")
Back to Journals » International Journal of General Medicine » Volume 14
High Seroprevalence Against SARS-CoV-2 Among Faculty of Medicine and Health Sciences Personnel and Students of the University of Alcalá, Spain: Contributing Factors
Authors Pérez-Tanoira R , Lledó García L , Torralba González de Suso M , Rodríguez Zapata M, Arroyo Serrano T, Giménez Pardo C, Rodríguez Pedrosa MI, Romero Badía MN, Pérez-García F , González López P, Villaescusa García C, Cuadros González J
Received 5 August 2021
Accepted for publication 28 September 2021
Published 21 October 2021 Volume 2021:14 Pages 7017—7024
DOI https://doi.org/10.2147/IJGM.S332803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ramón Pérez-Tanoira,1,2 Lourdes Lledó García,1 Miguel Torralba González de Suso,3,4 Manuel Rodríguez Zapata,4 Teresa Arroyo Serrano,2 Consuelo Giménez Pardo,1 María Isabel Rodríguez Pedrosa,5 Mª Nuria Romero Badía,5 Felipe Pérez-García,1,2 Patricia González López,5 Cristina Villaescusa García,5 Juan Cuadros González1,2
1Department of Biomedicine and Biotechnology, Alcalá University, Alcalá de Henares, Madrid, Spain; 2Department of Clinical Microbiology, Hospital Universitario Príncipe de Asturias, Alcalá de Henares, Madrid, Spain; 3Unidad de Apoyo a Investigación de la Gerencia Integrada de Guadalajara, Guadalajara, Castilla-La Mancha, Spain; 4Department of Medicine and Medical Specialties, Alcalá University, Guadalajara, Castilla-La Mancha, Spain; 5Servicio de Prevencion, Alcalá University, Alcalá de Henares, Madrid, Spain
Correspondence: Ramón Pérez-Tanoira
Department of Clinical Microbiology, Hospital Universitario Príncipe de Asturias, Alcalá de Henares, Madrid, Spain
Tel/Fax +34 9187 8100
Email [email protected]
Purpose: Seroprevalence against SARS-CoV-2 within university systems is poorly studied, making evidence-based discussions of educational system reopening difficult. Moreover, few studies evaluate how antibodies against SARS-CoV-2 are maintained over time. We assessed serological response against the SARS-CoV-2 virus among our university students and staff.
Patients and Methods: In this prospective cohort study, seroprevalence was determined in 705 randomly selected volunteers, members of the Faculty of Medicine and Health Sciences of the University of Alcalá, using a chemiluminescent Siemens’ SARS-CoV-2 immunoassay for total antibodies. Positive samples were tested for IgG and IgM/IgA using VIRCLIA® MONOTEST (Vircell). A first analysis took place during June 2020, and in those testing positive, a determination of secondary outcomes was performed in November 2020.
Results: A total of 130 subjects showed anti-SARS-CoV-2 antibodies (18.5%, 95% CI, 15.8– 21.5%). Of these, IgM/IgA was positive in 27 and indeterminate in 19; IgG was positive in 118, indeterminate in 1. After 23 weeks, among 102 volunteers remeasured, IgG became undetectable in 6. Presence of antibodies was associated, in multivariable logistic regression, with exposure to infected patients (31.3%) [OR 1.84, 95% CI, 1.14– 2.96; P = 0.012], presence of COVID-19 symptoms (52.4%) [OR 6.88, 95% CI, 4.28– 11.06; P < 0.001], and confirmed earlier infection (82.9%) [OR 11.87, 95% CI, 4.26– 33.07; P < 0.001].
Conclusions: The faculty of medicine and health sciences personnel and students of our university showed a high infection rate for SARS-CoV-2 during 2020 associated with providing clinical care to infected patients. This emphasizes the importance of the performance of continuous surveillance methods of the most exposed health personnel, including health science students.
