")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 14
Histopathological Pattern of Kidney Diseases Among HIV-Infected Treatment-Naïve Patients in Kano, Nigeria
Authors Abdu A, Atanda A , Bala SM, Ademola B, Nalado A , Obiagwu P, Duarte R , Naicker S
Received 29 January 2021
Accepted for publication 30 March 2021
Published 18 May 2021 Volume 2021:14 Pages 143—148
DOI https://doi.org/10.2147/IJNRD.S304341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Aliyu Abdu,1 Akinfenwa Atanda,2 Sunusi M Bala,3 Babatunde Ademola,1 Aishat Nalado,1 Patience Obiagwu,4 Raquel Duarte,5 Saraladevi Naicker5
1Nephrology Unit, Department of Medicine, Aminu Kano Teaching Hospital, Bayero University, Kano, Nigeria; 2Department of Histopathology, Aminu Kano Teaching Hospital, Bayero University, Kano, Nigeria; 3Department of Medicine, Muhammad Abdullahi Wase Teaching Hospital, Kano, Nigeria; 4Department of Paediatrics, Aminu Kano Teaching Hospital, Bayero University, Kano, Nigeria; 5Department of Medicine, University of Witwatersrand, Johannesburg, South Africa
Correspondence: Aliyu Abdu
Nephrology Unit, Department of Medicine, Aminu Kano Teaching Hospital, Bayero University, Kano, Nigeria
Email [email protected]
Introduction: Kidney biopsy in patients with HIV-associated kidney diseases allows for histopathologic diagnosis and institution of appropriate treatment as well as proper prognostication. There is a paucity of data on the histopathological pattern of HIV-associated kidney diseases in most sub-Saharan African countries. This study was aimed at evaluating the histopathologic patterns of kidney diseases seen among HIV-infected treatment-naive patients in our center as this will allow for proper diagnosis and institution of appropriate treatment.
Methods: In this cross-sectional study, consecutive patients who satisfied inclusion criteria and consented to participate were recruited. Percutaneous kidney biopsies were carried out as day procedures under real-time ultrasound guidance using an automatic spring-loaded biopsy gun as per our unit protocols. Baseline investigations including urea, creatinine, electrolytes, CD4 count, complete blood count, and glomerular filtration rate (eGFR) calculations, urinalysis and urine protein creatinine ratios were done on all the participants.
Results: Fifty-five patients who satisfied the inclusion criteria were studied. The mean age of the study population was 38.34± 9.26 years, with 32% females. Mean serum creatinine was 249.6± 164.6 μmol/L, and mean CD4 count was 238 ± 210 cells/mL. The commonest histological type was FSGS seen in 20 patients (37.7%), followed by HIVAN seen in 17 (32.1%) patients; chronic interstitial nephritis in 7 patients (13.2%) and 6 (11%) had no significant pathological finding. Compared to non-HIVAN, HIVAN patients tended to have higher systolic BP (p= 0.05); higher serum creatinine levels (p= 0.05); lower eGFR (0.03) and higher urine protein to creatinine ratio [uPCR; p= 0.02].
Conclusion: Kidney involvement is still a form of presentation among HIV-infected treatment-naïve patients and though a wide range of glomerular and tubulointerstitial lesions may be seen, FSGS and HIVAN are still the most common. We recommend assessment of kidney function, including urinalysis, as part of the routine evaluation of newly diagnosed HIV patients and biopsy where indicated to prognosticate and institute appropriate early treatment.
Keywords: HIV, kidney disease, histology
Introduction
Human Immunodeficiency Virus (HIV) infection remains a huge burden in sub-Saharan Africa; including Nigeria.1 Increase in numbers of HIV infection coupled with improved long-term survival has led to increasing prevalence of HIV-associated organ dysfunction, including kidney diseases.
