")
Back to Journals » Infection and Drug Resistance » Volume 14
High Acquisition Rate of Gram-Negative Multi-Drug Resistant Organism Colonization During Hospitalization: A Perspective from a High Endemic Setting
Authors Baljin B , Gurjav U, Tulgaa K, Baldan G, Gunchin B, Sandag T, Pfeffer K , Wendel AF, MacKenzie CR
Received 8 July 2021
Accepted for publication 26 August 2021
Published 23 September 2021 Volume 2021:14 Pages 3919—3927
DOI https://doi.org/10.2147/IDR.S328139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Bayaraa Baljin,1 Ulziijargal Gurjav,1 Khosbayar Tulgaa,2 Ganbaatar Baldan,1 Batbaatar Gunchin,3 Tsogtsaikhan Sandag,3 Klaus Pfeffer,4 Andreas F Wendel,5 Colin R MacKenzie4
1Department of Microbiology, Infection Prevention and Control, School of Biomedicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 2Department of Molecular Biology and Genetics, School of Biomedicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 3Department of Immunology, School of Biomedicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 4Institute of Medical Microbiology and Hospital Hygiene, University Hospital, Heinrich-Heine-University Dusseldorf, Dusseldorf, Germany; 5Institute of Hygiene, Cologne Merheim Medical Centre, University Hospital of Witten/Herdecke, Cologne, Germany
Correspondence: Bayaraa Baljin
Department of Microbiology, Infection Prevention and Control, School of Biomedicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia
Email [email protected]
Objective: The aim of the study was to compare the rate of gram-negative multi-drug resistant organism (GN-MDRO) colonization at admission and during hospitalization and to describe the strains and antibiotic resistance genes acquired during hospitalization.
Methods: Rectal swabs were collected from patients hospitalized at the National Trauma Center (NTC), Mongolia, at the time of admission and after 14 days of hospitalization as has been detailed on our previous study. GN-MDRO antibiotic resistance was determined using EUCAST standards, and resistance genes were detected using multiplex PCR.
Results: A total of 158 patients were screened, and baseline colonization rate at admission was 29.1% (46/158). The rate went up to 69.9% (110/158) after 14 days of hospitalization (p< 0.001). Of all participants, 74 patients (46.8%) screened GN-MDRO negative at admission acquired colonization by day 14. Other 36 patients (22.8%) maintained colonization that was screened positive at both time points. Only 38 patients (24.0%) remained free of GN-MDRO during hospitalization. There was a difference in GN-MDRO acquisition between these groups. Patients who were negative at admission acquired up to 3 GN-MDRO species, and there were 10 different species isolated. Reversely, patients who were screened positive at both time points had fairly homogenous isolates; up to 5 species of Enterobacterales were identified at admission and day 14 hospitalization. Overall, Enterobacterales were the dominant colonizers (61.4%, 97/158), and all Enterobacterales were resistant to cefotaxime as CTX-M resistance was our inclusion criteria.
Conclusion: GN-MDRO baseline colonization rate on admission was high and, alarmingly, doubled during hospitalization in the study area. Enterobacterales was the predominant colonizer and was highly resistant to 3rd generation cephalosporin. This data supports a need for an improved infection control policy including routine surveillance of the GN-MDROs and improved antibiotic stewardship program.
Keywords: multi-drug resistant organism, colonization, antibiotic resistance, hospital
Introduction
An increasing prevalence and dissemination of gram-negative multi-drug resistant organisms (GN-MDRO) remains at worldwide public health concern. Mongolia is part of the Western Pacific region which has the second highest reported rate of community level faecal carriage of extended spectrum β-lactamase producing Escherichia Coli, second only to the South East Asia Region.1,2 Both these regions are also reported to have a high rate of GN-MDRO hospital acquired infections (HAI).2 One of the sources of HAI, GN-MDROs cause more than 30% of HAI including blood stream infections and urinary tract infections.3,4 Infections caused by Enterobacterales are often related with a high mortality, morbidity and delay in effective treatment.5,6 Therefore developed countries have given much importance to the colonization of patients admitted to the hospital and established guidelines to screen drug-resistant organisms from rectal swab, groin, etc. depending on the species of the organism.7,8 Further, the guideline recommends an organism- or resistance mechanism-specific (detected by the presence of specific resistance gene) approaches to reduce the risk of transmission and outbreaks within the hospital.7,8 However none of these approaches are routinely practiced in our setting despite the presence of Ministerial decrees to screen some multi-drug resistant organisms and to monitor organisms that could transmit via specific procedures.9,10 Therefore it was important to detect baseline colonization in our setting to monitor the fluctuations of the MDROs.
In an attempt to detect the baseline colonization in our setting, in our previous study, we screened GN-MDRO from patients admitted to the National Trauma Center (NTC) and Burn Center.11 We reported an extremely high burden of GN-MDRO colonization at admission, which probably represents the high prevalence of community GN-MDRO. The publication has presented a data of 985 patients’ whose swabs were collected at admission. However, it does not show how colonization changes during hospitalization. The present study analyzed the data of 158 patients, a subset of 985 patients from the initial study, who had swab samples at admission and an additional swab taken after 14 days of hospitalization. Objectives of the study were to determine the rate of GN-MDRO colonization during hospitalization and to describe dynamics of GN-MDRO species, antibiotic resistance genes at both time points. The outcome of the study could become the basis of the organism- or resistance mechanism-specific approaches for improved infection, prevention and control guidelines in participating hospital.
