")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
How Can We Use the Promoting Action on Research in Health Services (PARIHS) Framework to Move from What We Know to What We Should Do for the Rehabilitation of a Painful Hemiplegic Shoulder (PHS)?
Authors Alatawi SF
Received 6 October 2022
Accepted for publication 6 December 2022
Published 14 December 2022 Volume 2022:15 Pages 2831—2843
DOI https://doi.org/10.2147/JMDH.S392376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Salem F Alatawi
Department of Physical Therapy, Faculty of Applied Medical Sciences, University of Tabuk, Tabuk City, Kingdom of Saudi Arabia
Correspondence: Salem F Alatawi, Email [email protected]
Introduction: Several theoretical frameworks currently promote the evidence-based clinical practice. One of these is Promoting Action on Research Implementation in Health Services (PARIHS) framework. However, The PARIHS framework emphasizes the use and implementation of pre-existing knowledge. This study aims to integrate of PARIHS conceptual framework to categorize evidence, context, and facilitation elements for the successful implementation of evidence-based painful hemiplegic shoulder (PHS) rehabilitation.
Methods: Stroke therapists (n=21) were interviewed to elicit important PHS rehabilitation concepts. Following that, a consensus approach was undertaken to tailor PHS recommendations to the local context. All consensus recommendations have been included in the PARIHS framework. The consensus level was set at 75% or more.
Results: The interviews revealed four broad themes of PHS rehabilitation, each further subdivided. Based on the themes and subthemes, 74 recommendations were deemed pertinent to PSH rehabilitation from a reliable source. Out of 74 recommendations, 63 recommendations reach the consensus level for PHS practice. Secondary prevention of PHS (n=10), assessment (n=14), PHS care management (n=19), and service delivery (n=20). A consensus was not reached for the remaining 11 recommendations. Each recommended guideline was integrated into the appropriate element of the PARIHS framework as follows: evidence (28), context (18), and facilitation (17).
Discussion: The findings showed how the PARIHS framework has been configured to empirically support the implementation of robust stroke rehabilitation recommendations in the field of rehabilitation. Using an implementation intervention theory (for example, PARIHS) as a guide, provide a thorough picture of the many levels that may affect implementation requirements.
Conclusion: Many prior studies on evidence-based stroke rehabilitation in physical therapy practice lacked knowledge of translation theories. This result illustrates how to use an intervention implementation (such as PARIHS) to enhance evidence-based practice implementation in routine stroke rehabilitation. Further study is required for the clinical use of the PARIHS framework.
Keywords: implementation, PARIHS framework, knowledge translation, stroke, hemiplegic shoulder, rehabilitation and clinical guidelines
Background
Painful hemiplegic shoulder (PHS) is a frequent post-stroke condition.1 It is a common clinical condition that arises after a stroke. Recent study shows that this condition affects 6–40% of people.1 Shoulder joint (humeral head subluxation or rotator cuff injury) and neurological disorders (spasticity, lack of sensation, hemispatial neglect, and initial flaccid paralysis) are all possible causes of PHS. Consequently, PHS may discourage patients from engaging in rehabilitation programs, prolonging disability.2
Numerous interventions have been investigated in PHS management. This includes: limb positioning,3 proper handling,4 upper limb supports such as slings, orthotics, and strapping,5,6 acupuncture,7 electrical stimulation for muscle contraction, transcutaneous electrical nerve stimulation for pain relief,8 intra-articular corticosteroids,9 and intramuscular botulinum injections,9 and mirror therapy.10 These treatment options were designed to avoid shoulder subluxation, reduce pain, and improve function. However, there is no consensus about which of these treatments is the most effective or useful for managing common PHS problems.11,12
Stroke clinical practice guidelines (CPGs) may help clinicians and patients make evidence-based treatment decisions.13,14 However, CPGs and actual practice diverge.7 Numerous studies suggest that inadequate research implementation leads to unsatisfactory healthcare outcomes.13–15 Time constraints, the process of disease management, patient engagement, validity, staffing concerns, training/education, treatment selection and priority, equipment availability, and team functioning/communications have all been identified as significant barriers to implementing stroke guidelines.13–15 Some strategies for physiotherapy implementation have been described in the physiotherapy literature,16–18 such as a theory-based guideline implementation tailored to identified barriers and facilitators, education, knowledge and experience sharing between researchers and clinicians, and institutional expertise. However, these suggested strategies focused on individual barriers, attitudes, abilities, and knowledge. As a result, improvements were limited to certain components of the implementation process, such as positive attitudes, increased knowledge of EBP, increased access to EBP resources, and the identification of potential barriers for future implementation efforts.
To address the problem of evidence-based stroke rehabilitation implementation, a paradigm change is necessary. This transformation needs systemic change, the identification of barriers to applying recommendations, and a variety of other variables, including persons and organizations.19,20 The area is advancing at a breakneck rate, and several frameworks for implementing evidence are now available. Promoting action on research implementation in health services (PARIHS) is one such example.20
PARIHS is a framework for knowledge translation. It is a framework based on heuristics. Implementing evidence is widely acknowledged as a complex process requiring systemic change and involving both individuals and organizations.20–22 According to a recent study, the PARIHS framework is growing rapidly in peer-reviewed papers, with 367 citations.23 However, its precise use remains unknown. According to this framework, successful implementation is dependant upon evidence, the environment, and the tactics employed to facilitate transformation.23
The PARIHS framework stresses the application and execution of pre-existing knowledge.20–23 This paper examined the PARIHS framework because it contends that successful implementation is the result of a relationship between evidence, the environment, and the tools used to facilitate transformation.20–23 This decision was made due to the complexity of implementation, which necessitates the integration of a large number of factors for a successful implementation process. Therefore, the multidimensional structure of PARIHS facilitates the acquisition of all the information required for the implementation process.
