")
Back to Journals » Advances in Medical Education and Practice » Volume 13
How Can We Improve the Delivery of Urology Teaching to Medical Students Using Modern Educational Techniques?
Authors Gaba F , Gaba QQ, Fernando DA
Received 25 April 2022
Accepted for publication 22 July 2022
Published 27 July 2022 Volume 2022:13 Pages 777—780
DOI https://doi.org/10.2147/AMEP.S372242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Fortis Gaba,1 Qassi Q Gaba,2 Dilini A Fernando3
1University of Edinburgh Medical School, University of Edinburgh, Edinburgh, UK; 2Department of Medical Sciences, University of Oxford, Oxford, UK; 3Ninewells Hospital and Medical School, University of Dundee, Dundee, UK
Correspondence: Fortis Gaba, University of Edinburgh Medical School, University of Edinburgh, 47 Little France Cres, Edinburgh, EH16 4TJ, UK, Tel +447783985984, Email [email protected]
Abstract: It is generally well-known that the medical school curriculum is becoming increasingly busy, more so with the COVID-19 pandemic. By itself, urology education will need to adapt to meet the changing circumstances, but it remains uncertain on how best to address this need. In this article, we will discuss several methods that will allow institutions to ease and overcome pressures using modern educational techniques. These methods can be classified based on the aspect of the curriculum they seek to improve, namely core-curricular teaching, anatomy training, virtual reality, and electronic learning opportunities. We anticipate that the implementation of these suggestions will enhance medical school teaching.
Keywords: surgical education, urology, medical school curriculum, modern educational techniques
Background
Urology-related emergencies account for >20% of all acute surgical admissions and 5%–10% of general practitioner visits.1 Yet, urology teaching only appears in 37% of UK medical school curricula.2 Therefore, there is a clear need to improve the extent of urology education and the quality at which it is administered. There are many views on how best to address this unmet need. However, based on our experience and the evidence we will describe, we believe that the most fundamental components of medical school education are anatomy demonstrations, lectures, virtual reality-based, and electronic learning opportunities. Hence, focusing our efforts on improving these aspects should be the priority.
New Approach
Bridging the Gap Between Theory and Practice: Anatomy Training
In the classroom, students who engaged with interactive anatomy significantly improved their academic performance.3 Whilst in clinical practice, 32% of claims to the Medical Defence Union are due to anatomical errors.4 Such evidence illustrates that anatomy teaching is essential for future doctors, both in education and practice. Current anatomy teaching is often performed using cadavers, which are expensive and sometimes inaccessible. Hence, we ought to develop sustainable alternatives. Whilst anatomical videos and virtual models have been proposed, they too are limited, particularly given the lack of tactile learning. One more promising suggestion is the use of simulation models, which offers similar opportunities for anatomy demonstrations without the associated challenges. Simulation exercises with models can be performed via online platforms with an instructor. One example of a model for prostatectomy is illustrated in Figure 1. Of course, one may argue that the models are not cost-effective and do not mimic human tissue. However, findings from a study conducted by Matsumoto et al (2002) addresses this criticism. The group showed no significant difference in endourological performance between anatomical models that cost $20 versus $3700.5 Therefore, models do not need to be expensive to be useful. Similarly, given the speed at which technology is progressing, anatomical models will soon be sufficient to mimic cadavers for demonstration purposes. For inspiration, we only need to look at companies like Peninsula Radiology Academy™ who have made a renal pelvicalyceal system that responds to fluid, akin to a hydronephrotic kidney.6 During times where some universities have completely abandoned dissection, anatomical models may provide the best solution.
