")
Back to Journals » International Journal of Women's Health » Volume 13
Hispanic Ethnicity and Cervical Cancer Precursors Among Low-Income Women in Arizona
Authors Riggs SL, Thomson CA, Jacobs E, Cutshaw CA, Ehiri JE
Received 4 July 2021
Accepted for publication 8 October 2021
Published 19 October 2021 Volume 2021:13 Pages 929—937
DOI https://doi.org/10.2147/IJWH.S327812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Sally L Riggs,1 Cynthia A Thomson,1 Elizabeth Jacobs,2 Chistina A Cutshaw,1 John E Ehiri1
1Department of Health Promotion Sciences, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson, AZ, USA; 2Department of Epidemiology and Biostatistics, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson, AZ, USA
Correspondence: Sally L Riggs
Department of Health Promotion Sciences, Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson, AZ, USA
Tel +1 520 499 4111
Email [email protected]
Purpose: In the United States, Hispanics are more likely to be diagnosed with cervical cancer compared to Non-Hispanic Whites. Annually, 250,000 to 1 million women are diagnosed with a precursor to CC. The aim of this study was to assess whether Hispanics have a higher prevalence of cervical dysplasia compared to Non-Hispanics Whites among a population of low-income women.
Patients and Methods: We analyzed the results of 10,911 cervical cytology tests administered between 2003 and 2016 that were funded through the Center for Disease Control and Prevention’s (CDC) program for low-income, uninsured women entitled the National Breast and Cervical Cancer Early Detection Program (NBCCEDP). In the state of Arizona, the program is called the Well Women HealthCheck Program (WWHP). Logistic regression was used to identify increased risk of dysplasia, including low-grade squamous intraepithelial lesions (LSIL) and high-grade squamous intraepithelial lesions (HSIL/ICC), and multinomial logistic regression was used to assess increased likelihood for LSIL and HSIL/ICC as separate categories.
Results: In the crude analysis, Hispanic ethnicity was modestly associated with higher prevalence of LSIL (odds ratio (OR)=1.39, 95% CI=1.01– 1.91), but this association was not statistically significant after adjusting for confounders. However, in the final models, lower income was independently associated with LSIL (adjusted odds ratio [aOR]=1.55, 95% CI=1.30– 1.44), while smoking (aOR=2.88, 95% CI=1.21– 6.84) and no history of Pap test within five years (aOR=3.54, 95% CI=1.61– 6.99) were independently associated with HSIL.
Conclusion: After adjusting for confounding in a sample of low-income women with comparable Pap screening rates, ethnicity was not associated with greater prevalence of abnormal pap smears. However, other variables were independently associated with LSIL and HSIL. The higher proportion of LSIL cases among lower income individuals compared to those with higher incomes, and the higher proportion of HSIL cases observed among those screened least regularly stresses the importance of programs like WWHP: programs that target low-income, uninsured women. These programs help save lives.
Keywords: low-grade squamous intraepithelial lesions, high-grade squamous intraepithelial lesions, well women health check program, national breast and cervical cancer early detection program, COVID-19
Introduction
The introduction of the Papanicolaou smear screening test (Pap test) in the 1950’s led to a 60% reduction in the incidence of cervical cancer in the United States (US).1 It is anticipated that the development of human papillomavirus (HPV) vaccine will reduce the incidence even further.2 However, some groups of women have benefitted from these advances more than others. Compared to non-Hispanic whites, Hispanic women have a 40% higher rate of cervical cancer diagnosis and are 26% more likely to die from the disease.3 Between 2013–2017, the incidence of cervical cancer in Arizona (AZ) was 8.7 per 100,000 among Hispanics and 6.8 per 100,000 among non-Hispanic whites.4
While a diagnosis of cervical cancer (CC) is relatively uncommon in the US, the precursors to the disease, low-grade squamous intraepithelial lesions (LSIL) and high-grade squamous intraepithelial lesions (HSIL), are not.5 Caused by persistent infection of a high-risk variant of the human papillomavirus (HrHPV), 1.4 million women are diagnosed with LSIL and 330,000 women are diagnosed with HSIL in the US every year.6
There are financial and emotional costs associated with cervical dysplasia diagnoses. Also, depending on insurance status and severity of disease, the cost of treating cervical pre-cancerous lesions range from a few hundred dollars for ablative treatments to thousands of dollars for excisional treatments.7 Treating more advanced disease frequently requires excisional methods, which, in some cases, have been linked to adverse outcomes, such as preterm delivery (PTD), while new research has indicated that the higher risk for PTD associated with high grade cervical lesions may be due to the disease process itself rather than the treatment.8–10 Treating more advanced disease frequently requires excisional methods, which, in some cases, have been linked to adverse outcomes, such as preterm delivery (PTD). It should be noted, however, that new research has indicated that the higher risk for PTD associated with high grade cervical lesions may be due to the disease process itself rather than the treatment.11,12
It is believed that the higher incidence of cervical cancer observed among Hispanics is largely due to variations in Pap test coverage.13 Compared to Non-Hispanic whites, Hispanic women are less likely to report having a Pap smear within the last 5 years.5,14,15 Obstacles to screening among Hispanics in Arizona include cultural attitudes, linguistic barriers and immigration status; undocumented immigrants and new immigrants (undocumented immigrants residing in AZ for less than 5 years) are ineligible to receive health insurance.16,17
With a population of nearly 60 million people, Hispanics constitute the largest ethnic minority group in the US, and they are projected to comprise nearly one-third of the US population by 2060.18–20 Gaining more understanding about the effects of cervical cancer precursors among a population disproportionately affected by cervical cancer is of public health significance. Annually, US healthcare systems spend over one billion dollars evaluating and treating this condition.6 The aim of this study was to assess the burden of cervical precancers among Hispanic women as compared to non-Hispanic whites, all of whom received screening through the Arizona division of the Center for Disease Control and Prevention’s (CDC) National Breast and Cervical Cancer Early Detection Program (NBCCEDP), the Well Woman HealthCheck program (WWHP). The Pap screenings were administered in federally funded health care clinics located in Pima County between 2003 and 2016.
