")
Back to Journals » Cancer Management and Research » Volume 11
High expression of dedicator of cytokinesis 1 adversely influences the prognosis of acute myeloid leukemia patients undergoing allogeneic hematopoietic stem cell transplantation
Authors Zhang G, Zhang J , Yang X, Zhang X, Yang S, Wang J, Hu K, Shi J, Ke X, Fu L
Received 31 October 2018
Accepted for publication 27 February 2019
Published 11 April 2019 Volume 2019:11 Pages 3053—3060
DOI https://doi.org/10.2147/CMAR.S192845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Gaoqi Zhang,1 Jilei Zhang,2 Xinrui Yang,1 Xinpei Zhang,1 Siyuan Yang,1 Jing Wang,1 Kai Hu,1 Jinlong Shi,3,4 Xiaoyan Ke,1 Lin Fu1
1Department of Hematology and Lymphoma Research Center, Peking University, Third Hospital, Beijing, People’s Republic of China; 2Department of Otolaryngology, Peking University People’s Hospital, Beijing 100044, People’s Republic of China; 3Department of Biomedical Engineering, Chinese PLA General Hospital, Beijing 100853, People’s Republic of China; 4Department of Medical Big Data, Chinese PLA General Hospital, Beijing 100853, People’s Republic of China
Background: Overexpression of dedicator of cytokinesis 1 (DOCK1) has been confirmed as an unfavorable prognostic marker in acute myeloid leukemia (AML).
Purpose: This study is to explore the clinical implications of DOCK1 on AML patients underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT).
Patients and methods: We analyzed 71 de novo AML patients treated with allo-HSCT and divided them into two groups (DOCK1high, vs DOCK1low,) by the median expression level of DOCK1.
Results: High DOCK1 expression was associated with older age (P=0.019), wild-type CEBPA (P=0.002), IDH1/2 mutations (P=0.010) and RUNX1 mutation (P=0.005). Univariate analyses showed that DOCK1high, and RUNX1 mutation were associated with shorter OS (P<0.001, P=0.024). Multivariate analysis confirmed the negative effect of high DOCK1 level on overall survival (P=0.010).
Conclusion: Our results demonstrate that in AML patients who received allo-HSCT, high DOCK1 expression might have a persistent negative prognostic impact post-transplant.
Keywords: acute myeloid leukemia, allo-HSCT, DOCK1, prognosis
Background
Acute myeloid leukemia (AML) is a malignant disease of hemopoietic stem cells. It is characterized by clonal expansion of differentiated blasts of myeloid lineage.1 The current version of the WHO classification provides guidance on AML diagnosis, treatment and prognostication.2 The outcome of AML patients is heterogeneous, depending on both patient- and disease-related risk factors. Genomic abnormalities account for at least 60% of the variables in AML prognostication.3 For example, FLT3-ITD has a clear correlation with a poor outcome, while mutations in NPM1 bode a particularly better prognosis.4 The presence of biallelic mutations of CEBPA is an independent factor for favorable outcome in AML patients.5 A recent meta-analysis indicated that IDH1 mutations confer a poorer survival,6 so do genetic aberrations of TP537 or RUNX1.8 Genetic factors are incorporated to treatment design because they determine disease sensitivity to treatment as well as the tolerability of therapy.
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) has a strong anti-leukemic effect and it is a commonly used option for AML post-remission consolidation therapy.9 It especially improves the outcomes of patients with poor-risk or intermediate-risk disease.10 Although allo-HSCT can decrease the frequency of relapse and prolong survival, many patients still relapse post-transplant.1 An increasing number of research focusing on post-transplant relapse have pointed out several factors including WBC count at diagnosis,11 cytogenetic risk status,12 initial induction response,13 and most importantly, minimal residual disease (MRD) status at the time of transplantation.14 In the MRD-negative patients who still experience relapse, genetic alterations might play an even bigger role in leukemogenesis and prognostication.15
The dedicator of cytokinesis 1 (DOCK) family is a class of the atypical Rho guanine nucleotide exchange factors (GEFs).16 As a major Rac GEF, DOCK proteins are involved in various cellular processes, such as cell adhesion, cell migration, actin cytoskeleton, and tumorigenesis.17,18 Sze-Hwei Lee, et al, have discovered that high expression of DOCK1 implied poor prognosis in AML patients.19 However, it is yet to be determined whether the expression level of DOCK1 has prognostic value in AML patients undergoing allo-HSCT. In this study, we will focus on the prognostic significance of DOCK1 in a cohort of AML patients undergoing allo-HSCT and discuss its clinical implications.