Keywords: seroprevalence, COVID-19, SARS-CoV-2, university, degree of health sciencies
Introduction
The ease of viral transmission of SARS-CoV-2 from symptomatic and asymptomatic cases in crowded and confined indoor spaces or indoor events is directly associated with higher infection rates. Viral loads in samples from asymptomatic or symptomatic cases have been similar among reports.1–6
Temporary measures to limit and delay COVID-19 infection through confinement and social distancing may – in addition to their immediate effects on health – have other unintended consequences. Rapid identification of coronavirus infectious disease 2019 (COVID-19) cases is crucial for outbreak containment and is challenging due to lack of pathognomonic symptoms.7 Prediction models that include rapidly ascertainable clinical findings and clinical tests can stratify at-risk populations for laboratory testing, isolation, and contact-tracing measures.7,8
RT-PCR, which allows detection of viral nucleic acids, has its sensitivity reduced by half in the second week of symptom evolution, if involving study of only nasopharyngeal samples.7–9
Due to the significant number of university staff and staff working or interning in our university hospitals, a high proportion of university staff, especially healthcare personnel, are at high risk of exposure. As with all educational institutions in Spain, the Faculty of Medicine and Health Sciences (FMHS) of the University of Alcalá (UAH) complied with the decision of the Spanish Government and suspended its operations from March to September 2020. To ensure the safe reopening of UAH institutional facilities, we attempted to assess the seroprevalence of SARS-CoV-2 among UAH members to estimate key epidemiological parameters, namely the epidemic growth rate and the fraction of asymptomatic cases, as well as the proportion of UAH members who may have remained susceptible to SARS-CoV-2 infection.
Following our analysis of 705 UAH members’ plasma samples collected randomly in June 2020, results, may to eventually aid UAH in its management of available human resources.
Materials and Methods
Study Population
Our cross-sectional study of antibody presence took place at the Faculty of Medicine and Health Sciences of the University of Alcalá in the Communities of Madrid and Castilla-La Mancha, Spain, during June 8–16, 2020. Our cohort study of antibody prevalence involved those volunteering individuals who were positive in the first analysis during November 23–30, 2020.
Stratified randomization was according to the various university bachelor’s degrees of the FMHS and according also to high or low risk of infection by SARS-CoV-2. Sample collection involved UAH members, comprising students of the FMHS for Physical Activity and Sports Sciences (PASS), Nursing-Alcalá, and the Guadalajara campus, Physiotherapy and Medicine, and the teaching and research staff (TRS) and administrative officers (AO).
We divided subjects into those at high or low risk of acquiring SARS-CoV-2 according to epidemiologically differentiated groups based on their contact with patients in health centres and hospitalization areas.
We recorded demographic variables (age and sex), time from onset of symptoms, and the presence of symptoms, history of prior contact with COVID-19 patients, and a questionnaire with clinical variables (immunosuppression, comorbidities, treatment with ACE inhibitors).
Sample Size
The overall population available (2019–20 academic year) was 654 TRP, 83 AO, 788 medical students, 404 nursing students on the Alcalá campus, 311 nursing students on the campus in Guadalajara, and 250 physical-therapy and 367 PASS students. These groups were each stratified into a low-risk and a high-risk population.
The minimum sample size of 678 (265 low risk, 413 high risk) assumed an a priori 10 and 18% IgG anti-SARS-CoV-2 seroprevalence in the low-risk and in the high-risk population, with a power of 80% and a ratio of 1:2.3 (low risk:high risk), a confidence in the estimate of 95%, and a maximum allowable error in the prevalence of 1%.