Materials and Methods
Study Design and Population
This is a cross-sectional analysis of 11,326 Pap tests and follow-up test results funded by Pima County’s Well Women HealthCheck (WWHP) program between 2003 and 2016. WWHP was established in Arizona in 1993 as part of the National Breast and Cervical Cancer Early Detection Program (NBCCEDP). To be eligible to receive services under WWHP, women must be residents of Arizona, be uninsured or underinsured (have insurance that does not cover the services offered by the WWHP or have a co-pay of $100 or more for breast and cervical cancer screening and/or diagnostic services), do not have Medicare Part B, are not enrolled in the Arizona Health Care Cost Containment System (AHCCCS) and have a household income that does not exceed 250% of the federal poverty limit. WWHP provides clinical breast exams, mammograms, pelvic exams and pap tests. If screening tests are abnormal, the program offers colposcopy with or without biopsy and ultrasounds.21 Patient navigators help women diagnosed with precancerous cervical lesions or cervical cancer enroll in the Breast and Cervical Cancer Treatment Program (BCCTP) offered through the state’s Medicaid program, the Arizona Health Care Cost Containment System (AHCCCS).
Bi-annually, NBCCEDP grantees are required to submit a subset of standardized patient and clinical level program data known as Minimum Data Elements (MDEs) to the CDC consisting of information related to clinical encounters, including date of service, patient age, race, ethnicity, screening history (yes, no, not within the past 5 years and unknown), symptoms, indication for test, examination received, examination results, and final diagnosis.22 MDE demographics include age, race, and ethnicity, and on the intake form, Hispanic ethnicity is referred to as Hispanic/Latino.22 In addition to demographic characteristics and clinical outcomes, MDEs also contain unique patient identifiers that can be used to track program utilization and health outcomes over time.23 In addition to the MDEs, states can elect to collect data on other variables.23 For example, the state of Arizona collects information on household size and smoking status, defined as “the use of tobacco or electronic nicotine (tobacco-like) products in the last 30 days.” The complete dataset used for this study was extracted from Arizona’s NBCCEDP database.
In total, 10,911 test results were included in the study; four hundred and four (404) cases were excluded because the women tested did not fit the study criteria as identifying as either Hispanic or Non-Hispanic white, and an additional 11 cases did not have a conclusive diagnosis. Prior to transferring the database to the University of Arizona for use in this study, the Arizona Department of Health Services (ADHS) removed all identifiers, including names, addresses, and zip codes from the NBCCEDP dataset. After review, the study was exempted from full human subjects review by the Mel and Enid Zuckerman College of Public Health Research Office.
Definition of Outcome Variables
In this study, an abnormal Pap smear included a diagnosis of LSIL or HSIL/CC. LSIL consisted of LSIL diagnoses, atypical squamous cells of undetermined significance (ASCUS) with concurrent high-risk HPV (HrHPV+) infection and mild cervical intraepithelial neoplasia (CIN 1) as determined by biopsy. HSIL included HSIL diagnoses, moderate and severe cervical intraepithelial neoplasia (CIN 2 and CIN 3, respectively) adenocarcinoma and cervical cancer (CC). Adenocarcinoma and CC were added to the HSIL category because of the limited number of cases (1 and 3, respectively). In addition to normal/benign results, the reference group incorporated diagnoses of benign inflammation due to the transitory nature of the condition.
Statistical Analysis
To compare demographic differences between the two study groups (Non-Hispanic whites vs Hispanics), Chi Square tests were used to analyze differences in the distribution among categorical variables, and the Student’s T-test was used to assess continuous variables. Odds ratios (ORs) were calculated using logistic regression to evaluate the predictor of primary interest (Hispanic ethnicity) and cervical disease status. Before fitting the complete model, associations between the independent variables and the outcome variable were examined individually.
