPI=7.85) were the top 3 ones that participants rated highest, while illegal procurement (CRPI=7.38), violating teaching ethics (CRPI=7.12) and medical ethics (CRPI=6.93) were rated lowest. Corruption risks were mainly concentrated in internal management, treatment regulation, professional conduct, and external cooperation. The OR value that the CRPI of leaders was 0.768 times that of ordinary employees (95% CI: 0.623– 0.945, χ 2=6.189, P=0.013). Fluke ideas were the most selected personal reason for corruption. Suggestions for strengthening the education of corruption risk were mentioned most.
Conclusion: The results indicate the emphasis and direction of hospital management. First, WCH needs to pay attention to the construction and dynamic improvement of the hospital’s internal management regulations and external cooperation management regulations, and increase the transparency of decision-making and implementation. Second, it is necessary to restrict the discretion of leaders at all levels and strengthen supervision. In addition, WCH needs to carry out education from the perspectives of power awareness and corruption cost, and to strive to build a clean, honest culture.
Keywords: corruption risk perception index, corruption risk, anti-corruption, public hospital
Introduction
Transparency International (TI) defines corruption as “the abuse of entrusted power for private gain”.1 In China, the definition of corruption encompasses almost any form of “misconduct”.2 In addition to bribes, there are other corrupt manifestations related to public hospital staff, such as the theft of supplies and equipment, overbilling, unfair hiring practises,3 the embezzlement of research funds,4 absenteeism, informal payments, and dual practise.5–7 Corruption includes a series of extensive practices ranging from unethical behavior, and administrative misconduct to direct criminal offenses.8,9 To reduce corruption, the risks of corruption need to be identified and controlled as early as possible. As public hospital employees are potential subjects of corruption, the identification and perception of corruption risks by employees also require attention.
It is critical and necessary to assess the risk of corruption in public hospitals. The World Bank proposed that corruption risk assessment is the widespread evaluation of the level of governance.10 The worse regional governance is, the greater the risk of corruption.11 This evaluation also helps with transparency. Arostegui mentioned that citizens’ perceptions of corruption tend to change as the government undertakes reforms to control corruption.12 Additionally, corruption risk assessment is considered an anti-corruption intervention and an innovative method. The United Nations Development Fund (UNDP), the Council of Europe, the United States Agency for International Development (USAID) and others have assessed corruption risk in the health sector in Rwanda and Kosovo.7 According to Vian T, in the Middle East and North Africa (MENA), the UNDP is working on corruption risk mapping as part of long-term engagement based on prevention, risk management, and multistakeholder engagement.7 Mostafa Hunter developed the Conceptual Framework for Corruption Risk Assessment at the Sectoral Level as an approach to tackle corruption and enhance transparency and accountability in health care in Arab countries.13 However, previous studies have mainly focused on medical corruption at the regional or national levels, and anti-corruption tools are mostly based on large environments such as the health care industry, and the interactions between hospitals and enterprises.7,14 There is a lack of research on the corruption risk perceptions of public hospital staff.
To examine how employees perceive corruption risks in their hospital, we designed the “Questionnaire of Corruption Risk Perception Index in Public Hospitals” based on common types of corruption in public hospitals, and conducted a cross-sectional survey at West China Hospital (WCH) of Sichuan University. WCH is a large general public hospital and is one of 44 hospitals managed by the National Health Commission of the People’s Republic of China (PRC). It has 4300 beds and 7910 staff. With its functions of medicine, teaching, research and administration, WCH has a profound social influence in China, especially in the western region. Accordingly, due to the diversity and complexity of the work, employees (especially leaders at all levels at WCH) are exposed to a certain degree of corruption risk. The leadership structure in this hospital includes heads of the hospital, heads of administrative departments/clinical departments/laboratories (hereafter “departments”), deputy heads of departments, area leaders of departments, and leaders of professional teams (explanations are provided in Supplementary File 1). Generally, heads of the hospital, and heads and deputy heads of departments are referred to as the hospital’s core leaders; area leaders and professional team leaders are referred to as ordinary leaders. Understanding the corruption risk perception the hospital’s employees—especially leaders— can, to a certain extent, reflect awareness of corruption risks within the hospital among employees of Chinese public hospitals and provide a basis for further anti-corruption efforts.
Materials and Methods
Survey Instrument
Common individual corrupt practices are the focus of corruption research and intervention.15 To understand employees’ perceptions of corruption risks in public hospitals and to compare differences among employees with different characteristics, we developed a questionnaire based on information from five aspects: (1) manifestations of corruption (especially those in high-risk areas);16 (2) common corruption cases reported in the news; (3) criminal judgements made in China; (4) relevant research papers; and (5) key points of anti-corruption management in Chinese health care. TI defines corruption risk as the potential probability that corruption may occur and the costs associated with it; an increase in corruption risk implies a greater probability of corruption or a higher potential cost, or both.17 Referring to Mostafa Hunter’s work on the development of a risk heatmap for the health care sector in Arab countries,13 we used two dimensions to evaluate corruption risk: (1) the likelihood of corruption occurring; and (2) the impact of corruption when it does occur. The participants had to evaluate the likelihood and impact of each risk, which were divided into five levels represented by 5, 4, 3, 2, and 1, representing highly possible, easy, possible, unlikely, extremely rare and very serious, relatively serious, generally serious, not too serious, and no impact, respectively.18 Corruption risk can be expressed as a factor of the likelihood (L) multiplied by the impact (I), thus providing a ranking score.16 We defined the result of multiplying L by I as the Corruption Risk Perception Index (CRPI) score. According to previous research, we divided the CRPI scores into five levels: negligible, minor, moderate, serious, and critical (the levels and connotations of CRPI are displayed in Table 1).16 Six participants with various job positions (ie, head of the hospital, head of a department, nurse, doctor, officer) and education levels (ie, college to Ph.D) were invited to comment on the questionnaire and classification criteria, which we then modified. Afterward, using convenience sampling, we recruited 12 participants in a pilot study to evaluate feasibility and to obtain further comments on the questionnaire and classification criteria. We asked the 12 participants to assess whether the questionnaire was well laid out, whether the questions were clearly stated and easy to answer, and whether the classification criteria were reasonable (details are outlined in Supplementary File 2).
