")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Historical evolution of the concept of anorexia nervosa and relationships with orthorexia nervosa, autism, and obsessive-compulsive spectrum
Authors Dell'Osso L, Abelli M, Carpita B, Pini S, Castellini G, Carmassi C , Ricca V
Received 21 March 2016
Accepted for publication 13 April 2016
Published 7 July 2016 Volume 2016:12 Pages 1651—1660
DOI https://doi.org/10.2147/NDT.S108912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Liliana Dell’Osso,1 Marianna Abelli,1 Barbara Carpita,1 Stefano Pini,1 Giovanni Castellini,2 Claudia Carmassi,1 Valdo Ricca2
1Psychiatry Section, Department of Clinical and Experimental Medicine, University of Pisa, Pisa, 2Department of Neuroscience, Psychology, Drug Research and Child Health (NEUROFARBA), University of Florence, Florence, Italy
Abstract: Eating disorders have been defined as “characterized by persistence disturbance of eating or eating-related behavior that results in the altered consumption or absorption of food and that significantly impairs health or psychosocial functioning”. The psychopathology of eating disorders changed across time under the influence of environmental factors, determining the emergence of new phenotypes. Some of these conditions are still under investigation and are not clearly identified as independent diagnostic entities. In this review, the historic evolution of the eating disorder concept up to the recent Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, has been evaluated. We also examined literature supporting the inclusion of new emergent eating behaviors within the eating disorder spectrum, and their relationship with anorexia, autism, and obsessive–compulsive disorder. In particular, we focused on what is known about the symptoms, epidemiology, assessment, and diagnostic boundaries of a new problematic eating pattern called orthorexia nervosa that could be accepted as a new psychological syndrome, as emphasized by an increasing number of scientific articles in the last few years.
Keywords: anorexia nervosa, autism spectrum disorders, eating disorders spectrum, obsessive–compulsive spectrum, orthorexia nervosa, DSM-5
Introduction
Eating disorders have been defined as “characterized by persistence disturbance of eating or eating-related behavior that results in the altered consumption or absorption of food and that significantly impairs health or psychosocial functioning”.1
The last version of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5),1 places eating disorders in the “Feeding and Eating Disorders” chapter, featuring several modifications of DSM-IV-TR. These changes include the inclusion of three disorders – avoidant/restrictive food intake disorder (ARFID), rumination disorder, and pica – previously described in the “Feeding and Eating Disorder of Infancy or Early Childhood” chapter and subsequently removed with the aim to produce a single chapter for eating disorders in childhood and adulthood. It includes anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), ARFID, rumination disorder, pica, other specified feeding or eating disorder, and unspecified feeding or eating disorder.1 The modifications of the diagnostic criteria appearing in the DSM-5 are relatively few, although significant, and involve clarifications to language and adjustments to existing diagnoses.2 In AN, the amenorrhea criterion was removed, and in BN, the threshold frequency of binge episodes and compensatory behaviors were decreased as the two subtypes (purging type and non-purging type) were deleted. Moreover, the DSM-5 officially recognized BED as a formal diagnosis.1 In reviewing and revising these disorders, the DSM-5 Eating Disorders Work Group had two objectives: clarify the existing diagnostic criteria, and decrease the frequency with which individuals, presenting for eating disorder treatment, were assigned to the heterogeneous category residual category, other specified feeding or eating disorder (or, in DSM-IV, eating disorders not otherwise specified [EDNOS]), reassigning someone to a specific diagnosis. Le Grange et al,3 in a nationwide study in the US, reported that 80.97% of adolescents and 75.38% of adults with an eating disorder were classified as having EDNOS, making it the most common eating disorder diagnosis.
This “miscellaneous” category provides less clinical utility. Conversely, by using DSM-5 criteria, many of these individuals will be returned to a diagnosis with a greater clinical utility.
The National Comorbidity Survey Replication estimates the lifetime prevalence of AN, BN, and BED at 0.9%, 1.5%, and 3.5% in women and 0.3%, 0.5%, and 2.0% in men, respectively.4 The new criteria adopted in the last edition of the DSM included in the main diagnoses the majority of patients who were classified as EDNOS, maintaining this category as a residual condition. However, several data seem to indicate that the new DSM-5 criteria determine mainly quantitative changes, and some issues related to the DSM categorization of eating disorders were not solved with the new edition. For example, it is noteworthy that the majority of the diagnoses change across time and a considerable number of AN patients develop BN, and vice versa.5,6 The DSM categories can only represent a temporary condition that would eventually changes with time. Indeed, several psychopathological dimensions, such as body image disorder or emotion dysregulation, represent stable markers associated with eating disorders. In this regard, DSM-5 modifications seem to represent quantitative rather than qualitative changes to the previous criteria.7 Moreover, the relationship of eating disorder psychopathology with other conditions outside the DSM categories, such as obsessive–compulsive and autism spectrum, is still far from clarified.
Indeed, the psychopathology of eating disorders changes across time under the influence of environmental factors, determining the emergence of new phenotypes. These conditions are still less investigated and are not clearly identified in a diagnostic category.
In the light of these considerations, this review took into consideration the historic evolution of the eating disorder concept up to the last version of the DSM, to the latest proposal for a new conceptualization of the eating disorder spectrum, and the new emergent eating disorders and behaviors. In particular, we focused on what is known about the symptoms, epidemiology, assessment, and diagnostic boundaries of a new problematic eating pattern called orthorexia nervosa (ON) that could be accepted as a new psychological syndrome, as emphasized by an increasing number of scientific articles in the last few years.8–11
Before the DSM: historical perspective on self-starvation
Although the symptomatology of AN shows an evolution related to environmental factors across history, it is important not to consider it as a contemporary disorder (Table 1).