CPGs for stroke are vital sources of evidence in clinical practice.13,14 However, CPGs are applicable to all aspects of strokes. This may explain why, when treating persons diagnosed with PHS, physiotherapy treatments do not always follow these guidelines. To overcome this problem, this paper aims to integrate the PARIHS conceptual framework as a way of categorizing evidence, context, and facilitation elements for effective implementation of evidence-based PHS rehabilitation from a vast dataset of rigorous stroke sources of evidence such as Royal College of Physicians national clinical guidelines for stroke.24
Methods
A mixed-methods approach was used (Figure 1). These included interviews and consensus approach.25 The local research ethics committee (LREC) at the University of Tabuk; Tabuk-Saudi Arabia; approved the study’s continuation. Prior to participation, all interviewees provided signed consent after receiving enough information, and all participants gave their approval for the release of their anonymised data.
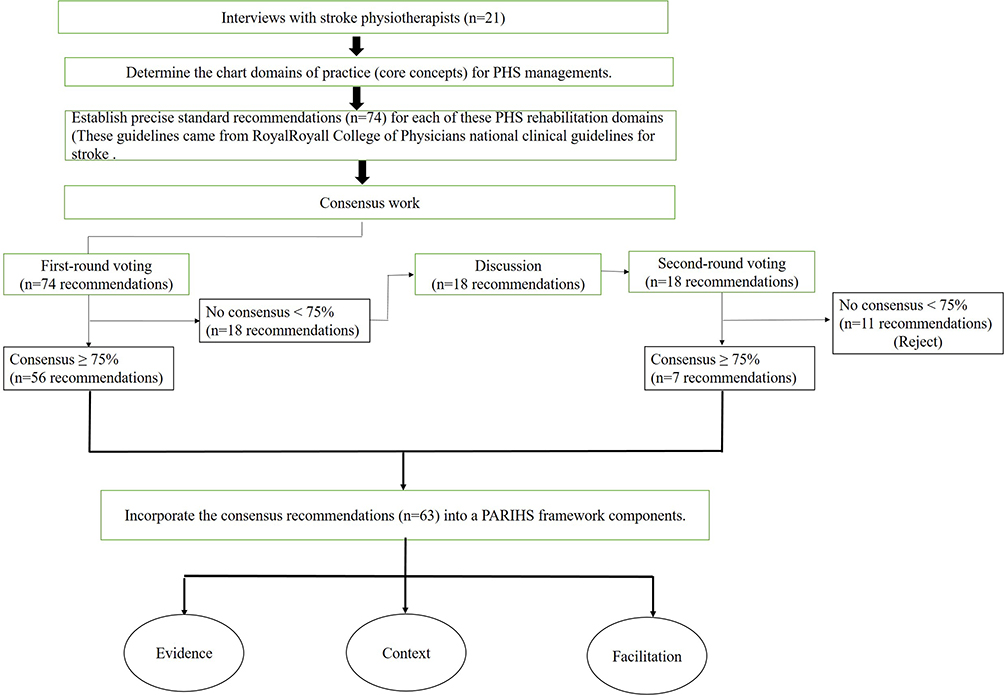 |
Figure 1 Diagram of the study design. A mixed-methods design, including interviews and a consensus approach, was used. |
Method 1: Interviews
Data was collected through individual/group interviews with stroke physiotherapists, and may be face to face or by telephone. In-depth interviews were conducted between June and August of 2022 at three separate stroke rehabilitation centres. Typically, the semi-structured interviews lasted between 20 and 30 minutes. The interview questions focused on the PHS rehabilitation practice of physiotherapists. The challenges of integrating evidence into practice were also questioned.
The managers of three stroke rehabilitation centres in Tabuk, Saudi Arabia, were invited to the introductory meeting to explain the purpose of the study and encourage their staff to participate. This was the most efficient recruitment approach for stroke physiotherapists.
The study project was presented separately to the staff at each of the three rehabilitation centres. The researcher gave a 20-minute presentation describing the study and the type of required participation, followed by an opportunity for questions. Everyone who attended the introductory sessions received an invitation and a letter of information. These meetings were attended by 35 stroke physiotherapists from three different rehabilitation centres. Twenty-one stroke physiotherapists were interested in taking part in the study. Within the context of the physiotherapist’s practice in PHS rehabilitation, participants were interviewed in a familiar environment.
The interview data were analysed using thematic analysis in accordance with the phases of theme analysis outlined by Braun and Clarke.26 The themes important to answering the study question were identified. The verbatim transcripts were reviewed line-by-line to identify patterns of meaning and potential issues of interest in order to identify emerging codes for interpreting what was occurring in terms of PHS interventions. Field notes were used to capture observations and conversational elements outside of recorded interviews.
Initially, a thematic map enabled the organizing of data into understandable groups and the formation of broader themes, which served as the basis for the interpretative analysis of the data. In the final theme map, data analysis reflects the reality of PHS interventions in physiotherapy practice to guide the adaptation of stroke best practice recommendations in this context.
Method 2: Consensus Workshop
Based on the key themes that were collected from the interviews (method 1), tailoring recommendations for PHS rehabilitation were acquired from a particular stroke source (Royal College of Physicians national clinical guidelines for stroke).24 Consequentially, a consensus method was used to determine the therapists’ perspectives on the chosen PHS rehabilitation recommendations. The data collecting workshops were organized in collaboration with interview participants and took place at a predetermined location. Consensus was defined as 75% or more.27,28 This option was chosen to preserve continuity with previous Chartered Society of Physiotherapy publications.27,28
Consensus workshop included three phases.25 However, prior to the workshops, the relevant PHS best practice recommendations were sent to the participants so that personnel could get familiar with the recommendations that will be adopted.
Phase 1: The First Round of the Voting
In this phase, on a three-point Likert scale (agree, neither agree nor disagree, disagree), 21 participants indicated their agreement or disagreement with using of a list of extracted recommendations form robust stroke to identify the relevance of each recommendation to PHS rehabilitation in real practice (Figure 2). These recommendations available in this phase came from Royal College of Physicians national clinical guidelines for stroke,24 and were based on the findings of the interviews (method 1).