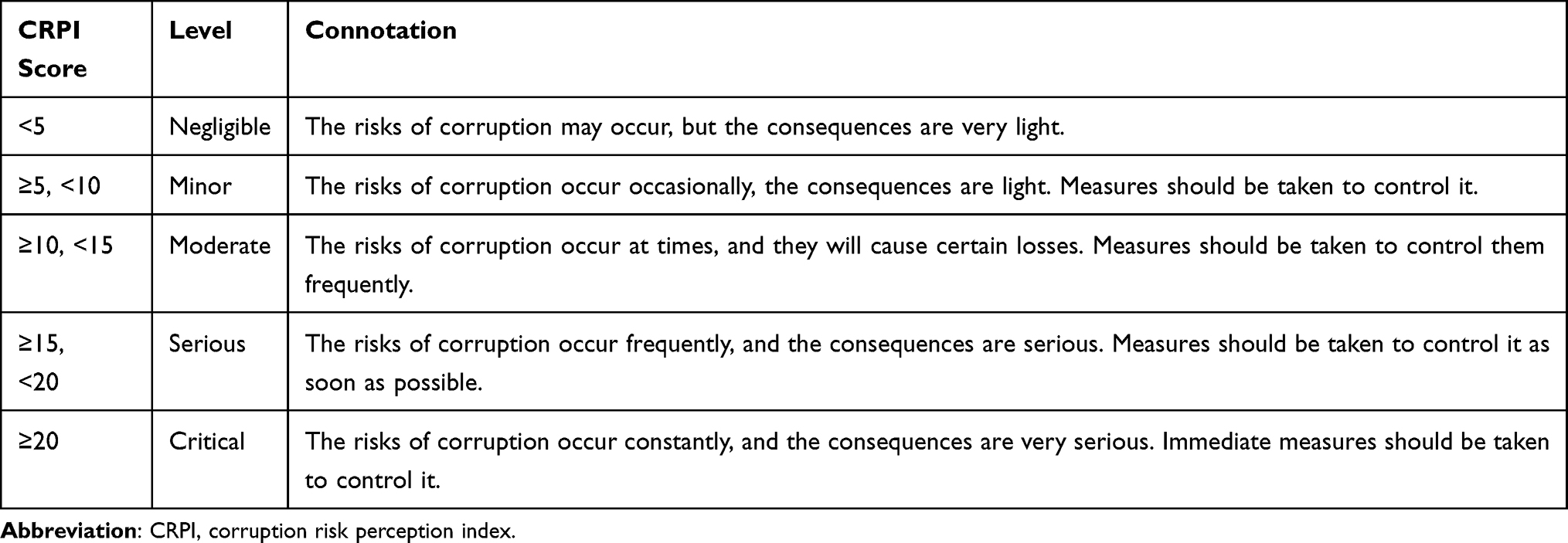 |
Table 1 The Levels and Connotations of the Corruption Risk Perception Index (CRPI) |
The final version of the questionnaire is titled the “Questionnaire of Corruption Risk Perception Index in Public Hospitals”. It consists of four parts: (1) sociodemographic characteristics, with 7 items including gender, age, years of work experience, unit type, professional title, occupation, and leadership; (2) an assessment of 15 corruption risks with which most hospital employees are familiar (Table 2); (3) potential personal causes of corruption with 3 items, including poor understanding of management regulations, fluke ideas, and inadequate supervision; and (4) the most desired learning content about anti-corruption efforts, including 3 items including rules about behavior, punishment regulations, and the revelation of corruption cases. In addition, we asked the participants to give suggestions for future.
