")
Back to Journals » Patient Preference and Adherence » Volume 8
How do health services researchers understand the concept of patient-centeredness? Results from an expert survey
Authors Scholl I, Zill JM, Härter M , Dirmaier J
Received 14 March 2014
Accepted for publication 4 June 2014
Published 30 August 2014 Volume 2014:8 Pages 1153—1160
DOI https://doi.org/10.2147/PPA.S64051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Isabelle Scholl, Jördis M Zill, Martin Härter, Jörg Dirmaier
Department of Medical Psychology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Background: The concept of patient-centeredness has gained in importance over recent decades, including its growing importance on a health policy level. However, many different definitions and frameworks exist. This renders both research and implementation into clinical practice difficult. This study aimed at assessing how German researchers conceptualize patient-centeredness, how they translate the German equivalent into English, and what they consider the most important references on the topic.
Methods: All researchers within a German research priority program on patient-centeredness were invited to participate in an online survey with open questions. The data regarding the definitions of patient-centeredness were analyzed using the method of conventional content analysis. Descriptive statistics were used to analyze the responses on translations and references.
Results: Thirty-eight (28%) of 136 invited researchers participated in the study. The definitions given by the participants could be classified into ten categories: patient as a unique person, involvement in decision-making, patient information, essential characteristics of the physician, biopsychosocial perspective, patient empowerment, individualized services, patient-reported outcomes, involvement in health policy and coordination and teamwork. The results for the translation of the German word “Patientenorientierung” into English indicate that uncertainty regarding the appropriate English terminology exists. All participants provided a different reference on patient-centeredness that was important to them.
Conclusion: The results show a certain degree of “shared meaning” regarding the concept of patient-centeredness. However, they also indicate a considerable amount of “surplus meaning”, which can be seen as an indicator for the fuzziness of a theoretical concept. All in all, this study has shown that the conceptual ambiguity found in the literature on patient-centeredness is partly reflected in the conceptualizations of German researchers working in that field. This calls for more conceptual work, eg, developing an integrative model on patient-centeredness grounded in the international literature.
Keywords: patient-centered care, concept analysis, expert survey
Background
In the last decade, patient-centeredness has gained in importance,1,2 including policies to promote patient-centered care at the level of legislation and regulation of health care.3 In the USA, the Institute of Medicine postulated patient-centeredness to be one of six aims for improvement in the US health care system.4,5 The importance of patient-centered care has also been stressed by the 2010 Patient Protection and Affordable Care Act.6 This led to the formation of the Patient-Centered Outcomes Research Institute, which has funding opportunities for research on patient-centeredness (http://www.pcori.org). In the UK, patient-centered care has been pushed forward by the Public and Patient Experience and Engagement Division set up by the Department of Health.7 In Germany, the Federal Ministry of Education and Research, together with the German statutory pension insurance scheme, the associations for statutory health insurance schemes, and the association for private health insurance funds, launched a large research priority program on patient-centeredness and chronic diseases. This ongoing research program started in 2007 and has a total funding volume of over 20 million euro for 77 research projects. The program focuses on three main topics in relation to patient-centeredness: research on patient information, efficient training programs for chronically ill patients, and patient-centered design of care.
In light of this vast amount of ongoing research on patient-centeredness and its prominent position on the political agenda, it might seem intuitively logical that the theoretical conceptualization of what constitutes patient-centeredness is clear. However, when looking closely at existing conceptual work, one can see that several models exist and describe various dimensions of patient-centeredness. For example, while Stewart et al8,9 describe six elements of the patient-centered method (eg, understanding the whole person, finding common ground), Mead and Bower10,11 include five key dimensions of patient-centeredness in their model (eg, the biopsychosocial perspective, the therapeutic alliance). At the same time, Epstein et al12 postulate four domains of patient-centered communication (eg, helping patients to share power and responsibility by involving them in choices to the degree that they wish), and Ouwens et al13 include eight domains of patient-centered care (eg, access to care, emotional and psychosocial support). However, these models are broad, and the existing literature reveals a lack of theoretical and conceptual clarity regarding the term “patient-centeredness”.14 This results in a heterogeneous use of the term,15 with unclear measurement dimensions and measurement instruments.16–18 Hence, research results regarding the effectiveness of interventions to promote patient-centeredness, found by such various measurement scales, are inconsistent.19,20 This can be seen as a barrier to the implementation of patient-centered care into routine practice,21 which is so much called for on the policy level.