Following the bivariate analysis, multivariate logistic regression was conducted. First, the dependent variable was broken down into two categories (negative and positive). In this analysis, tests were classified as “positive” if they were diagnosed as LSIL or HSIL/CC. Multinomial logistic regression was used to investigate the relationship between the predictor variable and three different categories of cervical cytology (negative, LSIL & HSIL/CC). In this model, women with normal cytology served as the reference category for the dependent variable. The model estimated two odds ratios (ORs) simultaneously for each risk factor evaluated: the OR for LSIL versus normal and the OR for HSIL/CC versus normal. Independent variables available from the NBCCEDP database provided by ADHS, included age (years), income (USD), household size, ethnicity/race, smoking status, prior Pap test and country of birth (United States or Mexico). Variables such as poverty, ethnicity, smoking, immigration status and Pap screen history have been associated with cervical dysplasia in the literature.24–28 A variable called “number of visits” was added to the model to adjust for the possible effect of multiple clinic visits by individual patients. Confounders were kept in the final model if they were significant at the p<0.05 level, and the adjusted odds ratio differed from the crude odds ratio by ≥10%. Potential effect modification was assessed, and if found, those variables were to be stratified and the effect modification documented. Data were analyzed using Stata version 1 (StataCorp LP, College Station, TX).29
Results
Participant characteristics are presented in Table 1. Seventy-eight percent (78%) of the participants were Hispanic and nearly three-quarters (73%) were born in Mexico. This is not surprising given Pima County’s proximity to the Mexican border, and the NBCCEDP’s role as the only screening program accessible to new and undocumented immigrants. Between 2003 and 2016, 44% of study participants received one Pap test, 38% received two to three Pap tests and 18% were screened four or more times. On average, non-Hispanic whites had fewer screening visits compared to Hispanics (Table 1).
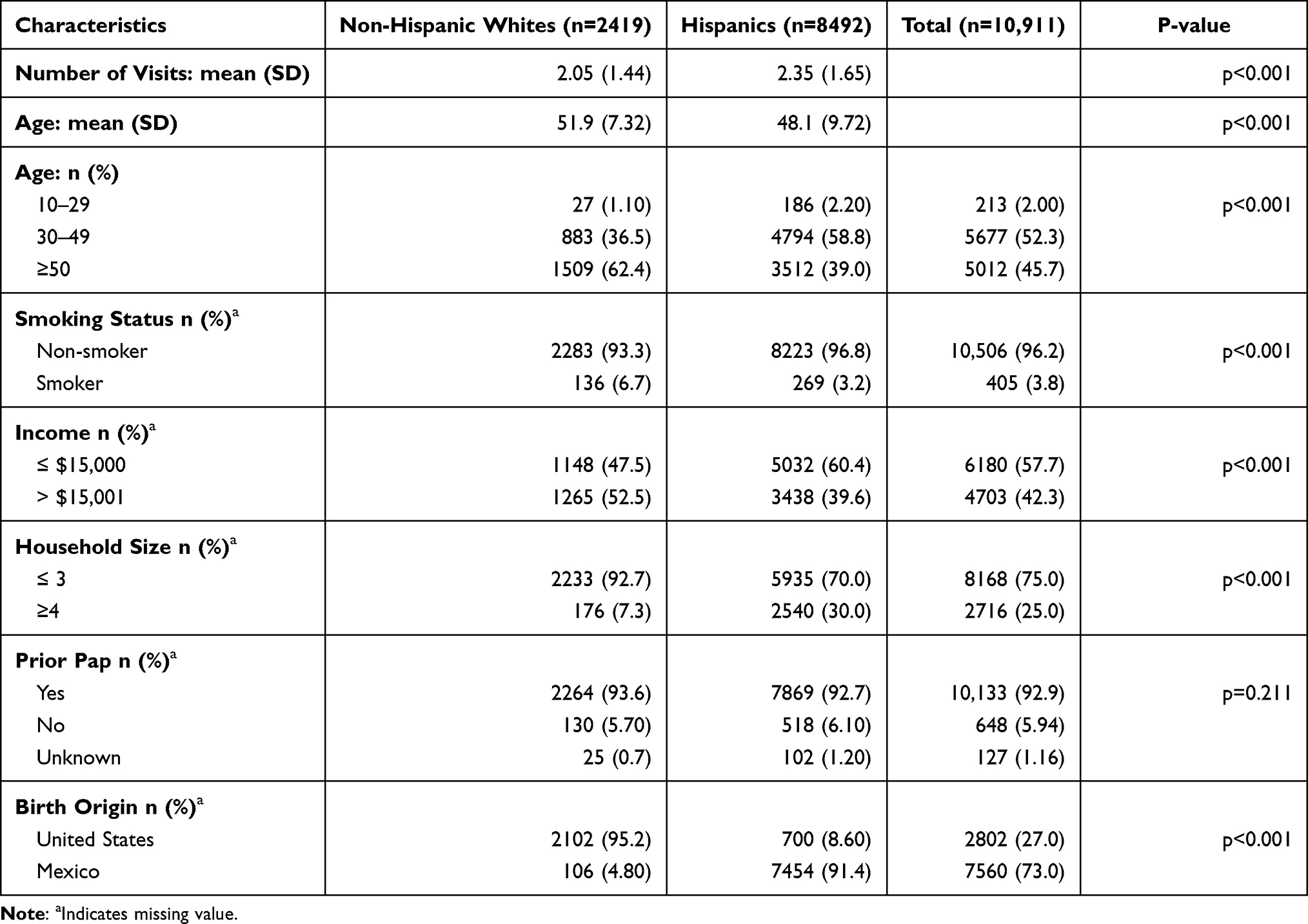 |
Table 1 Patient Characteristics by Ethnicity |
Compared to non-Hispanic whites, Hispanics were significantly younger (p<0.001), less likely to smoke (p<0.001), more likely to live in larger households (p<0.001), have a lower income (p=0.013) and more likely to be born in Mexico (p<0.001). There was no significant difference in Pap screening history between the two groups.