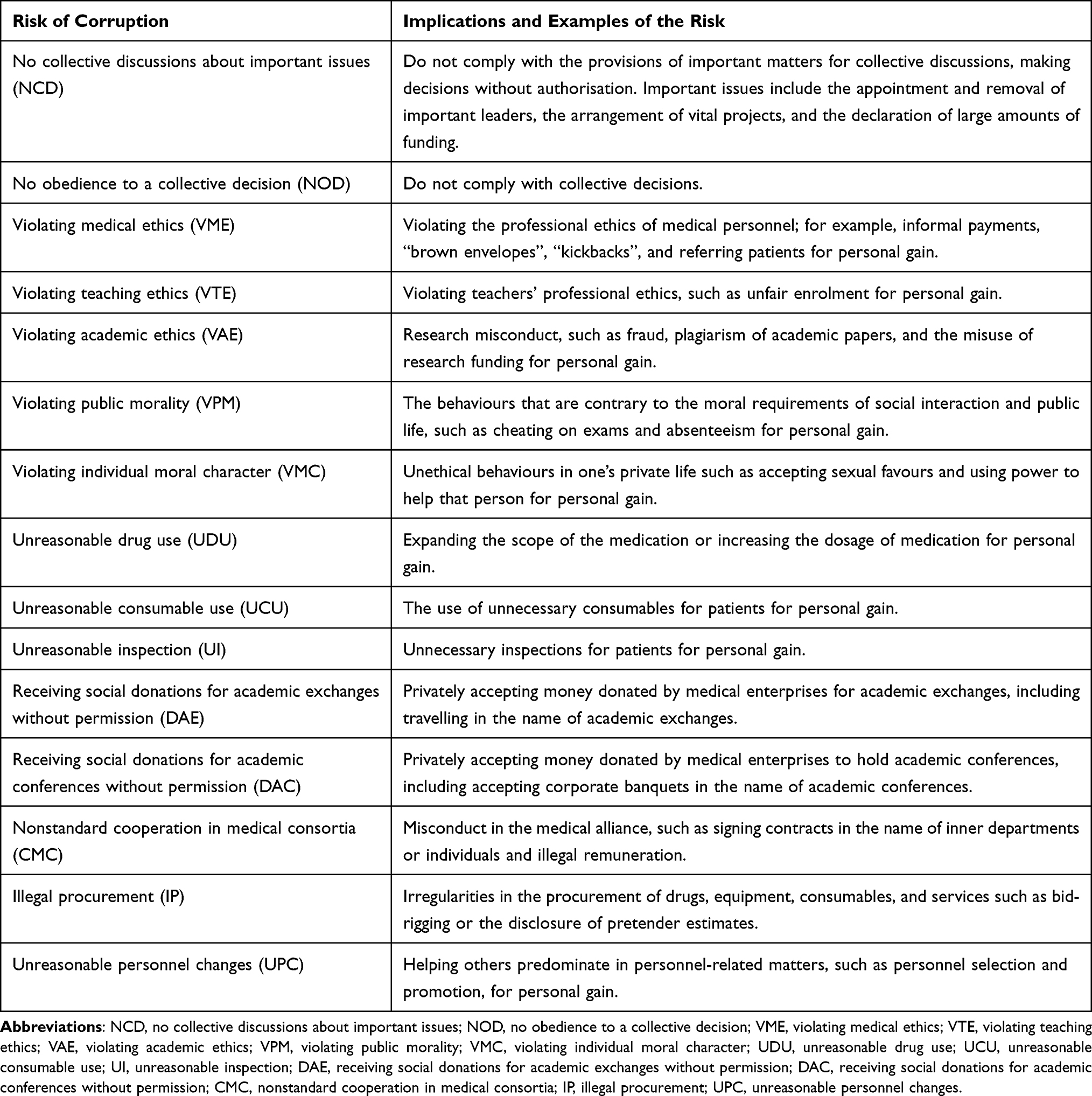 |
Table 2 Fifteen Common Corruption Risks in China’s Public Hospitals |
Data Collection and Analysis
We submitted the present study to WCH for approval and received it. To understand the true level of employees’ perceptions about the risk of corruption, we used an online survey format to avoid the oppressive feeling that a face-to-face survey may bring to employees. We used the software “WJX.CN” (Wenjuanxing) for data collection. This software formed a link that included survey invitations, confidentiality principles, and electronic questionnaires. We sent the link to employees on the hospital’s corporate WeChat platform (the platform incorporates all employees of the hospital, and each employee can send messages directly to other employees who are on the same platform). After the employees filled out the questionnaire, we fed the information directly into Wenjuanxing. No one except the research team knew the results of the responses.
All employees at WCH—including medical, administrative, teaching and research employees, except for interns—were eligible for the study. We adopted convenience sampling to obtain as many samples as possible. As we did not form any hypotheses, we did not estimate the sample size. To develop the study’s effectiveness and accuracy, we asked no less than two-thirds of employees in each department (5273 employees in total) to participate. We conducted the online, cross-sectional survey from 17 to 30 April, 2020. Before the investigation, we introduced a clear background explanation and set up the informed consent option for selection. If people did not want to participate, they could quit directly. We strictly adhered to the guidelines on research involving the use of human subjects based on the Helsinki Declaration, and we received approval for the ethics of the study.
Statistical Analysis
We exported the data to Excel 2016 and used IBM SPSS Statistics for Windows, Version 25.0 (SPSS, Inc., Chicago, IL, USA) to examine the results. The data are described as the mean, median, and quartile. We used hierarchical cluster analysis (Ward’s method and squared Euclidean distance interval measurement) to cluster the dimensions. We employed the Mann–Whitney U rank-sum test and the Kruskal–Wallis H rank-sum test to analyse the distribution of the CRPI among people with different characteristics. After we graded the CRPI, we used ordered multinomial logistic regression for multifactor analysis.
Results
CRPI Ratings and Dimensions
Among all staff, a total of 5552 employees agreed to participate, of which 5525 responses were valid. The response rate was 69.85%; the characteristics of the respondents are reported in Table 3. Cronbach’s α of the questionnaire was 0.836. All participants evaluated that the average likelihood score of corruption risk in the hospital was 1.71, the impact score was 4.45, and the average CRPI was 7.57. Among all 15 risks, unreasonable personnel changes (CRPI=8.24), no collective discussions about important issues (CRPI=7.95), and violating individual moral character (CRPI=7.85) were the top three which participants rated the highest, while illegal procurement (CRPI=7.38), violating teaching ethics (CRPI=7.12) and violating medical ethics (CRPI=6.93) were rated the lowest (Table 3).