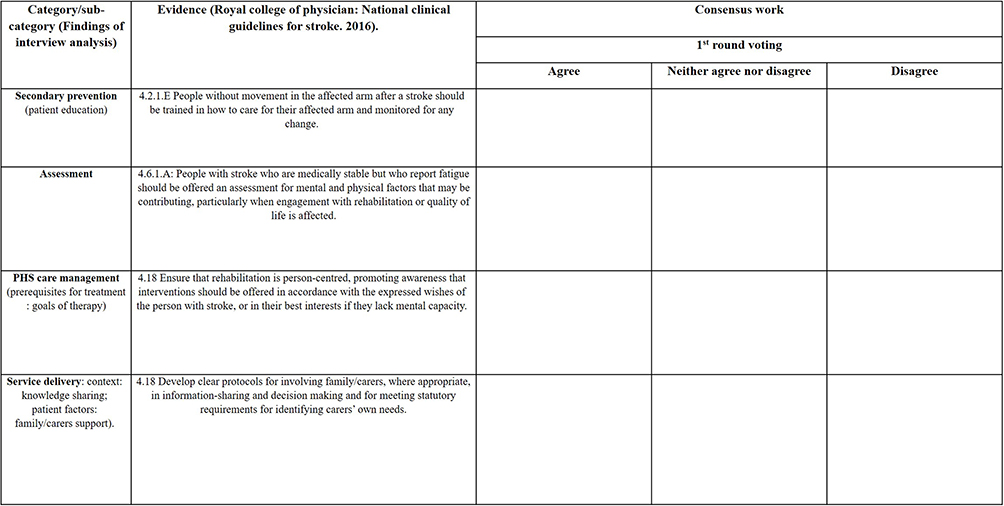 |
Figure 2 The first round of the voting. Participants were asked to score the recommendations retrieved from national guidelines and its relevance to their practice during this phase. |
Phase 2: Discussion Meeting
The results of the first round of voting were provided in order to determine which of the list of recommendations the majority of respondents deemed to be evidence of therapists’ practice in PHS rehabilitation. For those recommendations not reached consensus level (less than 75%), scores were discussed. Furthermore, the components of PARIHS framework (evidence, context, facilitation) were explained by the researcher. This discussion was a good way to unpack meanings of PARIHS framework components and enabled stroke therapists to give their opinions and any unobvious issue. This step was necessary for the second round of the voting. Supporting material was supplied on the context and facilitation components.
Phase 3: The Second Round of the Voting
In the same way as previously, participants were asked to indicate their agreement or disagreement on a three-point Likert scale for recommendations that did not get consensus (less than 75% in the first vote). However, this time they were asked to consider the discussion in addition to their knowledge and experience. Then, all recommendations from both rounds with 75% or more agreement were delivered to participants in order to incorporate each recommendation into a single PARIHS component (Figure 3).
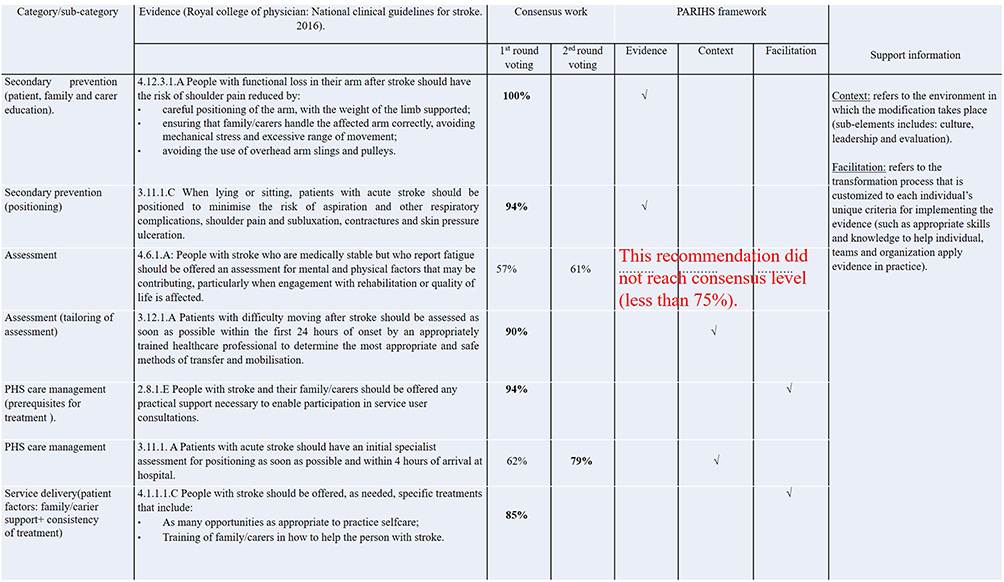 |
Figure 3 The second round of voting. Participants were asked to re-rate recommendations that fell short of consensus in the first round of voting (less than 75%), and then integrate each evidence from both rounds into one of the PARIHS components. |
Findings
Socio Demographic Characteristics of the Participants
Thirty-five physiotherapists participated in this study. Twenty-one physiotherapists from different centers responded, for a 60% response rate. Table 1 details the participants’ characteristics.