It remains unclear whether this theoretical and conceptual ambiguity is also found within the German context. If so, this would limit the impact of German research on the concept, as it would render comparison of results very difficult, both within the research program and internationally. Furthermore, it is not known if current research projects on patient-centeredness in Germany root their work in prominent models described in the international literature.8–13,22 This is particularly unclear, as the German language has two different terms for patient-centeredness, ie, “Patientenorientierung” (literal translation “patient orientation”) and “Patientenzentrierung” (which is closer to the English term). While German publications from the 70s and 80s often refer to “Patientenzentrierung”,23,24 the more recent literature mainly uses the term “Patientenorientierung”.25
Thus, the aim of this study was to assess how scientific experts in Germany define patient-centeredness, which dimensions they include in the concept, and how they would operationalize these dimensions. Furthermore, we wanted to know which English term they would use to translate the German term “Patientenorientierung” and which literature on patient-centeredness they consider most important.
Materials and methods
Participants
We invited all staff members (n=136) of projects funded within the German research priority program on patient-centeredness and chronic diseases by email to participate in the study. This included all principal investigators, project coordinators, research associates, and post-graduate research assistants involved in these projects. We chose this sample because they are conducting studies explicitly labeled as research on patient-centeredness (purposive sampling).
Data collection
Informal discussions among colleagues in the research program had revealed reluctance to discuss such a “vague topic” in personal interviews. Therefore, we chose an online survey as a method of data collection to assure anonymity and confidentiality to the participants. We conducted the online survey data collection using EFS Survey 8.1 software from November to December 2011. During this period of time, we sent two reminders by email to all invited participants (2 and 4 weeks after the start of data collection). The survey consisted of several open-ended questions on patient-centeredness (see Table 1) as well as questions regarding demographic characteristics of the participants.
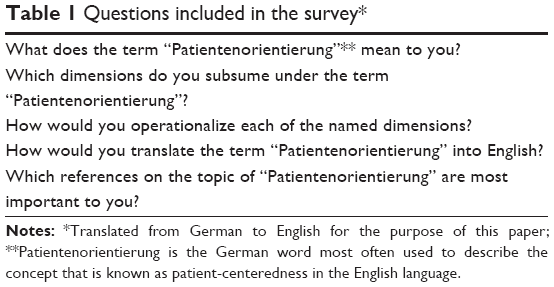 | Table 1 Questions included in the survey* |
Data analysis
We (IS, JZ, JD) analyzed the data yielded from survey questions 1 to 3 using the method of conventional content analysis,26 also described under the term of inductive category development.27 This method is considered appropriate when existing theory or research literature on a phenomenon is limited or fuzzy.26 As outlined above, this is the case for patient-centeredness. In a first step, one member of the research team (JZ) read the text and divided it into units. This team member (JZ) developed inductive categories from the material, leading to a first draft of the coding sheet. In a next step, we (IS, JZ, JD) discussed the coding sheet, leading to a revision. Next, two authors (IS, JD) used this revised coding sheet to code the data again independently. In a last step, discrepancies in coding were resolved by reviewing together the units in question (IS, JZ, JD). The few units that were mentioned only once were coded as “other”. Analysis was stopped when consensus was reached. We analyzed survey questions 4 and 5 as well as demographic data using simple descriptive statistics. Furthermore, the answers given to question 5 were classified into three categories: references focusing exactly on patient-centeredness (eg, term was included in title and abstract), work concentrating on a single aspect of patient-centeredness, and literature on a broader topic. Statistical analyzes were performed using PASW Statistics version 18 (SPSS Inc, Chicago, IL, USA).