Statistical Analysis
Statistical analysis was performed with STATA software 16.0 (Stata Corporation, College Station, TX, USA). In the results, we expressed the qualitative variables with absolute frequencies and percentages, and the quantitative variables with medians and interquartile ranges. Univariable and multivariable logistic regression models were performed with goodness-of-fit assessed using Hosmer–Lemeshow statistics. The logistic regression model was adjusted by the most significant variables using the Stepwise criterion, with results expressed as odds ratio (OR) and 95% confidence intervals (95% CI) to determine the association of different variables with the presence of positive serology for SARS CoV-2 (dependent variable). The paired t test served to analyze the evolution of antibody titres in subjects with SARS-CoV-2. All contrasts were bilateral, and statistical significance was considered as p value less than 0.05.
Test Procedure
Peripheral blood was collected in Hospital Universitario Principe de Asturias, by venipuncture in BD vacutainers with spray-coated K2EDTA (BD Biosciences, San Jose, CA, USA) and centrifuged at 500× g for 20 min. Blood plasma was transferred in DNA-RNA-free cryovials (Corning, NY, NY, USA) and frozen at −20 °C until Ig measurement, performed no later than 20 days after blood collection.
We used the Atellica Solution Immunoassay & Clinical Chemistry Analyzers Anti-SARS-CoV-2 IM (Siemens Healthineers®, Erlangen, Germany), an electrochemiluminescence immunoassay (ECLIA) for the qualitative detection of total Igs (IgG, IgM, and IgA) generated against SARS-CoV-2 [Siemens SARS-CoV-2 Total (COV2T) assay (Siemens Healthineers, Frankfurt, Germany)]. Test results are generated by interpolating the ECLIA signal with that of a threshold generated during calibration. A cut-off index (COI) of 1.0 or higher classifies a plasma sample as “reactive” (ie, anti-SARS-CoV-2 positive).
Those workers whose total antibodies were positive underwent a COVID-19 VIRCLIA® MONOTEST (IgG or IgM+IgA). A COI of 1.5 or 0.3 higher classifies a plasma sample as “reactive” (ie, anti-SARS-CoV-2 positive) for IgG or IgM+IgA. Individuals positive for IgM + IgA received an offer of the possibility of having a PCR determination by Allplex 2019-nCoV (Seegene, Seoul, South Korea) in their nasopharyngeal exudate to rule out the status of asymptomatic carrier. One automatic extractor served to obtain viral RNA from clinical samples, the Hamilton Microlab Starlet (Hamilton Company, Bonaduz, Switzerland). RNA amplification was made with the Allplex SARS-CoV-2 assay (Seegene). The test was performed according to manufacturer’s instructions.
Ethical Approval
The study was conducted according to the ethical requirements established by the Declaration of Helsinki (2013). This study was reviewed and approved by the Ethics Committee of Hospital Universitario Príncipe de Asturias (Madrid). Written informed consent to participate in this study came from the participants.
Results
Of 705 individuals tested, 69.5% were women. The median ages were 20.5 years (IQR: 20.5–23.5) for FMHS and 53.5 (IQR 45.5–58.5) for TRS/AO. Of the total 705, 507 were FMHS (71.9%), 132 TRS (18.7%), and 66 AO (9.4%).
Students’ year of study was first year, 92 (18.4%), second, 112 (22.4%), third, 109 (21.8%), fourth, 109 (21.8%), fifth, 34 (6.8%), and sixth, 45 (9.4%). Subjects were stratified into low risk, 328 (46.5%), and high risk (53.5%) based on exposure to patients with confirmed COVID-19.
Among all participants, 254 (36%) reported known contact with COVID-19 cases, and 144 (20.4%) reported some symptoms indicative of COVID-19 in the previous 3 months. Previously confirmed infection was reported by 35 subjects (5%). For the various comorbidities see Table 1.