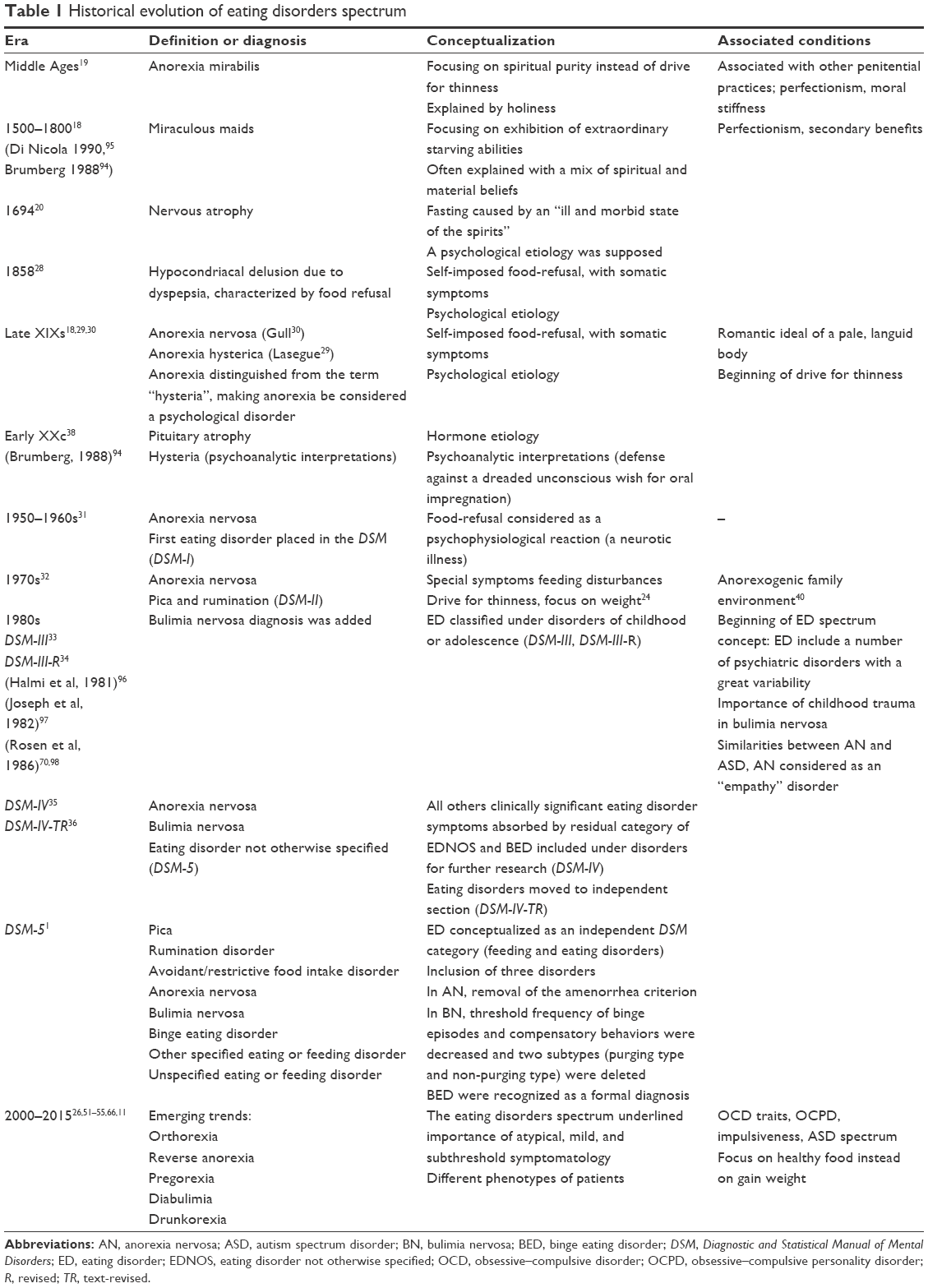 | Table 1 Historical evolution of eating disorders spectrum |
The first examples of self-starvation in Western countries have been reported as starting from the widespread diffusion of Gnostic philosophy and Christianity, both of which promoted a dichotomy between the evil, material world, and the holiness of souls.12 Christian hermits researched purification through self-starvation,13 and it seems that Saint Jerome professed the ascetic regime benefits to Roman women, to the extent that a Roman girl died of self-starvation following his precepts.12–14
During the Middle Age, and in particular from the 13th to the 16th century, it is possible to collect various evidence of extreme, self-induced fasting, often leading to premature death by starvation, such as Catherina from Siena.15 The characteristic sex difference was already evident, with fasting reported as a peculiar trait of feminine approach to medieval asceticism16 and female sainthood ideals were often related to self-sacrifice practices. Deprivation of food, except for the ritual of Eucharist, was an element of spirituality along with reclusion, self-flagellation, humble dressing, and other practices.17
A close relationship between inanition and spirituality in the Middle Age was described, although most of the cases of self-starvation were ascribed to demonic possessions.12,18 All fasting women were believed suspicious (even in the case of St Caterina) and only highborn charismatic ladies could convince men of the holy nature of their habits.15,18 Some authors named the common fasting habits reported in holy women as “holy anorexia” (also known as anorexia mirabilis).6,15,16,19 This condition differs from AN in focusing on spiritual purity instead of drive for thinness and overevaluation of body shape and body weight, and it is also associated with other penitential practices, as seen earlier.19
During the Renaissance period, religious context became less associated with extreme fasting, and new patterns of food deprivation appeared. Starving abilities were often explained with a mix of spiritual and material beliefs, but the trend toward medical explanations progressively increased, especially in the 18th century. In 1770, Morton published the seminal monography “Phthisiologia or a Treatise of Consumptions”, which described “nervous atrophy”, a condition of self-imposed reduction of food intake. The author stated that this kind of fasting was caused by an “ill and morbid state of the spirits”, supposing a psychological etiology.20
Finally, it is important to consider the evolution of the meaning of self-starvation during the last 3 centuries. Food restriction was progressively distanced from the religious connotation and was deeply interconnected with the body image self-representation. Indeed, since the mid-18th century, the ideal of feminine beauty slowly switched from a rounded figure to a slim and slender appearance. Industrialization led more women (in particular from lower classes) to work, and an ethereal and frail beauty became instead an upper-class statement, a demonstration of efficiency, prosperity, and “delicacy of mind”.21 An example was provided by the poet Lord Byron who promoted the new ideal of beauty as pale, languid body, anguished and surrounded by a melancholic aura.18,22 A similar ideal of feminine allure is also observable in pre-Raphaelites art, popular in the 19th century.18,22,23 In this framework, the case of the Empress Elizabeth of Austria, also known as Sissy, who followed strict diets and practiced strenuous physical activity, is remarkable. With her tall and very thin figure, during the second half of the 19th century, she embodied the modern ideal of beauty, based upon thinness, which progressively gained popularity until the 20th century.18
The ideal body shape for woman changes over time to suit the cultural and social norms. At one time, women were expected to aspire to a curvaceous, ample figure. Over the past 30 years, ideal body image has become progressively thinner. The ever-growing fitness industry has carried the popular misconception that health equals thinness. Miller and Pumariega,24 from a sociological perspective, ascribed these changes in eating disorders to the increasingly globalized, interconnected world that exposes more people to the societal pressures common to the Western culture emphasizing female body image and thinness. Moreover, foreign exchange programs and immigration can also predispose individuals, especially adolescents and young adults, to an eating disorder that contains features of the native culture blended with this pressure to conform. Authors considered the example of the Middle East, where vomiting rather than restriction were more frequent symptoms of AN, likely reflecting cultural values or traditions that make the act of vomiting more feasibly acceptable than restriction.24 To date, in the Western world, the sharp contrast between the wide availability of cheap, calorific, and highly palatable foods and the excessive value placed on slimness and dietary restraint, along with the daily bombardment with images of emaciated supermodels and other media images of thin role models, has meant that weight and shape concerns and dieting are the norm among young women.25 The recent increase of eating disorders may reflect a true increase in the incidence of these disorders, greater recognition by clinicians, and enhanced awareness of sufferers as a result of mass-media coverage.26
From sporadic observations to nosography
The evolution of the empirical method and positivism led to new approaches in the field of medicine, psychiatry, and in particular also in the way eating disorders were conceptualized. For example, the first complete pathological nosography was proposed by Erasmus Darwin in 1794. Later, Darwin categorized a voluntary fasting practice that would eventually lead to death, caused in young women by the obsessive idea of being too fat.27 The French physician Luis Victor Marcé – author of “Traité de la Folie des Femmes Enceintes, des Nouvelles Accouchées et de Nourices”, published in 1858, and of “Traité Pratique des maladies Mentales” published in 1862 – wrote a paper in 1860 that could be recognized as one of the first attempts to describe, from a proper psychiatric point of view, the nosography of what is currently defined as AN.28 In this work, he reported two clinical cases, outlining the delusional beliefs which led to food-refusal. In the second half of the 19th century, food-refusal was progressively described from a clinical point of view.