Patients and methods
Patients
A group of 71 de novo AML patients (41 males, 30 females) from The Cancer Genome Atlas (TCGA) (
Statistical analysis
Descriptive statistics were used to summarize demographics, clinical and molecular information. Continuous variables were described in the form of the median with range. The Mann–Whitney U test was used for comparing two groups of numeric variables, and chi-square analysis was applied to the comparison of categorical variables. The clinical endpoint of this study was overall survival (OS), which was defined as the time from diagnosis to death or was censored at the last follow-up. The OS rate was calculated using the Kaplan–Meier method, and the survival curves were plotted. The log-rank test was used to analyze significant differences between survival distributions. A cox proportional hazard model was applied to univariable and multivariable analyses to assess possible prognostic factors. The relapse-free survival (RFS) rate, defined as the time from the date of diagnosis to relapse, was also analyzed. The level of statistical significance was set at P<0.05 for all analyses. SPSS software version 20.0 and GraphPad Prism software version 6.0 were used for all the statistical analyses.
Results
Association of DOCK1 expression level with demographic characteristics and prognostic factors
The total of 71 patients was divided into two groups (DOCK1high group and DOCK1low group) based on the median DOCK1 expression level. High DOCK1 expressers were associated with older age (≥60, P=0.019), with an average age of 55 compared with 51 in DOCK1low group (P=0.010). Patients with higher DOCK1 expression had a lower percentage of peripheral blood (PB) blasts (P=0.010) and fewer IDH1/2 mutations (P=0.010). FLT3-ITD appeared more frequently in DOCK1high patients (P=0.051). All the patients with CEBPA double mutation were in DOCK1low group while RUNX1 mutations were observed only in DOCK1high group (P=0.005). There were no differences in other clinical factors including WBC count, FAB subtypes and karyotypes, as well as molecular prognostic features like TP53, MLL-PTD and NPM1 mutations. As for the ratios of relapse, no differences were found between the two groups. There was no difference between the two groups on the transplant status. The summary of the association between DOCK1 expression level and the demographic and prognostic factors is displayed in Table 1.
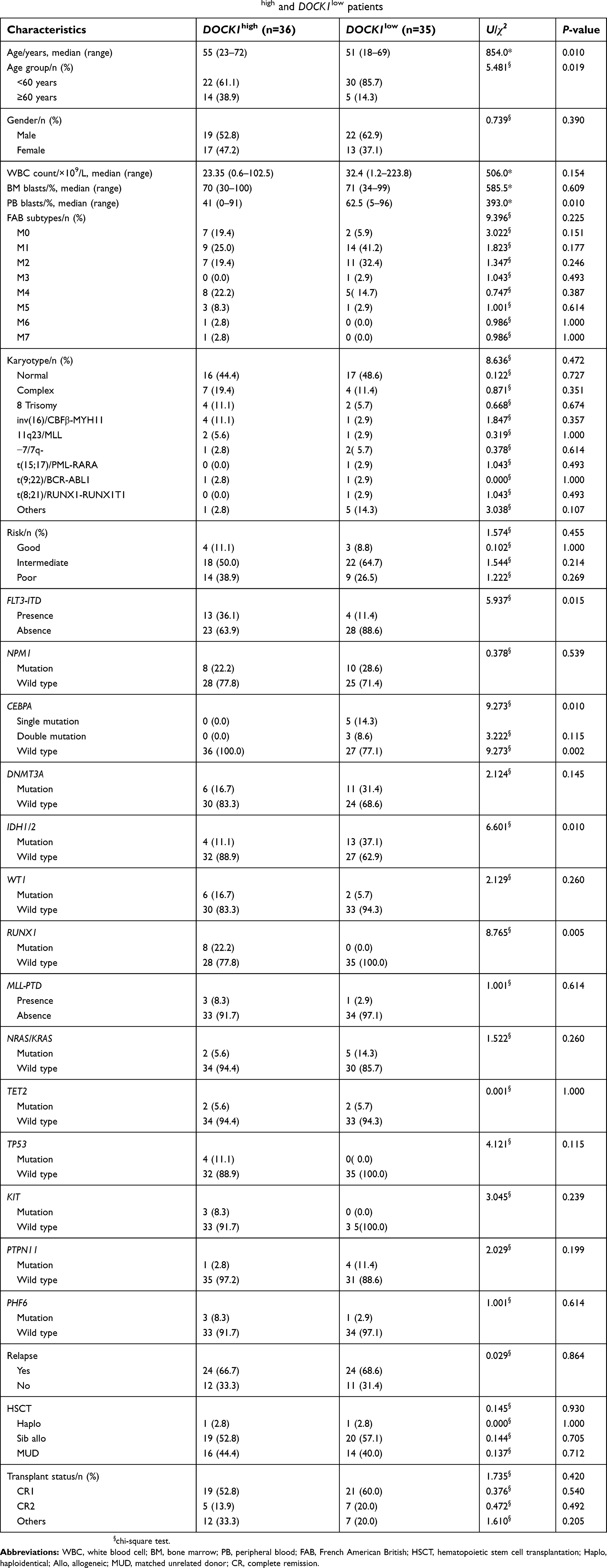 | Table 1 Clinical and molecular characteristics of DOCK1high and DOCK1low patients |
Higher expression level of DOCK1 indicated shorter OS in AML patients undergoing allo-HSCT