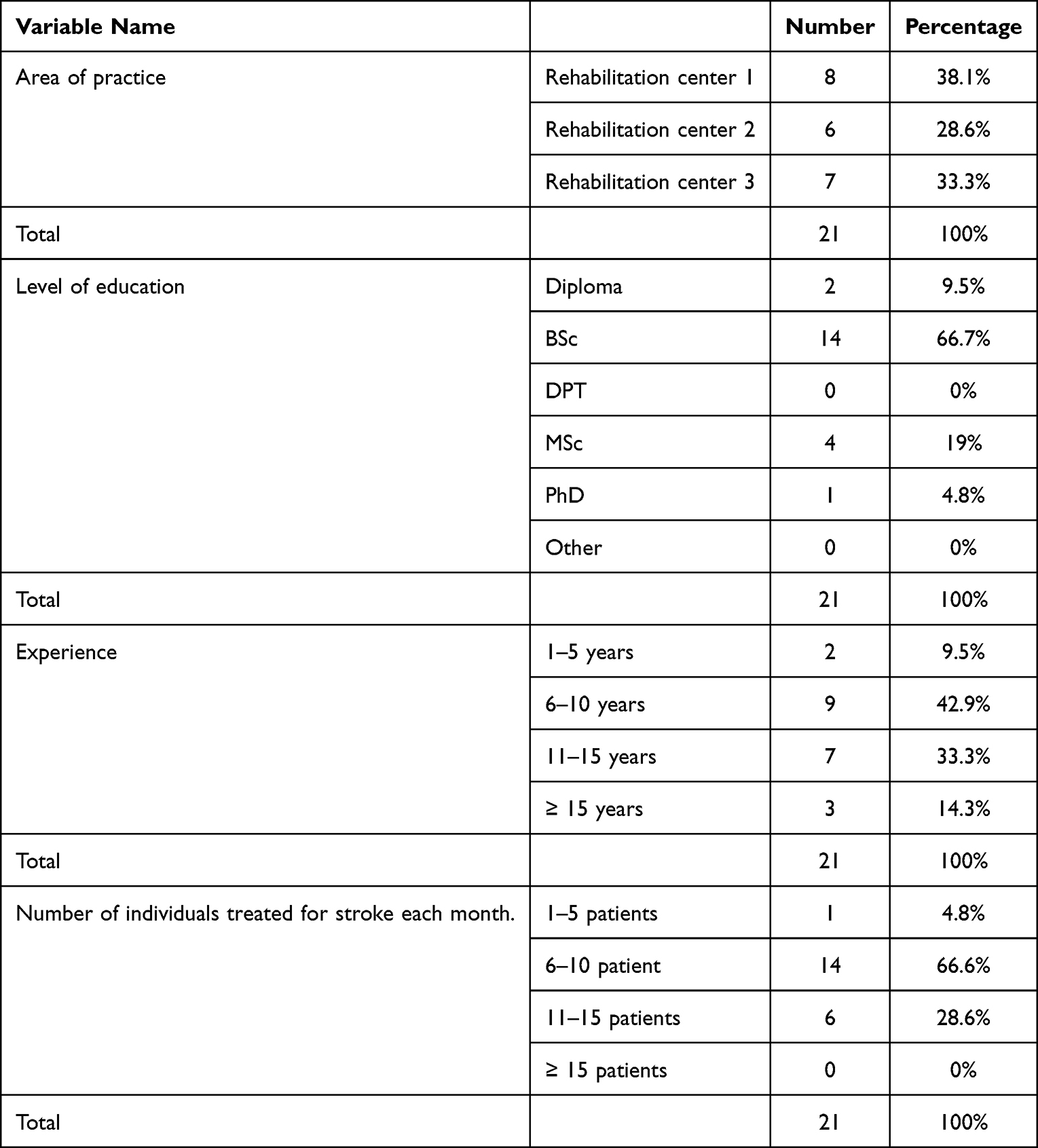 |
Table 1 Respondents Socio-Demographic Characteristics (n=21) |
Result of Method 1: Interviews
This part offered the analysis of interview data about current stroke therapist practices in PHS rehabilitation (first component of interviews), as well as the barriers to integrating evidence into practice (second component of interviews).
The domains of practice of the participating physiotherapists in relation to PHS rehabilitation stroke were mapped using interview data. Four major themes were discovered that affected PHS rehabilitation in physiotherapists’ practices and the implementation of evidence-based practice in this setting. These included prevention of secondary complications, assessment, management of PHS care, and service delivery. Each area was further subdivided based on the findings of interviews (Table 2).
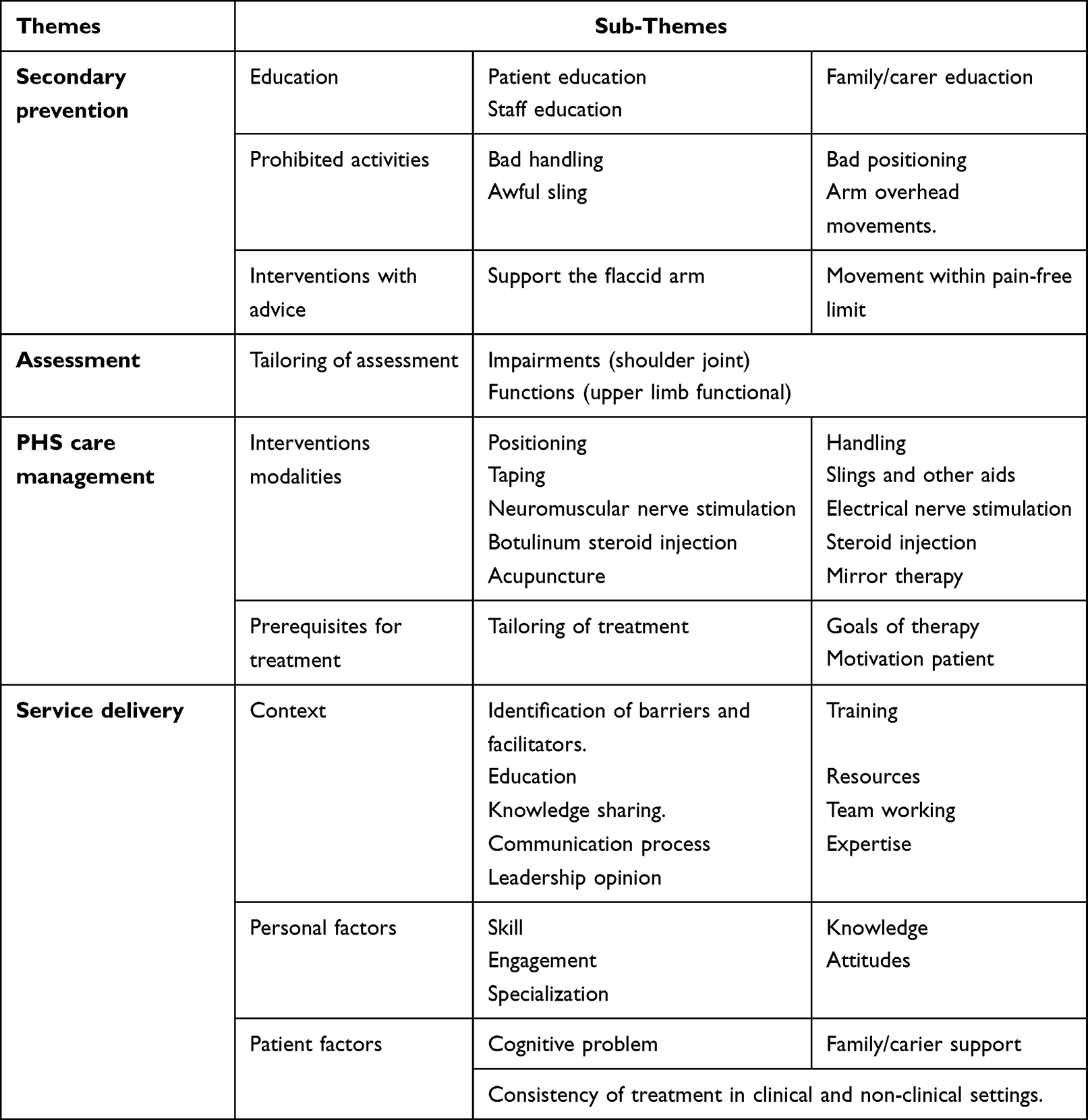 |
Table 2 Summarizes the Findings of the Interviews. It Provides an Illustration of the Major Themes and Subthemes |
Data Gathered from the First Component of Interviews (Current Practice of Physiotherapists in PHS Rehabilitation)
The data analysis from the first component of the interviews showed three core themes that may represent the primary areas of current physiotherapy practice in connection to PHS rehabilitation. These included of prevention of secondary complications, assessment, and management of PHS care.