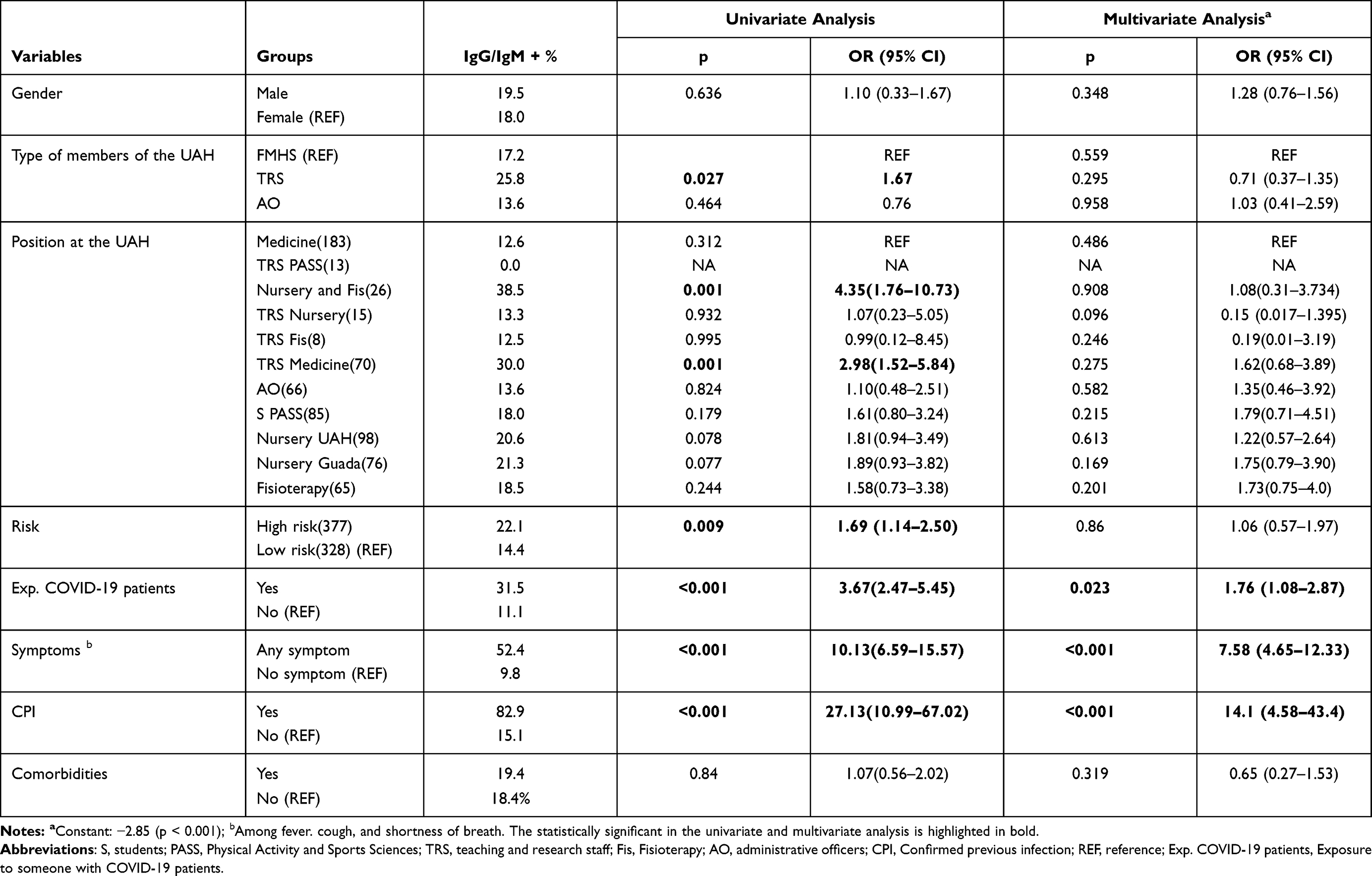 |
Table 1 Serological Assay Results and Epidemiological Characteristics of 705 Study Participants from the Faculty of Medicine and Health Sciences of the University of Alcalá, Madrid, Spain |
The prevalence of anti-SARS-CoV-2 (IgG/IgM+) was 18.4% (in 130) (95% CI 15.8–21.5%). Of these, IgG was positive in 118 (16.7%), and indeterminate in 1 (0.14%); IgM/IgA was indeterminate in 19 (14.6%), positive in 27 (20.8%), and negative in 84 (64.6%). RT-PCR was performed in individuals who presented a positive or indeterminate IgM/IgA (46 subjects), revealing only one volunteer with a positive result. The group with the highest prevalence of IgG/IgM+ Ab against SARS-CoV-2 were nursing and physiotherapy students (38.5%), and those in TRS medicine (30.0%).