Comorbidity of HIV with kidney disease has been associated with faster progression to AIDS and increased mortality. Mulenga et al2 in Lusaka, Zambia reported that anti-retroviral therapy (ART)-naïve adults living with both HIV and kidney disease had a 4-fold higher mortality rate than those without kidney disease. Reports on the prevalence of kidney disease among HIV-infected patients have varied across the globe. In a recent meta-analysis of studies on the prevalence of kidney disease among HIV patients the greatest burden was reported to be in the West African sub-region.3 Proteinuria, reduced glomerular filtration rate (GFR), or both, have been utilized to define kidney disease in most studies; however, definitive diagnosis by kidney biopsy, when indicated, is important among these patients and is critical to optimal management.4 A wide variety of histopathological lesions have been reported among HIV-infected patients, with the variation depending on many factors such as geographical and ethnic diversity of the population and type of study involved. Certain kidney diseases such as HIV-associated nephropathy (HIVAN) are exclusive to HIV-infected populations. This lesion has a higher prevalence among individuals of African descent and has been associated with an 18-fold higher relative risk of developing HIV-related end stage renal disease (ESRD) among African-Americans compared to Caucasians.5,6 Diagnosis of HIVAN is best made histologically and thus, kidney biopsy is important for instituting appropriate treatment and for prognostication.
Despite the strong association between certain histopathological lesions, such as HIVAN, and African ancestry there is paucity of literature detailing the spectrum of kidney morphologic changes of the disease in West Africa. This has been attributed to a scarcity of resources needed to perform or interpret a kidney biopsy on which the diagnosis of HIVAN or other HIV-related renal disease is based.7,8 This study aimed at having a histological diagnosis of HIV patients with kidney disease to help in instituting appropriate diagnosis and treatment.
Materials and Methods
This cross-sectional study was conducted at the dedicated HIV clinic of Aminu Kano Teaching Hospital (AKTH), one of the approved United States President’s Emergency Plan for AIDS Relief (PEPFAR) centers in Northern Nigeria. All the participants are Nigerians receiving treatment at this center. Ethical approval to conduct the study was granted by the Research Ethics Committee of AKTH (NHREC/21/08/AKTH/1090) and university of Witwatersrand Human Research Ethics Committee (M140116). All participants were aware of the purpose before giving their consent and the research was conducted in accordance with Helsinki Declaration. Consecutive patients who satisfied the inclusion criteria were recruited into the study and the criteria included:
- Treatment-naïve HIV positivity
- Persistent proteinuria and/or reduced eGFR
- Non-diabetic
- Not being treated for any kidney disease
- No contraindication to kidney biopsy and
- Consent to participate
Demographic variables including age, sex, ethnicity, history of kidney disease in the family and current use of medications were recorded using a questionnaire with specific identification numbers assigned to each participant.
A focused medical examination was conducted on all study participants and findings recorded included weight, height, body mass index (BMI) and systolic and diastolic blood pressures. Urinalysis was performed on mid-stream urine samples using Combi-9 urine Dipstick (Biotechnologies AG, Lichtenfels, Germany). All patients whose urine tested positive for protein were seen again after two weeks for a repeat of urinalysis to ascertain persistent proteinuria.
Venous blood samples were collected for baseline investigations including urea, creatinine, electrolytes, CD4 count, complete blood count, Hepatitis B surface antigen and Hepatitis C antibody. Glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation with no ethnicity factor used. Traceable Jaffe’s method was used to determine creatinine levels in both the blood and urine samples using Cobas C 311 Clinical Chemistry Analyser (Roche Diagnostics)
Percutaneous kidney biopsies were carried out as day procedures under real-time ultrasound guidance using an automatic spring-loaded biopsy gun (BARD 16/18 G, 22 mm cutting edge). Before the biopsy, patients were counseled on the procedure and had complete blood counts including platelets measured. Clotting profiles were also checked to exclude any bleeding tendencies and they were requested to sign a consent form. Patients were monitored both pre- and post-biopsy according to established unit protocols and were discharged after a minimum of 8 hours observation with no obvious complication.
Each biopsy specimen was fixed and transported in 10% neutral buffered formalin solution for analysis in the pathology laboratory of the hospital, where they were embedded in paraffin wax and stained with Haematoxylin and Eosin, Jones methenamine silver, Periodic Acid Schiff, Congo red and Masson’s trichrome stains. Light microscopy was performed on all the tissue samples; there were no facilities for immunofluorescence (IF) at the time when the study commenced. However, IF service became available before the end of the study and 10 of the tissue specimens were subjected to IF analysis. Electron microscopy is not available in our center hence it was not included in the evaluation of the renal tissues obtained in this study.
