")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Hospital Characteristics Associated with Certified EHR Adoption among US Psychiatric Hospitals
Authors Hu X, Qu H , Houser SH, Chen H, Zhou J, Yu M
Received 9 December 2019
Accepted for publication 14 March 2020
Published 2 April 2020 Volume 2020:13 Pages 295—301
DOI https://doi.org/10.2147/RMHP.S241553
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Xuejun Hu, 1, 2 Haiyan Qu, 2 Shannon H Houser, 2 Huoliang Chen, 1 Jinming Zhou, 1 Min Yu 3
1Department of Health Services Administration, Air Force Medical University, Xi’an, People’s Republic of China; 2Department of Health Services Administration, University of Alabama at Birmingham, Birmingham, AL, USA; 3Department of Health Services Administration, Academy of Military Medical Sciences, Beijing, People’s Republic of China
Correspondence: Min Yu
27 Taiping Road, Beijing 100850
Tel +86 10 6693 1042
Email [email protected]
Objective: The aim of this study was to explore the relationship between hospital characteristics and certified electronic health record (EHR) adoption in psychiatric hospitals in the US.
Methods: Data were drawn from the American Hospital Association Annual Survey Database and the Centers for Medicare and Medicaid Services Hospital Compare data sets in 2016. Binary logistic regression analysis and χ 2 tests were performed to examine the relationship between certified EHR adoption and hospital characteristics.
Results: Of 1,059 psychiatric hospitals in the US, 502 (47.4%) have adopted certified EHR technology. Large hospitals (OR 2.29, 95% CI 1.52– 3.44; p< 0.001), not-for-profit hospitals (OR 1.74, 95% CI 1.22– 2.49; p=0.008), and hospitals participating in a network (OR 1.78, 95% CI 1.34– 2.37; p< 0.001) were more likely to adopt certified EHRs. Hospitals in the northeast were less likely to implement certified EHRs compared to other regions. However, there was no significant association found between EHR utilization and system affiliation, urban location, teaching status, or participation of health-maintenance organizations and preferred provider organizations.
Conclusion: The study results suggested variations in EHR adoption according to hospital location, size, ownership, and network participation. This study fills a gap in previous work on certified EHR adoption that focused exclusively on general hospitals, but overlooked psychiatric hospitals. Future policies designed to influence the implementation of certified EHRs should take into consideration how hospital size, ownership, and network-affiliation status affect certified EHR adoption among psychiatric hospitals.
Keywords: hospital characteristics, electronic health records, health information technology, psychiatric hospitals
Introduction
Unprecedented progress has been made in the utilization of certified electronic health records (EHRs) in US health settings, especially since the implementation of EHR incentive programs authorized by the Health Information Technology for Economic and Clinical Health Act in 2009,1 which have demonstrated substantial influences on the health industry.2–4 According to published studies, positive impacts of EHR utilization can be found on therapeutic communications,5,6 hospital readmission,7 adverse drug events,8 and psychiatrist–patient relationships,9–11 as well as other quality measures12–14 based on psychiatric patient or practitioner level. Despite these significant benefits, psychiatric hospitals are still ineligible for the financial incentive programs, and see much lower rates of EHR adoption15,16 than other hospitals. In 2015, only 15% of psychiatric hospitals adopted at least a basic EHR system produced by different vendors, while >80%of general hospitals did.17 Lag in certified EHR adoption among psychiatric hospitals might not only limit quality improvement of psychiatric care but also stymie efforts to achieve targeted benefits, such as interoperability, across the health-care continuum.16,18 It is thus crucial to explore the reasons for less adoption of certified EHRs among psychiatric hospitals.
A body of studies have addressed concerns about factors associated with the adoption of EHRs among general hospitals, nursing homes,19,20 office settings,21 cancer hospitals,22 critical-access hospitals,23 obstetrician/gynecologists,24 and ophthalmologists.25 Commonly included factors are initial cost of implementing a system,19,20,23,26–31 maintenance/ongoing costs,19,27,30,32 financial incentives,20,23,24,33 technical support,19,20,23,26,28,30 privacy concerns,19,21 perception of hospital staff,24,28,31–34 and workload/workflow change.20,23,24,26,30,33 Factors concerning facility characteristics have also been mentioned, such as practice setting,35 teaching status,36 system affiliation,37–39 location,22,35,36,40,41 ownership,39 and hospital size.30,37,39,40
However, psychiatric hospitals have not yet been specifically examined. Furthermore, due to the stress on confidentiality of psychiatric records and the special reliance on information for psychiatric diagnosis and treatment, the findings of previous works in nonpsychiatric hospitals may not apply equally to psychiatric hospitals.11,42 Exploring the relationship between hospital characteristics and certified EHR adoption in psychiatric hospitals may be helpful inbetter understanding factors that facilitate or impede certified EHR adoption, which hopefully will have positive influences on future policies of certified EHR adoption among psychiatric facilities. The purpose of this study was to examine the association between hospital characteristics and adoption of EHRs in psychiatric hospitals.