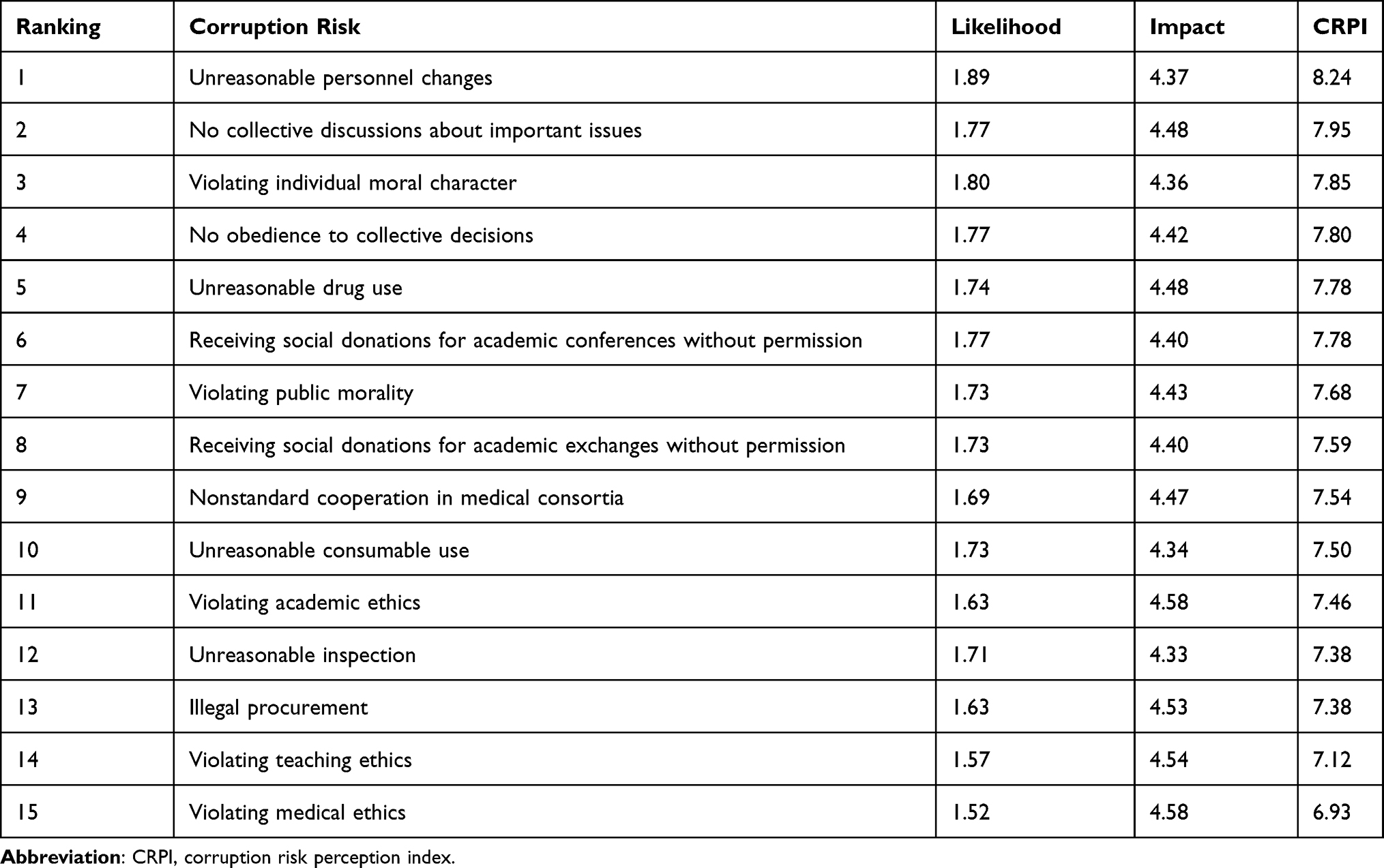 |
Table 3 Ranking of CRPI Scores for 15 Types of Corruption Risk |
The results of cluster analysis indicate that the corruption risks of WCH were mainly concentrated in four major areas: (1) internal management (collective discussions, employing and retaining people, obeying decisions); (2) treatment regulation (rational drug use, rational inspection, and the rational use of consumables); (3) professional conduct (social morality, life morality, medical ethics, teachers’ morality, and academic ethics); and (4) external cooperation (accepting social donations for academic exchanges or academic conferences, bidding and cooperation among medical associations) (Figure 1).