Materials and Methods
Study Population
A prospective cohort study was conducted between July and September 2014 at the NTC and we enrolled patients who stayed at least 14 days at the hospital as has been described previously.11 Rectal swab samples were collected from 158 patients at admission and day 14 hospitalization. A patient with a positive GN-MDRO rectal swab sample was considered to be GN-MDRO colonized. All patients were assigned to one of four categories based on the presence or absence of the GN-MDROs on admission and at day 14; the first group had no detectable GN-MDRO on admission and remained negative on day 14, the second group consisted of patients, who were negative on admission and positive on day 14, the third group of patients had positive swab samples at both time points and the fourth group consisted of patients, who were positive on admission and negative for GN-MDRO on day 14.
Strain Identification, Antibiotic Susceptibility Testing and Resistance Gene Detection
Rectal swab samples were inoculated directly onto selective CHROMagar ESBL/KPC (bioMerieux, France) and suspicious colonies were sub-cultured on blood agar for strain identification. Strains were identified using MALDI-TOF MS or VITEK 2 (bioMerieux, France). Antibiotic susceptibility testing was performed using a disk diffusion method on Mueller-Hinton agar (Becton Dickinson, Germany) for the following antibiotics: cefotaxime, ceftazidime, ertapenem, imipenem, meropenem, ciprofloxacin, gentamicin, tobramycin, tigecycline, chloramphenicol, nitrofurantoin, trimethoprim-sulfamethoxazole and colistin. European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints were used to interpret the results (Clinical breakpoints – bacteria v 4.0, Disc diffusion manual v 4.0). In a case of phenotypic susceptibility test mismatch with PCR test, confirmatory tests were performed (combined disk diffusion test, MIC gradient strip test and/or a modified Hodge test) to confirm the presence of an ESBL and/or carbapenemase. Conventional and real-time multiplex PCRs were performed to detect the extended spectrum beta lactamase-, AmpC beta-lactamase- and carbapenemase-encoding resistance genes that have been detailed in paper by Baljin et al.11
Statistical Analysis
Preliminary analysis has been done using Microsoft excel and advanced statistical analyses were performed using SPSS 22.0 software. McNemar test was used to compare paired swab samples taken at admission and after 14 days of hospitalization to calculate the GN-MDRO and E. coli colonization rate, respectively. Mean age and gender variance of all 4 groups have been calculated using one way analysis of variance and a p-value of <0.05 was considered statistically significant. All percentages were reported with 1 decimal place.
Results
Patient Characteristics and Colonization Rate at Admission and Day 14 Hospitalization
The 158 patients were divided into 4 groups based on the presence or absence of GN-MDRO at admission and at day 14 hospitalization. The mean age of group 2 and 3 patients were younger than other groups (p<0.027) (Table 1). There was no difference in gender between 4 groups. However more males were belonged to group 2 and 3 who acquired GN-MDRO during hospitalization.
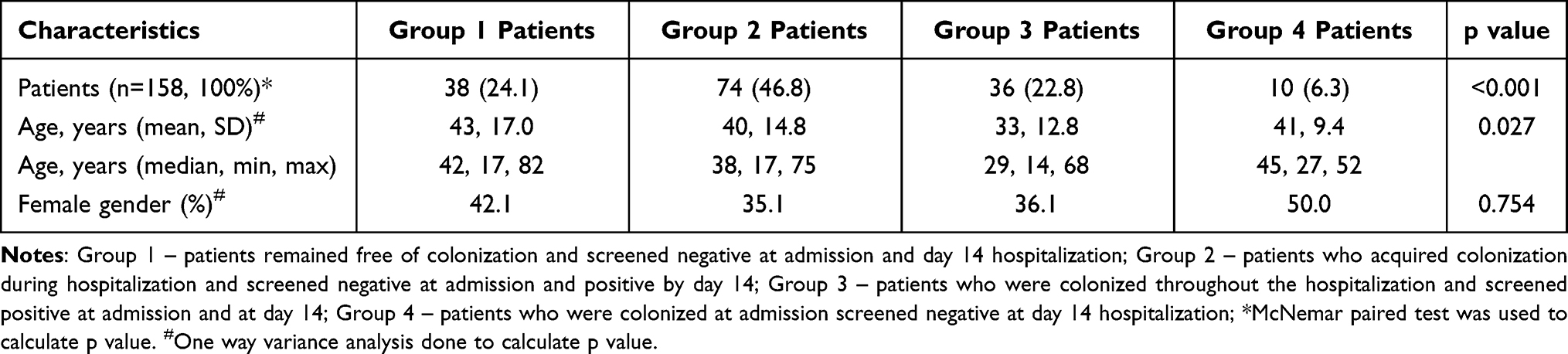 |
Table 1 Characteristics of Gram-Negative Multi-drug Resistant Organism Colonized Patients |
There were 38 patients in group 1 (24.1%) who remained free of colonization throughout the hospitalization and had no detectable GN-MDRO on admission nor on day 14 (Supplementary Table 1). Group two 74 (46.8%) patients were negative at admission and were GN-MDRO carriers by day 14. Group three 36 patients (22.8%) were positive for MDRO at both time points and thus maintained the GN-MDRO colonization during hospitalization (p<0.001). The baseline GN-MDRO colonization rate on admission was 29.1% (46/158) and the rate increased up to 69.6% (110/158) by day 14 of hospitalization (p<0.001). On the other hand, GN-MDRO acquisition rate during hospitalization was 40.5%.