Our statistical analysis revealed no significant associations between seroprevalence and age or gender. Table 2 shows that these original study volunteers’ position at UAH, their risk of infection, their known contact with COVID-19 cases, presence of symptoms indicative of COVID-19 in the previous 3 months, and confirmed previous infection were associated in the univariate analysis with the presence of anti-SARS-CoV-2 (IgG/IgM+). However, multivariate analysis showed that independently variables associated with past SARS-CoV-2 infection were known contact with COVID-19 patients, previous infection symptoms, and confirmed past infection.
 |
Table 2 Commorbidities of 705 Participants in the Faculty of Medicine and Health Sciences of the University of Alcalá, Madrid, Spain |
To follow overtime the antibody titres and neutralizing activity, we took a second blood sample 23 weeks after the first one from those individuals found to be positive (Figure 1). The antibody titers showed a clear decrease. A paired analysis showed a decrease in antibody response indicated by a lower signal-to-threshold ratio at the follow-up visit, in November, being the mean of IgG antibody titer was 5.93 (SD 4.23) units compared with the baseline visit that occurred in June, 8.44 (SD 5.25) (p < 0.001). It means a decrease of 2.91 points (95% CI: 1.94–3.88). The antibody titer decreased for the majority (>75%), being reduced >50% for 40 (39.2%) (Figure 1). Interestingly, in our assays, six (5.88%) became negative. No demographic or clinical variable was associated with an increase or decrease in antibody titre between June and November.
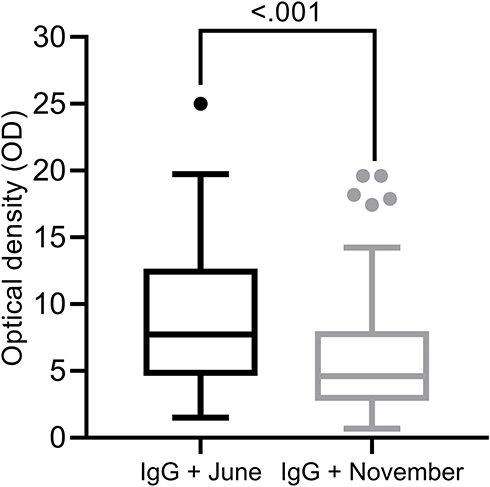 |
Figure 1 Serological profile follow-up over time. Samples from participants with IgG-positive serum at first blood sampling (IgG June) were reassessed with serum obtained 23 weeks later (IgG November). Whisker-plots summarizing test values for both tests (IgG June and IgG November). Paired-Samplets T-Test. Mean (SD) are shown in June: 8.84(5.25) and November: 5.93: (4.24), Median and interquartile range are respectively: 7.7 (IQR:4.6–12.7) and 4.4 (IQR:2.8–8.0). |
Thus, in the past few months, a serological-based survey of SARS-CoV-2 may run a risk of underestimating the number of formerly infected individuals.
The Hosmer–Lemeshow statistic for our model was 0.727. The multivariate model explained 35.5% of the positivite serology (Nagelkerke R2).