Lasegue29 and Gull30 presented a complete medical description of anorexia, considered the first true clinical recognition of the disorder. Gull coined the term “anorexia nervosa” to distinguish the disorder from the term “hysteria”, resulting in anorexia being considered a psychological disorder. After its acceptance as a psychogenic disorder in the late 1800s, AN was the first eating disorder placed in the Diagnostic and Statistical Manual of Mental Disorder (DSM) in its first edition (DSM-I),31 being considered a psychophysiological reaction (a neurotic illness). The second publication of the DSM-II,32 placed AN under special symptoms feeding disturbances, which also included pica and rumination. Later on, in the DSM-III33 and in its revised version (DSM-III-R),34 eating disorders were classified under disorders of childhood or adolescence, perhaps in part, contributing to previous underdiagnosis of later-onset cases. The American Psychiatric Association (APA) created two specific categories that formally recognized the diagnosis of eating disorders: AN and binge eating (called bulimia in DSM-III and BN in DSM-III-R and DSM-IV).34,35 In the DSM-IV, all other clinically significant eating disorder symptoms were absorbed by the residual categories of EDNOS and BED, included under disorders for further research. Subsequently, in the DSM-IV-TR, eating disorders moved to an independent section.36
The DSM-5 chapter for eating disorder – in addition to pica, AN, BN, BED, and ARFID – provides a section named “other specified feeding or eating disorder”, in which are included some other peculiar pathological eating patterns, like atypical AN (all other criteria for AN are met, but weight is in the normal range), and BN or BED with lower episode frequency and/or lasting <3 months. This section includes purging disorder (recurrent purging behavior to influence weight or shape, without binge eating) and night eating syndrome, characterized by recurrent episodes of night eating, as manifested by eating after awakening from sleep or excessive food consumption after the evening meal.1
The evolution of etiological theories on AN
The first attempt to understand the causes of self-starvation encompasses biological as well as psychological interpretations. For example, some clinicians first hypothesized hormonal etiology,37 while others doubted a hormonal etiology. Indeed, Sheehan and Summers38 documented significant clinical differences between anorexia and pituitary atrophy and proposed a psychological etiology. On a different perspective, according to a psychoanalytic interpretation, the refusal to eat should be considered as a manifestation of a defense against a dreaded unconscious wish for oral impregnation.39 During the 1960s and 1970s, a crucial role of family environment was postulated, and an “anorexogenic family” was associated with the development of AN.40 This model stressed the anorexic’s confusion between her own body and the internalized maternal “bad object”, and suggests that exercise and starvation could allow better control over the body itself.41 Bruch42 gained long-standing experience in treating patients with eating disorders and singled out the disturbed perception of the body as a significant feature of AN. The author describes the anorexic as lacking an autonomous sense of self and a continued obedience to parental figures, leading to an inability to master the psychological tasks of adolescence such as individuation and separation from the family. The anorexic turns to extreme control over her body because everything else in her life appears out of control. Thereafter, Palazzoli41,43 confirmed these theories adding the notion of lack of differentiation between one’s own body and the maternal object. Bemporad12 suggested that control over the body via starvation, exercise, and, at times, self-punishment, has provided a vehicle for psychopathology in females since the Middle Ages and that this form of behavior flourished in certain periods of history and receded in others. Those historical epochs in which females, in contemporary nonindustrialized, non-Westernized societies, have a role limited to nurturing and procreation, were dominated by its male citizens, and suffered economic hardship, do not seem to have experienced frequent episodes of female self-starvation. In contrast, those periods that offered substantial opportunities for women beyond a basic biological role, such as the Renaissance and late Victorian eras which were more egalitarian and more affluent, seemed to have witnessed spiraling rates of self-starvation. This finding is exemplified in some modern Muslim societies, and where, despite very high per capita income, females’ social roles continue to be determined by male dictates and eating disorders are not reported. Moreover, it should be underlined that not all the historical settings are equally favorable for the development of AN. As Palazzoli pointed out,43 lack of food and/or economic depression are inversely correlated with AN onset. This hypothesis could explain the observed reduction of self-starvation cases in the early Middle Ages or during the Second World War, and its gradual increase in step with the postwar economic recovery.43 With the advent of new biotechnologies (molecular biology, neuroimaging), the current scientific approach to the etiology of eating disorders is multifactorial, including sociocultural factors, underlying personality and behavioral traits, and neurobiological basis, in particular genetic factors and heritability. Social and cultural context could promote peculiar kinds of food intake management and control above others, also influencing the subjective and semantic aspects of pathological manifestations in patients with a genetic vulnerability to develop this disorder.19 As is the case for other psychiatric disorders, the psychopathology of eating disorders is thought to arise from the interplay of multiple risk and protective factors, despite the fact that the challenge for the future is to understand better the relative importance of neurobiological and psychosocial risk factors and how these elements interact.40