Univariate and multivariate analysis using cox proportional hazard models synthesized possible prognostic elements including DOCK1 expression level (high vs low), age (≥60 vs <60 years), WBC (≥30 vs <30×109/L), risk stratification (poor vs non-poor) and genetic mutation like FLT3-ITD, NPM1, DNMT3A, CEBPA double mutation, IDH1 and RUNX1. The results are shown in Tables 2 and 3.
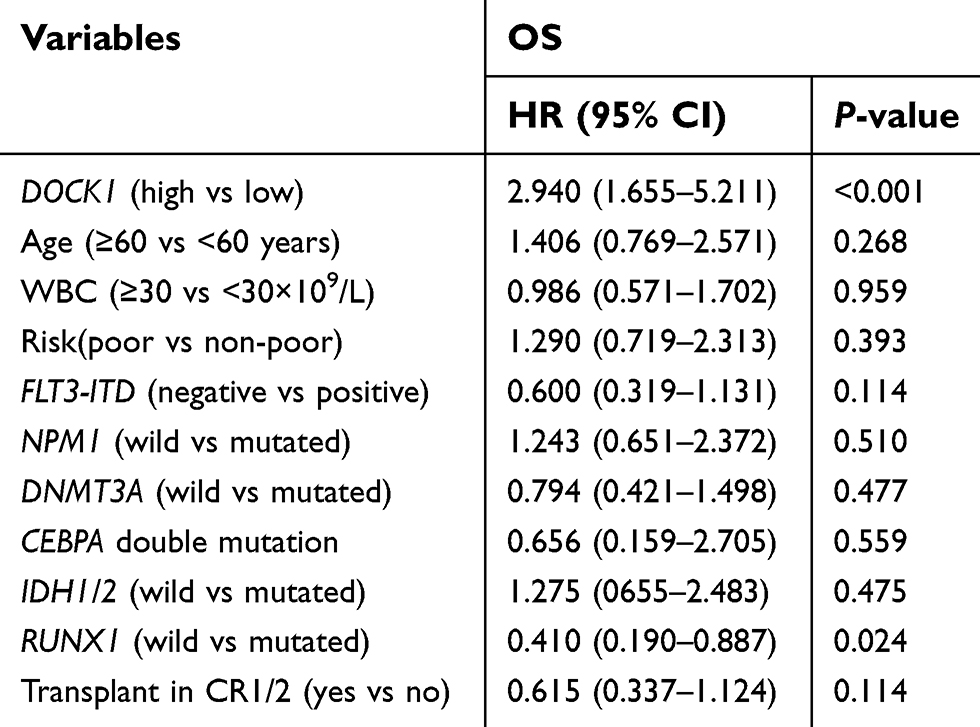 | Table 2 Univariate analysis for OS |
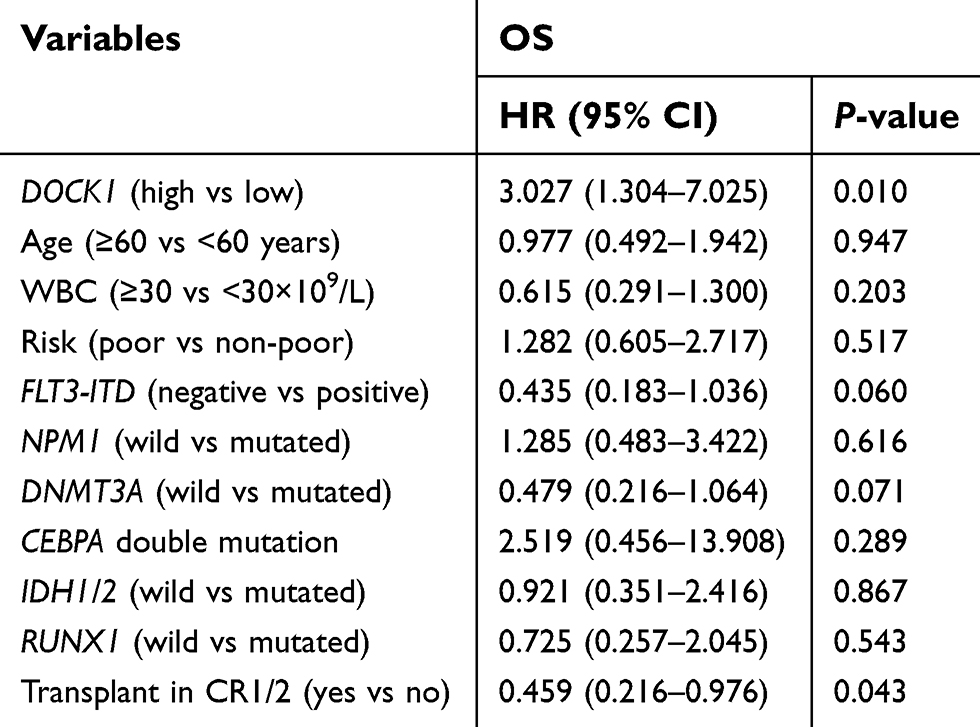 | Table 3 Multivariate analysis for OS |
Univariate analysis and Kaplan–Meier survival curve both revealed that patients undergoing allo-HSCT in DOCK1high group had a shorter OS (Table 2, Figure 1, both P<0.001). Mutations in RUNX1 also had an adverse effect on OS (Table 2, P=0.024). The result of multivariate analysis further demonstrated the unfavorable effect of high DOCK1 expression (Table 3, P=0.010). Multivariate analysis also showed that patients who received a transplant in CR1/2 had longer OS (Table 3, P=0.043). RUNX1, FLT3-ITD and NPM1 were not correlated with the OS in AML patients undergoing allo-HSCT in our cohort. The results of univariate and multivariate analysis of RFS, as well as the Kaplan-Meier curve, were provided in Tables S1and S2 and Figure S1 in the Supplementary Appendix.