Discussion
The Covid pandemic has closed down Spanish Universities since March 2020; as of November 2020, most of them are running online-learning programs, and some partially remote. The impact of virus spread on the well-being and mental health of university students and staff has been well described on a global scale, and many medical students will have to compensate for those classes lost because of cancellation of hospital practice.10−12 The disastrous reopening of US universities in the middle of the pandemic in August 2020, driven by recommendations issued by the CDC, which did not include screening testing before admission, was a clear warning signal for Europe.13 All Spanish Universities have resumed their activities in the academic year 2020–21, adopting all the security measures recommended by the sanitary authorities; these measures have been taken with the intention of minimizing to the maximum all consequences of the spread of the infection in the school environment: classrooms, dormitories, and other off-campus premises. The symptomatic infection of students aged 18–34 years has been associated with a post-acute COVID-19 syndrome in up to a quarter of them and the transmission of the virus from asymptomatic students to more vulnerable and older staff of the University such as professors or other non-academic personnel can occur at an explosive pace.13,14
This serological survey occurred after the first epidemic wave and shows that as high as 18.5% of everyone studying or working at the University were infected. Only, medical students at the University of Copenhagen showed a higher anti-SARS-CoV-2 seropositivity (34.58%) in a study performed during October 2020.15 Our study showed a significantly higher proportion than that stated in the DIANCUSAL study, which was a Salamanca university population-based cross-sectional study conducted from July–October 2020, where the seroprevalence of all was 8.25% overall and was highest for students from the education campus (12.5%) and professors from the biomedical campus (12.6%), with significant differences among faculties (p = 0.006).16 Tuells et al found 2.64% of seroprevalence in a random sample selected from the University of Alicante during July 2020.17 The Kapodistrian University of Athens (NKUA), had an extremely low general seroprevalence of 0.83% with no significant difference from that of the students of School of Health Sciences.18 These data reflect the low prevalence of COVID-19 in Greece at the time of publication due to the early implementation of public health measures in that country at the beginning of the pandemic.
At the China University of Science and Technology, seroprevalence data, along with molecular testing, quarantine, and on-campus and off-campus restrictions, have been useful for scheduling a safe return to classrooms and containing the risk of transmission.19 That institution, located in a low-risk area for COVID-19 in China, had only 0.3% of the 9049 participants testing positive for antibodies. Comorbidities were rare (0.2%–1.5%) in this group, in contrast to our study population, who had up to 9.7%, probably due to assessment of a higher percentage of staff members who were older non-students.
Our high infection rate could be explained by many medical students and nurses having already had contact with COVID-19 patients (up to 36%) in hospitals and Health Centers, where the attack rate in healthcare workers was as high as 37%. The virus was widely disseminated in the community (up to 20%), as was shown in a nation-wide serosurvey.20–22 Although most of the students were released from hospital work at the beginning of the pandemic, many of them had, by that point, already been infected. It is very likely that there has been a common source of contagion with that of the general population, but also it is clear that there has also been a risk exposure, especially in the first days of the outbreak when the virus situation was not exactly known and HCW were not taking the appropriate protective measures.23
Our results concur well with the 15.8 and 19.9% of prevalence of SARS-CoV-2 infection among healthcare workers founded in Kasr Al-Aini University Hospital, Cairo University, and Hospital Universitario de Fuenlabrada, respectively.24,25 Reports from various countries show different seroprevalence of SARS-CoV2 patterns among healthcare workers (HCWs), with an 8.7% in the meta-analysis by Galanis et al, being higher in studies conducted in North America (12.7%) compared to those in Europe (8.5%), Africa (8.2%) and Asia (4%).26
Seroprevalence over time is the main indicator of the maintenance of specific antibodies against SARS-CoV-2. Our results were similar to those of other studies that showed a decline of median IgG antibody titers over time.17 The epidemiological impact of the decrease in seroprevalence over time in academic communities must be elucidated.
Several limitations of this study must be considered. It was carried out in a specific population, thus the extrapolation of the results cannot be applied directly to the general population. Anyway, we consider it representative of the university community and the findings were useful for decision-making during the reopening of the campus phase. Additionally, data were obtained through a self-report questionnaire completed by the participants. Finally, from our cohort, there are some patients who had already passed COVID-19, this may have slightly affected the results but other similar studies also included patients who had been diagnosed with the disease.17 However, the combination of both data sources has allowed us to have a more complete picture of the pandemic impact in our center, since there have been up to 15.1% of participants who have had a confirmed infection by a positive RT-PCR but have not seroconverted.