For the purpose of this study, we considered eGFR to be reduced at values less than 60 mls/min/1.73m2 and defined persistent proteinuria, as the presence of dipstick protein ≥ + 1 or a urine protein: creatinine ratio (uPCR) ≥ 150 mg/g on 2 occasions at least 2 weeks apart.
Data was analysed using SPSS version 24 and statistical significance was set at p-value >0.05 at 95% confidence interval.
Results
Fifty-five patients who satisfied the inclusion criteria were studied; however, complete data was available for only 53 patients. The mean age of the study population was 38.3± 9.3 years, with 32% females and 68% males. None of the patients had symptoms suggestive of kidney failure such as body swelling, nausea or vomiting. Mean serum creatinine was 249.6± 164.6 μmol/L; mean eGFR 40.0± 19.2, mean CD4 count was 238 ±210 cells/mL details as depicted in Table 1. Although all the patients had persistent proteinuria, only two had nephrotic range proteinuria at the time of review. All the tissue samples obtained had renal cortex with a number of glomeruli ranging between 9 and 26. None of the patients had a major bleeding complication that required blood transfusion or any invasive intervention following the kidney biopsy procedure. One patient had haematuria that lasted for more than 24 hours necessitating an overnight hospital stay, he was later discharged in a stable condition without requiring blood transfusion.
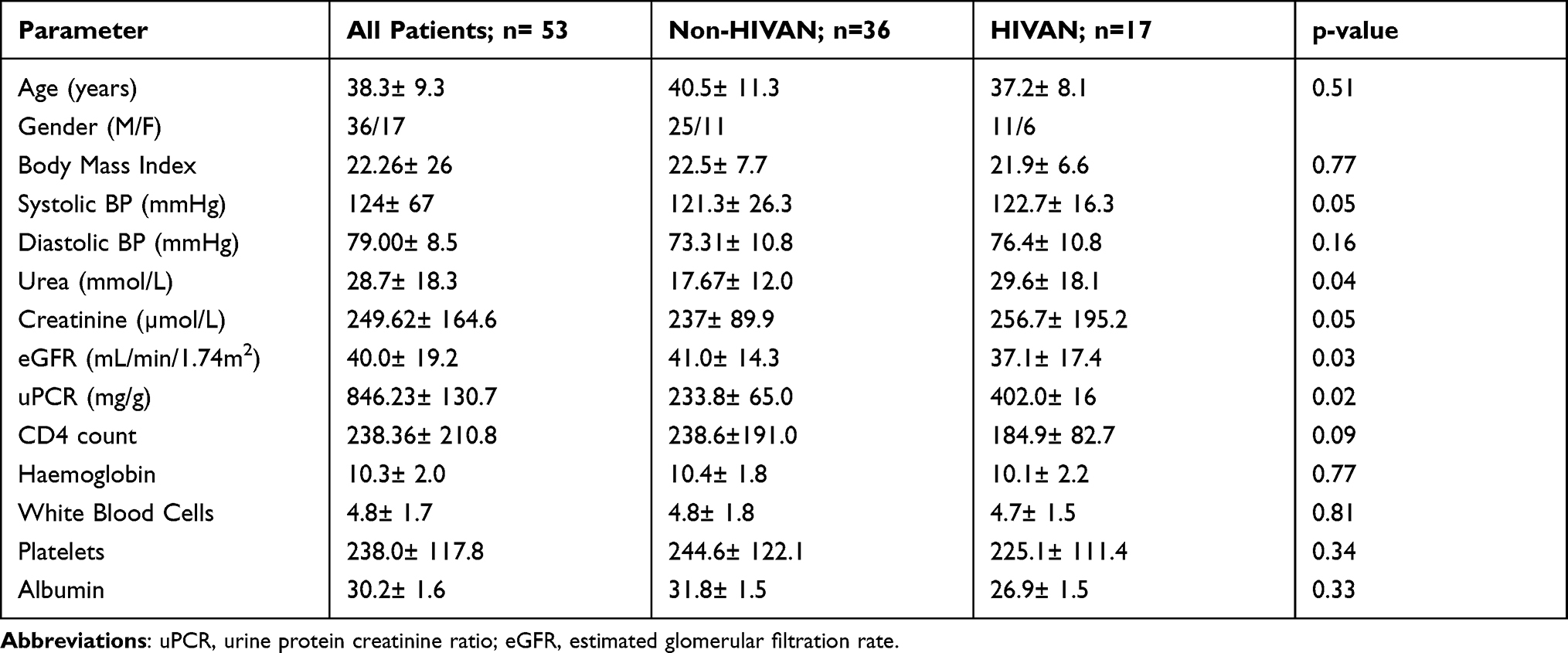 |
Table 1 Clinical and Laboratory Parameters of the Study Patients |
The histopathological lesions on kidney biopsy are shown in Table 2. The characteristic lesions consistent with HIVAN including collapsing Focal Segmental Glomerulosclerosis (FSGS), cystic tubular dilatation, interstitial infiltrates, and dilated tubules were reported in 17 (32%) of the patients; however the majority (37.7%) had FSGS as the histological diagnosis and 6 (11.3%) had no significant pathological finding. Majority of the FSGS seen in this study were of the NOS sub type with only a few being of the tipped sub type. Among the 10 patients that had IF evaluation of their tissues, none showed features of immune complex disease.
 |
Table 2 Summary of the Histopathological Findings of the Study Population |
Patients with HIVAN (compared to non-HIVAN patients) tended to have higher systolic BP (p= 0.05); higher serum creatinine levels (p= 0.05); lower eGFR (0.03) and higher uPCR; (p= 0.02). Other clinical and laboratory parameters including age, BMI, diastolic BP, CD4 count and hematological indices did not show any statistically significant differences between the two groups. Similarly, there were no significant differences between those with HIVAN and those with FSGS when the clinical and laboratory parameters were compared.
Similarly, only uPCR showed a statistically significant difference (p=0.00) on analysis of variance between the 3 groups those with FSGS, those with HIVAN and those with other histologic types.
Discussions
We report on the histopathologic pattern of kidney lesions seen among newly diagnosed, treatment-naïve HIV patients with either persistent proteinuria and/or reduced eGFR in a tertiary health facility in Nigeria.
