")
Back to Journals » Cancer Management and Research » Volume 13
High Prevalence of Triple-Negative Breast Cancer in Southern Shaanxi Province, China
Authors Xing X, Fan Z, Gao Y, Liu Z
Received 1 December 2020
Accepted for publication 22 January 2021
Published 17 February 2021 Volume 2021:13 Pages 1609—1615
DOI https://doi.org/10.2147/CMAR.S295085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eileen O'Reilly
Xuemei Xing,1,* Zhigang Fan,2,* Yue Gao,3 Zheng Liu1,3
1Department of Clinical Laboratory, 3201 Hospital, Xi’an Jiaotong University Health Science Center, Hanzhong, Shaanxi, 723000, People’s Republic of China; 2Department of Oncology, 3201 Hospital, Xi’an Jiaotong University Health Science Center, Hanzhong, Shaanxi, 723000, People’s Republic of China; 3College of Medical Laboratory Science, Guilin Medical University, Guilin, Guangxi, 541004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheng Liu
Department of Clinical Laboratory, 3201 Hospital, Xi’an Jiaotong University Health Science Center, 783 Tianhan Ave, Hanzhong, Shaanxi, 723000, People’s Republic of China
Tel/Fax +86 916 2383201
Email [email protected]
Purpose: Describing the clinical features of patients with breast cancer in an area is important to provide the information for the local oncologist to make sound treatment plans. In this study, we explored the clinical features of breast cancer patients in Southern Shaanxi Province, China.
Patients and Methods: A total of 328 breast cancer patients between 2010 and 2015 were recruited at our hospital. Patients’ clinical information and the results of the histopathological examination were collected. Independent sample t-test and Cox regression were used to analyze the data.
Results: The peak age onset of these patients was between 45 and 50. At diagnosis, 8.23% of patients were at clinical stage 1 and 29.57% were triple-negative breast cancer subtype. High expression of Ki-67 in these patients was found associated with triple-negative breast cancer. The 5-year survival rate in these patients was 66.4%, and the survival rate in stage 1 and 2 patients (88.2%) was significantly higher than that in stage 3 and4 (57.4%).
Conclusion: We here reported the clinical features of patients with breast cancer in Southern Shaanxi Province, China. The breast cancer patients in Southern Shaanxi Province showed a unique clinical feature.
Keywords: 5-year survival rate, breast cancer, clinical features, triple-negative breast cancer
Introduction
Breast cancer is one of the most common cancers in women worldwide, and it is the leading cause of death in both developed and developing countries.1 Although the incidence rate of breast cancer is lower in Asian population compared with other races, there is an increasing trend in China over the past two decades.2 Environmental pollution is considered to be one of the main causes of breast cancer.3 Metals are ubiquitous in the environment from natural sources, industry, and fossil fuel combustion.4 Some metals, including mercury, cadmium, and lead have been judged carcinogenic in humans by the International Agency for Research on Cancer, but the mechanism of these chemicals causing breast cancer is unclear.5 One explanation is that these chemicals are traditionally defined as carcinogens, and some of them fall into the class of endocrine-disrupting compounds.6
In recent years, several biomarkers including estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor-2 (HER2), and proliferation marker Ki-67 have been used for prediction and treatment guidance of breast cancer.7 Usually, ER-positive patients will benefit from hormonal therapy. Overexpression of HER2 is associated with more aggressive tumor type and poor clinical outcome.8 Ki-67 is a nuclear protein associated with cell proliferation and used as a prognostic marker in many malignant tumors including breast cancer.9
Breast cancer can be divided into triple-negative breast cancer (TNBC) and non-TNBC. TNBC is defined by the lack of expression of hormone receptors (ER and PR) and low expression of HER2, and do not respond to hormonal or anti-HER2 therapies.10 Therefore, reporting the prevalence of breast cancer subtypes in an area will guide local oncologists to make an efficient treatment plan. In this study, we collected and analyzed the data of 328 breast cancer patients from Southern Shaanxi province, China, and reported the clinical feature of these breast cancer patients.