Distribution of GN-MDRO Across Different Units on Day 14
On day 14, 133 GN-MDRO isolates were collected from 110 patients (69.6%, 110/158). Eleven different species of GN-MDROs were detected on day 14. Other than non-fermenting Acinetobacter baumannii, all species were belonged to Enterobacterales. The most prevalent species was E. coli and the percentage of patients carrying CTX-M-producing E. coli was increased from 27.8% (44/158) on admission to 54.6% (86/158) by day 14 (p<0.001) (Supplementary Table 2). The majority of GN-MDROs were isolated in 3 of the 4 units (88.0%, 117/133), the highest being the traumatic brain and spine injury unit (33.1%) followed by the bone and joints unit (30.8%) (Table 2). Up to 6 different species of GN-MDRO were present in a single unit. Predominant CTX-M producing E. coli (65.4%, 87/133) was present in all units.
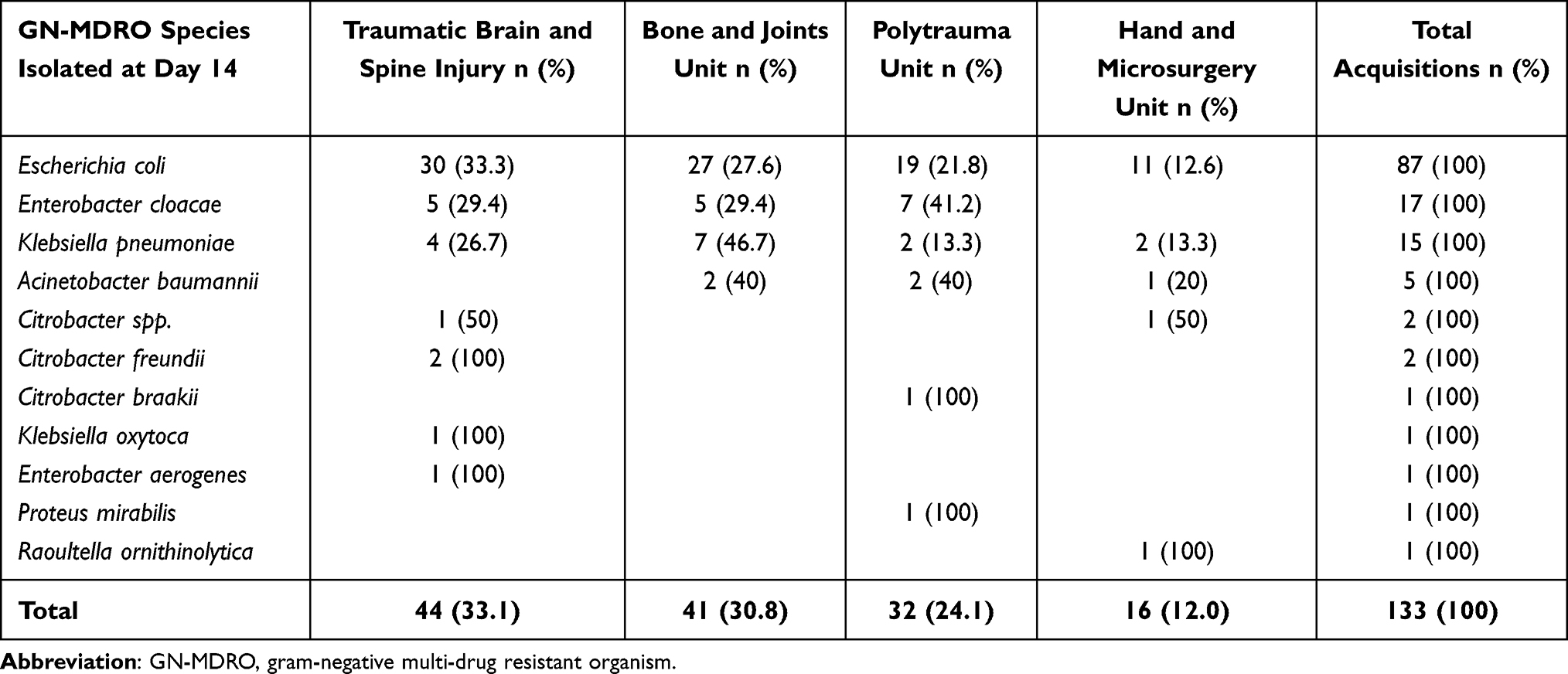 |
Table 2 Distribution of GN-MDRO Species Across Different Hospital Units at Day 14 Hospitalization |
Antibiogram of GN-MDROs Acquired at Day 14 Hospitalization
There were 88 GN-MDROs isolated from 74 patients at day 14 who were not colonized at admission. Enterobacterales were dominant (96.6%, 85/88) and were fully resistant to cefotaxime. Non-β-lactam antibiotics resistance was moderate to high, for example resistance to trimethoprim-sulfamethoxazole was 80.7% (71/88) and tobramycin was 42.4% (36/88). Resistance to carbapenem antibiotics was rare and only 1 E. coli isolate was determined to be ertapenem resistant. The remaining 3 isolates belonged to A. baumannii and were fully susceptible to colistin and resistant to the other 4 antibiotics (Table 3).