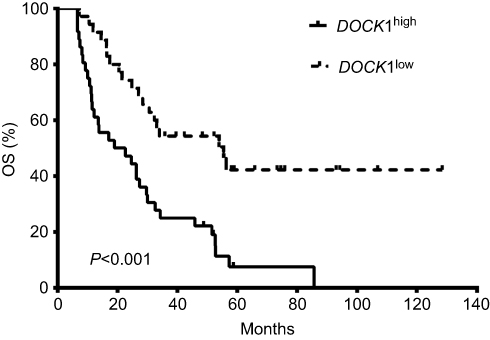 | Figure 1 Kaplan–Meier curves of overall survival (OS). Patients in DOCK1high group have shorter OS than those in DOCK1low group. |
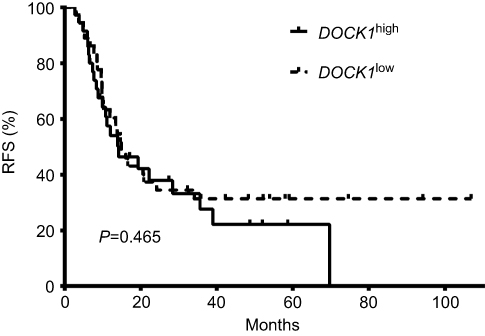 | Figure S1 Kaplan–Meier curves of relapse-free survival (RFS). There is no difference between DOCK1high group and DOCK1low group in the length of RFS. |
Discussion
In our study, overexpression of DOCK1 can shorten OS in AML patients undergoing allo-HSCT, implying that allo-HSCT cannot eliminate the negative effect of DOCK1 overexpression. As an important prognostic marker, DOCK1 might be a potential therapeutic target for AML treatment.
Sze-Hwei Lee, et al19 showed that higher DOCK1 expression was associated with many other prognostic factors including intermediate-risk cytogenetics. As a curative-intent method, allo-HSCT has a well-documented anti-tumor effect especially on high-risk and intermediate-risk AML patients.20 The prognostic influence of some prognostic mutations can be ameliorated by allo-HSCT.21 For example, Ma Y, et al concluded that allo-HSCT could efficiently reduce relapse and boost survival for patients with FLT3-ITD mutation.22 Yang Xu, et al have shown that allo-HSCT could prolong survival in cytogenetically normal AML.23 Our study came to similar conclusions that allo-HSCT could overcome the adverse effect of some prognostic factors, such as FLT3-ITD, DNMT3A and RUNX1. However, the inferior outcome associated with DOCK1 overexpression could not be completely overcome by allo-HSCT. Though transplant status in CR1/2 prolongs survival to some extent, the statistical significance still brings the level of DOCK1 expression to our attention.
Consistent with the previous study,19 our study showed that patients with DOCK1 overexpression were older and had higher PB blast percentage at diagnosis. But there was no distinct relationship between DOCK1 expression and karyotype or cytogenetics, probably due to the implementation of allo-HSCT. We found a negative correlation between DOCK1 expression and frequencies of FLT3-ITD, RUNX1 mutations in our cohort. Since these were well-defined poor prognostic factors, the negative correlation could further imply that high DOCK1 expression could be an independent risk factor for AML outcome post-transplant.
As a GEF, DOCK1 plays multiple roles in physiological and pathological conditions. Researches have shown that DOCK1 regulates cell motility and tumor invasion in glioma cell by binding with engulfment and cell motility protein 1 (ELMO1).24,25 Laurin, et al, reported that DOCK1 was a critical regulator in HER2-mediated breast cancer metastasis.18 In human colorectal cancer, DOCK1 was simulated by cortactin, which could promote cell migration and invasion.26 Downregulation of DOCK1 may prevent epithelial–mesenchymal transition in bladder cancer.16 Furthermore, in vivo researches by Tajiri, et al. have demonstrated the effectiveness of targeting DOCK1 in the ras-driven cancer cell.27 Hence, targeted therapy against DOCK1 deserves attention for future anti-cancer drug design. As demonstrated by the current study, the unfavorable effect of DOCK1 could not be eliminated by allo-HSCT, it would be worth investigating DOCK1-targeted therapy in AML patients for post-transplant maintenance.
Our study is limited by sample size and its retrospective nature. A larger cohort study is in need to confirm our findings. Further bench work exploring the role of DOCK1 in leukemogenesis are also imperative.