Patients and Methods
Patients
This retrospective study was conducted from 2010 to 2015 at 3201 hospital, Xi’an Jiaotong University Health Science Center, in Southern Shaanxi Province. A total of 328 patients were recruited. The medical information including age, tumor position, expression of ER and PR, expression of Ki-67, HER2 status and disease stage at diagnosis, etc. were recorded. Eighty-nine patients have available information of survival time during the follow-up. The study was approved by the Institutional Review Board of 3201 hospital. The informed consent was obtained from all patients. The procedures performed in this study involving human participants were in accordance with the Helsinki Declaration of 1975, as revised in 2008.
Histopathological Examination
The patients were grouped into four subtypes based on the expression of genetic markers. Tumor phenotypes were categorized as luminal A (ER+ and/or PR+/HER2-), luminal B (ER+ and/or PR+/HER2+), triple-negative (ER- and PR-/HER2-), and basal-like (ER-/PR-/HER2+). The patients were also divided into two groups with a commonly used Ki-67 expression value of 20% as the cutoff. Breast cancer is designated as T4d in the American Joint Committee on Cancer Tumor, Node, Metastasis (TNM) staging system as previously described.11
Patients were examined at our hospital and the clinical characteristics including histology information, tumor size, axillary lymph node metastasis, pathological tumor-node-metastasis staging, ER, PR, HER-2 status, and Ki-67 expression level were collected. Tumor specimens were processed within 30 minutes from surgery for pathology testing. Tumor tissues were fixed in 10% neutral formaldehyde for 6~48 hours, and then embedded in paraffin and cut into 5 μm slices. Tumors were graded as 1, 2, and 3 based on the information of three parameters: the formation of nuclear pleomorphism, the formation of tubules, and the number of mitoses. The scores from the three parameters were summed up and ranged from 3 to 9: 3–5 for grade 1 with well-differentiated tumor; 6–7 for grade 2 with moderately differentiated tumor; and 8–9 for grade 3 with the poorly differentiated tumor. HER-2 status was decided by immunohistochemistry staining, scores 0 and 1 were considered as negative, 2 and 3 were considered as positive. For ER and PR scoring, the breast cancer specimens with >1% positively staining cells by immunohistochemistry were considered ER or PR positive. Ki-67 proliferation level was determined by the percentage of positive cells among the tested cells. For each patient, the pathological testing results were reviewed by two qualified pathologists for interpretation and diagnosis.
Treatment
The treatment methods include surgical resection, chemotherapy, radiotherapy, and endocrine therapy. Most of the time, the treatment plan is the result of communication between doctors and patients based on the development of the tumor, the patient’s economy, and the patient’s reasons.
Statistical Analysis
Data are reported as the mean±SD. An independent sample t-test was used to assess the difference between different disease subtypes. Cox regression was used for survival analysis. R version 3.0.2 was used for all the statistical analyses in this study.
Results
The Characteristics of Patients
The average age of the breast cancer patients is 50.49 in this study. Of the patients, 85.64% have an age-onset between 35 and 65 years old, and the peak age of breast cancer is from 45 to 50 years old (Table 1). The histopathology classification showed about 97 (29.57%) breast cancer patients are TNBC subtype, followed by luminal B subtype (32.01%). Luminal A and HER2 positive subtypes share the rest of the patients. Of the patients, 40.24% were at T1 stage. Of the patients, 32.93% were at T2 stage. 15.55% and 11.28% of the patients were at T3 and T4, respectively. One hundred and forty-eight patients were at N0, 119 patients at N1, 76 and 22 patients were at N2 and N3, respectively (Table 1).