Prevalence and characteristics associated with different categories of cervical dysplasia (negative, positive, LSIL & HSIL/CC) are displayed. In Table 2, bivariate analysis was used to explore individual factors related to different categories of disease. A total of 10,911 cases were analyzed: 10,575 negative test results (96.92%) and 336 positive test results (3.08%).
 |
Table 2 Cervical Cytology: Associations with Socio-Demographics (n=10,911) |
Within the positive test category, there were 275 (2.52%) cases of LSIL and 61 (0.56%) cases of HSIL/CC. Four cases of CC were identified; 3 of which were diagnosed in Hispanic women. In the bivariate analysis, Hispanic ethnicity was marginally associated with positive Pap test results (OR=1.39, 95% CI=1.01–1.91). Older age (≥50 years) was protective for abnormal Pap, LSIL and HSIL/CC (OR=0.32, 95% CI=0.18–0.57); (OR=0.39, 95% CI=0.20–0.75); (OR=0.16, 95% CI= 0.05–0.48), respectively, while the middle age group (30–49 years) was protective for abnormal Pap (OR=0.57, 95% CI=0.33–0.99).
Lower income (≤ $15,000) was associated with abnormal Pap results (OR=1.40, 95% CI=1.12–1.75) and LSIL (OR=1.52, 95% CI=1.18–1.95), while smoking was positively associated with HSIL/CC (OR=2.16, 95% CI=1.23–6.70). Absence of a Pap test within the past five years was associated with HSIL/CC prevalence (OR=2.68, 95% CI=1.03–4.42), and “unknown” Pap test history was associated with abnormal Pap (OR=3.02, 95% CI=1.61–5.67) and HSIL/CC (OR=7.99, 95% CI=3.14–20.4). Women born in Mexico were more likely to be diagnosed with an abnormal Pap test result (OR=1.49, 95% CI=1.14–1.94) and LSIL (OR=1.53, 95% CI=1.13–2.07) compared to women born in the US.
Results from the multivariate analysis are presented in Table 3. After adjusting for confounders, ethnicity was no longer associated with a higher likelihood of LSIL (Adjusted Odds Ratio [aOR]=1.04, 95% CI=0.75–1.45). Number of visits was positively associated with abnormal Pap smears, LSIL and HSIL ((aOR=1.34, 95% CI=1.28–1.41); (aOR=1.37, 95% CI=1.30–1.44); (aOR=1.19, 95% CI=1.04–1.36, respectively)). This is not surprising given that more abnormal findings are going to be uncovered through more screening; this is especially true of HPV disease, given its transient nature and unpredictable course.