In conclusion, higher DOCK1 expression could predict a worse outcome in AML patients and its effect could not be overcome by allo-HSCT. DOCK1 is a potential anti-leukemia target for AML treatment.
Ethics approval and consent to participate
The study was approved by the Human Research Ethics Committee of Washington University. Informed consent was obtained from all the participants.
Availability of data and materials
All the data in this study were generated by TCGA database.
Acknowledgments
We thank all of the members who participated in providing and collating data. We also would like to thank Yifan Pang for editing the article. This study was supported by grants from the National Natural Science Foundation of China (nos 81500118 and 61501519), the China Postdoctoral Science Foundation Funded Project (project no. 2016M600443), and PLAGH Project of Medical Big Data (project no. 2016MBD-025).
Author contributions
Lin Fu and Xiaoyan Ke designed the study and substantially contributed to the overall analysis of the study. Gaoqi Zhang wrote the manuscript. Jinlong Shi organized the data. Xinrui Yang, Xinpei Zhang, Jilei Zhang, Siyuan Yang and Jing Wang performed statistical analyses and analyzed the data. Jilei Zhang provided guidance on modification. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Short NJ, Rytting ME, Cortes JE. Acute myeloid leukaemia. Lancet. 2018. doi:10.1016/S0140-6736(18)31041-9
2. Barbui T, Thiele J, Gisslinger H, et al. The 2016 WHO classification and diagnostic criteria for myeloproliferative neoplasms: document summary and in-depth discussion. Blood Cancer J. 2018;8(2):15. doi:10.1038/s41408-018-0054-y
3. Dohner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
4. Gale RE, Green C, Allen C, et al. The impact of FLT3 internal tandem duplication mutant level, number, size, and interaction with NPM1 mutations in a large cohort of young adult patients with acute myeloid leukemia. Blood. 2008;111(5):2776–2784. doi:10.1182/blood-2007-08-109090
5. Taskesen E, Bullinger L, Corbacioglu A, et al. Prognostic impact, concurrent genetic mutations, and gene expression features of AML with CEBPA mutations in a cohort of 1182 cytogenetically normal AML patients: further evidence for CEBPA double mutant AML as a distinctive disease entity. Blood. 2011;117(8):2469–2475. doi:10.1182/blood-2010-09-307280
6. Rakheja D, Konoplev S, Medeiros LJ, Chen W. IDH mutations in acute myeloid leukemia. Hum Pathol. 2012;43(10):1541–1551. doi:10.1016/j.humpath.2012.05.003
7. Bowen D, Groves MJ, Burnett AK, et al. TP53 gene mutation is frequent in patients with acute myeloid leukemia and complex karyotype, and is associated with very poor prognosis. Leukemia. 2009;23(1):203–206. doi:10.1038/leu.2008.173