Methods
Data Sources
This study was a cross-sectional, secondary analysis based on data from two open and freely available primary databases: the American Hospital Association Annual Survey Database and the Centers for Medicare and Medicaid Services Hospital Compare data sets. The Annual Survey Database provided hospital characteristics information for 6,251 hospitals, including teaching status, bed numbers, location, ownership, and system affiliation. The Hospital Compare datasets provided data for 1,655 psychiatric hospitals on the adoption of certified EHRs from the Inpatient Psychiatric Facility Quality Reporting (IPFQR) program in 2016. Using Medicare identification numbers, data from those two sources were merged into one data set, and 596 hospitals were excluded because of missing data. The current study included 1,059 psychiatric hospitals. Because the information was anonymous and no personal information collected, this study was exempt from requirement for institutional review board approval.
Certified EHR Adoption and Cohorts
In the IPFQR program, there was a structural measure evaluating the degree to which hospitals adopted certified EHRs in health services. Hospitals were required to attest to one of three statements that best represented their highest level of adoption of EHRs: certified EHR technology is employed most commonly to exchange health information at times of transitions in care, uncertified EHR technology is used most commonly to transfer health information at times of transitions in care, and paper or other form (eg, email) is the most common approach to conduct information exchange not involving the transfer of health information using EHR technology at times of transitions in care. Two groups were categorized to these hospitals based on their EHR-adoption status. Psychiatric hospitals choosing the first statement were defined as hospitals with certified EHRs, whereas those responding with “uncertified EHRs” or “paper or other form” were categorized as hospitals with uncertified EHRs.
Hospital Characteristics
Hospitals were classified based on their bed numbers (small, <200 beds; medium, 200–400 beds; large, ≥400 beds), system affiliation (no/yes), teaching status (nonteaching/teaching), location (urban/rural), and region (northeast, south, west, midwest). Hospital ownership was classified as government, non-government, nonprofit, or for profit. Additional factors used for this study were network-affiliation status (no/yes), health-maintenance organization (HMO) participation (no/yes), and preferred provider organization (PPO) participation (no/yes). "Network" here refers to a group of hospitals, physicians, other providers, insurers, and/or community agencies that voluntarily work together to coordinate and deliver health services. Participation of HMOs/PPOs means having a formal written contract with an HMO or PPO.
Data Analysis
Descriptive statistics were derived for hospital characteristics to report frequencies and percentages for each categorical variable, and χ2-tests were employed to examine bivariate associations between certified EHR-adoption and hospital characteristics among psychiatric hospitals. Correlation analyses (Pearson’s R) were derived among EHR-adoption and hospital characteristics. To determine independent associations, binary logistic regression analysis was conducted. All p-values were two-tailed and p<0.05 considered statistically significant. Data analyses were conducted using SPSSversion 24.0.
Results
Hospital characteristics, represented by certified EHR-adoption status, are summarized in Table 1. Of the 1,059 psychiatric hospitals in the US included, 502 (47.4%) had adopted certified EHR technology. The majority of these hospitals were system-affiliated (66.4%) and located in rural areas (78.9%). Slightly more than half were non-government and nonprofit entities (57.6%) and 57.5% teaching hospitals. In addition, hospitals with <200 beds accounted for 48.5%.