The majority of patients in our study were males. Though this is similar to the findings by Vali et al9 who reported a greater male preponderance, it differs from that reported by Emem-chioma et al10 who reported a female preponderance in their study. The mean age of the study population is also similar to findings by others who have documented that most patients are young and in the most productive age group (30 to 50 years of age).10 The youngest patient in our study was 20 years while the oldest was 54 years and mean age was 38.3±9.3 years.
The results from this study corroborate the wide spectrum of renal changes that have been observed in HIV infection; with pathologies involving the glomerulus, tubules, and interstitium, and similar to what has been reported in other studies.11,12 This may be due to multiple pathogenetic mechanisms underlying renal affectation by the virus including a direct intrarenal HIV gene expression and lesions related to comorbidities, effects of drugs, immune dysregulation, and co-infections. This underscores the relevance of kidney biopsy among these patients.13
The predominant lesion was FSGS (37.7%), followed by HIVAN (32.1%) and then interstitial nephritis together with various others. This wide variation in observed histopathologic lesions has also been reported globally and has been attributed to factors such as the geographical and ethnic diversity as well as sample sizes of the reported studies.6
There are only a few studies with sizable numbers of HIV patients that had kidney biopsy done in Nigeria. Emem-Chioma et al10 reported that 7 (70%) of their 10 patients that were biopsied had histopathologic features of HIVAN. We have also earlier reported HIVAN in 55% of 25 patients that had kidney biopsy in our center.14 Though these frequencies of HIVAN are higher than the 32.1% found in this study, our current sample size is larger and thus may give a better representation of the true prevalence. This may also be due to the changing epidemiology of kidney disease among HIV-infected patients, characterized by reports of decrease in frequency of HIVAN over time.8,15,16 Although common genetic susceptibility to CKD and limited resources for the diagnosis and management of chronic diseases may allow HIVAN to still be relevant in this region.8
There are limited numbers of histopathological studies from other sub-Saharan African countries as well, with most of the reports from South Africa (SA). Reports from various studies in SA revealed that HIVAN in more than 80% of biopsies in Durban as reported by Han et al,17 in 27% in Johannesburg by Gerntholtz et al18 and in 57.2% in report from Cape Town by Wearne et al.11 A study from the Congo by Assounga et al19 reported a lower rate of HIVAN at 19% among black Africans. Koech et al20 reported that, out of the 27 patients with persistent proteinuria that underwent renal biopsy in Kenya, none had the classic HIVAN with the majority (41%) only having interstitial Nephritis.