8. Gaidzik VI, Bullinger L, Schlenk RF, et al. RUNX1 mutations in acute myeloid leukemia: results from a comprehensive genetic and clinical analysis from the AML study group. J Clin Oncol. 2011;29(10):1364–1372. doi:10.1200/JCO.2010.30.7926
9. Schlenk RF. Post-remission therapy for acute myeloid leukemia. Haematologica. 2014;99(11):1663–1670. doi:10.3324/haematol.2014.114611
10. Koreth J, Schlenk R, Kopecky KJ, et al. Allogeneic stem cell transplantation for acute myeloid leukemia in first complete remission: systematic review and meta-analysis of prospective clinical trials. JAMA. 2009;301(22):2349–2361. doi:10.1001/jama.2009.813
11. Kihara R, Nagata Y, Kiyoi H, et al. Comprehensive analysis of genetic alterations and their prognostic impacts in adult acute myeloid leukemia patients. Leukemia. 2014;28(8):1586–1595. doi:10.1038/leu.2014.55
12. Yanada M, Mori J, Aoki J, et al. Effect of cytogenetic risk status on outcomes for patients with acute myeloid leukemia undergoing various types of allogeneic hematopoietic cell transplantation: an analysis of 7812 patients. Leuk Lymphoma. 2018;59(3):601–609. doi:10.1080/10428194.2017.1357173
13. Takami A. Hematopoietic stem cell transplantation for acute myeloid leukemia. Int J Hematol. 2018;107(5):513–518. doi:10.1007/s12185-018-2412-8
14. Rashidi A, Linden MA, DeFor TE, et al. History of consolidation is prognostic in acute myeloid leukemia patients undergoing allogeneic hematopoietic cell transplantation in minimal residual disease-negative first complete remission. Am J Hematol. 2017;92(10):1032–1036. doi:10.1002/ajh.24834
15. Araki D, Wood BL, Othus M, et al. Allogeneic hematopoietic cell transplantation for Acute myeloid leukemia: time to move toward a minimal residual disease-based definition of complete remission? J Clin Oncol. 2016;34(4):329–336. doi:10.1200/JCO.2015.63.3826
16. Chen DJ, Chen W, Jiang H, Yang H, Wang YC, Chen JH. Downregulation of DOCK1 sensitizes bladder cancer cells to cisplatin through preventing epithelial-mesenchymal transition. Drug Des Devel Ther. 2016;10:2845–2853. doi:10.2147/DDDT.S101998
17. Gadea G, Blangy A. Dock-family exchange factors in cell migration and disease. Eur J Cell Biol. 2014;93(10–12):466–477. doi:10.1016/j.ejcb.2014.06.003
18. Laurin M, Huber J, Pelletier A, et al. Rac-specific guanine nucleotide exchange factor DOCK1 is a critical regulator of HER2-mediated breast cancer metastasis. Proc Natl Acad Sci U S A. 2013;110(18):7434–7439. doi:10.1073/pnas.1213050110
19. Lee SH, Chiu YC, Li YH, et al. High expression of dedicator of cytokinesis 1 (DOCK1) confers poor prognosis in acute myeloid leukemia. Oncotarget. 2017;8(42):72250–72259. doi:10.18632/oncotarget.19706