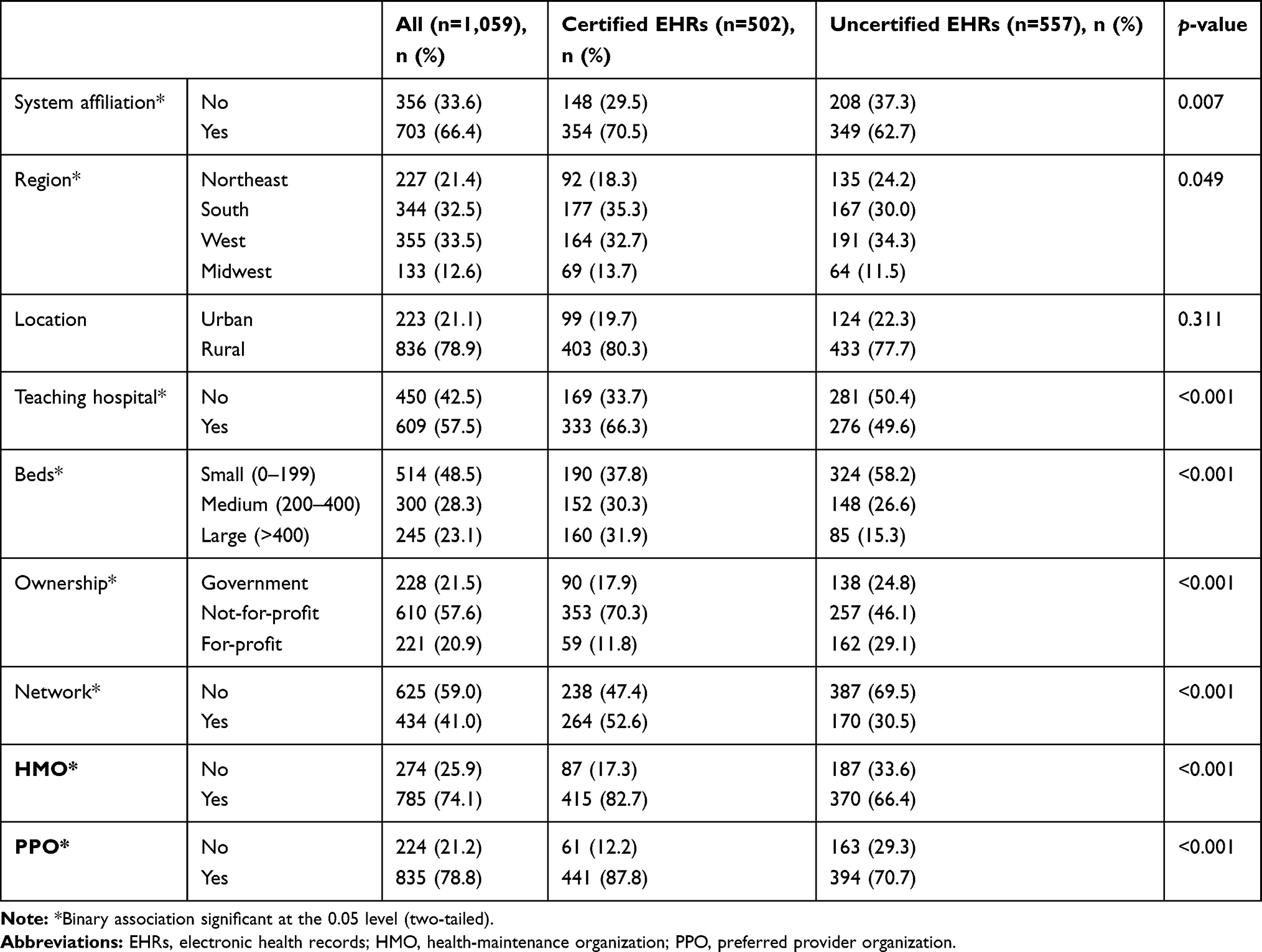 |
Table 1 Psychiatric hospital characteristics (n=1,059) |
On univariate analysis, psychiatric hospitals with certified EHRs were more likely to be larger (62.2% vs 41.8%, p<0.001), system-affiliated (70.5% vs 62.7%, p=0.007), not-for-profit (70.3% vs 46.1%, p<0.001), and teaching hospitals (66.3% vs 49.6%, p<0.001) than those with uncertified EHRs. Moreover, compared to hospitals not using certified EHRs, those using certified EHRs were also more likely to be a member of a network (52.6% vs 30.5%, p<0.001), HMO (82.7% vs 66.4%, p<0.001), and PPO (87.8% vs 70.7%, p<0.001). Furthermore, there was an association between hospital region and certified EHR adoption, while no significant relationship was found between urban/rural location and certified EHR utilization. In addition, results from Pearson's correlation analysis showed there was an association between certified EHR implementation and most of the aforementioned variables, excluding urban location and region (Appendix 1).