Theme 1: Prevention of Secondary Complications
This theme was divided into three subthemes (education, prohibited activities, and intervention with advice). Each of these subthemes has fundamental elements (Table 2).
Educating the patient, their family or carers, and the staff is one of the most effective approaches to prevent secondary prevention of PHS and improve PHS rehabilitation. Participants highlighted the need of educating the whole rehabilitation team, patients, and families/caregivers about prohibited activities, such as improper handling, positioning, slinging, and arm overhead movements. Participants underlined the need of physiotherapists informing other teams about the importance of preventing shoulder pain via training staff in the correct arm manipulation method. If stroke treatment practitioners lacked certain skills and training, there would have been a loss of trust, anxiety, and contempt.
You’ve got to step in and say, “Stop, you can’t do that”. That’s unacceptable. We must demonstrate why it is important to support and positioned properly and why it should not be abused. The manner in which the patient is handled should be essential, understood by all team members, and then consistently carried out.
Participants clearly concentrated their attention on preventing secondary complications of PHS. Participants highlighted the need of preventing secondary complications before to making any progress, since these complications might cause shoulder pain and limit PHS rehabilitation. The results revealed that physiotherapists were aware of many PHS risk factors. According to participants, movement out of pain limit, and unsupported the flaccid arm after a stroke causes shoulder pain. This has been found as a significant contributor to PHS.
Initially, the priority lies in protecting the limb and the shoulder from complications. I focus a lot on the movement within pain-free limit and support the flaccid arm. I think that the biggest risk straight after stroke is subluxation, and then that leads to pain. It is always to stop things from happening early on.
Theme 2: Assessment
Tailoring of assessment was the main sub-theme in this section. However, the two key components of the PHS assessment, impairment and activity restriction, were covered during the therapist interviews. Numerous participants said that they would begin evaluating patients’ abilities, including their range of motion, pain threshold, and sense of touch. The physiotherapists agreed that since pain is frequently subjective, self-reported pain measures are the most widely used to assess shoulder pain after stroke. However, such assessments might be difficult to use, particularly after a stroke, when cognitive deficiencies and communication issues exist.
It’s self-evident that fundamental characteristics such as range of motion, whether active or passive, are critical. I’d be delighted if shoulder movement resulted in pain. Their strength, sensation, coordination, joint integrity, and stiffness. If patients have significant shoulder discomfort, I examine them using the visual analogue scale.
All participants agreed that they evaluated patients’ functional activities. According to participants, it focuses on patients’ ability to do an activity. These were the best ways to examine the whole upper limb after a stroke. The wide variety of techniques to measure shoulder pain after stroke is largely due to the variety of difficulties that hinder shoulder pain. As a consequence, physiotherapists recognized the need of tailoring assessments of shoulder pain.
Outcome measures in stroke are quite hard. Our goal would be to improve functional measures across the board, rather than concentrating only on the shoulder. Thus, I generally begin by assessing their current active mobility and then focusing on ways to improve it, which is usually the primary objective.
Theme 3: Management of PHS Care
This theme covers two primary subthemes: intervention modalities and treatment prerequisites. However, each comprises of several necessary elements.
According to interviews, physiotherapists may use a variety of interventions to aid patients in preventing shoulder pain. Some physiotherapists believed that using a strapping, splint or arm support cushion to treat a subluxed shoulder was equally effective. Additionally, physiotherapists advocated positions that kept the arm away from the body in order to stretch tight muscles and maintain their length in order to prevent contractures.
My view is from day one patients’ position. It is imperative to look at the position of the arm, muscle strength, and the amount of tone. I typically sling, support them straight, and correct the arm position.
Shoulder pain after a stroke may result in a variety of complications. Participants reported that tailoring interventions helped alleviate shoulder pain after stroke. Depending on the priority, interventions may be modified to deviate from the treatment plan. Participants saw a dramatic change in PHS management’s rehabilitation strategies. During the early phases of PHS rehabilitation, the major objective was to avoid secondary complications. On the other hand, later stages emphasize preserving range of motion and functional ability. According to the participants, tailoring of interventions was essential for resolving shoulder pain after stroke. Tailoring of interventions may be used to deviate from the treatment plan depending on prioritization.
If it was completely flaccid. To avoid subluxation, I usually sling them straight. It is imperative to look at the position of the arm, muscle strength, and the amount of tone. If the stroke patient’s main complaint is a loss of power, then concentrate on active range of motion, sitting balance, and trunk posture, which acts as the foundation for the upper limb, is your adaptive shift here.
Participants highlighted that there was a substantial shift in the emphasis of treatments from preventative in the early stages to supportive in the late stages with the use of a variety of intervention modalities.