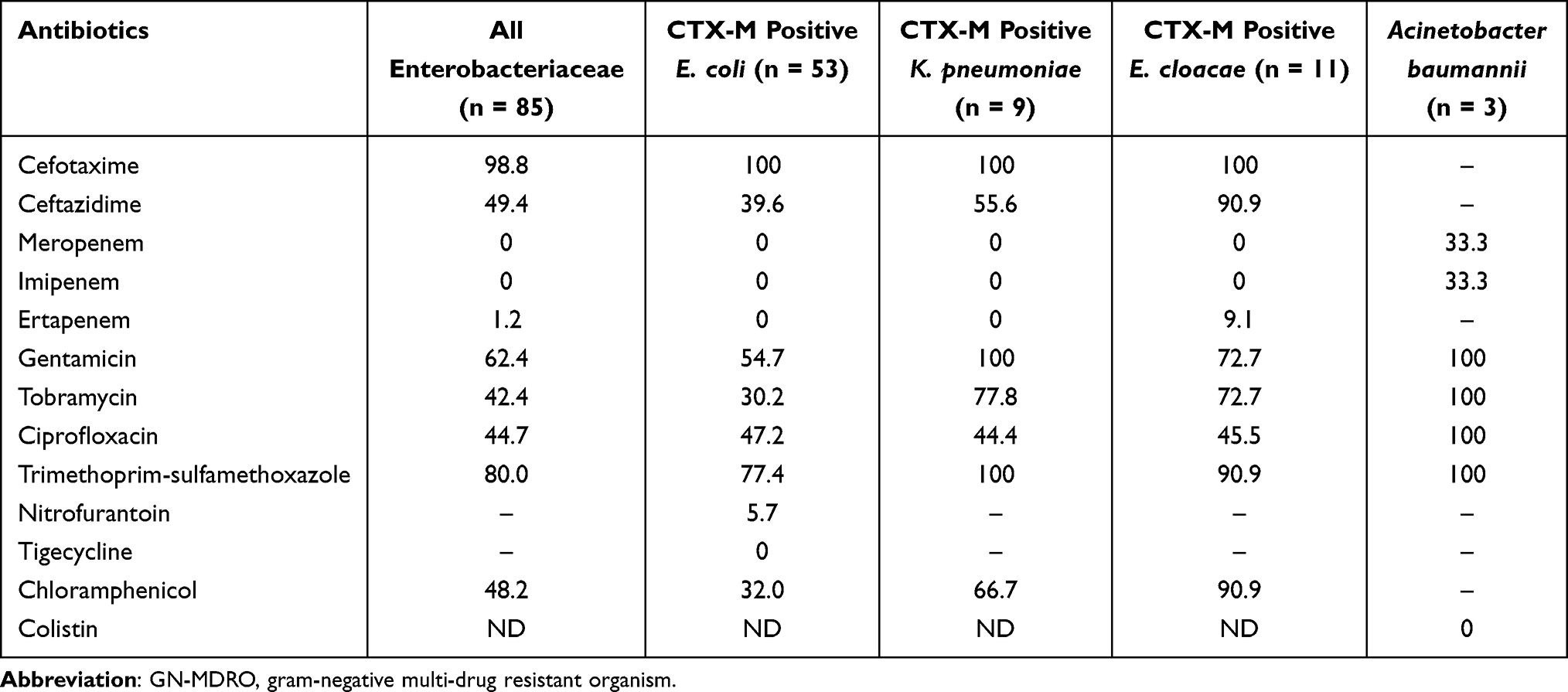 |
Table 3 Antibiotic Resistance of Newly Acquired GN-MDROs at Day 14 Hospitalization |
Acquisition of New GN-MDRO Species at Day 14
A total of 99 patients (62.6%, 99/158) that belonged to group 2 and 3 acquired a GN-MDRO by day 14 and overall Enterobacterales were the most prevalent colonizer (61.4%, 97/158) in both groups.
Of the isolated 10 different species of GN-MDRO from group two, 9 belonged to Enterobacterales and one was A. baumannii (Table 4). The most prevalent GN-MDRO of group 2 was CTX-M-9- and CTX-M-1-producing E. coli (37.8%, 28/74 and 31.0% 23/74), respectively. One patient was colonized with E. coli carrying both blaCTX-M-1 and blaCTX-M-9 genes and another patient was colonized with blaOXA-51-58-carrying A. baumannii. The co-colonization rate for patients acquiring >1 GN-MDRO was 17.6% (13/74). One patient from group 2 (2.7% 1/74) had acquired 3 different species and 12 patients (16.2%, 12/74) had acquired 2 different species. Enterobacterales carrying CTX-M-1 was the predominant co-colonizer (84.6%, 11/13).