Binary logistic regression was conducted to explore independent associations between hospital characteristics and certified EHR adoption (Table 2). The logistic regression model was statistically significant (χ2=175.71, p<0.001) and explained 20.4% (Nagelkerke R2) of the variation in the outcome variable. Four variables in this model were significant at the p<0.05 level. Consistently with results from univariate analysis, large hospitals (OR 2.29, 95% CI 1.52–3.44; p<0.001), not-for-profit hospitals (OR 1.74, 95% CI 1.22–2.49; p=0.008), and thoseaffiliated with a network (OR 1.78, 95% CI 1.34–2.37; p<0.001) were more likely to adopt certified EHRs. Hospitals in the Northeast region were less likely to implement certified EHRs compared to the midwest (OR 1.96, 95% CI 1.35–2.84; p<0.001), south (OR 2.49, 95% CI 1.67–3.72; p<0.001), or west (OR 2.88, 95% CI 1.77–4.66; p<0.001). However, no significant association was found between certified EHR utilization and system affiliation, urban location, teaching status, and participation in HMOs/PPOs.
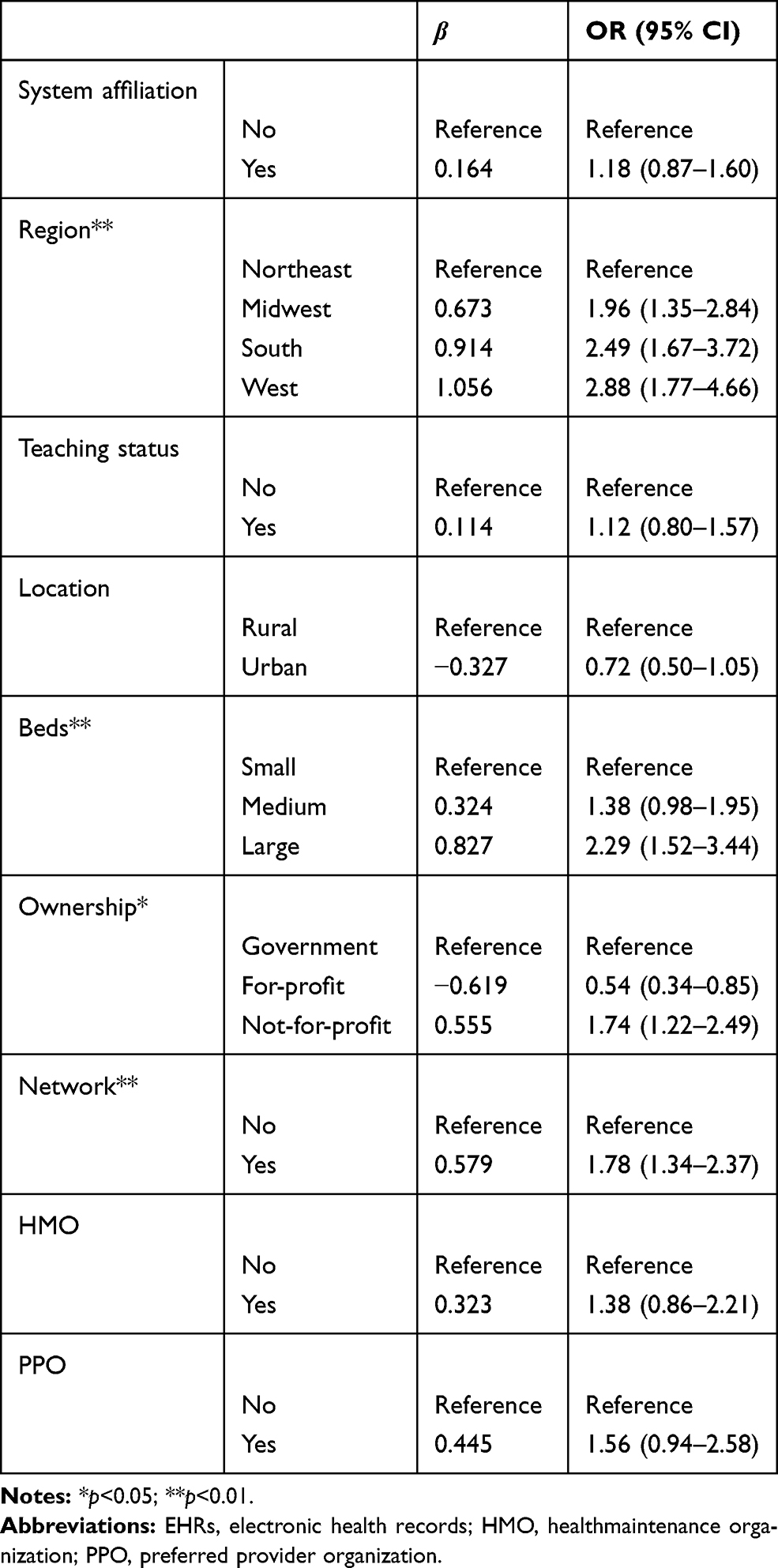 |
Table 2 Multivariate associations between certified EHR adoption and hospital characteristics among psychiatric hospitals (n=1,059) |
Discussion
Despite the large number of studies demonstrating how environmental factors influence adoption of certified EHRs among general hospitals, no study has specifically examined the impact ofhospital characteristics on certified EHR utilization in psychiatric hospitals. This study focused on psychiatric hospitals, with their special structures and unique challenges, and the results added specific understanding of the relationship between hospital characteristics and certified EHR implementation. The overall findings of this study showed that hospital characteristics played an important role in certified EHR adoption for psychiatric facilities, which echoes previous studies among general hospitals. Hospital characteristics, including region of hospital, bed numbers, ownership, and network participation, were significant predictors of certified EHR adoption. These findings have practical implications for policy-makers and hospital administrators who are tasked with strategy development for certified EHR adoption in psychiatric settings.
First, our findings suggest that the relationship of a hospital with a health network/system is associated with the adoption of certified EHRs in psychiatric hospitals. Specifically, psychiatric hospitals without involvement in a health network were less likely to use certified EHRs. Independent hospitals that have not formed a coalition or joined a health system may not have access to the benefits of economies of scale. As a multientity network/system, EHR networks can increase the value of individual EHR investment by minimizing infrastructure redundancy, employing bargaining power, and drawing upon operational and technical efficiencies.43
Second, hospital bed numbers were also found to be a predictor of certified EHR adoption, confirming prior findings.39,40 Large hospitals were more likely to implement certified EHRs, which require significant investment in hardware and software. Small hospitals are more challenged in terms of financial or human resources available to set up or run certified EHRs, which is consistent with prior findings that cost is a great barrier to certified EHR implementation.31,36,40 Requirements for providing quality of care, supporting routine operations, and renovating facilities may be much more pressing than investment in certified EHRs. On the contrary, large, revenue-rich hospitals with have the flexible capital to purchase EHRs. Therefore, it may be more challenging to promote the meaningful use of EHRs in small psychiatric facilities.