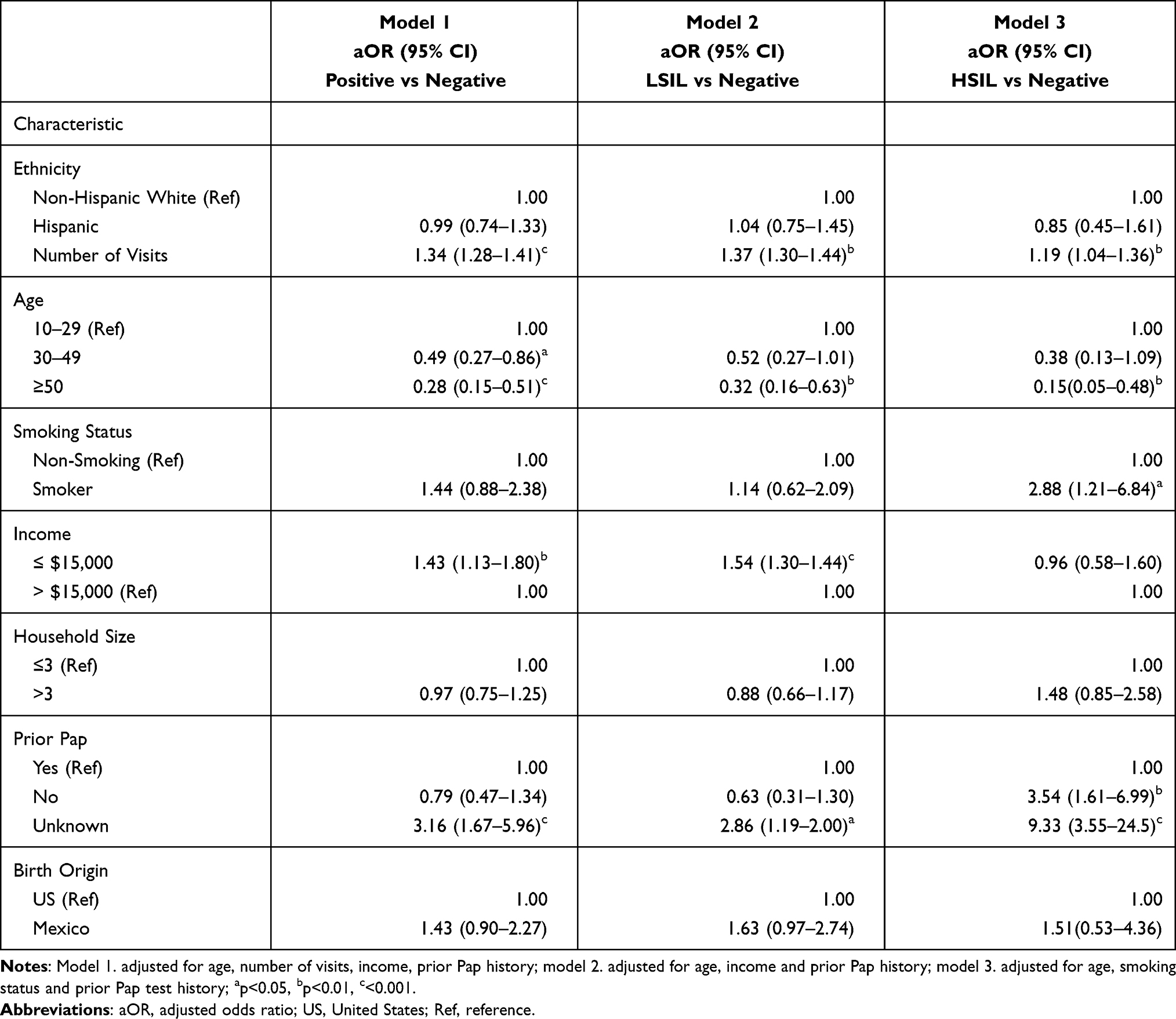 |
Table 3 Factors Associated with Ethnicity (Non-Hispanic Whites/Hispanics) and Positive Pap Smear Results, LSIL & HSIL: Adjusted Models |
The oldest age group (≥50 years) remained protective in all three disease categories: positive Pap test (aOR=0.28, 95% CI=0.15–0.51), LSIL (aOR=0.32, 95% CI=0.16–0.63) and HSIL/CC (aOR=0.15, 95% CI 0.05–0.48). The middle age group (30–49 years) remained protective for abnormal Pap test (aOR=0.49, 95% CI=0.27–0.86). In the final model, lower income remained associated with a higher likelihood for an abnormal Pap test (aOR=1.43, 95% CI=1.13–1.80) and LSIL (aOR=1.54, 95% CI=1.30–1.44), and smoking remained associated with higher HSIL/CC prevalence (aOR=2.88, 95% CI=1.21–6.84). Absence of Pap test within past five years remained associated with higher HSIL/CC prevalence (aOR=3.54, 95% CI=1.61–6.99) and “unknown” Pap test history remained associated with higher likelihood to be diagnosed with an abnormal Pap test (aOR=3.16, 95% CI=1.67–5.96) or HSIL/CC (aOR=9.33, 95% CI=3.55–24.5). Mexican nativity was no longer statistically significant in the final model.
Discussion
In this study, we looked at risk factors for cervical precancerous lesions among low-income women living in Pima County, AZ. Among our sub-sample of NBCCEDP recipients, there was no statistically significant difference in Pap test history between Hispanics and non-Hispanic whites and no significant difference in the prevalence of abnormal Pap test results. These findings are inconsistent with current research that puts Hispanics at higher risk for cervical dysplasia.29–31 This finding may be due to the comparable screening histories between the two groups in our study.32 Nevertheless, we did identify other independent risk factors, including smoking, lower income and Pap smear history.