Casanova et al,21 in a study among white Italian HIV-positive patients, reported that none had the classic HIVAN. Similarly, Praditpornsilpa et al22 in their study among 26 HIV-positive patients presenting with varying degrees of proteinuria in Thailand did not demonstrate a single case of HIVAN. These are at variance with the findings of this study, where HIVAN was the second most frequent histopathologic diagnosis. This may be related to genetic variations, especially the low prevalence of high-risk genotypes of APOL1 reported in these populations, compared to those reported among the West African population.
Reports from the Indian sub-continent also demonstrated wide variation in the prevalence of HIVAN ranging from 0 to 83%. However, a pooled analysis of data from 10 studies in India showed that HIVAN constituted 16.5%, followed by mesangioproliferative glomerulonephritis (MPGN) 13.9%, FSGS 7.7% and tubulointerstitial lesions 22.7% among other histologic diagnoses.23 Though this prevalence of HIVAN is lower than what we found in this study, the wide variation in the histopathologic findings is similar to that of our study.
Berliner et al24 from Baltimore in USA reported a frequency of 35% for HIVAN, 22% cases of FSGS, and 7.9% cases of acute interstitial nephritis along with other less frequent lesions. Kudose et al25 in a retrospective analysis of a cohort of 437 HIV-positive patients who had kidney biopsy at Columbia University also reported diverse pathologic diagnoses with the commonest being ICGN (17%), diabetic nephropathy (DN) (16%), classic HIVAN (14%) and FSGS (12%). The figures from Baltimore were similar to our finding as HIVAN and FSGS were the majority of the histologic diagnoses, the finding of ICGN and DN as the commonest diagnosis in the study from Baltimore was however at variance with our findings.
Presence of HIV-related tubulointerstitial lesions is commonly reported in all kidney biopsy series across the world, and may be present in up to 70% of cases.12 In this study, tubulointerstitial disease was seen in only 15% of our patients; and although higher than the 7.9% reported by Berliner et al, it is lower than the 27.7% and the 41% reported from India and Kenya respectively.23,24 Concurrent medications, use of herbal concoctions and infections, among other causes, may underlie the reasons for the high frequency of tubulointerstitial disease among these patients. A number of immune complex diseases have also been described in the setting of HIV, including IgA nephropathy, lupus-like glomerulonephritis (GN), membranous glomerulopathy, post-infectious GN, mesangiocapillary GN and the “ball-in-cup” phenomenon.13 However, none of those who had IF showed features of immune complex disease in our study. In contrast, Fabian et al26 in Johannesburg reported HIV immune-complex kidney disease as the predominant diagnosis in 8 (40%) of their 20 cases. This variation may be due to relatively small number (10) that had IF in our study or may actually be a result of low prevalence of immune-complex disease in this part of the world. This calls for further studies as there was no study from Nigeria that had IF evaluation to our knowledge.
Kidney involvement in HIV-infected patients can present at any stage of the illness although HIVAN commonly occurs late in the course of the illness.27 In this study we recruited newly diagnosed and treatment-naïve patients, presumably at an early stage of their illness. However, low CD4 cell counts may suggest advanced disease.