Third, the empirical findings of this study show that not-for-profit psychiatric hospitals were more likely to use EHRs than for-profit ones. Psychiatric hospitals that are ineligible for Health Information for Technological and Clinical Health incentives face the challenge of initial investment to implement certified EHRs. As costs of providing care are steadily increasing, additional investments in certified EHRs may not be a priority among for-profit hospitals. It might also be possible that for-profit psychiatric hospitals have calculated that the implementation cost of certified EHRs exceeds their potential benefits. Policy-makers should draw attention to and address hospitals’ concerns for return on investment, especially for for-profit psychiatric hospitals.
Moreover, this study suggests that certified EHR adoption in psychiatric hospitals was related to geographic location, which potentially indicates that market-level factors may influence psychiatric hospitals' decisions on adoption of health-information technology. Those factors include market competition,22,41,44 number of ophthalmologists per capita,41 managed care penetration,22,41 HMO penetration,45 munificence (availability of critical resources in the environment),44–46 population >65 years of age,22 and unemployment and poverty rates.44–46 Further studies are needed to explore associations among these multiple factors, and specifically on how geographic factors influence adoption of certified EHRs among psychiatric hospitals. Additionally, in the regression model, even though teaching status, system affiliation, and urban location were not significant predictors of certified EHR adoption in psychiatric hospitals, they were included in the analysis as control variables to reduce the chance of confounding influencs on hospitals’ behavior. It appears that certified EHR adoption in psychiatric hospitals is not very responsive to urban location or teaching status, which is inconsistent with previous findings.47,48
This study has several limitations worth noting. Findings in this cross-sectional research design are unable to indicate causal associations and can only be interpreted as associations. Another limitation of this work is the approach to identify psychiatric hospitals that have adopted certified EHRs. EHRs from different vendors or manufacturers varied in features and functions. Even though the IPFQR program clearly defined a structural measure to evaluate the degree to which hospitals adopted certified EHRs in health services, the responses may contain reporting bias. In addition, cases with missing values for some variables were excluded from the model in the current study, which imposes a potential selection bias on the findings. With available data, comparison studies between general and psychiatric hospitals should be conducted to explore the particular effect of organizational factors on EHR adoption among psychiatric hospitals.