Occasionally, in chronic conditions, electrical nerve stimulation, TENES, injections, acupuncture, and mirror therapy may be used to help in pain management and function improvement.
Participants agreed that educating patients on patient-centered goal setting and giving accurate information about their health, prognosis, and length of treatment were critical to PHS rehabilitation. As a result, more effective goal setting may have a beneficial influence on not just patient satisfaction, but also on the rehabilitation quality.
I feel that bringing up the patient’s objectives is a really effective way to keep them engaged in rehabilitation.
The level of motivation shown by the patient was an essential factor in the progression of the PHS patients’ rehabilitation. Participants who were interviewed said that in order for patients to keep a high level of motivation during the exercise program, they need support or help from a caregiver or assistant.
Stroke patients may have several difficulties. It is essential to determine what works best for them. You may need to include their family as a strategy to increase their motivation.
Data Gathered from the Second Component of Interviews (Integrating Evidence into Practice)
The second section of the interview data revealed a number of different motivations and restrictions, which may either facilitate or impede the implementation of PHS best practice respectively. The main theme in this section was service delivery. However, this theme has three basic sub-themes: the context, personal factors, and patients’ factors. Every sub-themes includes a variety of key aspects that were necessary to ensuring the rehabilitation of PHS was successful (Table 2).
Participants indicated that their workplaces had a major influence on the evidence integration process. Everyone believed that identifying local barriers and facilitators inside rehabilitation institutions was one of the most important factors. In order to maximize the effectiveness of the implementation process, it is necessary to regularly evaluate the internal characteristics of the organizations. These include the availability of resources, staff training, expertise, local opinion leaders, discussion groups, information sharing, and educational meetings.
Each day, there was a group discussion, and we engage with one another and the speech therapist, phoning my colleagues on occasion. So, any concerns regarding a hemiplegic arm may be discussed, and the most effective treatment can be considered.
In addition to organizational factors, there are also individual physiotherapy factors that must be taken into account. Physiotherapists emphasized the significance of knowledge, skill, training, and clinical experience as potential elements that may play a role in the treatment of more challenging rehabilitation conditions, such as PHS.
I believe it is essential for organizational structures to ensure that therapists are up-to-date, get continual training, have high skill levels and confidence, and that staff members who specialize in stroke and treating stroke patients are reading all the evidence.
Integrating evidence into practice and improving the management of PHS rehabilitation may be significantly influenced by patient factors. Consistency in treatment procedures across professional and personal contexts, physiotherapists believe, may aid in the reduction of post-stroke shoulder soreness. The most effective treatments for shoulder pain after a stroke differ significantly between home and professional settings. Participants stressed the critical nature of patient adherence to prescribed home exercise routines. On the other hand, consistency in treatment across professional and household settings is a serious problem.
It may be due to inconsistency in treatment approaches from hospital to home, or it could be due to the environment changing and therefore the way the patient respond. Patients’ families, caregivers, and diaries all play an important role in encouraging and inspiring them to exercise.
Cognitive difficulties may have an effect on how physiotherapists treat stroke patients. Poor compliance, according to interview data, may have harmed treatment efficacy. Patients’ inability to interact or participate actively in the treatment session, as well as their difficulties comprehending the content presented, were important problems. They agreed that motivation is critical in physiotherapy treatment, much more so when patients are hopeless, despairing, or confused. In these instances, physiotherapists recommend discussing treatment with the patient and including family members or carers in the delivery and completion of the treatment program. Many physiotherapists believe patients’ aversion to rehabilitation treatments comes from a fear of pain. Despite their desire to engage in upper limb rehabilitation exercises, patients were physically unable to do so, which was disappointing and sad.
Many stroke patients may have cognitive impairment as a result of the stroke. So it’s vital to figure out what works best for them. Therapists may need to bring the family and judge with them to determine how they operate.
Participants believed that patients needed support or help from an aid or caregiver to maintain a high degree of motivation to continue with the exercise program. For stroke patients engaged in a rehabilitation program, measures such as including family members and maintaining diaries to monitor patients’ skills were recommended. Participants emphasized the critical significance of patients adhering to their home exercise program.
Patients’ families, caregivers, and diaries all play an important role in encouraging and inspiring them to exercise.
Alignment of Interview Findings with Stroke National Clinical Guidelines from the Royal College of Physicians
Synthesis of the two components of interviews provides the opportunity to enrich understanding of evidence-based healthcare practice. Based on the findings of the interviews (themes/sub-themes), the researcher derived several recommendations from the Royal College of Physicians’ national clinical guidelines for stroke.24 From the total number of recommendations (n = 402), 74 “core recommendations” were selected for use in the consensus work as following: prevention of secondary complication of PHS rehabilitation (n=10), assessment (n= 18), management (n=23), and service delivery (n=23). These recommendations (n=74) were rated on a three-point Likert scale (agree, neither agree nor disagree, disagree). This step was necessary to plan consensus data collection (method 2).
Result of Method 2: Consensus Work
The consensus work method was designed to incorporate national best practice recommendations for stroke into PHS management. This method may also enable participants in being familiar with stroke best practice guidelines and adapting them to PHS rehabilitation. Three phases was included in this consensus approach: first round voting, discussion meeting, and second round voting.
Result of Phase 1: First Round of Voting
From this list of recommendation (n=74) based on the interviews findings, a number of recommendations (n=56) were reached a consensus level (75% or more) in the first round of the questionnaire (Figure 2). The 18 recommendations with less than 75% agreement in the first round of the voting were subjected to a discussion meeting.
Result of Phase 2: Discussion Meeting
In this phase, participants discussed those recommendations (n=18) did reach a consensus level (<75%) from the first round of voting. At this meeting, the results of the first round of voting were presented, with a particular focus on the 18 recommendations that failed to achieve consensus. Participants explored the reasons why these recommendations did not reach consensus. The discussion also revealed the impact of individual, organizational, and internal practices on the first round of voting. At the end of this discussion, the researcher provided an explanation of the PARIHS framework and allowed participants to express their views on any ambiguous issue.