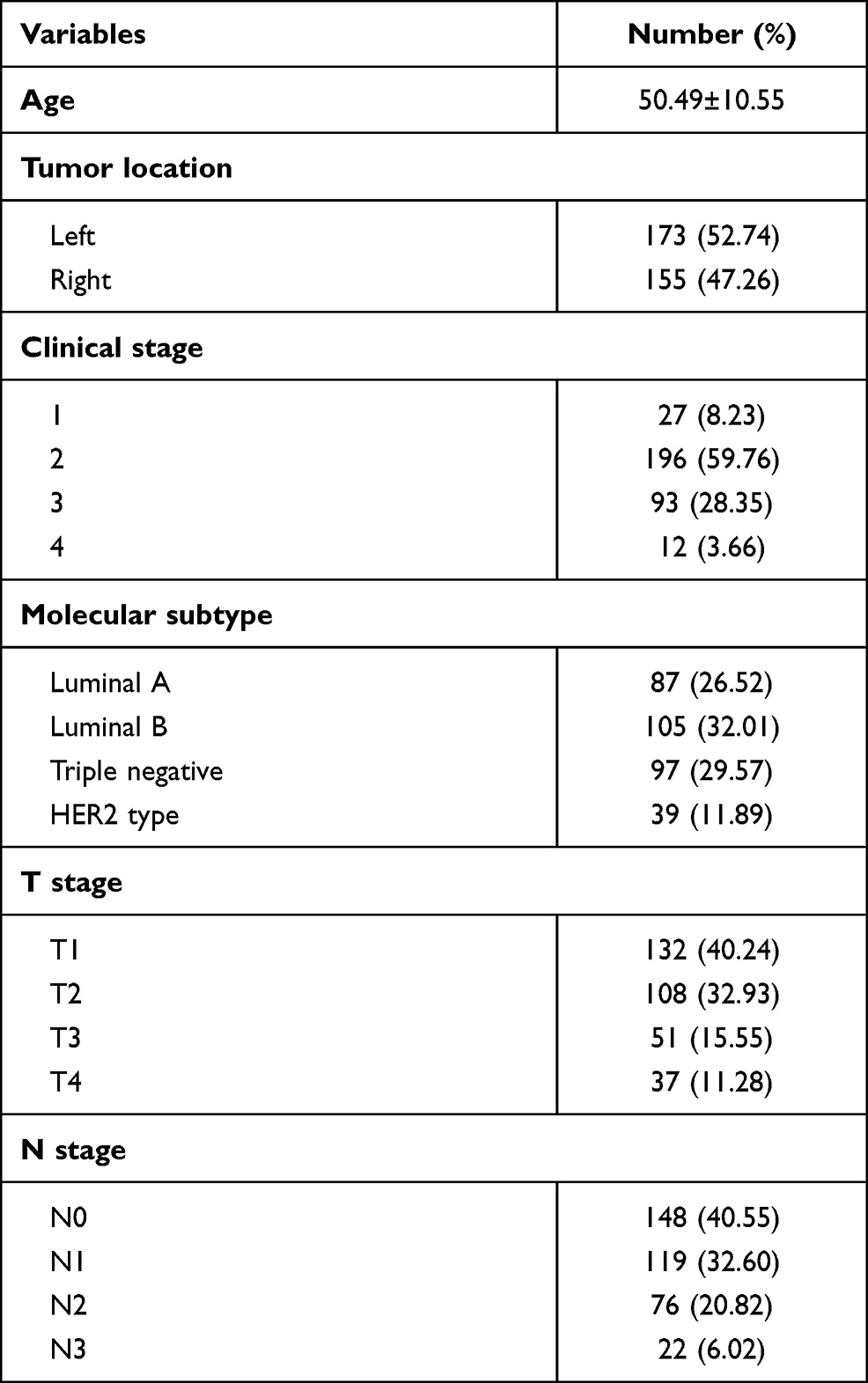 |
Table 1 Demographic Characteristics of Breast Cancer Patients Included in Study |
Clinical Characteristics and Breast Cancer Subtypes
We further tested the relationship between clinical characteristics and breast cancer subtypes. There were 159 and 169 patients in age-onset “<50” and “≥50” groups. Of the patients, 23.27% and 55.97% were Luminal B and TNBC subtype in the “<50” group, compared with 10.65% and 69.82% for the two subtypes in the “≥50” group (Table 2). The results showed there was a significant difference in subtypes distribution between the early and late age-onset group (P value=0.012). The average value of Ki-67 expression among the patients was 45.11±25.90% (range 1–90%). Of the patients, 61.05% and 11.58% in the low Ki-67 expression group are luminal A and luminal B, respectively. Of the patients, 21.05% are triple-negative and 7.22% for HER2 type. In high Ki-67 expression group, only 19.31% of the patients are luminal subtype and 76.82% for triple-negative, and 3.86% for HER2 type (Table 2). The statistical test produced a P value less than 2.1×10−15, which displayed a strong association between Ki-67 expression level and breast cancer subtypes. We also detected an association between T stage and breast cancer subtype (P value=0.008).