Conclusion
Hospital characteristics, such as regional location, bed numbers, ownership, and network participation, were associated with certified EHR adoption in psychiatric hospitals in the US. This research fills a gap in previous work focusing on general hospitals, but largely overlooking psychiatric hospitals. To inform these adoption decisions, this study provides evidence on hospital features that are associated with adoption of certified EHRs for psychiatric hospitals. Future policies targeting implementation of certified EHRs should take into consideration economies of scale and return on investment of psychiatric-facility network affiliation and ownership status. More efforts may be needed to promote small psychiatric hospitals to utilize EHRs. Further research is necessary to explore factors that influence certified EHR adoption among psychiatric hospitals, such as market-level environmental factors. In addition, studies applying conceptual and theoretical frameworks to explore such variables as interactions among technological, organizational, and environmental factors should be undertaken.
Acknowledgments
This work was supported by a scholarship from the China Scholarship Council (201703170149). We are also grateful to Dr. Christy Harris Lemark (Department of Health Services Administration, University of Alabama at Birmingham), who offered a precious chance to the authors to conduct this research in the Department of Health Services Administration.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval to the version to be published, and agree to be accountable for all aspects of the work. Dr. H Qu is the co-first author.
Disclosure
The authors report no competing interests associated with this study.
References
1. Centers For Medicare Medicaid HHS. Medicare and medicaid programs; electronic health record incentive program–stage 3 and modifications to meaningful use in 2015 through 2017. Final rules with comment period. Fed Regist. 2015;80(200):62761–62955.
2. Payne TH. The electronic health record as a catalyst for quality improvement in patient care. Heart. 2016;102(22):1782–1787. doi:10.1136/heartjnl-2015-308724
3. Jones SS, Rudin RS, Perry T, et al. Health information technology: an updated systematic review with a focus on meaningful use. Ann Intern Med. 2014;160(1):48–54. doi:10.7326/M13-1531
4. Bright TJ, Wong A, Dhurjati R, et al. Effect of clinical decision-support systems: a systematic review. Ann Intern Med. 2012;157(1):29–43. doi:10.7326/0003-4819-157-1-201207030-00450
5. Salomon RM, Blackford JU, Rosenbloom ST, et al. Openness of patients’ reporting with use of electronic records: psychiatric clinicians’ views. J Am Med Inform Assoc. 2010;17(1):54–60. doi:10.1197/jamia.M3341
6. Ser G, Robertson A, Sheikh A. A qualitative exploration of workarounds related to the implementation of national electronic health records in early adopter mental health hospitals. PLoS One. 2014;9(1):e77669. doi:10.1371/journal.pone.0077669
7. Rumshisky A, Ghassemi M, Naumann T, et al. Predicting early psychiatric readmission with natural language processing of narrative discharge summaries. Transl Psychiatry. 2016;6(10):e921. doi:10.1038/tp.2015.182
8. Iqbal E, Mallah R, Jackson RG, et al. Identification of adverse drug events from free text electronic patient records and information in a large mental health case register. PLoS One. 2015;10(8):e134208. doi:10.1371/journal.pone.0134208
9. Kaufman KR, Hyler SE. Problems with the electronic medical record in clinical psychiatry: a hidden cost. J Psychiatr Pract. 2005;11(3):200–204. doi:10.1097/00131746-200505000-00008
10. Krishna R. The impact of health information technology on the doctor-patient relationship in child and adolescent psychiatry. Child Adolesc Psychiatr Clin N Am. 2017;26(1):67–75. doi:10.1016/j.chc.2016.07.007