The conceptualization of the eating disorders spectrum
As previously reported, the new edition of the DSM represents a relevant step toward the nosography of eating disorders, including the majority of clinical phenotypes into the main diagnostic categories. However, patients who seek for a treatment represent only the tip of an iceberg, encompassing subthreshold conditions, as well as high-risk population according to a continuum of common psychopathological features. Moreover, other features typically associated with clinical presentation of eating disorders challenged the actual nosological system based on the categorical approach. For example, there is a substantial fluidity between diagnoses across time,5,44 and a relevant overlap with other psychiatric and medical conditions such as obsessive–compulsive disorder (OCD), obesity, and atypical manifestations. For this reason, researchers began focusing on attitudinal and behavioral traits rather than full syndromes.40 In line with this perspective, the “spectrum approach” may represent a valid tool to overcome the actual limitation of the eating disorder diagnoses.
The term “spectrum” has been used frequently in psychiatry to refer to putative etiologically related clinical features.45–47 Eating disorders spectrum involves core, atypical and subclinical symptoms and signs, temperament and personality traits, and behavioral patterns that, as a whole, represent a range of psychiatric symptomatology linked to eating disorders. Spectrum symptoms may develop as prodromes to a full-blown disorder, or occur as vulnerability factors for the development of a not-yet-fully expressed disorder, or as sequelae of a previous disorder.48,49 The eating disorders spectrum concept, as for the other psychiatric disorders, was created by clinical experience of the Pisa and Pittsburgh groups, with the aim of defining whether atypical, mild, and subthreshold symptomatology (usually considered soft and irrelevant), are effectively associated with a significant impact on everyday life with special regard to social impairment and to discriminate between different phenotypes of patients.26
Emerging trends in eating disorders and abnormal eating behaviors
The concept of a spectrum could represent a new instrument to better describe the complex pattern of the psychopathological features and behaviors of eating disorders, which have been recently found to be widespread across the general population, overcoming the boundaries of DSM categories. Indeed, new eating habits, with possible pathological implications, come to the observation of clinicians. For example, researchers identified a maladaptive behavior peculiar to males, among which eating disorders seem to be increasingly prevalent;50 “muscle dysmorphia”, also called “reverse anorexia” or “bigorexia”. This disorder is based on social pressure for males to be muscular and large. A possible lack of muscularity could be perceived as a malformation. Considering that this particular phenotype seems not to share the psychopathological core of eating disorders, Leone et al51 suggested that muscle dysmorphia should be eventually categorized as a subtype of body dysmorphic disorder. Another emerging phenomenon is “diabulimia”, which refers to people with type 1 diabetes intentionally avoiding taking insulin for the purpose of causing weight loss.52 In “drunkorexia”, the food intake is restricted before drinking alcohol: this behavior has been highlighted in particular among college students.53 An alarming restrictive eating pattern which can involve women during or after pregnancy is “pregorexia”. In this framework, women try to reduce caloric intake, or excessively intensify physical exercise due to the desire to avoid or control pregnancy weight gain.54
Although attention to food selection is not pathological itself, and considering the emphasis given by media on proper nutrition, the emergence of ON as a new eating behavior has been emphasized by an increasing public interest. This condition, defined as a “fixation on healthy food”, is characterized by highly sensitive cognitions and worries about healthy nutrition leading to such an accurate food selection that a correct diet becomes the most important part of life.55 The term “orthorexia nervosa”, derived from the Greek words orthos (correct) and orexis (appetite). Dunn and Bratman summarized in more detail the clinical picture of this condition in a recent review.56
Individuals with higher tendency to ON are primarily characterized by nutritional beliefs leading to a greater importance given to the perceived healthiness and nutritional properties rather than to taste and enjoyment of the foods.9,57 In some cases, there is a strict focus on biological nondairy vegetarianism, veganism, or raw food. The food quality, source, packaging, and processing are carefully checked daily, due to pervasive preoccupations with health-from-food and the desire to improve one’s own physical health and well-being. Apart from meals, a great amount of time is consumed by intrusive, food-related thoughts, with chronic worrying about food flaws and health threats, resulting in a severe distress or impairment of relationships, school, and work domains.10,58–60
As with the other conditions mentioned, ON is not formally present in DSM-5,1 neither in the section on disorders requiring more scientific research, nor in ICD-10.61 Considering the heterogeneity of features described earlier, it is still the object of debate whether ON can be considered a single, defined syndrome, a variance of other syndromes, or merely a behavioral and culturally influenced attitude.62,63 Moroze et al10 proposed four diagnostic criteria for ON, based on the review of literature,56,59,64 underscoring the fact that these criteria will have to be corroborated from validation studies along the lines of other DSM-5 diagnostic entities before they could be accepted into a future version of the DSM.