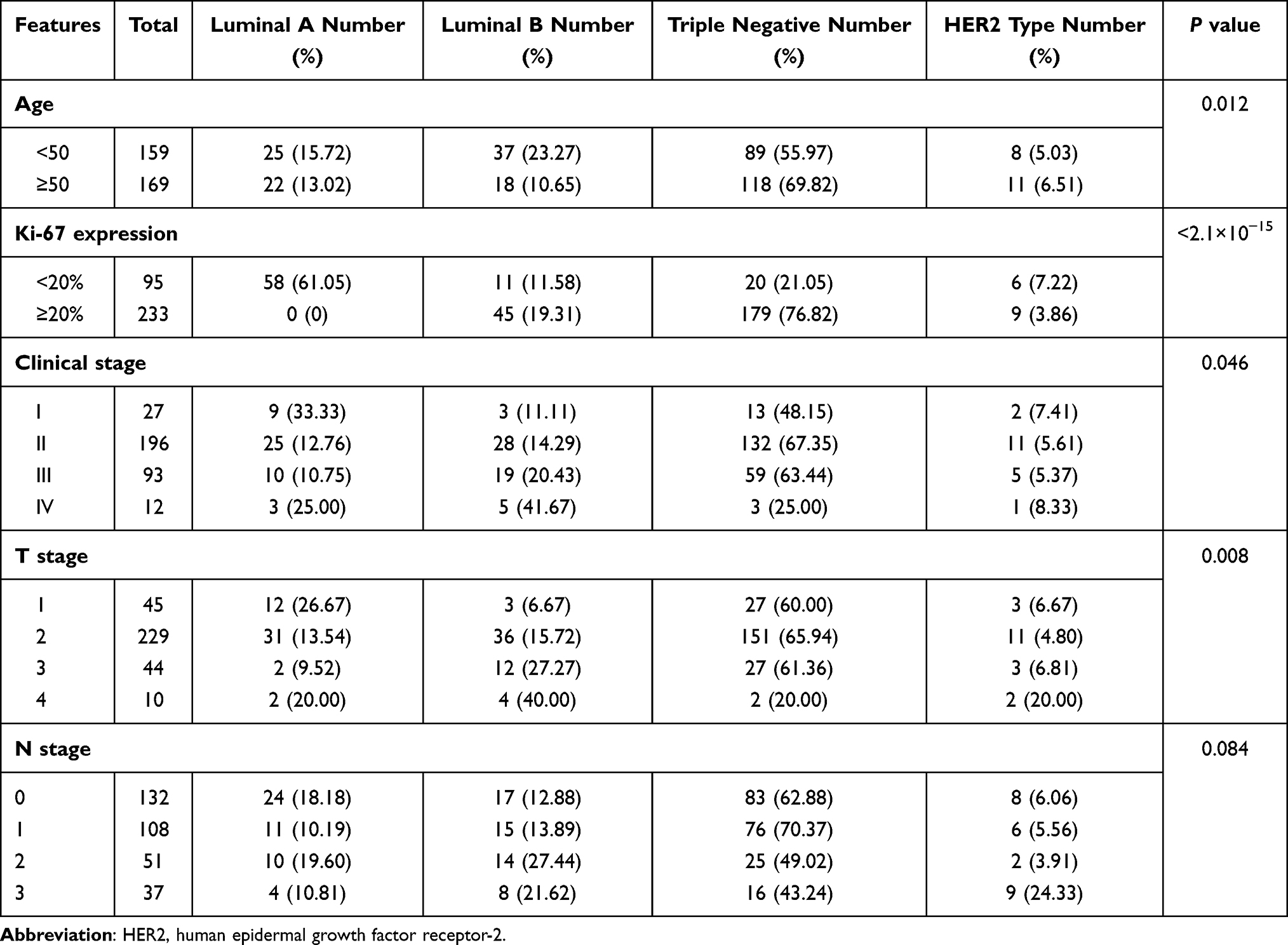 |
Table 2 Breast Cancer Subtypes in Our Patients |
The Correlation Between ER/PR Status and Ki-67 Expression Level
We further studied the correlation between ER/PR status and Ki-67 expression level as ER/PR status was important prognostic marker in breast cancer subtype classification. Ninety-seven patients were ER+ and/or PR+ group and 206 patients in ER-/PR-group (Table 3). The average Ki-67 expression value in ER+ and/or PR+ group was 19.48% and 57.38% in ER-/PR-group (Table 3). There was a significant difference in Ki-67 expression between ER+ and/or PR+ and ER-/PR-group (P value < 2e−16). This result suggested a strong relationship between the level of Ki-67 expression and ER/PR status.