Among our sample of 10,911 Pap test results, 3.08% were diagnosed as abnormal; 3.20% among Hispanics compared to 2.48% among non-Hispanic whites. In a nation-wide study that looked at cervical dysplasia among NBCCEDP recipients between 2002–2012, 2.35% of Hispanics presented with abnormal Pap smear results.33 These findings suggest that our sample of Arizona residents may be at greater risk for abnormal Pap findings compared to national data, thus supporting the need for more in-depth study in this population. When we divided positive tests results into two categories, the prevalence of LSIL was 2.68% among Hispanics compared to 1.94% among non-Hispanic whites. The overall prevalence of HSIL/CC was 0.56% with little difference between Hispanics (0.57%) and non-Hispanic whites (0.54%). A large-scale study of 1,761,146 Pap test results collected between 2007 and 2011 revealed an HSIL prevalence of 0.25%, an LSIL prevalence of 1.54%.34 After removing the 4 cases of cervical cancer in our database, HSIL prevalence remained relatively high (0.52%).35
In our study, women who smoked were nearly 3 times more likely to be diagnosed with HSIL/CC. This is not an unusual finding. Studies have linked cigarette smoking to increased risk of HSIL and cervical cancer.36 A large-scale study that followed women diagnosed with ASCUS or LSIL over a two-year period found an association between smoking intensity and duration with progression to HSIL37 Furthermore, research has determined that among HPV infected individuals, smoking has been linked to reoccurrence of HSIL after treatment and progression to invasive cervical disease.38
Screening history was associated with abnormal Pap tests and HSIL. Women who did not receive a Pap screen within the previous five years were 2.9 times more likely to be diagnosed with HSIL compared to women who were screened more regularly. Participants who responded “unknown” to the question about Pap test history were 3.16 times more likely to have an abnormal Pap smear and 7.75 times more likely to be diagnosed with HSIL/CC; however, due to the large standard error, one must be cautious interpreting the result. In a study looking at cancer diagnosis and stage among NBCCEDP recipients, Miller et al found that women who had been rarely or never screened and women with “unknown” Pap histories were more likely to be diagnosed with cancer, and at later stages, compared to women who were screened regularly.39 It may be of value to explore this finding further in order to determine whether this is an issue of social desirability bias, lack of English language proficiency, poor health literacy or a combination of factors.
When compared to a group with a comparable Pap screening history, as in this study, Hispanic ethnicity was not an independent risk factor for cervical dysplasia. This finding supports the hypothesis that cervical cancer differences in Hispanic vs non-Hispanic white women may be driven by access to care rather than by ethnicity. Nationally, Hispanic women are screened less frequency than non-Hispanic whites, especially among women of Mexican origin.40,41 The US is home to five million Mexican-born women, both documented and undocumented, making it the largest female immigrant group living in the United States.19 Screening programs like the NBCCEDP are essential; they help save lives. It was encouraging to see patients returning for annual screenings and follow-up visits, especially given the lack of healthcare options for new and undocumented immigrants in Arizona.
This study adds to the existing research on cervical cancer precursors, especially among Hispanic immigrants. As the disease advances, so do associated treatment costs and concerns. Given that much of the literature pertaining to Hispanics and cervical disease focuses exclusively on cervical cancer, assessing prevalence and risks associated with cervical dysplasia is relevant. With the introduction of the HPV vaccine in 2006, there has been enhanced monitoring of cervical dysplasia to help gage the efficacy of the vaccine. Currently, the Human Papillomavirus Vaccine Impact Monitoring Project (HPV-IMPACT) monitors rates of moderate and severe dysplasia (CIN2+) in an effort to assess the efficacy of the HPV vaccine.42 Given the disruption of the COVID-19 pandemic, screening is more important than ever. A study comparing the percentage of woman receiving cervical cancer screening pre and during the pandemic (January 1 – September 30, 2019 vs January 1 – September 30, 2020) found that the screening rate declined significantly across all ages and ethnicities during the second time period.43 It will take time to assess the full impact of the pandemic. In the meanwhile, it is important to study the factors related to cervical dysplasia among high-risk populations in hopes of developing more effective prevention programs.
A number of weaknesses can be found with this study. Temporality of risk factors associated with cervical disease cannot be established given its cross-sectional design. In addition, because the sub-sample size of HSIL was small, only strong associations could be detected. Conducting a similar study of NBCCEDP beneficiaries across the state would help confirm or dispel these findings. In addition, a number of factors that have previously been associated with cervical dysplasia were not available, including oral contraceptive use, sexually transmitted infection status, parity, age at first intercourse, number of sexual partners and HPV genotype.18 And finally, this study may lack generalizability given it specific geographic focus.
Conclusion
The prevalence of cervical dysplasia among our study participants, the majority of whom (78%) were Hispanic, speaks to the need for continued screening, particularly given the relatively high prevalence of HSIL. Considering that it will take decades to detect a significant reduction in cervical cancer prevalence resulting from the HPV vaccination, ongoing research is needed to identify communities with a higher burden of cervical disease in order to target cervical cancer screening and vaccination services where they are needed most.
Acknowledgments
The author(s) would like to acknowledge Francisco Garcia, MD, Pima County Chief Medical Officer, for his generous assistance with this paper and for aiding our efforts to access the data.
Disclosure
The authors report no conflict of interest in this work, nor have they received financial support for research, authorship, and/or publication of this article.
References
1. Hallowell BD, Endeshaw M, McKenna MT, Senkomago V, Razzaghi H, Saraiya M. Cervical cancer death rates among U.S.- and foreign-born women: U.S., 2005–2014. Am J Prev Med. 2019;56(6):869–874. doi:10.1016/j.amepre.2019.01.007
2. Burdette AM, Webb NS, Hill TD, Jokinen-Gordon H. Race-specific trends in HPV vaccinations and provider recommendations: persistent disparities or social progress? Public Health (London). 2016;142:167–176. doi:10.1016/j.puhe.2016.07.009.