Changes of GN-MDRO Structure During Hospitalization
There was a major change in GN-MDRO structure for group 3 patients who maintained the colonization throughout the hospitalization. Twenty five patients (69.4%, 25/36) had different GN-MDRO species and/-or antibiotic resistance genes at day 14 than were present at admission while the other 11 patients (30.6%, 11/36) retained the same species and resistance genes at both time points (Table 5).
 |
Table 4 GN-MDRO-Free Patients at Admission Acquired Up to 3 Species of GN-MDROs at Day 14 Hospitalization |
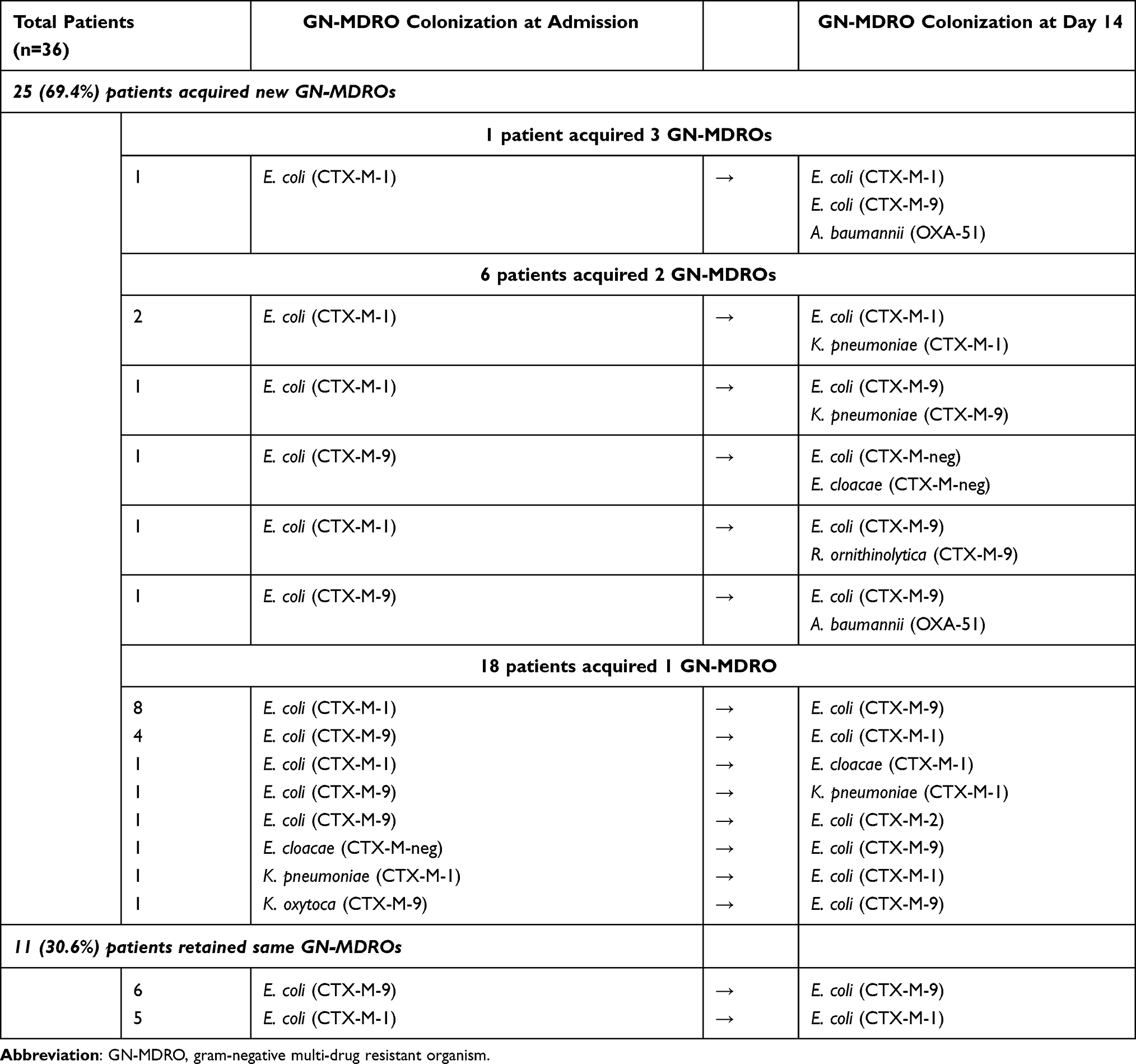 |
Table 5 Most of GN-MDRO Colonized Patients at Admission Acquired New GN-MDRO Species and or Genes by Day 14 |
At admission, GN-MDRO species was homogenous with only 4 GN-MDRO species identified. CTX-M-1 producing E. coli was the prevalent colonizer (52.8%, 19/36) followed by CTX-M-9 producing E. coli (38.9%, 14/36). However by day 14 hospitalization, there were 5 different species identified that included non-fermenting A. baumannii (5.5%, 2/36). The rate of CTX-M-9 producing E. coli rose to 55.5% (20/36) and CTX-M-1 producing E. coli was down to 36.1% (13/36) as compared to admission. The co-colonization rate for patients acquiring >1 GN-MDRO was 19.4% (7/36) which was similar to group 2 patients. Single patient had acquired 3 new GN-MDRO species (2.8%, 1/36) and 6 patients (16.7%) had acquired 2 new species of GN-MDRO, respectively. Interestingly, the dominant co-colonizer CTX-M-1 producing Enterobacterales was only present in 28.6% (2/7) of group 3 patients – 3 times less than group 2 patients. Instead, CTX-M-9-producing Enterobacterales (57.1%, 4/7) was the most prevalent co-colonizers in group 3 patients.