20. Zhang J, Shi J, Zhang G, et al. BAALC and ERG expression levels at diagnosis have no prognosis impact on acute myeloid leukemia patients undergoing allogeneic hematopoietic stem cell transplantation. Ann Hematol. 2018;97(8):1391–1397. doi:10.1007/s00277-018-3331-8
21. Chou SC, Tang JL, Hou HA, et al. Prognostic implication of gene mutations on overall survival in the adult acute myeloid leukemia patients receiving or not receiving allogeneic hematopoietic stem cell transplantations. Leuk Res. 2014;38(11):1278–1284. doi:10.1016/j.leukres.2014.08.012
22. Ma Y, Wu Y, Shen Z, Zhang X, Zeng D, Kong P. Is allogeneic transplantation really the best treatment for FLT3/ITD-positive acute myeloid leukemia? A systematic review. Clin Transplant. 2015;29(2):149–160. doi:10.1111/ctr.12495
23. Xu Y, Sun Y, Shen H, et al. Allogeneic hematopoietic stem cell transplantation could improve survival of cytogenetically normal adult acute myeloid leukemia patients with DNMT3A mutations. Am J Hematol. 2015;90(11):992–997. doi:10.1002/ajh.24135
24. Grimsley CM, Kinchen JM, Tosello-Trampont A-C, et al. Dock180 and ELMO1 proteins cooperate to promote evolutionarily conserved Rac-dependent cell migration. J Biol Chem. 2004;279(7):6087–6097. doi:10.1074/jbc.M307087200
25. Jarzynka MJ, Hu B, Hui KM, et al. ELMO1 and Dock180, a bipartite Rac1 guanine nucleotide exchange factor, promote human glioma cell invasion. Cancer Res. 2007;67(15):7203–7211. doi:10.1158/0008-5472.CAN-07-0473
26. Jing X, Wu H, Ji X, Wu H, Shi M, Zhao R. Cortactin promotes cell migration and invasion through upregulation of the dedicator of cytokinesis 1 expression in human colorectal cancer. Oncol Rep. 2016;36(4):1946–1952. doi:10.3892/or.2016.5058
27. Tajiri H, Uruno T, Shirai T, et al. Targeting ras-driven cancer cell survival and invasion through selective inhibition of DOCK1. Cell Rep. 2017;19(5):969–980. doi:10.1016/j.celrep.2017.04.016
Supplementary materials
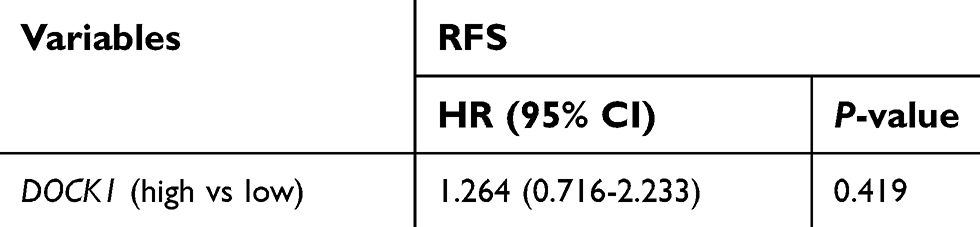
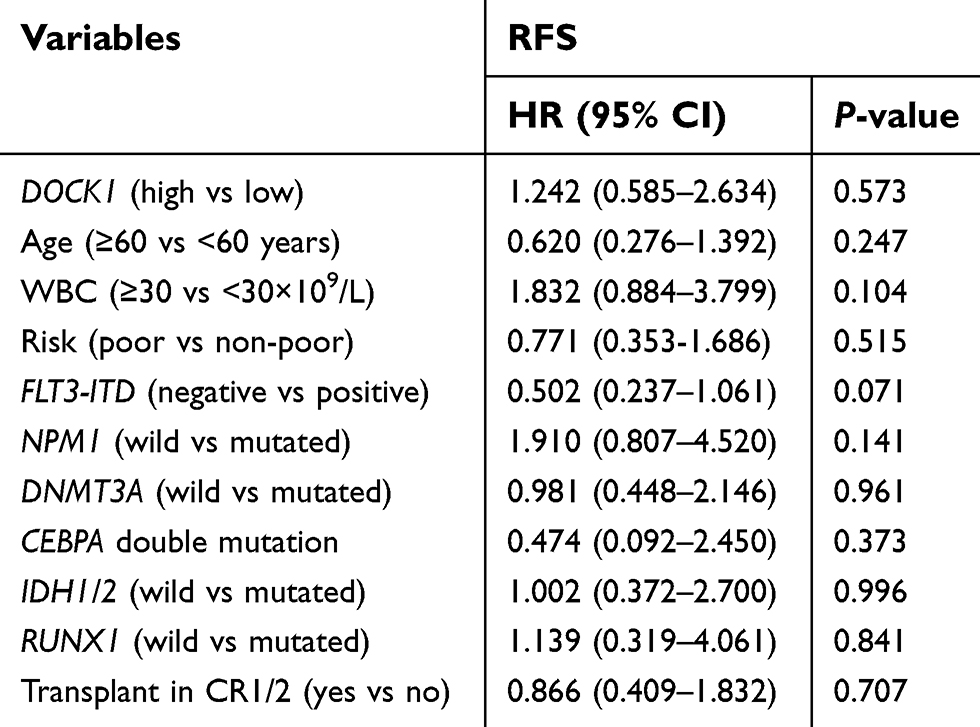
We analyze the relapse-free survival (RFS) rate using the univariate and multivariate analysis. The log-rank test was used to analyze significant differences between survival distributions. A cox proportional hazard model was applied to univariable and multivariable analyses to assess possible prognostic factors. DOCK1 expression did not show any significant effect on RFS outcome in uni- and multivariate analysis (Tables S1 and S2). The Kaplan–Meier curve of RFS showed no significance either (Figure S1).
 | Table S1 Univariate analysis for RFS |
 | Table S2 Multivariate analysis for RFS |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.