There was no major complication noted from the kidney biopsy procedure in this study, although HIV-infected patients that underwent renal biopsy are not expected to be at greater risk of major complications than the general population. Fine et al reported that 6 (3.2%) out of 187 HIV-infected patients who underwent ultrasound-guided biopsies in their center experienced a major complication and all were stabilized and discharged without further complications.28
Management of kidney disease in HIV-infected individuals poses some challenges, however suppression of HIV viral load, use of ARBs and ACEi in those with with confirmed or suspected HIVAN or those with significant proteinuria as well as special attention to therapeutic issues such as drug-drug interactions and drug-toxicity are important.29
Among the strengths of our study is the relatively high number of HIV-positive patients with kidney disease that had renal biopsy from a broad geographic area compared to other previous Nigerian studies that were limited by the small numbers of biopsied patients. Our institution receives referrals for kidney biopsy from many centers in our region because of our advantage in terms of resources and capacity for renal histology. Ten of the biopsy tissues had IF evaluation which is the first report from this locality even though limited by the small number; other studies from this region were limited by the fact that only light microscopic evaluation was done.
In conclusion, this study has demonstrated the safety and relevance of a kidney biopsy in the assessment of HIV-infected patients with renal involvement. It has demonstrated that although a wide range of histopathologic glomerular and tubulointerstitial lesions may be seen, FSGS and HIVAN are still the most common, with the frequency of HIVAN dropping from an earlier 55% to 32.1%.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Nigeria | UNAIDS [Internet]. [
2. Mulenga LB, Kruse G, Lakhi S, et al. Baseline renal insufficiency and risk of death among HIV-infected adults on antiretroviral therapy in Lusaka, Zambia. Aids. 2008;22(14):1821–1827. doi:10.1097/QAD.0b013e328307a051
3. Ekrikpo UE, Kengne AP, Bello AK, et al. Chronic kidney disease in the global adult HIV-infected population: a systematic review and meta-analysis. PLoS One. 2018;13(4):e0195443. doi:10.1371/journal.pone.0195443
4. Cohen SD, Kimmel PL. Renal biopsy is necessary for the diagnosis of HIV-associated renal diseases. Nature. 2014;8(1):22. doi:10.1038/ncpneph0990
5. Kopp JB, Winkler C. HIV-associated nephropathy in African Americans. Kidney Int. 2003;63(s83):43–49. doi:10.1046/j.1523-1755.63.s83.39.x
6. Lucas GM, Lau B, Atta MG, et al. Chronic kidney disease incidence, and progression to end-stage renal disease, in HIV-infected individuals: a tale of two races. J Infect Dis. 2008;197(11):1548–1557. doi:10.1086/587994
7. Arendse CG, Wearne N, Okpechi IG, Swanepoel CR. The acute, the chronic and the news of HIV-related renal disease in Africa. Kidney Int. 2010;78(3):239–245. doi:10.1038/ki.2010.155
8. Mallipattu SK, Salem F, Wyatt CM. The changing epidemiology of HIV-related chronic kidney disease in the era of antiretroviral therapy. Kidney Int. 2014;86(2):259–265. doi:10.1038/ki.2014.44
9. Vali PS, Ismal K, Gowrishankar S, Sahay M. Renal disease in human immunodeficiency virus - not just HIV-associated nephropathy. Indian J Nephrol. 2012;22(2):98–102. doi:10.4103/0971-4065.97117
10. Emem chioma P, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant. 2008;23(2):741–746. doi:10.1093/ndt/gfm836
11. Wearne N, Swanepoel CR, Boulle A, Duffield MS, Rayner BL. The spectrum of renal histologies seen in HIV with outcomes, prognostic indicators and clinical correlations. Nephrol Dial Transplant. 2012;27(11):4109–4118. doi:10.1093/ndt/gfr702
12. Cohen AH, Nast CC. HIV-associated nephropathy. A unique combined glomerular, tubular, and interstitial lesion. Mod Pathol. 1988;1(2):87–97.