In particular, Moroze et al’s10 criterion B refers to impairment, caused by obsessional preoccupation of physical health due to an unbalanced diet and specify the severe distress or impairment of social, academic, or vocational functioning owing to obsessional thoughts and behaviors focusing on patient’s beliefs about “healthy eating”. As far as the diagnostic boundaries are concerned, it is of note that this condition shows similarities and differences with AN and OCD, which are themselves often comorbid.65,66 Even if ON and AN share abnormal eating attitudes and behaviors, and ON and AN patients both have a poor insight about the consequences of their disorders,67,68 the core beliefs of the two syndromes are different in nature.8,11 As a matter of fact, AN patients are mainly worried about body image, the quantity of food consumed, and gaining weight. In these individuals, the eating pattern is the consequence of the need to lose weight, and self-esteem depends on the weight lost. However, it is of note that severe orthorexic attitude toward food can be a risk factor to evolve to AN.67 On the other hand, considering OCD, both syndromes share high anxiety traits, a need to exert control, perfectionism, and concerns about contamination, whereas the most significant difference is the ego-syntonic content of obsessions characterizing individuals with higher tendency to ON with a limited insight.56
At present, using the DSM classification system, disordered eating driven by the need to follow an obsessively rigid diet designed to promote good health would likely be best classified as ARFID. Dunn and Bratman56 suggest that ON is a distinct condition from ARFID. In fact, individuals with a tendency to ON choose to restrict their intake because of a pathological drive to be as healthy as possible. However, limited epidemiological information regarding ON and some methodological problems in available studies (eg, small sample size, no data on representative community samples, assessment in high-risk groups) do not allow generalization of the results.9 The average prevalence rate of orthorexic symptoms has been found to be 6.9% for the general population and 35%–57.8% for high-risk groups (eg, dieticians, nutrition students, and other health care professionals including medical students, artists, fitness participants, and performance artists).9
To date, there are interesting hypotheses on the neurobiological, genetic, neuroanatomical, neurochemical, or psychophysiological correlates of the orthorexic condition.11
The theoretical overlap with anorexia and OCD, and maybe with autism spectrum disorders (ASDs), suggests that the neuropathophysiology of ASDs may represent the starting points for this kind of research. Neuropsychological studies corroborate these associations.
ASDs and eating disorders: an innovative hypothesis
In the light of the spectrum disorder approach, it is important to consider the relevant overlap between the clinical characteristics of specific AN phenotypes and some conditions included in ASDs. This diagnostic category included autistic disorder, Asperger’s disorder, and pervasive developmental disorder, according to the Neurodevelopmental Disorders Work Group position for the DSM-5.1 Symptoms of these disorders represent a single continuum of mild to severe disorders, and the triad of impairments spanning social interaction, communicative behavior, and repetitive and restricted behaviors, distinctive of DSM-5, was collapsed into two domains, preserving restricted and repetitive behaviors but converging social and communicative difficulties into a single domain.1
Research on the link between ASDs and eating disorders has evolved since conceptualization by Gillberg.69,70 The author identified some similarities between AN and ASD and proposed that AN should be conceptualized as an empathy disorder on the same spectrum as autism.69 This hypothesis was enlightened by longitudinal studies indicating that ASD, recently subsume by DSM-5 criteria under ASD, was overrepresented in the AN population.70 In other samples, 16% of teenagers with AN had a premorbid diagnosis of autism spectrum condition71 and 23% of adults with AN met the clinical criteria for autism spectrum condition.72,73
Tchanturia et al74 observed that in spite of differences in presentation, such as a later age of onset in AN, a biased sex ratio toward females in AN and on the contrary toward males with ASD, and higher than average intelligence quotient in AN vs more heterogeneous intelligence quotient levels for ASD, empirical studies from the last decade corroborated an overlap in behavioral and cognitive features between AN and ASD. Rigid attitudes and behaviors are typical features of AN, which can be seen as resembling the unusually narrow interests and rigid and repetitive behavior in ASD, albeit in AN these are focused on food or weight. Both ASD and AN show social anhedonia,74,75 deficits in emotional intelligence,76,77 difficulties on advanced theory of mind tests (such as the Reading the Mind in the Eyes test),78 rigidity on tests of set-shifting,79–82 excellent performance on tests of attention to detail, such as the Embedded Figures test,78 and alexithymia. Finally, these two disorders present atypical structure and function in “social brain” regions, including the superior temporal sulcus, fusiform face area, amygdala, and orbitofrontal cortex.83,84
For these reasons, Gillberg et al’s initial assumption has gathered evidence with reports of the possibility that autism and AN share common underlying cognitive and neural phenotypes.70,83,85,86
Currently, research confirms important point of symptom overlap between ON, AN, OCD, and obsessive–compulsive personality disorder (OCPD).87 In particular, the resemblance with AN is prompting debate as to whether ON is a unique disorder or a subset of AN or OCD. ON and AN share common traits of perfectionism, high traits of anxiety, and a high need to exert control, in addition to the potential for significant weight loss. Both have limited insight into their condition and often refuse the consequent functional impairments.
Concerning the relationship between ON and obsessive–compulsive spectrum disorders, there is some evidence that OCPD, rather than OCD, has a close link with eating disorders,66 in particular with AN.88 These similarities with ON include perfectionism, rigid thinking, and preoccupation with details and perceived rules. Anderluh et al89 have shown that the presence of OCPD traits positively predicts development of pathological eating habits.