Conclusion
The infection rate for SARS-CoV-2 was very high in the faculty of Medicine and Health Sciences of our University. This prevalence has been significantly higher than general population. This emphasizes the importance of the performance of continuous surveillance methods of the most exposed health personnel, including health science students who may have closer contact with infected people, and not only based on the appearance of symptoms. These methods should include both antibody and viral detection methods to have a more realistic picture of the virus circulation in a certain population. In future pandemics, early identification and isolation of suspected cases and rapid implementation of infection control measures is essential to interrupt the spread the virus. Ongoing surveillance including serosurveillance plays a critical role in monitoring infection and transmission of SARS-CoV-2 in educational settings.
Acknowledgments
The authors thank Vice deans Helena Hernandez, Beatriz Muros, and Daniel Pecos, and the administrators Francisca Ibarro, Gema Sánchez, Soledad Pastor, Ana Martínez, and Laly Muñoz, all from the Faculty of Medicine and Health Sciences and the Prevention Service of the University of Alcala for their essential help in logistical tasks. We also thank Carolyn Brimley Norris, from the University of Helsinki Language Services for her help with the language of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Perera RA, Mok CK, Tsang OT, et al. Serological assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), March 2020. Euro Surveill. 2020;25:1.
2. Stadlbauer D, Amanat F, Chromikova V, et al. SARS-CoV-2 seroconversion in humans: a detailed protocol for a serological assay, antigen production, and test setup. Curr Protoc Microbiol. 2020;57:
3. Wang D, Yin Y, Hu C, et al. Clinical course and outcome of 107 patients infected with the novel coronavirus, SARS-CoV-2, discharged from two hospitals in Wuhan, China. Crit Care. 2020;24(1):24. doi:10.1186/s13054-019-2723-z
4. Nikpouraghdam M, Jalali Farahani A, Alishiri G, et al. Epidemiological characteristics of coronavirus disease 2019 (COVID-19) patients in Iran: a single center study. J Clin Virol. 2020;127:104378. doi:10.1016/j.jcv.2020.104378
5. Pan X, Chen D, Xia Y, et al. Asymptomatic cases in a family cluster with SARS-CoV-2 infection. Lancet Infect Dis. 2020;20:410–411. doi:10.1016/S1473-3099(20)30114-6
6. Huang L, Zhang X, Zhang X, et al. Rapid asymptomatic transmission of COVID-19 during the incubation period demonstrating strong infectivity in a cluster of youngsters aged 16-23 years outside Wuhan and characteristics of young patients with COVID-19: a prospective contact-tracing study. J Infect. 2020;80:e1–e13. doi:10.1016/j.jinf.2020.03.006
7. Sun Y, Koh V, Marimuthu K, et al. Epidemiological and clinical predictors of COVID-19. Clin Infect Dis. 2020;71(15):786–792. doi:10.1093/cid/ciaa322
8. Padoan A, Sciacovelli L, Basso D, et al. IgA-Ab response to spike glycoprotein of SARS-CoV-2 in patients with COVID-19: a longitudinal study. Clin Chim Acta. 2020;507:164–166. doi:10.1016/j.cca.2020.04.026
9. Yu X, Sun X, Cui P, et al. Epidemiological and clinical characteristics of 333 confirmed cases with coronavirus disease 2019 in Shanghai, China. Transbound Emerg Dis. 2020;67(4):1697–1707. doi:10.1111/tbed.13604
10. Rodríguez-Hidalgo AJ, Pantaleón Y, Dios I, Falla D. Fear of COVID-19, stress, and anxiety in university undergraduate students: a predictive model for depression. Front Psychol. 2020;11:3041.