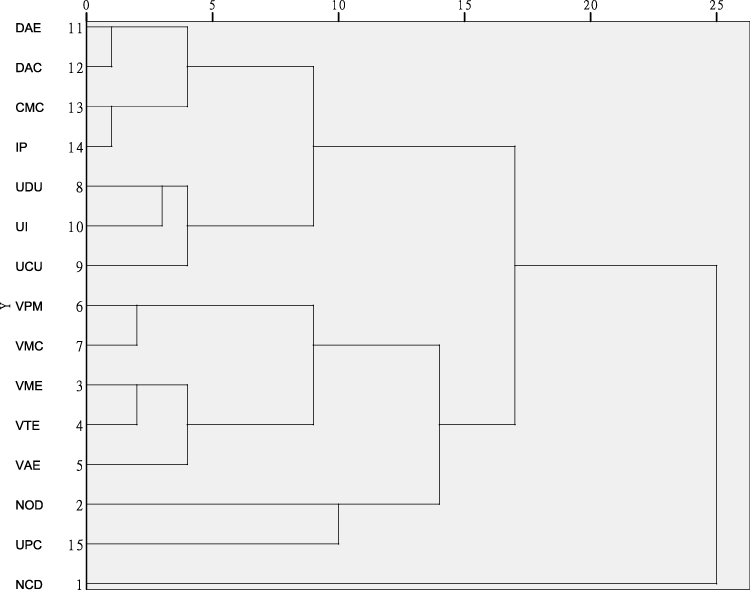 |
Figure 1 Cluster analysis plot for the CRPI. Abbreviations: DAE, receiving social donations for academic exchanges without permission; DAC, receiving social donations for academic conferences without permission; CMC, nonstandard cooperation in medical consortia; IP, illegal procurement; UDU, unreasonable drug use; UI, unreasonable inspection; UCU, unreasonable consumable use; VPM, violating public morality; VMC, violating individual moral character; VME, violating medical ethics; VTE, violating teaching ethics; VAE, violating academic ethics; NOD, no obedience to a collective decision; UPC, unreasonable personnel changes; NCD, no collective discussions about important issues. |
The CRPI Distribution Difference
The CRPI distribution of employees with different genders, ages, years of work experience, professional titles, and occupations was significantly different, while there was no obvious difference between that of different unit types (H=0.618, P=0.734). Among all participants, the CRPI of males was higher than that of females (U=2794928.500, P=0.000). The distribution of the CRPI in different age groups (H=87.637, P=0.000) was different, and the CRPI of workers over age 40 was significantly higher than that of workers under 40. The distribution of the CRPI in groups with different years of work experience (H=87.637, P=0.000) was different, and the CRPI of those with more than 20 years of work experience was significantly higher than that of people with less than 20 years of experience. The professional title groups (H=178.635, P=0.000) also had significantly different CRPIs. There were significant differences in the CRPI distribution among workers of each occupation (H=136.925, P=0.000); doctors scored highest (M=8.000), while nurses scored lowest (M=6.89) (Supplementary File 3).
Being a leader was also one of the influencing factors of CRPI. Leaders had a greater CRPI score than clerks (U=2012206.500, P=0.000). The CRPI of leaders with ≥2 titles was higher than that of leaders with 1 title (U=38588.000, P=0.004). Length of leadership also led to a different distribution of a leader’s CRPI (H=9.061, P=0.028). The distribution of the CRPI in different position groups varied (H=77.089, P=0.000), and the CRPI of core leaders (including hospital heads, as well as heads and deputy heads of departments) was significantly higher than that of ordinary leaders (including area leaders of departments and leaders of a professional team). Hospital heads had the highest CRPI score (M=13.1650), which was much higher than that of the other groups (Supplementary Files 3 and 4).
The results of ordered multinomial logistic regression revealed that for all participants, being a leader was the key factor. The OR value of the CRPI of leaders was 0.768 times that of ordinary employees (95% CI: 0.623–0.945, χ2=6.189, P=0.013) (Table 4). For leaders, the position grade was the main point. The OR value of the CRPI of hospital heads was 28.552 times that of professional group leaders (95% CI:4.222–193.095, χ2=11.812, P=0.001), and the OR value of the CRPI of deputy heads was 2.217 times that of professional group leaders (95% CI: 1.046–4.699, χ2=4.320, P=0.038) (Table 5).
 |
Table 4 Final Model of Variables Associated with Participants’ CRPI (N=5525) |
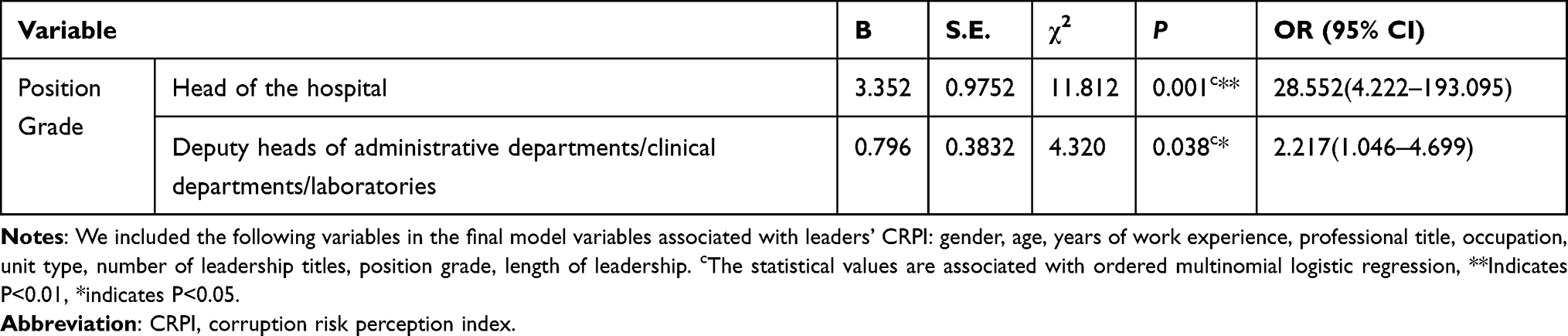 |
Table 5 Final Model of Variables Associated with Leaders’ CRPI (N=1029) |
The Causes of Corruption and Suggestions for the Future
The 5525 participants also evaluated the causes of corruption. A total of 76.34% (4218/5525) suggested that the main cause was fluke ideas, reflected in the employee’s belief that his/her corrupt behavior will not be discovered, or even if discovered, will not be punished. A total of 53.94% (2980/5525) attributed the cause to a poor understanding of management regulations, while 37.85% (2091/5525) thought it was related to inadequate supervision. Regarding the most desired learning content about anti-corruption efforts, 84.71% (4680/5525) proposed “the revelation of corruption cases”, followed by “rules about behavior” and “punishment regulations”, which accounted for 78.55% (4340/5525) and 74.30% (4105/5525), respectively. A total of 317 participants put forward suggestions for future anti-corruption efforts, among which 66.30% (210/317) proposed that “education on corruption risks should be continuously strengthened, including the education of risk points, to improve our anti-corruption ability”, and 33.70% thought attention should be paid to “transparency”, “strengthening supervision and inspection” and “assistance in sorting out risk points”.