Discussion
Here we report a high GN-MDRO colonization rate at the time of admission. This rate was 3 to 7 times higher than industrialized countries such as Italy and Germany but was comparable to neighboring country Inner Mongolia, China.12–15 A high baseline colonization rate is often associated with previous hospitalization and/or antibiotic use.13,14 In our setting unregulated use of prescription antibiotics in the community may have contributed to the high colonization rate.16 Animal to human transmission of drug-resistant bacteria is also one possible factor as half of the Mongolian population have a nomadic lifestyle herding livestock all year round.17
We observed a doubling of GN-MDRO colonization rate during hospitalization and there could be different reasons for the acquisition of drug-resistant organisms. One possibility is patient to patient transmission as it has been shown in our previous study that drug resistant P. aeruginosa and A. baumannii each shared the same genotypes.11 Also an excessive use of antibiotics may have exerted selection pressure in gut microbiota that promoted growth of the resistant bacteria.18,19 Some tertiary hospitals in Mongolia including the participating hospitals have been documented as having an above average antibiotic prescription rate.20,21 In particular, NTC prescribes antibiotics in up to 85% patients when admitted to the hospital.22
Study participants’ mean age was significantly different. Especially patients who acquired- (group 2) and maintained- (group 3) GN-MDRO during hospitalization was younger than the patients who remained negative during hospitalization (group 1). Although the gender did not differ significantly, male patients were prone to GN-MDRO colonization. Therefore it is important to pay special attention to young and male patients when admitted to the hospital and screen for GN-MDRO. In addition, the fact that: 1) patients screened negative at admission and acquired up to 3 GN-MDRO species (group 2 patients); and 2) patients switching species during hospitalization (group 3 patients) warrants continued patient screening while at the hospital. Especially at day 14, the GN-MDRO burden was high in all 4 units of the NTC and there were 11 different GN-MDRO species present. Also 6 different GN-MDRO species co-circulating in one unit was worrisome, especially NTC does not conduct routine surveillance of the drug-resistant bacteria. From a hospital perspective, it is poor management of infection control and prevention and it is known that the environment including inanimate objects and hospital staff can harbor various gram-negative drug resistant bacteria.23,24 In addition, high resistance to various antibiotics has been observed in our study. Resistance to 3rd generation cephalosporin was moderate to high for Enterobacterales. Carbapenem resistance was rare and could be offered for serious cases. This finding prompts to update antimicrobial guideline to direct appropriate agents with the right regimen for individual clinical cases.5,6
Of the 11 different species detected at day 14, 10 species belonged to Enterobacterales; CTX-M producing E. coli was the most prevalent species however its rate was lower than in other high prevalence setting (53.1% vs. 94.9%).25 Being colonized with extended spectrum β–lactamase E. coli increases the risk of infections such as blood stream infection and reversely, underlying disease increases the risk of acquisition of E. coli.26,27 Therefore it is important to take an organism-specific approach in the participating hospital including active screening of these organisms on admission.5,6 Concerningly A. baumannii was detected in polytrauma and bone and joints unit and patients admitting to these facilities should be prioritized for screening.
While hospitalized, patients with no- or existing GN-MDRO colonization had the same propensity for acquiring more than 1 bacterial species (17.6% vs. 19.4%). CTX-M-1 carrying Enterobacteriales were the major co-colonizer for the patients who had no pre-existing colonization. However it was different for patients with underlying rectal colonization in whom, CTX-M-9 was the major co-colonizer. A recent study showed that being colonized with a MDRO considerably increases the risk of subsequent colonization of other multi-drug resistant organisms.28 The same paper by Wang et al showed that P. mirabilis colonization increased the acquisition of A. baumannii, methicillin resistant S. aureus and vancomycin resistant enterococci by least 2-times. Vise versa, a pre-existing colonization with E. coli, A. baumannii and P. aeruginosa increased the acquisition of P. mirabilis by 2-times.28 In our study, interestingly a single patient had acquired P. mirabilis and was co-colonized with blaCTX-M-1-9 producing E. coli.
Previous studies have established that MDRO colonization increases the length of hospital stay, treatment cost and mortality rate.26,29,30 A study conducted by Mutters et al showed that MDRO-colonized trauma patients stayed at least 2-times longer than all other colonized patients.31 Thus our findings highlight the importance of improving antibiotic stewardship and establishing routine surveillance for GN-MDROs. If the international guidelines and evidence backed interventions are strictly adhered to, a reduction of GN-MDRO burden in a healthcare setting can be expected.32,33
Some limitations of the study must be noted. The rectal swab was collected within 72 hours upon admission to the hospital and there is a chance that colonization occurred before the screening. Nevertheless we undertook an anonymous questionnaire from a subset of patients and half of the patients reported having antibiotics in last 6 months (data not shown). Thus pre-selection of a drug-resistant organism in the gut may have already occurred prior to the hospital admission. Therefore our finding GN-MDRO high admission rate could reflect community prevalence of GN-MDRO. Another limitation was that clinical samples from the same cohort were not collected and thus we were unable to establish a relationship between colonization and infection. However, there are many studies that showed isolation of Enterobacterales, non-fermenting P. aeruginosa and A. baumannii from clinical samples and established infection from rectal colonization.34–37 Some studies from Mongolia also showed presence of extended-spectrum β-lactamase-producing E. coli, Klebsiella spp. and A. baumannii from clinical samples.38,39 Therefore the relationship of colonization and infection needs to be further explored in Mongolia.