11. Rodríguez-Rey R, Garrido-Hernansaiz H, Collado S. Psychological impact of COVID-19 in Spain: early data report. Psychol Trauma. 2020;12:550–552. doi:10.1037/tra0000943
12. Sahu P. Closure of universities due to Coronavirus Disease 2019 (COVID-19): impact on education and mental health of students and academic staff. Cureus. 2020;12:4.
13. Yamey G, Walensky RP. Covid-19: re-opening universities is high risk. BMJ. 2020;370:m3365. doi:10.1136/bmj.m3365
14. Tenforde MW. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate Health Care Systems Network — United States, March–June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(30):993–998. doi:10.15585/mmwr.mm6930e1
15. Madsen JR, Nielsen JPS, Fogh K, et al. Anti-SARS-CoV-2 seropositivity among medical students in Copenhagen. Open Forum Infect Dis. 2021;8(8):ofab273. PMID: 34423066; PMCID: PMC8374058. doi:10.1093/ofid/ofab273
16. Figueiredo-Campos P, Blankenhaus B, Mota C, et al. Seroprevalence of anti-SARS-CoV-2 antibodies in COVID-19 patients and healthy volunteers up to 6 months post disease onset. Eur J Immunol. 2020;50(12):2025–2040.
17. Tuells J, Egoavil CM, Pena Pardo MA, et al. Seroprevalence study and cross-sectional survey on COVID-19 for a plan to reopen the University of Alicante (Spain). Int J Environ Res Public Health. 2021;18:4. doi:10.3390/ijerph18041908
18. Tsitsilonis OE, Paraskevis D, Lianidou E, et al. Seroprevalence of antibodies against SARS-CoV-2 among the personnel and students of the National and Kapodistrian University of Athens, Greece: a preliminary report. Life (Basel). 2020;10:214.
19. Cai G, Luo S, Zheng X, et al. Safety of reopening universities and colleges using a combined strategy during coronavirus disease 2019 in China: cross sectional study. SSRN Electron J. 2020. doi:10.2139/ssrn.3696819
20. Lopez L, Nguyen T, Weber G, et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in the staff of a public school system in the Midwestern United States. PloS One. 2020;16(6):e0243676.
21. Pérez-García F, Pérez-Zapata A, Arcos N, et al. Severe acute respiratory coronavirus virus 2 (SARS-CoV-2) infection among hospital workers in a severely affected institution in Madrid, Spain: a surveillance cross-sectional study. Infect Control Hosp Epidemiol. 42:803–809.
22. Pollán M, Pérez-Gómez B, Pastor-Barriuso R, et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet. 2020;396:535–544.
23. Heinzerling A, Stuckey MJ, Scheuer T, et al. Transmission of COVID-19 to health care personnel during exposures to a hospitalized patient—Solano County, California, February 2020. MMWR Morb Mortal Wkly Rep. 2020;69(15):472–476. doi:10.15585/mmwr.mm6915e5
24. Musa S, Abdel Alem S, Amer K, et al. Prevalence of SARS-CoV-2 infection and dynamics of antibodies response among previously undiagnosed healthcare workers in a university hospital: a prospective cohort study. J Infect Public Health. 2021;14(10):1466–1473. doi:10.1016/j.jiph.2021.06.001
25. Garralda Fernandez J, Molero Vilches I, Bermejo Rodriguez A, et al. Impact of SARS-CoV-2 pandemic among health care workers in a secondary teaching hospital in Spain. PLoS One. 2021;16(1):e0245001. doi:10.1371/journal.pone.0245001
26. Galanis P, Vraka I, Fragkou D, Bilali A, Kaitelidou D. Seroprevalence of SARS-CoV-2 antibodies and associated factors in healthcare workers: a systematic review and meta-analysis. J Hosp Infect. 2021;108(February):120–134. doi:10.1016/j.jhin.2020.11.008
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.