Discussion
According to the results of cluster analysis and the ranking of items, the CRPI scores of internal management-related items ranked higher. The ranking of the three items was as follows: personnel recruitment ranked highest, collective decision-making ranked second, and decision-making execution ranked fourth. For external cooperation, the order of the three items was as follows: social donations for academic conferences ranked sixth, social donations for academic exchanges ranked eighth, and academic cooperation ranked ninth. This prompted us to conclude that compared with treatment regulations and professional conduct, internal management and external cooperation have a greater risk of corruption. The results are inconsistent with findings on corruption, such as “red envelopes” and “kickbacks”, which patients think are risky. This shows that hospital staff’s attention to the risk of corruption is different from that of patients, and the outcome is similar to that of Maxwell.19 Employees pay more attention to the influence on the cultivation of their abilities and job security. This indicates that hospital staff may be both implementers and victims of corruption, and corruption will also infringe on the interests of hospital staff.20 The result of corruption risk assessment reflects a series of institutional loopholes in the hospital management system or process that may be beneficial or conducive to corruption,16 and which can help the hospital to improve its management. Therefore, based on our findings, from the perspective of democratic management, WCH needs to pay attention to the construction and dynamic improvement of management regulations (especially those for internal management and external cooperation) to ensure that they have effective policies and procedures. In addition, the transparency of decision-making and implementation should be increased to reduce and control the source of corruption risk from inside the hospital.7
The results of the leadership and corruption risk assessment imply that leaders’ awareness of corruption risk is higher than that of ordinary employees. Among all leaders at WCH, the leaders with higher positions had higher CRPI scores than those with lower positions. Leaders who held multiple positions at the same time had higher CRPI scores than those who held a single position. Leaders who had been in their positions for longer had higher CRPI scores than those who held shorter positions. The four characteristics were all related to the use and supervision of discretion. The occurrence of corruption in the health sector is highly professional with job responsibilities and related to discretion.21,22 Compared with ordinary employees, leaders have greater public power. For example, pharmaceutical department heads had autonomous power in making decisions on medicine procurement and were able to influence the prescription of particular medicines in their hospitals.23 In addition, the higher the position, the more positions and the longer the tenure, the greater the discretion that leaders can control, and the greater the corresponding risk of corruption, which were similar to the findings of Nguyen.23 Therefore, it is necessary to restrict the exercise of the discretion of leaders at all levels in hospitals. We argue that we can strengthen this constraint from four angles. First, it is necessary to clarify the responsibilities and scope of each leader and to establish a list. Second, job responsibilities should be announced and staff should accept supervision. Third, there should be a separation of duties.19 In the decision-making and implementation process of major issues, according to the attributes and needs of events, key nodes should be divided according to workflow to ensure that different nodes are under the responsibility of different responsible personnel; each post forms mutual restrictions. Fourth, the rotation of key staff can be adopted to prevent excessive concentration of power.19 In addition, imperfect supervision mechanisms are considered important reasons for corruption.6,24–26 Zhang mentioned two reasons for the failure of supervision: the lack of incentives for supervision itself; and the fact that regulators themselves are in the chain of supervision failure.27 Because there is a multilevel leadership system in public hospitals, it is necessary to ensure the supervision of leaders at each level. Our results show that the CRPI varied significantly among those with different levels of leadership positions at WCH. The CRPI of core leaders was statistically higher than that of ordinary leaders (P<0.05), suggesting that the effect of the supervisory chain is not ideal. Hence, we think that in the internal supervision of the hospital leadership system, leaders should be both supervised and also supervisors. When discussing the anti-corruption responsibility system, the supervision function should be one of their duties. Guo Yong asserted that supervision influences the effectiveness of the anti-corruption system to a large extent.28 The “grid” supervision method can be adopted. In a vertical chain, superior leaders should supervise the subordinate leaders they manage and pass on the supervision pressure. Horizontally, adequate employee supervision should be adopted.16
Most employees think that the main personal cause of corruption is fluke ideas, which belong to the rationalization of corruption at the individual level. Vian T suggested that rationalization is one of the driving factors of corruption in the health care field.6 Fluke ideas manifest in the self-belief that corruption will not be discovered,29 and are largely due to the estimation of corruption costs by individuals in hospitals.30 To reduce fluke ideas, employees need to be aware of the increased cost of corruption. Thus, anti-corruption and integrity education should be continuously strengthened. In 2020, an editorial published in Lancet raised three questions about the governance of corruption in the health sector: (1) What is driving a particular form of corruption? (2) Who holds the power? (3) Who can make a difference?31 The risk of corruption should be recognized and managed based on power. As such, WCH needs to carry out education from the perspectives of power awareness and corruption costs. First, all employees should know that they have discretion and realize that they may face the choice of whether to engage in corrupt behavior. Employees should be vigilant in consciousness. Second, combined with the construction and improvement of hospital management regulations, employees should know these strict regulations and be aware of the increased cost of corruption and the inevitability and consequences of being discovered. Therefore, employees might choose not to be corrupt. In terms of educational methods, in addition to formal and informal education,32 it is very important to build a clean, honest culture in hospitals so that staff can be rooted in organizational values such as honesty and good management and promote integrity.19
Conclusion
Medical corruption leads to serious economic losses,33,34 distorts the distribution of health investment via its impact on people’s fair access to health resources,35 and has a huge effect on personal health, especially that of vulnerable groups.36 Medical corruption also undermines the progress of achieving the goal of universal health coverage (UHC) and affects the realization of sustainable development goals (SDGs).37 Hence, the fight against medical corruption has always been an important task for all stakeholders, including all staff members of medical institutions, regardless of whether they are leaders, specialists, or ordinary employees.