Results
Sample characteristics
Thirty-eight of the 136 invited experts filled in the survey, leading to a response rate of 28%. The characteristics of the participants are displayed in Table 2. Half of them (53%) were female. On average they were 43 years old. Most had a background in psychology (66%), and the others had a background in either sociology (18%) or medicine (16%).
 | Table 2 Characteristics of participants |
Meaning of patient-centeredness
The coding process on the meaning of patient-centeredness (see question 1 in Table 1) resulted in ten categories. The categories were classified into two broad groups that surfaced in the data: those referring to the micro level of care (ie, categories that describe patient-centeredness inside and around the patient-clinician encounter), and those referring to the meso or macro level of care (ie, categories that describe patient-centeredness on institutional, health policy, or health care system levels). The ten categories are displayed in Figure 1. On average, each expert’s answer could be classified into three categories (range 1–6).
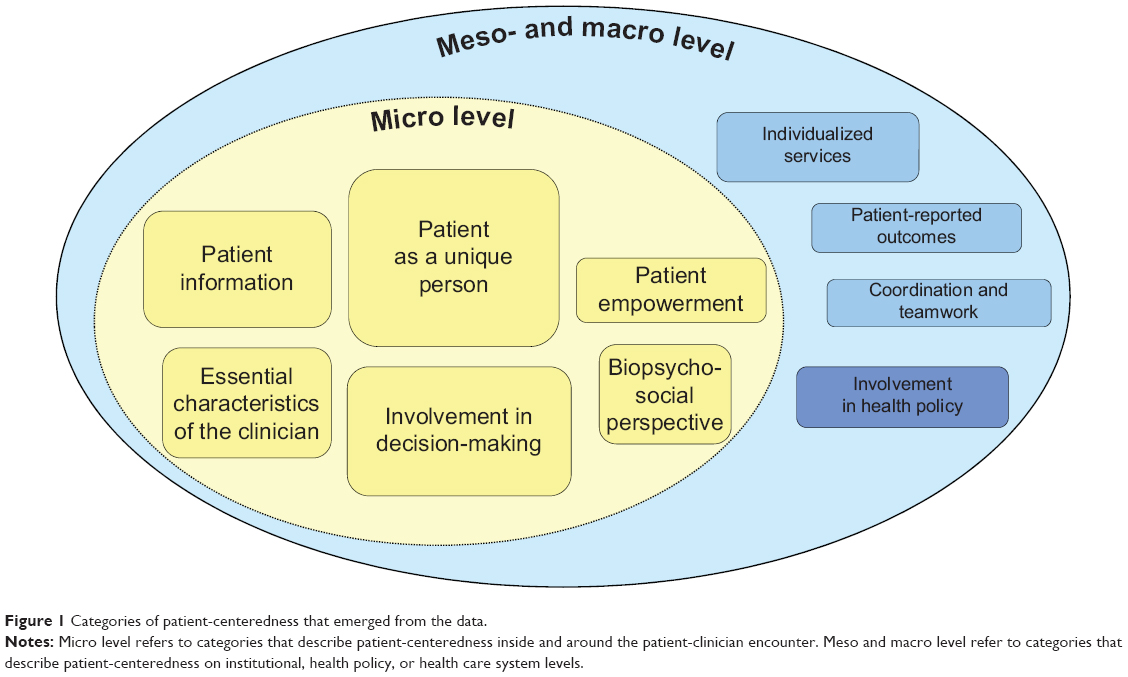 | Figure 1 Categories of patient-centeredness that emerged from the data. |
Patient-centeredness on the micro level of care
The elements that were named most often by health services researchers can be classified into the category of patient as a unique person (n=26). This means that the patient-centered clinician should elicit and respond to the goals, values, needs, wishes, and fears of each individual patient. Furthermore, the clinician should ask the patient about his or her perspectives on the illness and his or her expectations and subsequently use this information for the treatment or management of the disease.
The clinician actively assesses the wishes, perspectives and concerns of the patient and uses them as a basis for the following consequences (eg, treatment, prescription). (Participant 2)
The second most often described category was involvement in decision-making (n=20). In patient-centered care, the patient should be involved in decisions about his or her medical treatment to the degree that he or she wishes. This ranges from a paternalistic approach to decision-making to informed decision-making, with shared decision-making being the middle ground, depending on the patient’s preference for involvement.