11. Stewart RF, Kroth PJ, Schuyler M, et al. Do electronic health records affect the patient-psychiatrist relationship? A before & after study of psychiatric outpatients. BMC Psychiatry. 2010;10(1):3. doi:10.1186/1471-244X-10-3
12. Boyer L, Renaud MH, Baumstarck-Barrau K, et al. Establishment of an electronic medical record in a psychiatric hospital: evolution of professionals’ perceptions. Encephale. 2010;36(3):236–241. doi:10.1016/j.encep.2009.05.004
13. Boyer L, Samuelian JC, Fieschi M, et al. Implementing electronic medical records in a psychiatric hospital: a qualitative study. Int J Psychiatry Clin Pract. 2010;14(3):223–227. doi:10.3109/13651501003717243
14. Riahi S, Fischler I, Stuckey MI, et al. The value of electronic medical record implementation in mental health care: a case study. JMIR Med Inform. 2017;5(1):e1. doi:10.2196/medinform.6512
15. Wolf L, Harvell J, Jha AK. Hospitals ineligible for federal meaningful-use incentives have dismally low rates of adoption of electronic health records. Health Aff. 2012;31(3):505–513. doi:10.1377/hlthaff.2011.0351
16. Walker D, Mora A, Demosthenidy MM, et al. Meaningful use of EHRs among hospitals ineligible for incentives lags behind that of other hospitals, 2009–13. Health Aff. 2016;35(3):495–501. doi:10.1377/hlthaff.2015.0924
17. Henry J, Pylypchuk Y, Searcy T, et al. Adoption of Electronic Health Record Systems Among U.S. Non-Federal Acute Care Hospitals: 2008–2015: ONC Data Brief, 35: 1–9[R]. Washington DC: Office of the National Coordinator for Health Information Technology; 2016.
18. West JC, Clarke DE, Duffy FF, et al. Are psychiatrists ready for health care reform? Findings from the study of psychiatric practice under health care reform. Psychiatr Serv. 2016;67(12):1292–1299. doi:10.1176/appi.ps.201500536
19. Abramson EL, McGinnis S, Moore J, et al. A statewide assessment of electronic health record adoption and health information exchange among nursing homes. Health Serv Res. 2014;49(1pt2):361–372. doi:10.1111/hesr.2014.49.issue-1pt2
20. Abramson EL, Edwards A, Silver M, et al. Trending health information technology adoption among New York nursing homes. Am J Manag Care. 2014;20(11 Spec No. 17):P53–P59.
21. Furukawa MF, King J, Patel V, et al. Despite substantial progress in EHR adoption, health information exchange and patient engagement remain low in office settings. Health Aff. 2014;33(9):1672–1679. doi:10.1377/hlthaff.2014.0445
22. Tarver WL, Menachemi N. Environmental market factors associated with electronic health record adoption among cancer hospitals. Health Care Manage Rev. 2018;43:303–314.
23. Gabriel MH, Jones EB, Samy L, et al. Progress and challenges: implementation and use of health information technology among critical-access hospitals. Health Aff. 2014;33(7):1262–1270. doi:10.1377/hlthaff.2014.0279
24. Raglan GB, Margolis B, Paulus RA, et al. Electronic health record adoption among obstetrician/gynecologists in the united states: physician practices and satisfaction. J Healthc Qual. 2017;39(3):144–152. doi:10.1111/jhq.12072
25. Lim MC, Boland MV, McCannel CA, et al. Adoption of electronic health records and perceptions of financial and clinical outcomes among ophthalmologists in the United States. JAMA Ophthalmol. 2018;136(2):164. doi:10.1001/jamaophthalmol.2017.5978
26. Wang T, Biedermann S. Adoption and utilization of electronic health record systems by long-term care facilities in Texas. Perspect Health Inf Manag. 2012;9:1g.
27. Adler-Milstein J, DesRoches CM, Furukawa MF, et al. More than half of US hospitals have at least a basic EHR, but stage 2 criteria remain challenging for most. Health Aff. 2014;33(9):1664–1671. doi:10.1377/hlthaff.2014.0453
28. Jamoom E, Hing E. Progress with electronic health record adoption among emergency and outpatient departments: United States, 2006–2011. NCHS Data Brief. 2015;187:1–8.