Due to the great harm of corruption in public hospitals, the assessment, control, and prevention of corruption have drawn attention.38 Understanding public hospital staff’s perceptions of corruption will help to identify areas where reforms are needed and provide a basis for good governance in that hospital. Our results indicate that among WCH employees, the corruption risks of internal management and external cooperation were greater than those of treatment regulations and professional conduct. People with different social characteristics had different perceptions of corruption. The corruption risk of leaders was higher than that of ordinary employees. The main personal reason for employees’ corruption behavior was fluke ideas. The findings imply the emphasis and direction of hospital management. First, WCH needs to pay attention to the construction and dynamic improvement of the hospital’s internal management regulations and external cooperation management regulations, and increase the transparency of decision-making and implementation. Second, it is necessary to restrict the discretion of leaders at all levels and to strengthen supervision. In addition, WCH needs to carry out education from the perspectives of power awareness and corruption costs, and to strive to build a clean, honest culture. The specific development mode and effectiveness of these measures should be examined in future research.
There are also some limitations of this study. We collected CRPI data in only one hospital and were unable to reveal the perceptions of hospital staff toward corruption on a large scale; the sample size needs to be increased. In the questionnaire, we covered 15 kinds of corruption risks that are mentioned most frequently in the literature, news, and criminal judgements, easily occur in public hospitals, and could be involved in and understood by most employees in hospitals. However, we did not include some corruption risks in which the majority of hospital staff may be seldom involved, such as hospitals’ infrastructure projects and gene detection. Therefore, follow-up studies in specific groups should be considered. In addition, this was a cross-sectional study, so we could not uncover the effectiveness of specific anti-corruption measures.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its supplementary information files. The datasets are available from the corresponding author Li Luo on reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for the study was obtained from the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University on the 21st April of September 2020 (2020/350). Permission was obtained from WCH. The guidelines on research involving the use of human subjects were adhered to according to the Helsinki Declaration strictly. There was no financial inducement, and participants did not incur any cost by participating in this study.
Informed consent was obtained from participants before the commencement of the study. First, we noticed the hospital staff and introduced the background, purpose, and privacy protection in detail. Second, because it was an online survey, we set the informed consent option before formal content. The participants need to answer whether he/she was willing to participate in this research, anyone who did not wish to be involved can choose “no” to leave before the survey started. It was an anonymous survey for protecting the privacy of participants. Participants completed the questionnaire by themselves.
Acknowledgments
The authors would like to thank all managers and employees in West China Hospital of Sichuan University who took part in data collection. We would also like to thank Sichuan Science and Technology Department, China for funding.
Funding
This study was supported by a grant from Sichuan Science and Technology Department, China (21RKX0514).
Disclosure
Ms Fang Zhu and Ms Juan Xie report grants from Sichuan Science and Technology Department, during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. International T. What is corruption? 2018. Available from: https://www.transparency.org/what-is-corruption.
2. Wederman A. The intensification of corruption in China. China Q. 2005;180:895–921. doi:10.1017/S0305741004000670
3. Gadit AAM. Opinion and debate-corruption in medical practice: how far have we gone? J Pak Med Assoc. 2011;61(1):93. PMID: 22368915.
4. Han X, Feng M, Wang F. Ethical governance of medical corruption: taking the university affiliated hospital as an example. Med Philos. 2019;40(18):32–36. Chinese. doi:10.12014/j.issn.1002-0772.2019.18.07
5. Mackey TK, Vian T, Kohler J. The sustainable development goals as a framework to combat health-sector corruption. Bull World Health Organ. 2018;96(9):634–643. doi:10.2471/BLT.18.209502
6. Vian T. Review of corruption in the health sector: theory, methods and interventions. Health Policy Plan. 2008;23(2):83–94. doi:10.1093/heapol/czm048
7. Vian T. Anti-corruption, transparency and accountability in health: concepts, frameworks, and approaches. Glob Health Action. 2020;13(sup1):1694744. doi:10.1080/16549716.2019.1694744
8. Hussmann K. Demystify false dilemmas to speak about corruption in health systems: different actors, different perspectives, different strategies: comment on” We need to talk about corruption in health systems”. Int J Health Policy Manag. 2019;8(10):620. doi:10.15171/ijhpm.2019.61
9. Sekalala S, Masud H, Bosco RT. Human rights mechanisms for anti-corruption, transparency and accountability: enabling the right to health. Glob Health Action. 2020;13(sup1):1699343. doi:10.1080/16549716.2019.1699343
10. Guo Y, Song W. Measuring corruption: a new framework including corruption situation, anti-corruption performance and corruption risk. J Public Adm. 2016;9(3):
11. Põlajeva T. Governance power impact on corruption and the business environment-determining factors.
12. Arosteguí J, Hernandez C, Suazo H, et al. Auditing Nicaragua’s anti-corruption struggle, 1998 to 2009. BMC Health Serv Res. 2011;11(2):1–10. doi:10.1186/1472-6963-11-S2-S3
13. Hunter M, Mardini RU, El-Seblani A, et al. Anti-corruption, transparency and accountability: case study of healthcare in the Arab countries. Glob Health Action. 2020;13(sup1):1704529. doi:10.1080/16549716.2019.1704529
14. World Health Organization. Reinforcing the focus on anti-corruption, transparency and accountability in national health policies, strategies and plans; 2019. Available from: https://apps.who.int/iris/handle/10665/326229.