Conclusion
We report a high GN-MDRO colonization rate at the time of admission and that the colonization rate doubled during hospitalization. Enterobacterales were predominant colonizers and had increased resistance to third generation cephalosporin. Improved antibiotic stewardship and a targeted routine screening and surveillance program is necessary to contain the dissemination of the drug-resistant bacteria in the study area.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Research Ethics Committee of the Mongolian National University of Medical Sciences (No. 14-15/1A). Informed consent was obtained from all patients (if minor from the parent) participating in the study and the study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Authors thank the Institute of Medical Microbiology and Hospital Hygiene Dusseldorf for providing consumables and reagents. The authors also thank the PAGEL project coordinators Thomas Bruhn, Wilfried Schwippert and Ulamnemekh Otgonbayar from the Institute of Medical Microbiology and Hospital Hygiene, Dusseldorf, Germany for their continuous support. The project was supported by the Medical Faculty of the Heinrich-Heine-University, Dusseldorf, Germany in collaboration with the ESCMID Study Group on Genomic and Molecular Diagnostics (ESGMD), Basel, Switzerland and by the DAAD-PAGEL program (54448058).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Prof. Dr. Colin R MacKenzie report grants from German Academic Exchange Service (DAAD), during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Bezabih YM, Sabiiti W, Alamneh E, et al. The global prevalence and trend of human intestinal carriage of ESBL-producing Escherichia coli in the community. J Antimicrob Chemother. 2021;76(1):22–29. doi:10.1093/jac/dkaa399
2. Molton JS, Tambyah PA, Ang BS, et al. The global spread of healthcare-associated multidrug-resistant bacteria: a perspective from Asia. Clin Infect Dis. 2013;56(9):1310–1318. doi:10.1093/cid/cit020
3. Peleg Y, Hooper DC. Hospital-acquired infections due to gram-negative bacteria. N Engl J Med. 2010;362(19):1804–1813. doi:10.1056/NEJMra0904124
4. Exner M, Bhattacharya S, Christiansen B, et al. Antibiotic resistance: what is so special about multidrug-resistant gram-negative bacteria? GMS Hyg Infect Control. 2017;12:Doc05. doi:10.3205/dgkh000290
5. Sweber M, Carmeli Y. Mortality and delay in effective therapy associated with extended-spectrum β-lactamase production in Enterobacteriaceae bacteraemia: a systematic review and meta-analysis. J Antimicrob Chemother. 2007;60(5):913–920. doi:10.1093/jac/dkm318
6. Gualtero S, Valderrama M, Valencia M, et al. Factors associated with mortality in infections caused by carbapenem-resistant Enterobacteriaceae. J Infect Dev Ctries. 2020;14(6):654–659. doi:10.3855/jidc.12267
7. Centers for Disease Control and Prevention. Management of multi-drug resistant organisms in healthcare setting; 2006. Last updated in 2017. Available from: https://www.cdc.gov.
8. Queensland Health [homepage on the Internet]. Queensland health guideline: management of multi-resistant organisms guideline; 2017. Available from: https://www.health.qld.gov.au.
9. Ministry of Health Mongolia. Systematic approach to improve infection, prevention and control. Decree 2017 A/169; 2017. Available from: https://www.moh.gov.mn/.
10. Ministry of Health Mongolia. Surveillance of hospital acquired infections. Decree 2019 A/539; 2019. Available from: https://www.moh.gov.mn/.
11. Baljin B, Baldan G, Chimeddorj B, et al. Faecal carriage of gram-negative multidrug-resistant bacteria among patients hospitalized in two centres in Ulaanbaatar, Mongolia. PLoSOne. 2016;11(12):e0168146. doi:10.1371/journal.pone.0168146
12. Boldt AC, Schwab F, Rohde AM, et al. Admission prevalence of colonization with third-generation cephalosporin-resistant Enterobacteriaceae and subsequent infection rates in a German university hospital. PLoSOne. 2018;13(8):e0201548. doi:10.1371/journal.pone.0201548
13. Tacconelli E, De Angelis G, Cataldo MA, et al. Antibiotic usage and risk of colonization and infection with antibiotic-resistant bacteria: a hospital population-based study. Antimicrob Agents Chemother. 2009;53(10):4264–4269. doi:10.1128/AAC.00431-09
14. Yan L, Sun J, Xu X, et al. Epidemiology and risk factors of rectal colonization of carbapenemase-producing Enterobacteriaceae among high-risk patients from ICU and HSCT wards in a university hospital. Antimicrob Resist Infect Control. 2020;9(1):155–163. doi:10.1186/s13756-020-00816-4
15. Zhang J, Zheng B, Zhao L, et al. Nationwide high prevalence of CTX-M and an increase of CTX-M-55 in Escherichia coli isolated from patients with community-onset infections in Chinese county hospitals. BMC Infect Dis. 2014;14(1):659–669. doi:10.1186/s12879-014-0659-0
16. Dorj G, Hendrie D, Parsons R, et al. An evaluation of prescribing practices for community-acquired pneumonia (CAP) in Mongolia. BMC Health Serv Res. 2013;13(1):379–387. doi:10.1186/1472-6963-13-379
17. Muloi D, Ward MJ, Pedersen AB, et al. Are food animals responsible for transfer of antimicrobial resistant Escherichia coli or their resistance determinants to human populations? A systematic review. Foodborne Pathog Dis. 2018;15(8):467–474. doi:10.1089/fpd.2017.2411
18. Willmann M, El-Hadidi M, Huson DH, et al. Antibiotic selection pressure determination through sequence-based metagenomics. Antimicrob Agents Chemother. 2015;59(12):7335–7345. doi:10.1128/AAC.01504-15
19. Kolar M, Urbanek K, Latal T. Antibiotic selective pressure and development of bacterial resistance. Int J Antimicrob Agents. 2001;17(5):357–363. doi:10.1016/S0924-8579(01)00317-X
20. Bor L. Antibiotic use and bacterial resistance to the antibiotics; 2019. Available from: Http://www.hdc.gov.mn.
21. Dorj G, Salvesen Blix H, Sunderland B, et al. Antibiotic utilization trends in two state hospitals of Mongolia from 2013 to 2017. Biomed Res Int. 2019;2019:9160296. doi:10.1155/2019/9160296.