Involvement of the patient in all medical steps of his or her treatment that is tailored to his or her wish for involvement. (Participant 29)
The third most named aspects of patient-centeredness were categorized as patient information (n=15). In a patient-centered approach, the clinician should inform the patient in a way that is tailored to the patient’s needs and cognitive capacities. Information must be given in a transparent and understandable way.
Tailoring the information regarding quantity and language to the needs and abilities of the patient. (Participant 16)
The next facets described by the participants (n=12) can be classified as essential characteristics of the clinician. This category includes the clinician’s readiness to see the patient as an equal partner, to show empathy and emotional support, and to be able to reflect on himself/herself as a clinician.
Acknowledging that the patient is an equal dialogue partner [in the medical consultation] and taking him or her seriously. (Participant 20)
Furthermore, several experts (n=9) named facets of patient-centeredness that can be integrated into the category called biopsychosocial perspective. This relates to understanding the patient and his or her illness within a broader context (eg, family, social network, employment, life history, and cultural background) and seeing the patient as a whole person.
[It] requires a comprehensive assessment of the patient’s personal and surrounding environment. (Participant 24)
As a last category on the level of the micro system, several participants (n=8) described elements of the category known as patient empowerment. The clinician should encourage the patient’s self-management capacities and support the patient’s autonomy. This should include patient training and education programs.
Encouraging [the patient] to take responsibility and engage in self-management. (Participant 6)
Patient-centeredness on the meso and macro levels of care
The last four categories that emerged from the data refer to the meso or macro level of care. They were mentioned both less frequently and in less detail. The first of them is individualized services (n=8). This involves medical services that are tailored to different patient groups as well as offering a broad variety of support services.
Offering target-group-specific services (eg, for elderly patients, patients with a migrant background, lower-income groups). (Participant 29)
Furthermore, a few participants (n=6) indicated the importance of patient-reported outcomes to be part of patient-centered care. This includes the assessment of the patient’s quality of life and satisfaction with care and using this information to improve care. Another aspect of this category is that patient-reported outcomes should play a central role in research.
Using studies that illuminate the patients’ perspectives (eg, what is important for patients in their therapy?) and not only [using] efficacy studies that proceed objectively (external observation). (Participant 2)
A small number of participants (n=5) briefly mentioned aspects that can be categorized into involvement in health policy. This category describes the participation of patients and community members in health policy decisions, plans, and actions that are undertaken to make the health care system more patient-centered.
Participation of patients/community and their representatives in processes that can influence medical care (eg, financing, range of services, guidelines) on the level of service and care providers […] and [on the level of] legislation. (Participant 29)
Finally, a range of aspects that fall into the category of coordination and teamwork were identified a few times (n=4). This category includes the culture within a medical facility and the interaction between team members (eg, communication and coordination processes).
The conditions within a medical facility (structures, interaction and culture within the teams and within the clinic) [facilitate] the implementation of patient-centered care (eg, information, communication and coordination processes with the team, the clinic or the practice). (Participant 21)
Dimensions of patient-centeredness and their operationalizations
When participants were asked to name directly the dimensions of patient-centeredness (see question 2 in Table 1), they described approximately the same dimensions that were found in the categories regarding the micro system of care described above (see section on Patient-centeredness on the micro level of care). However, the frequency of mentions was slightly different, with most participants (n=18) naming involvement in decision-making. In general, there was a larger heterogeneity of given answers with several dimensions that were mentioned only by one participant. The question on how to operationalize each of the named dimensions (see question 3 in Table 1) yielded a very large amount of heterogeneous suggestions. However, although asked to map each operationalization on its respective dimension, many of the operationalizations given could not be clearly classified into a certain dimension, ie, were vague and ambiguous. For example, one participant gave the following explanation for operationalization of involvement in decision-making:
Several operationalizations are possible! (Participant 9).
Translation into English
The translations of the German term “Patientenorientierung” into English are displayed in Table 3. One third of the participants translated it as patient-centeredness, which would be considered the most appropriate translation, as it is the term most recognized in the international literature. Another third used the more literal, but internationally less frequently used term, patient orientation. Twenty-one percent of the translations were different altogether (eg, shared decision-making, empowerment) and 14% did not give a translation at all.