In summary, we hypothesize that individuals with higher tendency to orthorexia symptoms could share some traits of both ASD and OCD; the obsession for proper nutrition, ritualized patterns of food preparation and eating, spending time in researching, cataloging and measuring food, planning future meals, and the presence of additional and intrusive food-related thoughts characterize this condition.87 Furthermore, these individuals are at risk for social isolation due to their stance of moral superiority and intolerance to others’ food beliefs. These disturbing features and behaviors could resemble deficits in social-emotional reciprocity, restricted and repetitive patterns of behavior and interests, inflexible adherence to routines, and the resulting impairment in social and occupational areas typical of patients with low levels of autistic spectrum.
On the other hand, eating problems are frequently present in subjects with ASDs: these atypical eating behaviors and habits occur in childhood, and food selectivity is the most frequent of these problems.90,91 The tendency to be overly selective or have an aversion to specific texture, colors, smells, and temperatures and to show rigidity to the brands of particular foods, endure up to adulthood associated with an increased risk for underweight.92,93 Further and prospective studies are needed to clarify shared features and boundaries between ON, eating spectrum disorders and ASD.
Conclusion
This review considered the historic evolution of the concept of AN up to the last version of the DSM, and described some relevant psychopathological data able to support a new conceptualization of the eating disorder spectrum.
The relationships between eating disorders, autism, and obsessive–compulsive spectrum seem to be of great interest in order to achieve a better understanding of different eating attitudes and behaviors, and deserve more effort in terms of large, accurate psychopathological investigations.
Acknowledgment
This work was supported by the Università di Pisa under the Progetto di Ricerca di Ateneo (Institutional Research Grants 2015) – Project no 12/2016.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric Association; 2013. | ||
Call C, Walsh BT, Attia E. From DSM-IV to DSM-5: changes to eating disorder diagnoses. Curr Opin Psychiatry. 2013;26(6):532–536. | ||
Le Grange D, Swanson SA, Crow SJ, Merikangas KR. Eating disorder not otherwise specified presentation in the US population. Int J Eat Disord. 2012;45(5):711–718. | ||
Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. 2007;61(3):348–358. | ||
Castellini G, Sauro CL, Mannucci E, et al. Diagnostic crossover and outcome predictors in eating disorders according to DSM-IV and DSM-V proposed criteria: a 6-year follow-up study. Psychosom Med. 2011;73(3):270–279. | ||
Milos G, Kuenzli C, Soelch CM, Schumacher S, Moergeli H, Mueller-Pfeiffer C. How much should I eat? Estimation of meal portions in anorexia nervosa. Appetite. 2013;63:42–47. | ||
Fairburn CG, Cooper Z, Shafran R, Wilson GT. Eating disorders: a transdiagnostic protocol. In: Barlow D, editor. Clinical Handbook of Psychological Disorders: A Step-by-step Treatment Manual. 4th ed. New York, NY: Guilford Press; 2008:578–614. | ||
Brytek-Matera A. Orthorexia nervosa – an eating disorder, obsessive-compulsive disorder or disturbed eating habit. Arch Psychiatr Psychother. 2012;1:55–60. | ||
Varga M, Dukay-Szabo S, Tury F, van Furth EF. Evidence and gaps in the literature on orthorexia nervosa. Eat Weight Disord. 2013;18(2):103–111. | ||
Moroze RM, Dunn TM, Craig Holland J, Yager J, Weintraub P. Microthinking about micronutrients: a case of transition from obsessions about healthy eating to near-fatal “orthorexia nervosa” and proposed diagnostic criteria. Psychosomatics. 2015;56(4):397–403. | ||
Koven NS, Abry AW. The clinical basis of orthorexia nervosa: emerging perspectives. Neuropsychiatr Dis Treat. 2015;11:385–394. | ||
Bemporad JR. Cultural and historical aspects of eating disorders. Theor Med. 1997;18(4):401–420. | ||
Fox RL. Pagans and Christians: Religion and the Religious Life from the Second to the Fourth Century AD, When the Gods of Olympus Lost Their Dominion and Christianity, with the Conversion of Constantine, Triumphed in the Mediterranean World. New York: Alfred A. Knopf, Inc.; 1987. | ||
Wallman C. Ascetism. In: Edwards P, editor. The Encyclopedia of Philosophy. Volume 1. New York: Macmillan; 1967:171–174. | ||
Bell RM. Holy Anorexia. Chicago: University of Chicago Press; 1985. | ||
Bynum CW. Holy Feast and Holy Fast. Berkeley: University of California Press; 1987. | ||
Bell RM, Weinstein D. Saints and Society: The Two Worlds of Western Christendom, 1000–1700. Chicago: University of Chicago Press; 1982. | ||
Vandereycken W, Van Deth R. From Fasting Saints to Anorexic Girls: The History of Self-starvation. New York: New York University Press; 1994. | ||
Harris JC. Anorexia nervosa and anorexia mirabilis: Miss K. R- and St Catherine of Siena. JAMA Psychiatr. 2014;71(11):1212–1213. | ||
Morton R. Phthisiologia – or a Treatise on Consumptions. London: Smith & Walford at the Prince’s Arms in St Paul’s Churchyard; 1694. | ||
Veblen T. The Theory of the Leisure Class: An Economic Study in the Evolution of Institutions. New York: American Library; 1899. | ||
Paterson W. Was Byron anorexic? World Med. 1982;15:35–38. | ||
English D, Ehrenreich B. For Her Own Good. New York: Anchor Press; 1978. | ||
Miller MN, Pumariega AJ. Culture and eating disorders: a historical and cross-cultural review. Psychiatry. 2001;64(2):93–110. | ||