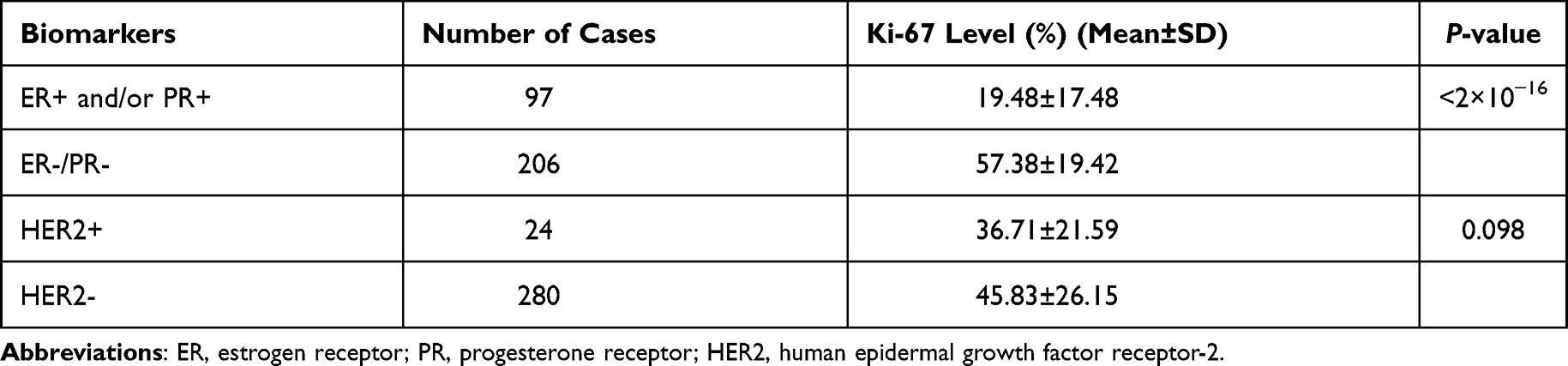 |
Table 3 Ki-67 Expression Between Groups |
The Correlation Between HER2 and ER/PR Status
HER2 and ER, PR are all important prognostic markers for breast cancer diagnosis. We investigated the correlation between HER2 and ER/PR status. Eighteen patients were HER2 positive and 310 were HER2 negative. Among the patients with HER2 negativity status, 66.2% of them were ER-negative and 71.9% of them were PR negative. There was a strong correlation between HER2 negativity and ER/PR negativity. The statistical test produced a P value of 1.80×10−4 (Table 4).
 |
Table 4 Correlation Between HER2 and ER/PR Status |
The Treatment and 5-Year Survival Rate
In Table 5, most patients received radical mastectomy (94.10%). Of the patients, 74.72% and 34.95% received chemotherapy and radiotherapy. Of patients, 29.48% received endocrine therapy for 2–5 years when their positive expression of ER was >5%. The 5-year survival rate in breast cancer patients is 66.4% (95% CI=(0.924, 1.00)). We further stratified the patients into stage 1 and 2 and stage 3 and 4. Five-year survival rate in stage 1 and 2 patients was 88.2% (95% CI= (0.95, 1.00)) and 57.4% (95% CI= (0.77,1.00)) in stage 3 and 4 patients. The survival curve between these two groups is significantly different (P value =3.84×10−5).