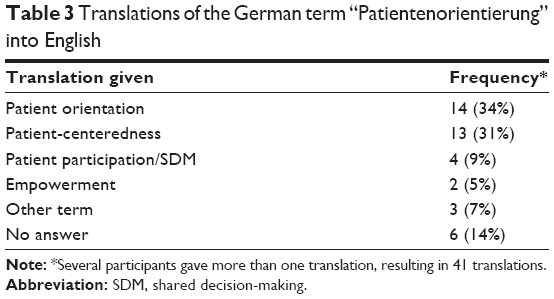 | Table 3 Translations of the German term “Patientenorientierung” into English |
Main references
Twenty-seven of the 38 participants (71%) gave a reference of work that they considered most important for the concept of patient-centeredness. Each of the 27 reported citations was only given by one participant. Fifteen (55%) of those references were in English, while the other 12 (45%) were in German. The analysis of those citations revealed that ten of the 27 references (37%) were focusing exactly on patient-centered care. Those references, both in German and English, are often cited in the literature on patient-centeredness, eg, the work of Stewart et al,8 Mead and Bower,10,11 and Gerteis et al.22 There was a second category of references given, eight in total (30%), which rather focused on one single, specific aspect of patient-centeredness. This includes several papers on shared decision-making (eg, Scheibler28) and on patient empowerment (eg, Aujoulat et al29). Furthermore, a third category of citations named by nine participants (33%) has a much broader topic, eg, on general and family medicine30 or on communication in general.31
Discussion
This study aimed to assess how researchers working in the field of patient-centeredness in Germany conceptualize patient-centeredness. The definitions given could be classified into ten categories. The ten dimensions identified in this study seem to be interrelated rather than completely independent, which has also been described in the literature.1,10 For example offering individualized services (mapped onto the meso and macro level of care) is certainly related to taking into account each person’s uniqueness (mapped onto the micro level of care). In summary, the results show a certain degree of “shared meaning” regarding the concept of patient-centeredness, especially regarding the micro level of care. However, they also indicate a considerable amount of “surplus meaning”, which can be seen as an indicator for the fuzziness of a theoretical concept.32 This is especially the case for the operationalization of the concept’s dimensions, where there is almost no consensus between experts to a point where it was hard to interpret the data. When comparing the ten categories that emerged from the data with the models of patient-centeredness described in the literature, it can be seen that the six categories found to describe patient-centeredness on the micro level of care are similar to the five conceptual dimensions identified in the prominent model of Mead and Bower.10 Their model is also a model that focuses on the patient-physician interaction, ie, the micro level of care. Another highly cited model that concentrates on the individual clinician is the one developed by Stewart et al8 which describes the “patient-centered clinical method”. The heterogeneity regarding the other categories that emerged from the data (especially regarding the meso and macro levels of care) reflects the international literature on patient-centeredness. While much conceptual work describes patient-centered care on the micro level, many prominent models (eg, Stewart et al8 and Mead and Bower10) do not address the broader health care system. This could explain why aspects of patient-centeredness relating to the broader health care system (rather than the micro level of care) were less frequently found in the results. Only few prominent models do have a broader focus, like the framework developed by the Picker Institute on the basis of the work of Gerteis et al.22 The heterogeneity of the answers given by the participants can also be explained by the references they listed as important to them. Each of the 27 citations provided in the survey was a different one. Thus, their divergent answers reflect the fuzziness found in the literature. However, the references given by the experts also suggest that sometimes only a certain dimension of patient-centeredness is taken into consideration (eg, shared decision-making). A possible explanation could be that researchers focus more on specific aspects of patient-centered care than looking at the broader meaning of patient-centeredness. Furthermore, the fact that about one third of the respondents did not cite a reference at all might be an indicator that they felt unsure which reference is best.
The results for the translation of the German word “Patientenorientierung” into English indicate that there is some confusion or uncertainty regarding the appropriate English terminology. This finding is important as it has serious consequences: it makes it both more difficult for German researchers to find international literature on patient-centeredness (ie, by only using the term “patient orientation” and not “patient-centeredness” in the database search) and to internationally disseminate their own results on patient-centeredness. It is possible that similar translation difficulties occur in other languages. This can also entail that work by English native speakers is not picked up in different parts of the world, as a consequence of wrong search terms and terminology. This should be assessed in future research.