British Medical Association. Eating Disorders, Body Image & The Media. London: British Medical Association; 2000. | ||
Mauri M, Borri C, Baldassari S, et al. Acceptability and psychometric properties of the Structured Clinical interview for Anorexic-Bulimic Spectrum (SCI-ABS). Int J Methods Psychiatr Res. 2000;9(2):68–78. | ||
Darwin E. Zoonomia; or, The Laws of Organic Life. Boston: Carlisle, D for Thomas and Andrews; 1803. | ||
Silverman JA. Louis-Victor Marcé, 1828–1864: anorexia nervosa’s forgotten man. Psychol Med. 1989;19(4):833–835. | ||
Lasegue C. On hysterical anorexia. Med Times Gazette. 1873;2(6):27. | ||
Gull WW. Anorexia nervosa. Trans Clin Soc Lond. 1874;7:22–28. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1952. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 2nd Edition. Washington, DC: American Psychiatric Association; 1968. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition. Washington, DC: American Psychiatric Association; 1980. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition, Revised. Washington, DC: American Psychiatric Association; 1987. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. Washington, DC: American Psychiatric Association; 1994. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Washington, DC: American Psychiatric Association; 2000. | ||
Simmonds M. Ueber Hypophysis-schwund mit tödlichem Ausgang. Deut Med Wochenschr. 1914;40(7):322–323. German. | ||
Sheehan HL, Summers VK. The syndrome of hypopituitarism. Q J Med. 1949;18(72):319–378. | ||
Thomae H. Some psychoanalytic observations on anorexia nervosa. Br J Med Psychol. 1963;36:239–248. | ||
Schmidt U. Aetiology of eating disorders in the 21(st) century: new answers to old questions. Eur Child Adolesc Psychiatry. 2003;12(Suppl 1):I30–I37. | ||
Palazzoli MS. L’anoressia mentale. Milan: Feltrinelli; 1963. | ||
Bruch H. Eating Disorders: Obesity, Anorexia Nervosa, and the Person Within. New York: Basic Books; 1973. | ||
Palazzoli MS. Anorexia nervosa: a syndrome of the affluent society. J Strat Syst Ther. 1985(22):199–205. | ||
Tozzi F, Thornton LM, Klump KL, et al. Symptom fluctuation in eating disorders: correlates of diagnostic crossover. Am J Psychiatry. 2005;162(4):732–740. | ||
Kety S, Rosenthal D, Wender D, Schulsinger F, Jacobsen B. The types and prevalence of mental illness in the biological and adoptives families of adopted schizophrenics. In: Rosenthal D, Kety S, editors. The Transmission of Schizofrenia. New York, NY: Pergamon Press; 1968:345–362. | ||
Akiskal HS. The bipolar spectrum: new concepts in classification and diagnosis. In: Grinspoon L, editor. Psychiatry Update: The American Psychiatric Association Annual Review. Volume 2. Washington, DC: American Psychiatric Press; 1983:271–292. | ||
Hollander E. Obsessive-compulsive spectrum disorders: an overview. Psychiatr Ann. 1993;23(7):355–358. | ||
Cassano GB, Michelini S, Shear MK, Coli E, Maser JD, Frank E. The panic-agoraphobic spectrum: a descriptive approach to the assessment and treatment of subtle symptoms. Am J Psychiatry. 1997;154(Suppl 6):27–38. | ||
Frank E, Cassano GB, Shear MK, et al. The spectrum model: a more coherent approach to the complexity of psychiatric symptomatology. CNS Spectrums. 1998;3(4):23–34. | ||
Hepworth K. Eating disorders today – not just a girl thing. J Christ Nurs. 2010;27(3):236–241; quiz 242–233. | ||
Leone JE, Sedory EJ, Gray KA. Recognition and treatment of muscle dysmorphia and related body image disorders. J Athl Train. 2005;40(4): 352–359. | ||
Davidson J. Diabulimia: how eating disorders can affect adolescents with diabetes. Nurs Stand. 2014;29(2):44–49. | ||
Roosen KM, Mills JS. Exploring the motives and mental health correlates of intentional food restriction prior to alcohol use in university students. J Health Psychol. 2015;20(6):875–886. | ||
Mathieu J. What is pregorexia? J Am Diet Assoc. 2009;109(6):976–979. | ||
Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C. Orthorexia nervosa: a preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat Weight Disord. 2004;9(2):151–157. | ||
Dunn TM, Bratman S. On orthorexia nervosa: a review of the literature and proposed diagnostic criteria. Eat Behav. 2015;21:11–17. | ||
Marazziti D, Presta S, Baroni S, Silvestri S, Dell’Osso L. Behavioral addictions: a novel challenge for psychopharmacology. CNS Spectr. 2014;19(6):486–495. | ||
Aarnio K, Lindeman M. Magical food and health beliefs: a portrait of believers and functions of the beliefs. Appetite. 2004;43(1):65–74. | ||
Mathieu J. What is orthorexia? J Am Diet Assoc. 2005;105(10):1510–1512. | ||
Aksoydan E, Camci N. Prevalence of orthorexia nervosa among Turkish performance artists. Eat Weight Disord. 2009;14(1):33–37. | ||
World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization; 1992. | ||
Bartrina JA. Ortorexia o la obsesión por la dieta saludable [Orthorexia or when a healthy diet becomes an obsession]. Arch Latinoam Nutr. 2007;57(4):313–315. Spanish. | ||
Vandereycken W. Media hype, diagnostic fad or genuine disorder? Professionals’ opinions about night eating syndrome, orthorexia, muscle dysmorphia, and emetophobia. Eating Disorders. 2011;19(2):145–155. | ||
Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C. Orthorexia nervosa: validation of a diagnosis questionnaire. Eat Weight Disord. 2005;10(2):e28–e32. | ||
Altman SE, Shankman SA. What is the association between obsessive-compulsive disorder and eating disorders? Clin Psychol Rev. 2009;29(7):638–646. | ||
Halmi KA, Tozzi F, Thornton LM, et al. The relation among perfectionism, obsessive-compulsive personality disorder and obsessive-compulsive disorder in individuals with eating disorders. Int J Eat Disord. 2005;38(4):371–374. | ||