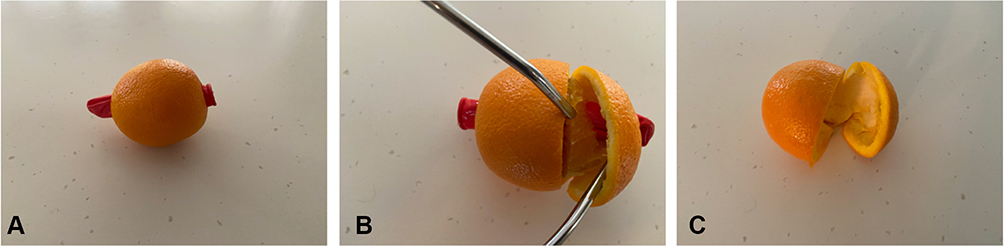 |
Figure 1 A prostatectomy model was used to teach medical students. (A) A balloon is inserted through the orange to act as the urethra. (B) The urethra can be stretched and incised as in real cases. (C) Once the pulp (benign tissue) has been removed using surgical dissection, the skin (normal prostate) can be closed. |
Virtual Reality (VR)
Traditional anatomy teaching encompasses lectures, cadaveric models and 2D atlases. Advance 3D VR software, is a stepping stone into the future of sustainable and interactive learning of anatomy. Chen et al in 2020 have shown that skull virtual learning resource is as effective for learning. VR allows for one to learn at their own pace, instead of designated anatomy learning time slots.7 As VR technology evolves, one may be able to enter the virtual surgical room and operate. Given the extra precautions mandated during the COVID-19 pandemic, this will provide students with the opportunity to operate in a virtual stimulated setting.
Turning Medical Education Upside Down: Flipped Classroom Approach (FCA)
Stuart and Rutherford (2003) analyzed 1353 questionnaires to show that a student’s attention span peaks in 10–15 min and then declines.8 Despite this data and those from similar experiments, UK institutions still hold hour-long lectures. Whilst some institutions have attempted to solve the problem by using audience response systems such as clickers, these were not associated with increased academic performance.9 A more promising alternative is the flipped classroom approach (FCA). Students learn core content on their own, then apply their knowledge in role-play, designing concept maps, and group discussions online or in person. Studies have shown medical students exposed to the FCA scored significantly higher in their modules than those attending traditional lectures.10 Furthermore, Morgan et al showed that a flipped classroom curriculum would decrease the amount of required teaching time without detrimentally affecting student performance on examinations.11 The time saved can be re-allocated through the implementation of ideas that we will outline in subsequent paragraphs. It is worth noting that the format of FCA places more importance on self-directed study. Whilst various approaches can be taken to complement FCA in this regard, few seem more effective than the use of electronic-learning (E-learning) resources.
Utilizing the Cloud: E-Learning
E-learning involves the use of electronic media for medical education; its implementation has shown to be beneficial. For example, Schneider and Albers (2015) found that students using computer-based cases scored 20% higher in urology exams than those using paper-based methods.12 This is particularly effective as a teaching tool for urology as it helps students practice imaging analysis and urological procedures, skills that are often essential in clinical cases, from the comfort of their own homes. As an example, Heinrich Heine University in Dusseldorf uses a web-based learning system, called CASUS™, which provides students with clinical cases in which they assess imaging data to devise a management plan. Students receive instant feedback regarding their performance and can watch videos from the operation theatre to gain an impression of the techniques used. Manalo et al 2021 created a 1-week virtual urology course with surgical video reviews and case-based exercises, enrolling nine medical students. All students reported an increased understanding of common urologic diagnoses by an average of 2.5 points on a 10-point Likert scale with 56% students reporting increased interest in urology as a specialty.13 As the longevity of the COVID-19 pandemic has become increasingly more prevalent, virtual teaching can be intertwined with the current medical curriculum.
Evaluation
It is Easier Said Than Done: Potential Challenges
Many of the ideas we have suggested are theoretical; it is also important to consider their feasibility on an institutional level. Despite the benefits of E-learning, only a few institutions have adopted E-learning approaches for teaching, principally owing to the associated costs. For example, Harvard Medical School has spent over $200,000 on facilities needed for their E-learning modules.14 Not all schools have this budget. Similarly, not all schools have the online resources or faculty to implement FCA, which is optimized with a class size of ≤18.15 Because of such difficulties, institutions should consider a more measured approach to implementation, perhaps collaborating to form an E-learning repository and maintaining a combination of lectures and FCA. Results from a multicenter, cross-sectional evaluation of urology teaching in the UK showed that 20.1% of foundation year 1 doctors received no medical school attachment in urology prior to working on the hospital ward.16 The results indicate urology teaching can vary considerably in the UK, which prompts speculation of inadequate “lobbying power” within our current medical school curriculum. These are a few challenges that may prevent the advancement of medical school urological teaching.