A strength of this study is that, to our knowledge, it is the first study in Germany examining this specific question. It is therefore an important step toward more conceptual and theoretical work on patient-centeredness, which has been called for by many, eg, Epstein et al.12
The main limitation of this study is related to the data collection method. Written online surveys might not be the most appropriate method to assess detailed expert information on a complex topic such as patient-centeredness. Personal interviews might have given more detailed information and would have made it easier to clarify unclear answers of participants. Regarding the dimensions and operationalizations of these dimensions, it would have been helpful to be able to ask clarifying questions, especially as responses were often quite short. However, while planning this study, some researchers had expressed their reluctance regarding personal interviews due to fear of not knowing enough about this complex topic. Thus, by choosing anonymous online surveys, we aimed at increasing the response rate. Nevertheless, there was a considerable amount of invited experts who did not participate in the study, limiting the generalizability of the results. Generalizability might also be limited by the fact that few participants had a background in medicine. Anecdotal evidence through personal communication (with IS) suggests that these researchers might have felt they knew too little to answer the questions or that they found them difficult to answer. Furthermore, although we did cross-check the questions with two senior researchers who are experts in the field, we did not do a larger-scale pilot testing of the questions to assess the clarity within the questions (especially regarding the term “operationalization”). A future study should certainly put more emphasis on this issue, in order to obtain more interpretable data. Furthermore, future research should focus on disentangling attitudes and behavioral aspects of patient-centeredness.
Conclusion
All in all, this study has shown that the theoretical and conceptual fuzziness found in the international literature on patient-centeredness is partly reflected in the conceptualizations of German researchers working in this field. This shows the necessity for developing an integrative model on patient-centeredness that systematically takes into account the broad variety of definitions and models found in the international literature. We are planning to realize this in a next step,33 in which we also plan to involve international experts (researchers, clinicians, and patient representatives) in an online Delphi survey. Such an integrative model can be used to identify gaps in the measurement of patient-centeredness. The development of such a model, together with ongoing research by other groups, is necessary for moving the field of measurement forward, which could lead eventually to a greater international comparability of research results. This again is a prerequisite for a large scale implementation of patient-centeredness into health care.
Acknowledgments
We would like to thank all the participants in this study for their valuable input. Furthermore, we want to thank Stephanie Pahlke, Marta Plonka, and Evamaria Müller for their work as student assistants in the project, and Eva Christalle, Musa Cömert, and Wiebke Frerichs for copyediting the manuscript. This work was supported by the Federal Ministry for Education and Research in Germany (grant number 01GX1043).
Author contributions
IS participated in the design of the study, collected the data, led the data analysis, and drafted the manuscript. JZ carried out the data analysis and helped to draft the manuscript. MH participated in the design of the study, participated in reviewing the codes, and revised the manuscript critically for important intellectual content. JD conceived of the study, participated in its design and analysis, and helped to draft the manuscript. All authors read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Epstein RM, Street RLJ. Patient-Centered Communication in Cancer Care: Promoting Healing and Reducing Suffering. NIH Publication No. 07-6225. Bethesda, MD, USA: National Cancer Institute; 2007. | ||
Lewin S, Skea Z, Entwistle VA, Zwarenstein M, Dick J. Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane Database Syst Rev. 2001;4:CD003267. | ||
Härter M, van der Weijden T, Elwyn G. [Policy and practice developments in the implementation of shared decision making: an international perspective]. Z Evid Fortbild Qual Gesundhwes. 2011;105(4):229–233. German. | ||