Result of Phase 3: The Second Round of Voting
After the discussion, participants were given a second chance to vote on those proposals that did not get 75% support during the first round of voting. In this phase, seven additional recommendations have reached consensus after re-rating (n=7), whilst eleven further recommendations were judged undesirable (n=11).
All consensus recommendations from both rounds of voting (n=63) were then allocated to a particular PARIHS component, as follows: evidence (n=28), context (n=18), and facilitation (n=17). Figure 3 illustrates how recommendations are disseminated to major key concepts and then subjected to consensus before being included into the PARIHS framework’s components. (For a complete list of recommendations, please refer to Supplementary File 1).
Discussion
This study presents a novel method for adapting specific recommendations applicable to the treatment of individuals with PHS from a large source of recommendations applicable to the treatment of individuals with stroke in general, and used the PARIHS framework to determine which constructs each recommendation matches.
It also provides a novel approach to extracting individualized PHS rehabilitation data from the broad consensus evidence on stroke. The interviews findings developed a tool to derive the related evidence in PHS rehabilitation from the different potential sources either theoretically from research findings (through literature), or real-world clinical experience and patient preferences (via interviews). The results of this study show that systemic changes are required to ensure that evidence is incorporated into clinical practice. This was accomplished by using consensus-based PHS rehabilitation recommendations and interviews to determine what variables impacted the usage of data in daily tasks Evidence-based clinical recommendations include high-quality clinical research with expert and patient feedback.13–15
The three components of the PARIHS framework (evidence, context, and facilitation)20 were linked to robust evidence in relation to PHS rehabilitation that guarantee to extracted this evidence with identify other factors (such as context, personal, and patient factors) and their impact on implementation process.
The study’s findings indicate that contextual and facilitator factors are inextricably linked to the development of evidence-based practice in PHS rehabilitation. For example, knowledge sharing is a critical component of the PARIHS framework’s item under context component. To increase knowledge sharing, organizations should encourage people to network often both inside and outside the organization.13,21,22 Organizations play a critical role in encouraging clinical specialty participation via core special interest groups, email services, and visits to other organizations.15,21,22 Additionally, organizations may collaborate with clinicians to create best practices. It may be possible to support the establishment of interdisciplinary local guidelines/protocols and organizational processes for service user engagement.22 Regular team meetings and informal interaction spaces may also facilitate sharing and learning amongst practitioners.13,15,21,22
Other recommendations concentrate on what organizations should do to implement successfully. Facilitators such as frequent and effective clinical supervision of individuals, groups, or teams, leadership, resources, as well as organized time, continuous training and education, and procedures for people and groups to reflect on their practice, are critical for effectively applying the knowledge in daily practice. Prior study findings,13–15,19–21 stress the critical role of organizations in encouraging and enabling the acquisition of new knowledge via the provision of appropriate facilitators and the elimination of obstacles.
The recommendations extracted from stroke guidelines and related to the facilitation component of the PARIHS framework emphasized the importance of conducting an investigation and determining the characteristics of the individuals who will deliver the intervention, as well as how these characteristics may affect implementation and effectiveness. Individual barriers (such as skills, training, experience, time and knowledge) have been shown to hinder innovation and the implementation of evidence-based practices in earlier researches. Identifying and overcoming these obstacles is crucial to implementing new evidence in practice.16–18,21,22
Patient preferences may facilitate or obstruct the implementation of PHS rehabilitation. Certain recommendations may be rejected due to worries about the patient’s worth, relevance, or a gap between actual and expected recovery. Rehabilitation takes into account pain, exhaustion, tone, aphasia, co-morbidities, and cognition. Furthermore, the recommendations derived from this study emphasize the need of a motivated patient during PHS rehabilitation. Patient motivation was critical in integrating evidence and enhancing PHS patient rehabilitation. As previously stated29,30 without effective goal setting during rehabilitation, patients’ motivation cannot be significantly increased. As a result, improved goal setting may result in an increase in patient satisfaction and rehabilitation effectiveness.
Family members were a key role in incorporating evidence into clinical practice in PHS rehabilitation. Family members may either facilitate or hinder the recommendation’s implementation. With limited time to supervise a large number of patients, physiotherapists relied on family members’ availability and willingness to follow recommendations, particularly outside of treatment time. However, the issue of treatment disparity between clinical and non-clinical settings was highlighted.11–14
Limitation
For the first time in physiotherapy, the PARIHS framework combined a large quantity of PHS rehabilitation evidence. However, since all participants are local Saudis, they are presumably familiar with the Saudi healthcare research environment. As a result, research results may be limited to these or similar circumstances. However, the study’s aim is to learn how to apply the PARIHS framework therapeutically, not to generalize statistically. Furthermore, rehabilitation center managers assisted in the recruitment of stroke physiotherapists during the phase of data collection. Participants may therefore feel compelled to participate in the study. It was, however, unable to communicate with the stroke physiotherapists without first speaking with and receiving permission from the rehabilitation center’s managers. Another limitation of this study is that the compliance of individuals and organizations with the derived recommendations was not examined. Internationally, further work is necessary.
Conclusion
This study, it is considered, gives conceptual clarity about the use of the PARIHS framework in a real-world practice context. Additional study is needed in this area to determine clear and consistent approaches to use the PARIHS framework in real-world clinical settings.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article [and its Supplementary Information File].