Ramacciotti CE, Perrone P, Coli E, et al. Orthorexia nervosa in the general population: a preliminary screening using a self-administered questionnaire (ORTO-15). Eat Weight Disord. 2011;16(2):e127–e130. | ||
Alvarenga MS, Martins MC, Sato KS, Vargas SV, Philippi ST, Scagliusi FB. Orthorexia nervosa behavior in a sample of Brazilian dietitians assessed by the Portuguese version of ORTO-15. Eat Weight Disord. 2012;17(1):e29–e35. | ||
Chaki B, Pal S, Bandyopadhyay A. Exploring scientific legitimacy of orthorexia nervosa: a newly emerging eating disorder. J Hum Sport Exerc. 2013;8:1045–1053. | ||
Gillberg C. Are autism and anorexia nervosa related? Br J Psychiatry. 1983;142:428. | ||
Gillberg IC, Gillberg C, Rastam M, Johansson M. The cognitive profile of anorexia nervosa: a comparative study including a community-based sample. Compr Psychiatry. 1996;37(1):23–30. | ||
Rastam M. Anorexia nervosa in 51 Swedish adolescents: premorbid problems and comorbidity. J Am Acad Child Adolesc Psychiatry. 1992;31(5):819–829. | ||
Wentz E, Lacey JH, Waller G, Rastam M, Turk J, Gillberg C. Childhood onset neuropsychiatric disorders in adult eating disorder patients. A pilot study. Eur Child Adolesc Psychiatry. 2005;14(8):431–437. | ||
Tchanturia K, Smith E, Weineck F, et al. Exploring autistic traits in anorexia: a clinical study. Mol Autism. 2013;4(1):44. | ||
Tchanturia K, Davies H, Harrison A, Fox JR, Treasure J, Schmidt U. Altered social hedonic processing in eating disorders. Int J Eat Disord. 2012;45(8):962–969. | ||
Chevallier C, Grezes J, Molesworth C, Berthoz S, Happe F. Brief report: selective social anhedonia in high functioning autism. J Autism Dev Disord. 2012;42(7):1504–1509. | ||
Petrides K, Hudry K, Michalaria G, Swami V, Sevdalis N. A comparison of the trait emotional intelligence profiles of individuals with and without Asperger syndrome. Autism. 2011;15(6):671–682. | ||
Hambrook D, Brown G, Tchanturia K. Emotional intelligence in anorexia nervosa: is anxiety a missing piece of the puzzle? Psychiatry Res. 2012;200(1):12–19. | ||
Baron-Cohen S, Jaffa T, Davies S, Auyeung B, Allison C, Wheelwright S. Do girls with anorexia nervosa have elevated autistic traits? Mol Autism. 2013;4(1):24. | ||
Russell J. Autism as an Executive Disorder. Oxford: Oxford University Press; 1997. | ||
Holliday J, Tchanturia K, Landau S, Collier D, Treasure J. Is impaired set-shifting an endophenotype of anorexia nervosa? Am J Psychiatry. 2005;162(12):2269–2275. | ||
Takahashi M, Tanaka K, Miyaoka H. Reliability and validity of communication skills questionnaire (CSQ). Psychiatry Clin Neurosci. 2006;60(2):211–218. | ||
Gillberg IC, Rastam M, Wentz E, Gillberg C. Cognitive and executive functions in anorexia nervosa ten years after onset of eating disorder. J Clin Exp Neuropsychol. 2007;29(2):170–178. | ||
Zucker NL, Losh M, Bulik CM, LaBar KS, Piven J, Pelphrey KA. Anorexia nervosa and autism spectrum disorders: guided investigation of social cognitive endophenotypes. Psychol Bull. 2007;133(6):976–1006. | ||
Treasure JL. Getting beneath the phenotype of anorexia nervosa: the search for viable endophenotypes and genotypes. Can J Psychiatry. 2007;52(4):212–219. | ||
Krug I, Penelo E, Fernandez-Aranda F, et al. Low social interactions in eating disorder patients in childhood and adulthood: a multi-centre European case control study. J Health Psychol. 2013;18(1):26–37. | ||
Karlsson L, Rastam M, Wentz E. The Swedish Eating Assessment for Autism spectrum disorders (SWEAA) – validation of a self-report questionnaire targeting eating disturbances within the autism spectrum. Res Dev Disabil. 2013;34(7):2224–2233. | ||
Serpell L, Livingstone A, Neiderman M, Lask B. Anorexia nervosa: obsessive-compulsive disorder, obsessive-compulsive personality disorder, or neither? Clin Psychol Rev. 2002;22(5):647–669. | ||
Anderluh MB, Tchanturia K, Rabe-Hesketh S, Treasure J. Childhood obsessive-compulsive personality traits in adult women with eating disorders: defining a broader eating disorder phenotype. Am J Psychiatry. 2003;160(2):242–247. | ||
Beighley JS, Matson JL, Rieske RD, Adams HL. Food selectivity in children with and without an autism spectrum disorder: investigation of diagnosis and age. Res Dev Disabil. 2013;34(10):3497–3503. | ||
Postorino V, Sanges V, Giovagnoli G, et al. Clinical differences in children with autism spectrum disorder with and without food selectivity. Appetite. 2015;92:126–132. | ||
Sobanski E, Marcus A, Hennighausen K, Hebebrand J, Schmidt MH. Further evidence for a low body weight in male children and adolescents with Asperger’s disorder. Eur Child Adolesc Psychiatry. 1999;8(4):312–314. | ||
Bolte S, Ozkara N, Poustka F. Autism spectrum disorders and low body weight: is there really a systematic association? Int J Eat Disord. 2002;31(3):349–351. | ||
Brumberg JJ. Fasting Girls: The History of Anorexia Nervosa. New York: Penguin Books; 1988. | ||
Di Nicola VFC. Anorexia multiforms: self starvation in historical and cultural context. Transcult Psychiatr Res Rev. 1990;27(3–4):part I:165–196, part II:245–286. | ||
Halmi KA, Falk JR, Schwartz E. Binge eating and vomiting: a survey of a college population. Psycol Med. 1981;11(4):697–706. | ||
Joseph A, Wood IK, Goldberg SC. Determining population at risk for developing Anorexia Nervosa based on selection of college major. Psychiatr Res.1982;7(1):53–58. | ||
Rosen JC, Leitemberg H, Fisher C, Kasham C. Binge eating in bulimia nervosa: the amount and type of food consumed. Int J Eat Dis. 1986;5(2):255–267. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.