13. Rosenberg AZ, Naicker S, Winkler CA, et al. HIV-associated nephropathies: epidemiology, pathology, mechanisms and treatment. Nat Rev Nephrol. 2015;11(3):150–160. doi:10.1038/nrneph.2015.9
14. Sakajiki AM, Adamu B, Arogundade FA, Abdu A, Atanda AT, Garba BI. Prevalence, risk factors, and histological pattern of kidney disease in patients with human immunodeficiency virus/acquired immunodeficiency syndrome at Aminu Kano Teaching Hospital: a Clinicopathologic Study. Ann Niger Med. 2014;8(2):69–75. doi:10.4103/0331-3131.153356
15. Cove-Smith A, Sheaff MT, Ashman N. HIVAN is increasingly less common in HIV- positive black Africans living in Europe. Kidney Int. 2006;70(9):1662. doi:10.1038/sj.ki.5001877
16. Jung O, Haack HS, Brodt HR, et al. Changing spectrum of renal disease in HIV infection. Dtsch Med Wochenschr. 2013;138(38):1887–1891. doi:10.1055/s-0033-1349438
17. Han TM, Naicker S, Ramdial PK, Assounga AG. A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney Int. 2006;69(12):2243–2250. doi:10.1038/sj.ki.5000339
18. Gerntholtz TE, Goetsch SJ, Katz I. HIV-related nephropathy: a South African perspective. Kidney Int. 2006;10(10):1885–1891. doi:10.1038/sj.ki.5000351
19. Assounga AG, Yala F, Mongo Y, et al. HIV and nephropathy in Congo: a comparative study of HIV-positive vs HIV-negative patients. Saudi J Kidney Dis Transpl. 1996;7(Suppl 1):S30–S32.
20. Koech MK, Owiti MOG, Owino-Ong’or WD, et al. Absence of HIV-associated nephropathy among antiretroviral naive adults with persistent albuminuria in Western Kenya. Kidney Int Rep. 2016;2(2):159–164. doi:10.1016/j.ekir.2016.11.007
21. Casanova S, Mazzucco G, Barbiano Di Belgiojoso G, et al. Pattern of glomerular involvement in human immuno-deficiency virus-infected patients: an Italian Study. Am J Kidney Dis. 1995;26(3):446–453. doi:10.1016/0272-6386(95)90490-5
22. Praditpornsilpa K, Napathorn S, Yenrudi S, Wankrairot P, Tungsaga K, Sitprija V. Renal pathology and HIV infection in Thailand. Am J Kidney Dis. 1999;33(2):282–286. doi:10.1016/S0272-6386(99)70301-X
23. Verma B, Singh A. Histological spectrum of renal disease in HIV/AIDS patients with significant proteinuria: an Indian perspective. J Family Med Prim Care. 2019;8(3):860–865. doi:10.4103/jfmpc.jfmpc_104_19
24. Berliner AR, Fine DM, Lucas GM, et al. Observations on a cohort of HIV-infected patients undergoing native renal biopsy. Am J Nephrol. 2008;28(3):478–486. doi:10.1159/000112851
25. Kudose S, Santoriello D, Bomback AS, et al. The spectrum of kidney biopsy findings in HIV-infected patients in the modern era. Kidney Int. 2020;97(5):1006–1016. doi:10.1016/j.kint.2020.01.018
26. Fabian J, Naicker S. HIV and kidney disease in Sub-Saharan Africa. Nat Rev Nephrol. 2009;5(10):591–598. doi:10.1038/nrneph.2009.141
27. Winston JA, Klotman ME, Klotman PE. HIV-associated nephropathy is a late, not early, manifestation of HIV-1 infection. Kidney Int. 1999;55:1036–1040. doi:10.1046/j.1523-1755.1999.0550031036.x
28. Fine DM, Perazella MA, Lucas GM, Atta MG. Kidney biopsy in HIV: beyond HIV-associated nephropathy. Am J Kidney Dis. 2008;51(3):504–514. doi:10.1053/j.ajkd.2007.12.005
29. Alfano G, Guaraldi G, Fontana F, Bellasi A, Cappelli G. Therapeutic management of HIV-infected patients with chronic kidney disease. J Nephrol. 2020;33(4):699–713. doi:10.1007/s40620-020-00701-8
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.