3. Jandorf L, Bursac Z, Pulley LV, Trevina M, Castillo A, Erwin DO. Breast and cervical cancer screening among Hispanics attending culturally specific educational programs. Prog Community Health Partnersh Res Educ Action. 2008;2(3):95–204. doi:10.1353/cpr.0.0034
4. American Cancer Society. Cancer facts and figures for Hispanics/Latinos 2018–2020. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-hispanics-and-latinos/cancer-facts-and-figures-for-hispanics-andlatinos-2018-2020.pdf.
5. U.S. Cancer Statistics Working Group. U.S. cancer statistics data visualizations tool, based on 2019 submission data (1999–2017): U.S. department of health and human services, centers for disease control and prevention and national cancer institute; 2020. Available from: www.cdc.gov/cancer/dataviz.
6. Cooper DB, McCathran CE. Cervical dysplasia; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430859.
7. Oregon Health Authority. Human papillomavirus infections in Oregon, 2018. CD Summary. 2018;67(7). www.oregon.gov/oha/PH/DISEASESCONDITIONS/COMMUNICABLEDISEASE/CDSUMMARYNEWSLETTER/Documents/2018/ohd6707.pdf.
8. Shah R, Nwankwo C, Kwon Y, Corman SL. Economic and humanistic burden of cervical cancer in the United States: results from a nationally representative survey. J Womens Health. 2020;29(6):799–805. doi:10.1089/jwh.2019.7858
9. Desravines N, Miele K, Carlson R, Chibwesha C, Rahangdale L. Topical therapies for the treatment of cervical intraepithelial neoplasia (CIN) 2–3: a narrative review. Gynecol Oncol Rep. 2020;33:1. doi:10.1016/j.gore.2020.100608
10. Maguire P, McCarthy C, Molony P, et al. Large loop excision of the transformation zone and preterm delivery over a decade in a major women’s hospital. Ir J Med Sci. 2019;188(2):579–581. doi:10.1007/s11845-018-1893-z
11. Maina G, Ribaldone R, Danese S, et al. Obstetric outcomes in patients who have undergone excisional treatment for high-grade cervical squamous intra-epithelial neoplasia. Eur J Obstet Gynecol. 2019;236:210–213. doi:10.1016/j.ejogrb.2019.02.025
12. Rask M, Swahnberg K, Lindell G, Oscarsson M. Women’s experiences of abnormal pap smear results - a Qualitative Study. Sex Reprod Health. 2017;12:3–8. doi:10.1016/j.srhc.2017.01.002
13. Thangarajah F, Einzmann T, Bergauer F, et al. Cervical screening program and the psychological impact of an abnormal pap smear: a self-assessment questionnaire study of 590 patients. Arch Gynecol Obstet. 2016;293(2):391–398. doi:10.1007/s00404-015-3821-z
14. Guardado-Estrada M, Juarez-Torres E, Roman-Bassaure E, et al. The distribution of high-risk human papillomaviruses is different in young and old patients with cervical cancer. PLoS One. 2014;9(10):1–12. doi:10.1371/journal.pone.0109406
15. Herrera DG, Schiefelbein EL, Smith R, et al. Cervical cancer screening in the US–Mexico border region: a binational analysis. Matern Child Health J. 2012;16(2):298–306. doi:10.1007/s10995-012-1130-8
16. Reininger BM, Barroso CS, Mitchell-Bennett L, et al. Social-ecological influences on health-care access and navigation among persons of Mexican descent living on the U.S./Mexico border. J Immigr Minor Health. 2014;16(2):218–228. doi:10.1007/s10903-012-9714-3
17. Moore de Peralta A, Holaday B, Hadoto IM. Cues to cervical cancer screening among U.S. Hispanic women. HCCI. 2017;15(1):5–12. doi:10.1177/1540415316682494
18. Kiser L, Butler J. Improving equitable access to cervical cancer screening and management. Am J Nurs. 2020;120(11):58–67. doi:10.1097/01.NAJ.0000721944.67166.17
19. Colby SL, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. Current Population Reports 2015. U.S. Census Bureau: Washington, DC; 2014:25–1143.
20. Krogstad JM. Hispanics have accounted for more than half of total U.S. population growth since 2010; 2020. Available from: https://www.pewresearch.org/fact-tank/2020/07/10/hispanics-have-accounted-for-more-than-half-of-total-u-s-population-growth-since-2010/.
21. Cancer prevention and control programs. Arizona department of health services web site. Available from: http://www.azdhs.gov/prevention/health-systems-development/cancer-prevention-control/index.php#healthcheck-home.
22. Siegl EJ, Miller JW, Khan K, Harris SE. Quality assurance through quality improvement and professional development in the national breast and cervical cancer early detection program. Cancer. 2014;120(S16):2584–2590. doi:10.1002/cncr.28822.
23. Yancy B, Royalty JE, Marroulis S, Mattingly C, Benard VB, DeGroff A. Using data to effectively manage a national screening program. Cancer. 2014;120(S16):2575–2583. doi:10.1002/cncr.28821.
24. Luhn P, Walker J, Schiffman M, et al. The role of co-factors in the progression from human papillomavirus infection to cervical cancer. Gynecol Oncol. 2012;128(2):265–270. doi:10.1016/j.ygyno.2012.11.003.