Conclusion
Optimal urology education using modern educational techniques can take many forms. We have proposed that improving virtual teaching has the most potential to enhance urological medical education. However, we should also consider the difficulties associated with the implementation of these approaches; addressing these challenges should be the primary focus in the coming years.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Miah S, Mangera A, Venugopal S, Luk A, McDermid R, Rosario D. The clinical need for undergraduate urology. Clin Teach. 2015;12(5):353–355. doi:10.1111/tct.12298
2. Shah J, Billington R, Manson J, Vale J. Undergraduate urology: a survey of current provisions and guidelines for a core curriculum. BJU Int. 2002;89(4):327–330. doi:10.1046/j.1464-4096.2001.01534.x
3. Nicholson LL, Reed D, Chan C. An interactive, multi-modal Anatomy workshop improves academic performance in the health sciences: a cohort study. BMC Med Educ. 2016;16:7. doi:10.1186/s12909-016-0541-4
4. Medico-legal EH. Litigation and its Links with Surgical Anatomy. Surgery. 2002;20(8):i–ii. doi:10.1383/surg.20.8.0.14518
5. Matsumoto ED, Hamstra SJ, Radomski SB, Cusimano MD. The effect of bench model fidelity on endourological skills: a randomized controlled study. J Urol. 2002;167(3):1243–1247. doi:10.1016/S0022-5347(05)65274-3
6. Rock BG, Leonard AP, Freeman SJ. A training simulator for ultrasound-guided percutaneous nephrostomy insertion. Br J Radiol. 2010;83(991):612–614. doi:10.1259/bjr/42026587
7. Chen S, Zhu J, Cheng C, et al. Can virtual reality improve traditional anatomy education programmes? A mixed-methods study on the use of a 3D skull model. BMC Med Educ. 2020;20(1):395. doi:10.1186/s12909-020-02255-6
8. Stuart J, Rutherford RJ. Medical student concentration during lectures. Lancet. 1978;2(8088):514–516. doi:10.1016/S0140-6736(78)92233-X
9. Tregonning AM, Doherty DA, Hornbuckle J, Dickinson JE. The audience response system and knowledge gain: a prospective study. Med Teach. 2012;34(4):e269–74. doi:10.3109/0142159X.2012.660218
10. Tune JD, Sturek M, Basile DP. Flipped classroom model improves graduate student performance in cardiovascular, respiratory, and renal physiology. Adv Physiol Educ. 2013;37(4):316–320. doi:10.1152/advan.00091.2013
11. Morgan H, McLean K, Chapman C, Fitzgerald J, Yousuf A, Hammoud M. The flipped classroom for medical students. Clin Teach. 2015;12(3):155–160. doi:10.1111/tct.12328
12. Schneider A-T, Albers P, Müller-Mattheis V. E-Learning in Urology: implementation of the Learning and Teaching Platform CASUS® - Do Virtual Patients Lead to Improved Learning Outcomes? A Randomized Study among Students. Urol Int. 2015;94(4):412–418. doi:10.1159/000368653
13. Manalo TA, Higgins MI, Pettitt-Schieber B, Pettitt BJ, Mehta A, Hartsell LM. A Strategy for Undergraduate Medical Education in Urology During the COVID-19 Pandemic. J Surg Educ. 2021;78(3):746–750. doi:10.1016/j.jsurg.2020.09.011
14. Medical School overhauls curriculum with major redesign | news | the harvard crimson. Available from: https://www.thecrimson.com/article/2015/9/2/hms-curriculum-major-revamp/.
15. Ravishankar J, Epps J, Ambikairajah E. A flipped mode teaching approach for large and advanced electrical engineering courses. Eur J Eng Educ. 2018;43(3):413–426. doi:10.1080/03043797.2017.1383974
16. Ng A, Chan VW-S, Asif A, et al. LEARN: a multi-centre, cross-sectional evaluation of Urology teaching in UK medical schools. BJU Int. 2022. doi:10.1111/bju.15758
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.