Disclosure
The authors report no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Nadler M, Pauls M, Cluckie G, Moynihan B, Pereira AC. Shoulder pain after recent stroke (SPARS): hemiplegic shoulder pain incidence within 72 hours post-stroke and 8–10 week follow-up (NCT 02574000). Physiotherapy. 2020;107:142–149. doi:10.1016/j.physio.2019.08.003
2. Treister AK, Hatch MN, Cramer SC, Chang EY. Demystifying poststroke pain: from etiology to treatment. PM R. 2017;9(1):63–75. doi:10.1016/j.pmrj.2016.05.015
3. Borisova Y, Bohannon RW. Positioning to prevent or reduce shoulder range of motion impairments after stroke: a meta-analysis. Clin Rehabil. 2009;23(8):681–686. doi:10.1177/0269215509334841
4. Lynch D, Ferraro M, Krol J, Trudell CM, Christos P, Volpe BT. Continuous passive motion improves shoulder joint integrity following stroke. Clin Rehabil. 2005;19(6):594–599. doi:10.1191/0269215505cr901oa
5. Huang YC, Chang KH, Liou TH, Cheng CW, Lin LF, Huang SW. Effects of kinesio taping for stroke patients with hemiplegic shoulder pain: a double-blind, randomized, placebo-controlled study. J Rehabil Med. 2017;49(3):208–215. doi:10.2340/16501977-2197
6. Liu J, Feng W, Zhou J, et al. Effects of sling exercise therapy on balance, mobility, activities of daily living, quality of life and shoulder pain in stroke patients: a randomized controlled trial. Eur J Integr Med. 2020;35:101077. doi:10.1016/j.eujim.2020.101077
7. Liu S, Zhang CS, Cai Y, et al. Acupuncture for post-stroke shoulder-hand syndrome: a systematic review and meta-analysis. Front Neurol. 2019;10:433. doi:10.3389/fneur.2019.00433
8. Whitehair VC, Chae J, Hisel T, Wilson RD. The effect of electrical stimulation on impairment of the painful post-stroke shoulder. Top Stroke Rehabil. 2019;26(7):544–547. doi:10.1080/10749357.2019.1633796
9. Chiu YH, Chang KV, Wu WT, Hsu PC, Ozçakar L. Comparative effectiveness of injection therapies for hemiplegic shoulder pain in stroke: a systematic review and network meta-analysis. Pharmaceuticals. 2021;14(8):788. doi:10.3390/ph14080788
10. Pervane Vural S, Nakipoglu Yuzer GF, Sezgin Ozcan D, Demir Ozbudak S, Ozgirgin N. Effects of mirror therapy in stroke patients with complex regional pain syndrome type 1: a randomized controlled study. Arch Phys Med Rehabil. 2016;97(4):575–581. doi:10.1016/j.apmr.2015.12.008
11. de Sire A, Moggio L, Demeco A, et al. Efficacy of rehabilitative techniques in reducing hemiplegic shoulder pain in stroke: systematic review and meta-analysis. Ann Phys Rehabil Med. 2021;65(5):101602. doi:10.1016/j.rehab.2021.101602
12. Dyer S, Mordaunt DA, Adey-Wakeling Z. Interventions for post-stroke shoulder pain: an overview of systematic reviews. Int J Gen Med. 2020;Volume 13(13):1411–1426. doi:10.2147/IJGM.S200929
13. Bernhardsson S, Larsson ME, Eggertsen R, et al. Evaluation of a tailored, multi-component intervention for implementation of evidence-based clinical practice guidelines in primary care physical therapy: a non-randomized controlled trial. BMC Health Serv Res. 2014;14:105. doi:10.1186/1472-6963-14-105
14. Van der Wees PJ, Moore AP, Powers CM, et al. Development of clinical guidelines in physical therapy: perspective for international collaboration. Phys Ther. 2011;91(10):1551–1563. doi:10.2522/ptj.20100305
15. Alatawi SF. From theory to practice: a conceptual framework to facilitate implementation of evidence in stroke rehabilitation for local context in Saudi Arabia. J Multidiscip Healthc. 2019;5(12):515–525. doi:10.2147/JMDH.S212372
16. Paci M, Faedda G, Ugolini A, Pellicciari L. Barriers to evidence-based practice implementation in physiotherapy: a systematic review and meta-analysis. Int J Qual Health Care. 2021;33(2). doi:10.1093/intqhc/mzab093
17. da Silva TM, Costa Lda C, Garcia AN, Costa LO. What do physical therapists think about evidence-based practice? A systematic review. Man Ther. 2015;20(3):388–401. doi:10.1016/j.math.2014.10.009
18. Scurlock-Evans L, Upton P, Upton D. Evidence-based practice in physiotherapy: a systematic review of barriers, enablers and interventions. Physiotherapy. 2014;100(3):208–219. doi:10.1016/j.physio.2014.03.001
19. Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust. 2004;180(S6):S57–S60. doi:10.5694/j.1326-5377.2004.tb05948.x
20. Rycroft-Malone J, Bucknall T. Models and Frameworks for Implementing Evidence-Based Practice: Linking Evidence to Action. Oxford: John Wiley & Sons; 2010.
21. Kitson A, Rycroft-Malone J, Harvey G, McCormack B, Seers K, Titchen A. Evaluating the successful implementation of evidence into practice using the PARiHS framework: theoretical and practical challenges. Implement Sci. 2008;3:1. doi:10.1186/1748-5908-3-1
22. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297–304. doi:10.1097/00001786-200410000-00002
23. Bergstrom A, Ehrenberg A, Eldh AC, et al. The use of the PARIHS framework in implementation research and practice—a citation analysis of the literature. Implement Sci. 2020;15(1):1–51. doi:10.1186/s13012-019-0962-7
24. Royal college of physicians. National clinical guidelines for stroke; 2016. Available from: https://www.strokeaudit.org/SupportFiles/Documents/Guidelines/2016-National-Clinical-Guideline-for-Stroke-5t-(1).aspx.
25. Rycroft-Malone J. Formal consensus: the development of a national clinical guideline. Qual Health Care. 2001;10(4):238–244. doi:10.1136/qhc.0100238
26. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
27. Bramwell L, Elaine H. The Delphi technique: a possible tool for predicting future events in nursing education. Canadian. J Nurs Res Arch. 1999;6(1):23–32.
28. Moore A, Jackson A, Jordan J, et al. Clinical Guidelines for the Physiotherapy Management of Whiplash Associated Disorder. London: Chartered Society of Physiotherapy; 2005.
29. Rice DB, McIntyre A, Mirkowski M, et al. Patient-centered goal setting in a hospital-based outpatient stroke rehabilitation center. PM R. 2017;9:856–865. doi:10.1016/j.pmrj.2016.12.004
30. Rosewilliam S, Roskell CA, Pandyan AD. A systematic review and synthesis of the quantitative and qualitative evidence behind patient-centred goal setting in stroke rehabilitation. Clin Rehabil. 2011;25(6):501–514. doi:10.1177/0269215510394467
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.