25. Roura E, Castellsagué X, Pawlita M, et al. Smoking as a major risk factor for cervical cancer and pre-cancer: results from the EPIC cohort. Int J Cancer. 2014;135(2):453. doi:10.1002/ijc.28666.
26. Niccolai LM, Russ C, Julian PJ, et al. Individual and geographic disparities in human papillomavirus types 16/18 in high‐grade cervical lesions. Cancer. 2013;119(16):3052–3058. doi:10.1002/cncr.28038.
27. Niccolai LM, Julian PJ, Bilinski A, et al. Geographic poverty and racial/ethnic disparities in cervical cancer precursor rates in Connecticut, 2008–2009. Am J Public Health. 2013;103(1):156–163. doi:10.2105/AJPH.2011.300447.
28. Gargano JW, Nisenbaum R, Lee DR, et al. Age-group differences in human papillomavirus types and cofactors for cervical intraepithelial neoplasia 3 among women referred to colposcopy. Cancer Epidemiol Biomarker Preven. 2012;21(1):111–121. doi:10.1158/1055-9965.EPI-11-0664.
29. StataCorp. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC; 2019.
30. Henk HJ, Insinga RP, Singhal PK, Darkow T. Incidence and costs of cervical intraepithelial neoplasia in a US commercially insured population. J Low Genit Tract Dis. 2010;14(1):29–36. doi:10.1097/LGT.0b013e3181ac05e9
31. Gomez N, Guendelman S, Harley KG, et al. Nativity and neighborhood characteristics and cervical cancer stage at diagnosis and survival outcomes among Hispanic women in California. Am J Public Health. 2015;105(3):538–545. doi:10.2105/AJPH.2014.302261
32. Baezconde-Garbanati L, Murphy ST, Moran MG, et al. Reducing the excess burden of cervical cancer among Latinas: translating science into health promotion initiatives. Calif J Health Promot. 2014;11(1):45–57. doi:10.32398/cjhp.v11i1.1517
33. Shoemaker ML, White MC. Breast and cervical cancer screening among Hispanic subgroups in the USA: estimates from the national health interview survey 2008, 2010, and 2013. Cancer Causes Control. 2016;27(3):453–457. doi:10.1007/s10552-016-0718-5
34. Benard VB, Royalty J, Saraiya M, Rockwell T, Heisel W. The effectiveness of targeting never or rarely screened women in a national cervical cancer screening program for underserved women. Cancer Causes Control. 2015;26(5):713–719. doi:10.1007/s10552-015-0542-3
35. Gage JC, Hunt WC, Schiffman M, et al. Similar risk patterns after cervical screening in two large U.S. populations: implications for clinical guidelines. Obstet Gynecol. 2015;128(6):1248–1257. doi:10.1097/AOG.0000000000001721
36. Fang JH, Yu XM, Zhang SH, Yang Y. Effect of smoking on high-grade cervical cancer in women on the basis of human papillomavirus infection studies. J Can Res Ther. 2018;14(Suppl S1):184–189. doi:10.4103/0973-1482.179190
37. McIntyre-Seltman K, Castle PE, Guido R, Schiffman M, Cosette M, Wheeler M. Smoking is a risk factor for cervical intraepithelial neoplasia grade 3 among oncogenic human papillomavirus DNA–positive women with equivocal or mildly abnormal cytology. Cancer Epidemiol Biomarker. 2005;14(5):1165–1170. doi:10.1158/1055-9965.EPI-04-0918
38. James SA, Meier EM, Wagener TL, et al. E-Cigarettes for immediate smoking substitution in women diagnosed with cervical dysplasia and associated disorders. Int J Environ Res Public Health. 2016;288(13):1–11. doi:10.3390/ijerph13030288
39. Miller JW, Royalty J, Henley J, et al. Breast and cervical cancers diagnosed and stage at diagnosis among women served through the national breast and cervical cancer early detection program. Cancer Causes Control. 2015;26(5):741–747. doi:10.1007/s10552-015-0543-2
40. Goel MS, Wee CC, McCarthy EP, Davis RB, Ngo-Metzger Q, Phillips RS. Racial and ethnic disparities in cancer screening: the importance of foreign birth as a barrier to care. J Gen Intern Med. 2003;18(12):1028–1035. doi:10.1111/j.1525-1497.2003.20807.x
41. Shoemaker ML, White MC. Breast and cervical cancer screening among Hispanic subgroups in the USA estimates from the national health interview survey 2008, 2010, and 2013. Cancer Causes Control. 2017;27(3):453–457. doi:10.1007/s10552-016-0718-5
42. McClung NM, Gargano JW, Park IU, et al. Estimated number of cases of high-grade cervical lesions diagnosed among women – United States, 2008 and 2016. MMWR Morb Wkly Rep. 2019;68(15):337–343. doi:10.15585/mmwr.mm6815a1
43. Miller MJ. Impact of COVID-19 on cervical cancer screening rates among women aged 21–61 years. MMWR. 2021;70(4):109–111.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.