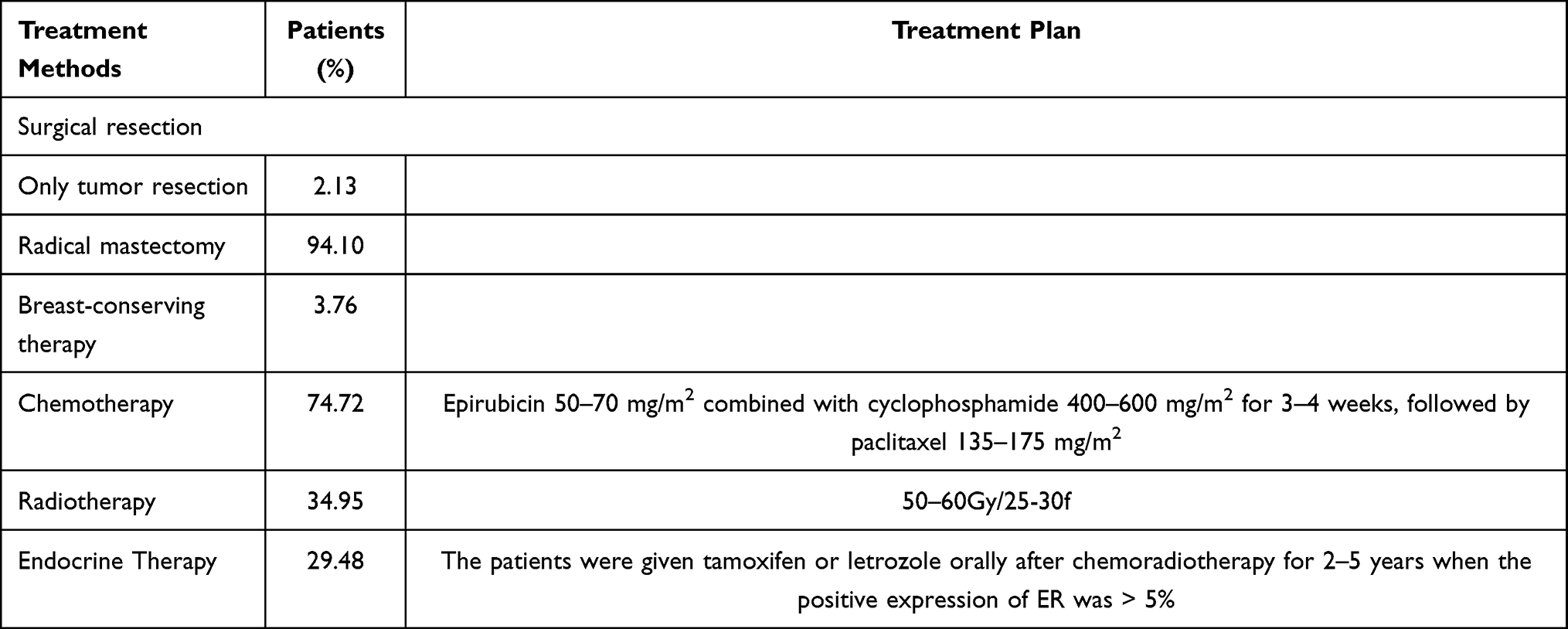 |
Table 5 The Treatment Methods and Plan for These Patients |
Discussion
TNBC usually accounts for 15–20% of breast cancer.12 It tends to more aggressive and is associated with a poor prognosis and high recurrence rate.13 In United States, TNBC could account for 39% of breast cancer cases in premenopausal African-American women.14 In Hong Kong and Southern China, only 13.4% of breast cancer patients was TNBC.15 A study from Shanghai showed that the prevalence of TNBC in breast cancer was 12.9%.16 These results indicate that the proportion of TNBC in different populations is very different. In our report, the result is quite different from other studies, and we found that a high proportion of patients was TNBC subtype in Southern Shaanxi province. Southern Shaanxi province is a special area in China. It is located in a relatively closed environment in Qinling Mountains. The previous report has shown that high soil selenium concentrations were found in this area where soil selenium concentrations could be >20 mg/kg.17 Some studies hypothesized that selenium deficiency may be associated with an increased risk of breast cancer.18 However, in the United States, the researchers found that selenium intake is not associated with incident breast cancer.19 These conflicting findings reveal that selenium plays a complex role in the development of breast cancer, showing that the relationship between selenium intake and the risk of breast cancer is unclear. Another report revealed that soil cadmium and mercury pollution was detected in the production of tea in Southern Shaanxi Province.20 Dietary mercury and cadmium were demonstrated to be associated with a higher risk of breast cancer.18,21 Methylmercury could promote breast cancer cell proliferation by stimulating estrogen.22 Similarly, cadmium also has been shown to demonstrate estrogen-like activity, which is known to increase breast cancer risk.23 Unfortunately, few studies have focused on the relationship between carcinogenic properties of these metals and TNBC subtype in breast cancer patients. The etiology of a high proportion of TNBC in breast cancer patients in Southern Shaanxi Province needs to be further investigated.