22. Ministry of health Mongolia. Surveillance of the antibiotic use in Mongolia; 2018. Available from: http://www.hdc.gov.mn.
23. Wang H, Zhang H, Liu J, et al. Antimicrobial resistance of 3 types of gram-negative bacteria isolated from hospital surfaces and the hands of health care workers. Am J Infect Control. 2017;45(11):143–147. doi:10.1016/j.ajic.2017.06.002
24. Chia PY, Sengupta S, Kukreja A, et al. The role of hospital environment in transmissions of multidrug-resistant gram-negative organisms. Antimicrob Resist Infect Control. 2020;9(1):29. doi:10.1186/s13756-020-0685-1
25. Moremi N, Silago V, Mselewa EG, et al. Extended-spectrum β-lactamase blaCTX-M-1 group in gram-negative bacteria colonizing patients admitted at Mazimbu hospital and Morogoro Regional hospital in Morogoro, Tanzania. BMC Res Notes. 2021;14(1):77–84. doi:10.1186/s13104-021-05495-x
26. Tseng WP, Chen YC, Chen SY, et al. Risk for subsequent infection and mortality after hospitalization among patients with multidrug-resistant gram-negative bacteria colonization or infection. Antimicrob Resist Infect Control. 2018;7(1):93–104. doi:10.1186/s13756-018-0388-z
27. Ferstl PG, Filmann N, Heilgenthal EM, et al. Colonization with multidrug-resistant organisms is associated with in increased mortality in liver transplant candidates. PLoS One. 2021;16(1):e0245091. doi:10.1371/journal.pone.0245091
28. Wang J, Foxman B, Mody L, et al. Network of microbial and antibiotic interactions drive colonization and infection with multidrug-resistant organisms. Proc Natl Acad Sci USA. 2017;114(39):10467–10472. doi:10.1073/pnas.1710235114
29. Engler-Husch S, Heister T, Mutters NT, et al. In-hospital costs of community-acquired colonization with multidrug-resistant organisms at a German teaching hospital. BMC Health Serv Res. 2018;18(1):737. doi:10.1186/s12913-018-3549-0
30. Filius PMG, Gyssens IC, Kershof IM, et al. Colonization and resistance dynamics of gram-negative bacteria in patients during and after hospitalization. Antimicrob Agents Chemother. 2005;49(7):2879–2886.
31. Mutters NT, Gunther F, Sander A, et al. Influx of multidrug-resistant organisms by country-to-country transfer of patients. BMC Infect Dis. 2015;15(1):466–472. doi:10.1186/s12879-015-1173-8
32. Tacconelli E, Cataldo MA, Dancer SJ, et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin Microbiol Infect. 2014;20(Suppl 1):1–55.
33. Hopman J, Tostmann A, Wertheim H, et al. Reduced rate of intensive care unit acquired gram-negative bacilli after removal of sinks and introduction of ‘water-free’ patient care. Antimicrob Resist Infect Control. 2017;59(6):1–9.
34. Cornejo-Juarez P, Suarez-Cuenca JA, Volkow-Fernandez P. Fecal ESBL Escherichia coli carriage as a risk factor for bacteremia in patients with hematological malignancies. Support Care Cancer. 2016;24(1):253–259. doi:10.1007/s00520-015-2772-z
35. Mirzaei B, Babaei R, Bazgir ZN, et al. Prevalence of Enterobacteriaceae spp. and its multidrug-resistant rates in clinical isolates: a two-center cross-sectional study. Mol Biol Rep. 2021;48(1):665–675. doi:10.1007/s11033-020-06114-x
36. Mirzaei B, Bazgir ZN, Goli HR, et al. Prevalence of multi-drug resistant (MDR) and extensively drug-resistant (XDR) phenotypes of Pseudomonas aeruginosa and Acinetobacter baumannii isolated in clinical samples from Northeast of Iran. BMC Res Notes. 2020;13(1):380. doi:10.1186/s13104-020-05224-w
37. Shadkam S, Goli HR, Mirzaei B, et al. Correlation between antimicrobial resistance and biofilm formation capability among Klebsiella pneumoniae strains isolated from hospitalized patients in Iran. Ann Clin Microbiol Antimicrob. 2021;20(1):13. doi:10.1186/s12941-021-00418-x
38. Kao CY, Udval U, Huang YT, et al. Molecular characterization of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella spp. isolates in Mongolia. J Microbiol Immunol Infect. 2016;49(5):692–700. doi:10.1016/j.jmii.2015.05.009
39. Kao CY, Udval U, Oyunchimeg R, et al. Dissemination of OXA-carbapenemase-producing Acinetobacter baumannii ST195 and ST642 in a Mongolian hospital. Infect Genet Evol. 2014;28:313–316. doi:10.1016/j.meegid.2014.10.024
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.