29. Harle CA, Huerta TR, Ford EW, et al. Overcoming challenges to achieving meaningful use: insights from hospitals that successfully received centers for medicare and medicaid services payments in 2011. J Am Med Inform Assoc. 2013;20(2):233–237. doi:10.1136/amiajnl-2012-001142
30. Vest JR, Yoon J, Bossak BH. Changes to the electronic health records market in light of health information technology certification and meaningful use. J Am Med Inform Assoc. 2013;20(2):227–232. doi:10.1136/amiajnl-2011-000769
31. Kruse CS, Mileski M, Alaytsev V, et al. Adoption factors associated with electronic health record among long-term care facilities: a systematic review. BMJ Open. 2015;5(1):e6615. doi:10.1136/bmjopen-2014-006615
32. Reganti KR, Kuruvella R, Syamala S, et al. An evaluation of EHR and the barriers to adoption by small medical practices[EB/OL]. Available from: http://robschumaker.com/publications/IJPHIM%20-%20An%20Evaluation%20of%20EHR%20and%20the%20Barriers%20to%20Adoption%20by%20Small%20Medical%20Practices.pdf.
33. Menon S, Singh H, Meyer AND, et al. Electronic health record-related safety concerns: A cross-sectional survey. J Healthcare Risk Manag. 2014;34(1):14–26. doi:10.1002/jhrm.v34.1
34. Ben-Zion R, Pliskin N, Fink L. Critical success factors for adoption of electronic health record systems: literature review and prescriptive analysis. Inf Syst Manag. 2014;31(4):296–312. doi:10.1080/10580530.2014.958024
35. Jones EB. Factors associated with electronic health record use among nurse practitioners in the United States. J Ambul Care Manage. 2017;40(1):48–58. doi:10.1097/JAC.0000000000000169
36. DesRoches CM, Worzala C, Joshi MS, et al. Small, nonteaching, and rural hospitals continue to be slow in adopting electronic health record systems. Health Aff. 2012;31(5):1092–1099. doi:10.1377/hlthaff.2012.0153
37. Hikmet N, Bhattacherjee A, Menachemi N, et al. The role of organizational factors in the adoption of healthcare information technology in Florida hospitals. Health Care Manag Sci. 2008;11(1):1–9. doi:10.1007/s10729-007-9036-5
38. Menachemi N, Burke D, Clawson A, et al. Information technologies in Florida’s rural hospitals: does system affiliation matter? J Rural Health. 2005;21(3):263–268. doi:10.1111/jrh.2005.21.issue-3
39. Wang BB, Wan TT, Burke DE, et al. Factors influencing health information system adoption in American hospitals. Health Care Manage Rev. 2005;30(1):44–51. doi:10.1097/00004010-200501000-00007
40. Kruse CS, Kothman K, Anerobi K, et al. Adoption factors of the electronic health record: a systematic review. JMIR Med Inform. 2016;4(2):e19. doi:10.2196/medinform.5525
41. Menachemi N, Shin DY, Ford EW, et al. Environmental factors and health information technology management strategy. Health Care Manage Rev. 2011;36(3):275–285. doi:10.1097/HMR.0b013e3182048e7e
42. Menachemi N, Powers TL, Brooks RG. Physician and practice characteristics associated with longitudinal increases in electronic health records adoption. J Healthc Manag. 2011;56(3):183–198. doi:10.1097/00115514-201105000-00007
43. Gesulga JM, Berjame A, Moquiala KS, et al. Barriers to electronic health record system implementation and information systems resources: a structured review. Procedia Comput Sci. 2017;124:544–551. doi:10.1016/j.procs.2017.12.188
44. Kazley AS, Ozcan YA. Organizational and environmental determinants of hospital EMR adoption: a national study. J Med Syst. 2007;31(5):375–384. doi:10.1007/s10916-007-9079-7
45. Menachemi N, Mazurenko O, Kazley AS, et al. Market factors and electronic medical record adoption in medical practices. Health Care Manage Rev. 2012;37(1):14–22. doi:10.1097/HMR.0b013e3182352562
46. Abdolrasulnia M, Menachemi N, Shewchuk RM, et al. Market effects on electronic health record adoption by physicians. Health Care Management Review. 2008;33(3):243–252. doi:10.1097/01.HMR.0000324904.19272.c2
47. Jones EB, Furukawa MF. Adoption and use of electronic health records among federally qualified health centers grew substantially during 2010–12. Health Aff (Millwood). 2014;33(7):1254–1261. doi:10.1377/hlthaff.2013.1274
48. Kruse CS, DeShazo J, Kim F, et al. Factors associated with adoption of health information technology: a conceptual model based on a systematic review. JMIR Med Inform. 2014;2(1):e9. doi:10.2196/medinform.3106
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.