In this study, there was no difference in peak age of breast cancer between our patients and other regions of China.24 Early detection of breast cancer is very important for patients as treatment is often more effective at an early stage. Only 8.23% of the diagnosed patients are stage 1 in this study. Of the patients, 32.01% are stage 3 and 4. This distribution of disease stage at initial diagnosis is similar to that (13.5%) from Renmin Hospital in Wuhan, China.25 Compared with 78% of newly diagnosed cases were stage 1 in Japan, this number was very low in China, which suggested a lack of breast cancer early detection program in China.26 That was easy to understand that the 5-year overall survival rate in this study was 66.4%, lower than 76.5% from China, 87.0% from Japan, and 88% from the United States.27 In our report, we detected a higher proportion of TNBC in Ki-67 expression. Ki-67 is a nuclear antigen present in fast proliferating cells that have been widely used in cancer diagnosis.28 Studies showed a high level of Ki-67 was associated with severity of tumor and poor prognosis in breast cancer and Ki-67 could be used to indicate different prognosis and treatment in TNBC patients.29
Conclusion
In conclusion, we here reported that 29.57% of the breast cancer patients in Southern Shaanxi Province were TNBC, which showed a unique clinical feature in these patients. Our study also provides evidence that the TNBC subtype was associated with high expression of Ki-67, which showed a similar pattern of clinical characteristics with other regions of China.
Acknowledgments
This work was supported by Key Research and Development Program of Shaanxi Province (2017ZDXM-SF-067), Natural Science Foundation of Guangxi Zhuang Autonomous Region (2018JJA140045/2018GXNSFAA281048) and Guangxi Science and Technology Base and Special Fund for Talents (2018AD19267/AD19110161).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tao Z, Shi A, Lu C, Song T, Zhang Z, Zhao J. Breast cancer: epidemiology and etiology. Cell Biochem Biophys. 2015;72(2):333–338. doi:10.1007/s12013-014-0459-6
2. Wang F, Yu ZG. Current status of breast cancer prevention in China. Chronic Dis Transl Med. 2015;1(1):2–8. doi:10.1016/j.cdtm.2015.02.003
3. Koual M, Tomkiewicz C, Cano-Sancho G, Antignac JP, Bats AS, Coumoul X. Environmental chemicals, breast cancer progression and drug resistance. Environ Health. 2020;19(1):117. doi:10.1186/s12940-020-00670-2
4. Hiatt RA, Brody JG. Environmental determinants of breast cancer. Annu Rev Public Health. 2018;39(1):113–133. doi:10.1146/annurev-publhealth-040617-014101
5. Hu A, Li L, Hu C, et al. Serum concentrations of 15 elements among helicobacter pylori-infected residents from Lujiang County with high gastric cancer risk in Eastern China. Biol Trace Elem Res. 2018;186(1):21–30. doi:10.1007/s12011-018-1283-4
6. Gray JM, Rasanayagam S, Engel C, Rizzo J. State of the evidence 2017: an update on the connection between breast cancer and the environment. Environ Health. 2017;16:94.
7. Van Asten K, Slembrouck L, Olbrecht S, et al. Prognostic value of the progesterone receptor by subtype in patients with estrogen receptor-positive, HER2 negative breast cancer. Oncologist. 2019;24(2):165–171. doi:10.1634/theoncologist.2018-0176
8. Hart CD, Migliaccio I, Malorni L, Guarducci C, Biganzoli L, Di Leo A. Challenges in the management of advanced, ER-positive, HER2-negative breast cancer. Nat Rev Clin Oncol. 2015;12(9):541–552. doi:10.1038/nrclinonc.2015.99
9. Soliman NA, Yussif SM. Ki-67 as a prognostic marker according to breast cancer molecular subtype. Cancer Biol Med. 2016;13(4):496–504. doi:10.20892/j.issn.2095-3941.2016.0066
10. Shi J, Liu F, Song Y. Progress: targeted therapy, immunotherapy, and new chemotherapy strategies in advanced triple-negative breast cancer. Cancer Manag Res. 2020;12:9375–9387. doi:10.2147/CMAR.S272685
11. Sawaki M, Shien T, Iwata H. TNM classification of malignant tumors (breast cancer study group). Jpn J Clin Oncol. 2019;49(3):228–231. doi:10.1093/jjco/hyy182
12. Nakai K, Hung MC, Yamaguchi H. A perspective on anti-EGFR therapies targeting triple-negative breast cancer. Am J Cancer Res. 2016;6(8):1609–1623.