15. Huss R. Our blind spots in the fight against health systems corruption comment on “we need to talk about corruption in health systems. Int J Health Policy Manag. 2020;9(1):34–38. doi:10.15171/ijhpm.2019.81
16. Hope KR. Contextualizing corruption in the health sector in developing countries: reflections on policy to manage the risks. World Med Health Policy. 2015;7(4):383–401. doi:10.1002/wmh3.165
17. Krishnamurti C, Shams S, Velayutham E. Corporate social responsibility and corruption risk: a global perspective. J Contemp Account Econ. 2018;14(1):1–21. doi:10.1016/j.jcae.2018.02.002
18. Khahro SH, Ali TH, Hassan S, et al. Risk severity matrix for sustainable public-private partnership projects in developing countries. Sustainability. 2021;13(6):3292. doi:10.3390/su13063292
19. Maxwell D, Bailey S, Harvey P, et al. Preventing corruption in humanitarian assistance: perceptions, gaps and challenges. Disasters. 2012;36(1):140–160. doi:10.1111/j.1467-7717.2011.01245.x
20. Rispel LC, de Jager P, Fonn S. Exploring corruption in the South African health sector. Health Policy Plan. 2016;31(2):239–249. doi:10.1093/heapol/czv047
21. Ou X. Research on Prevention and Control Management System of Public Hospitals Under the Background of New Medical Reform. Chengdu: Public administration, Southwest Jiaotong University; 2018.
22. Sun Y, Zhao D, Zhang Z. Study of the corruption risk control mechanism at public hospitals. Chin J Hosp Admin. 2018;34(7):609–611. Chinese. doi:10.3760/cma.j.issn.1000-6672.2018.07.021
23. Nguyen TA, Knight R, Mant A, et al. Corruption practices in drug prescribing in Vietnam - an analysis based on qualitative interviews. BMC Health Serv Res. 2018;18(1):587. doi:10.1186/s12913-018-3384-3
24. Naher N, Hoque R, Hassan MS, et al. The influence of corruption and governance in the delivery of frontline health care services in the public sector: a scoping review of current and future prospects in low and middle-income countries of south and South-East Asia. BMC Public Health. 2020;20(1):880. doi:10.1186/s12889-020-08975-0
25. Ahmed SM, Evans TG, Standing H, et al. Harnessing pluralism for better health in Bangladesh. Lancet. 2013;382(9906):1746–1755. doi:10.1016/S0140-6736(13)62147-9
26. Tam W. Organizational corruption by public hospitals in China. Crime Law Soc Change. 2011;56(3):265–282. doi:10.1007/s10611-011-9290-9
27. Zhang T. Research on control of medical kickbacks based on the fraud triangel theory. Med Philos. 2019; (18):37–40. Chinese. doi:10.12014/j.issn.1002-0772.2019.18.08
28. Guo Y. Corruption situation in China after the 18th CPC National Congress: evaluation from three dimensions. J Polit Sci. 2017;134(3):
29. Yang Y. The Research About Corrupt Psychological-Based on the Analysis of the Behaviors of the Behaviors of the 100 Corrupt Officials. Wuhan: College of Management, Central China Normal University; 2013.
30. Dong H. Research on the Construction of Clean Government CultureIn Tertiary Hospitals Based on the Psychological Causes ofCorruption. Nanjing: Nanjing Medical University; 2020.
31. The Lancet Global Health. 2020–30: the decade of anti-corruption? Lancet Glob Health. 2020;8(1):e1. doi:10.1016/s2214-109x(19)30500-5
32. Horodnic AV, Mazilu S, Oprea L. Drivers behind widespread informal payments in the Romanian public health care system: from tolerance to corruption to socio-economic and spatial patterns. Int J Health Plann Manage. 2018;33(2):e597–e611. doi:10.1002/hpm.2509
33. Gaspar V, Hagan S. Corruption: costs and mitigating strategies. Staff Discussion Notes. 2016;2016(005). doi:10.5089/9781513594330.006
34. Jones B, Jing A. Prevention not cure in tackling health-care fraud. Bull World Health Organ. 2011;89(12):858–859. doi:10.2471/BLT.11.021211
35. Hanf M, Van-melle A, Fraisse F, et al. Corruption kills: estimating the global impact of corruption on children deaths. PLoS One. 2011;6(11):e26990. doi:10.5089/9781513594330.00610.1371/journal.pone.0026990
36. Witvliet MI, Kunst AE, Arah OA, et al. Sick regimes and sick people: a multilevel investigation of the population health consequences of perceived national corruption. Trop Med Int Health. 2013;18(10):1240–1247. doi:10.1111/tmi.12177
37. Koller T, Clarke D, Vian T. Promoting anti-corruption, transparency and accountability to achieve universal health coverage. Glob Health Action. 2020;13(sup1):1700660. doi:10.1080/16549716.2019.1700660
38. Hutchinson E, Balabanova D, McKee M. We need to talk about corruption in health systems. Int J Health Policy Manag. 2019;8(4):191–194. doi:10.15171/ijhpm.2018.123
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.