Berwick DM. A user’s manual for the IOM’s ‘quality chasm’ report. Health Aff (Millwood). 2002;21(3):80–90. | ||
Committee on Quality of Health Care in America; Institute of Medicine. Crossing on Quality Chasm: A New Health System for the 21st Century. Washington, DC, USA: National Academy Press; 2001. | ||
Senate and House of Representatives. Patient Protection and Affordable Care Act. 2010. Available from: http://www.gpo.gov/fdsys/pkg/BILLS-111hr3590enr/pdf/BILLS-111hr3590enr.pdf. Accessed February 8, 2013. | ||
Department of Health. Putting people at the heart of care. 2009. Available from: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_111225.pdf. Accessed February 8, 2013. | ||
Stewart MA, Brown JB, Weston W, McWhinney IR, McWilliam CL, Freeman TR. Patient-Centered Medicine – Transforming the Clinical Method. 2nd ed. Abingdon, UK: Radcliffe Medical Press; 2003. | ||
Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152(9):1423–1433. | ||
Mead N, Bower P. Patient-centredness: a conceptual framework and review of the empirical literature. Soc Sci Med. 2000;51(7):1087–1110. | ||
Mead N, Bower P. Patient-centred consultations and outcomes in primary care: a review of the literature. Patient Educ Couns. 2002;48(1): 51–61. | ||
Epstein RM, Franks P, Fiscella K, et al. Measuring patient-centered communication in patient-physician consultations: theoretical and practical issues. Soc Sci Med. 2005;61(7):1516–1528. | ||
Ouwens M, Hermens R, Hulscher M, et al. Development of indicators for patient-centred cancer care. Support Care Cancer. 2010;18(1): 121–130. | ||
de Haes H. Dilemmas in patient centeredness and shared decision making: a case for vulnerability. Patient Educ Couns. 2006;62(3):291–298. | ||
van Dulmen S. Patient-centredness. Patient Educ Couns. 2003;51(3): 195–196. | ||
Epstein RM, Street RLJ. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100–103. | ||
Mead N, Bower P. Measuring patient-centredness: a comparison of three observation-based instruments. Patient Educ Couns. 2000;39(1): 71–80. | ||
McCormack LA, Treiman K, Rupert D, et al. Measuring patient-centered communication in cancer care: a literature review and the development of a systematic approach. Soc Sci Med. 2011;72(7):1085–1095. | ||
Michie S, Miles J, Weinman J. Patient-centredness in chronic illness: what is it and does it matter? Patient Educ Couns. 2003;51(3):197–206. | ||
Smith RC, Dwamena FC, Madhusudan G, Coffey J, Frankel RM. Behaviorally defined patient-centered communication – a narrative review. J Gen Intern Med. 2010;26(2):185–191. | ||
Lawrence M, Kinn S. Defining and measuring patient-centred care: an example from a mixed-methods systematic review of the stroke literature. Health Expect. 2012;15(3):295–326. | ||
Gerteis M, Edgman-Levitan S, Daley J, Delbanco TL. Through the Patient’s Eyes. Understanding and Promoting Patient-Centered Care. San Francisco, CA, USA: Jossey-Bass; 1993. | ||
Engelhardt K. [“Patient-centred” medicine]. Munch Med Wochenschr. 1971;113(21):803–809. German. | ||
Hannich H-J, Wendt M. [Patient-centered treatment of surgery patients]. Zeitschrift für Personenzentrierte Psychologie und Psychotherapie. 1983;2(3):311–320. German. | ||
Hoefert H-W, Härter M. [Patient-Centeredness in Hospital]. Göttingen, Germany: Hogrefe; 2010. German. | ||
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. | ||
Mayring P. Qualitative content analysis. Forum: Qualitative Social Research. 2000. Available from: http://www.qualitative-research.net/index.php/fqs/article/view/1089/2386. Accessed February 8, 2013. | ||
Scheibler F. [Shared Decision-Making: From compliance to partner-like decision-making]. Bern, Switzerland: Huber; 2003. | ||
Aujoulat I, d’Hoore W, Deccache A. Patient empowerment in theory and practice: polysemy or cacophony? Patient Educ Couns. 2007;66(1): 13–20. | ||
Kochen M. [Family and general medicine]. Stuttgart, Germany: Thieme; 2006. | ||
Schulz von Thun F. [Talking with each other 1 – Troubles and clarifying. General psychology of communication]. Hamburg, Germany: Rowohlt; 1981. | ||
Jaccard J, Jacoby J. Theory Construction and Model-Building Skills: A Practical Guide for Social Scientists. New York, NY, USA: The Guilford Press; 2010. | ||
Zill JM, Scholl I, Härter M, Dirmaier J. Conceptualization and measurement of patient-centeredness: a study protocol. Patient Prefer Adherence. 2013;7:345–351. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.