13. Wahba HA, El-Hadaad HA. Current approaches in treatment of triple-negative breast cancer. Cancer Biol Med. 2015;12(2):106–116. doi:10.7497/j.issn.2095-3941.2015.0030
14. Sturtz LA, Melley J, Mamula K, Shriver CD, Ellsworth RE. Outcome disparities in African American women with triple negative breast cancer: a comparison of epidemiological and molecular factors between African American and Caucasian women with triple negative breast cancer. BMC Cancer. 2014;14(1):62. doi:10.1186/1471-2407-14-62
15. Kwong A, Mang OW, Wong CH, Chau WW, Law SC. Hong Kong breast cancer research group. Breast cancer in Hong Kong, Southern China: the first population-based analysis of epidemiological characteristics, stage-specific, cancer-specific, and disease-free survival in breast cancer patients: 1997–2001. Ann Surg Oncol. 2011;18(11):3072–3078. doi:10.1245/s10434-011-1960-4
16. Su Y, Zheng Y, Zheng W, et al. Distinct distribution and prognostic significance of molecular subtypes of breast cancer in Chinese women: a population-based cohort study. BMC Cancer. 2011;11(1):292. doi:10.1186/1471-2407-11-292
17. Du Y, Luo K, Ni R, Hussain R. Selenium and hazardous elements distribution in plant-soil-water system and human health risk assessment of Lower Cambrian, Southern Shaanxi, China. Environ Geochem Health. 2018;40(5):2049–2069. doi:10.1007/s10653-018-0082-3
18. Cann SA, van Netten JP, van Netten C. Hypothesis: iodine, selenium and the development of breast cancer. Cancer Causes Control. 2000;11(2):121–127. doi:10.1023/A:1008925301459
19. Guo D, Hendryx M, Liang X, et al. Association between selenium intake and breast cancer risk: results from the women’s health initiative. Breast Cancer Res Treat. 2020;183(1):217–226. doi:10.1007/s10549-020-05764-6
20. Zhao ZP, Yan S, Duan M, et al. Assessing heavy metal pollution and potential ecological risk of tea plantation soils. Int J Agric Biol Eng. 2019;12:185–191.
21. Peng L, Huang Y, Zhang J, et al. Cadmium exposure and the risk of breast cancer in Chaoshan population of southeast China. Environ Sci Pollut Res Int. 2015;22(24):19870–19878. doi:10.1007/s11356-015-5212-1
22. Gaudet HM, Christensen E, Conn B, Morrow S, Cressey L, Benoit J. Methylmercury promotes breast cancer cell proliferation. Toxicol Rep. 2018;5:579–584. doi:10.1016/j.toxrep.2018.05.002
23. McElroy JA, Shafer MM, Trentham-Dietz A, Hampton JM, Newcomb PA. Cadmium exposure and breast cancer risk. J Natl Cancer Inst. 2006;98(12):869–873. doi:10.1093/jnci/djj233
24. Chen C, Sun S, Yuan JP, et al. Characteristics of breast cancer in Central China, literature review and comparison with USA. Breast. 2016;30:208–213. doi:10.1016/j.breast.2016.01.004
25. Chen XS, Nie XQ, Chen CM, et al. Weekly paclitaxel plus carboplatin is an effective nonanthracycline-containing regimen as neoadjuvant chemotherapy for breast cancer. Ann Oncol. 2010;21(5):961–967. doi:10.1093/annonc/mdq041
26. Ohuchi N, Suzuki A, Sobue T, et al. Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): a randomised controlled trial. Lancet. 2016;387(10016):341–348. doi:10.1016/S0140-6736(15)00774-6
27. Leong SP, Shen ZZ, Liu TJ, et al. Is breast cancer the same disease in Asian and Western countries? World J Surg. 2010;34(10):2308–2324. doi:10.1007/s00268-010-0683-1
28. Wu Q, Ma G, Deng Y, et al. Prognostic value of ki-67 in patients with resected triple-negative breast cancer: a meta-analysis. Front Oncol. 2019;9:1068. doi:10.3389/fonc.2019.01068
29. Zhu X, Chen L, Huang B, et al. The prognostic and predictive potential of Ki-67 in triple-negative breast cancer. Sci Rep. 2020;10(1):225. doi:10.1038/s41598-019-57094-3
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.