")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Heterogeneity in Psychological Resilience and Mental Health among Newly Graduated Nursing Students: A Latent Profile and Generalized Additive Model Analysis
Authors Mei XX, Wu XN, Wang HY , Wu JY, Wang XQ , Ye ZJ
Received 17 December 2021
Accepted for publication 25 February 2022
Published 10 March 2022 Volume 2022:15 Pages 597—606
DOI https://doi.org/10.2147/PRBM.S348661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xiao Xiao Mei, Xiao Na Wu, Hui Yuan Wang, Jie Yi Wu, Xin Qin Wang, Zeng Jie Ye
Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, 510006, People’s Republic of China
Correspondence: Zeng Jie Ye, People’s Republic of China, Tel +86 15914411786, Email [email protected]
Background: Psychological resilience is important to mental health and professional development in newly graduated nursing students (NGNSs). However, the association between psychological resilience and mental health in NGNSs is less explored.
Purpose: The current study was designed to determine mental health profiles measured by the Kessler 10 scale (K10) and evaluate the non-linear association between psychological resilience and mental health in NGNSs.
Methods: A total of 472 NGNSs from the Be Resilient to Nursing Career program were assessed using the K10 and ten-item Connor–Davidson Resilience Scale (CD-RISC 10). Latent profile analysis and generalized additive model analysis were performed.
Results: A four-class model based on the K10 was identified: lowest (28.0%), lower-middle (36.4%), upper-middle (26.1%), and highest (9.5%) subgroups. Academic degree and psychological resilience were significant indicators of mental health profiles. Psychological resilience was negatively and nonlinearly correlated with mental health when the CD-RISC 10 score was > 17.
Conclusion: There exists heterogeneity in NGNSs’ mental health. The negative and nonlinear association between psychological resilience and mental health can only be confirmed in NGNSs with moderate and high resilience levels.
Keywords: psychological resilience, mental health, latent profile analysis, generalized additive model analysis, newly graduated nursing students
Introduction
Nurses are the largest professional group in the field of health care.1 However, the global shortage of nurses is estimated to be 5.9 million. This issue can be addressed if nurse graduates increase by 8% every year before 2030.2 Newly graduated nursing students (NGNSs) will be the backbone of the nursing workforce in the future, and their mental health cannot be overstated.3 For example, a high prevalence of mental health problems has been identified among nursing students, especially in China,4,5 resulting in diminished quality of life and lower productivity. Therefore, it is crucial to identify NGNSs with mental health problems and implement health promotion. Anderson and Priebe argued that resilience enables people to withstand external pressures and not become distressed during major adversity, and resilience is itself the process of bouncing back from adversity over time.6 This hypothesis has been confirmed in Tanji and Kodama’s research, which identified a negative association between innate resilience and poor mental health.7 Moreover, resilience has consistently been found to be a protective factor for nurses in disasters and helps to transform adversity into positive growth experiences, which contributes to their professional development and better mental and physical health.8 Therefore, it is necessary to explore the relationship between psychological resilience and mental health among NGNSs. Many studies have focused on the mediating effect of psychological resilience against poor mental health in specific populations,9–12 but the direct association between resilience and mental health has been less explored in NGNSs, especially in a longitudinal cohort. As such, we developed a 2-year cohort program — Be Resilient to Nursing Career (BRNC; ChiCTR2000038693) — to estimate changes in mental health, psychological resilience, professional identity, burnout, and retention from the beginning of internship to the first year of employment. This study focuses on this prospective cohort and is based Rees’s resilience model in the workplace,13 which is illustrated in Figure 1. It was designed to identify latent subgroups in NGNSs with different mental health profiles using latent profile analysis (LPA), examine demographics associated with mental health profiles, and estimate the potential nonlinear association between psychological resilience and mental health with generalized additive model (GAM) analysis.
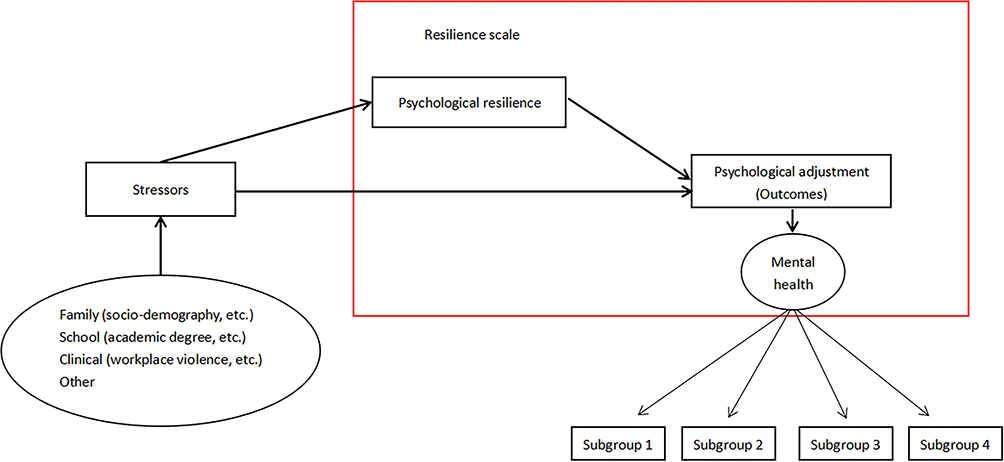 |
Figure 1 Hypothetical framework of psychological resilience and mental health among newly graduated nurses. |
Methods
Participants and Procedure
A total of 525 NGNSs were enrolled from two universities in southern and central China (Guangzhou and Zhengzhou) from June to July 2020. In sum, 55 questionnaires were excluded due to nonresponse and incompleteness, resulting in a final sample of 470 (response rate 89.5%). The subjects gave written consent before the formal investigation. Inclusion criteria were recent graduation, ability to communicate fluently in Mandarin, and agreement to participate. The exclusion criterion was presence or history of a diagnosis of mental disorders.
Sample Size
A sample size of 300–1,000 was recommended for latent profile analysis.14 In addition, the possibility of detecting rare profiles also needed to be considered. Therefore, 470 was efficiently powerful for LPA-based analysis.
Instruments
Demographics
Based on previous literature,15–17 we collected NGNSs’ demographics (age, sex, education, place of residence) and profession-related information (academic achievement, nursing role models, internship experience, medical staff as relatives).
Kessler 10 Scale (K10)
The K10 was developed by Kessler et al,18 and the Chinese version has been proved to be reliable.19 It has been used to measure mental health among medical students and NSs.20 The K10 has ten items and uses a five-point Likert scale, with possible scores of 10–50. Cronbach’s α coefficient for the K10 in this study was 0.948.
Connor–Davidson Resilience Scale (CD-RISC)
The CD-RISC was developed in 2003 and contains 25 items.21 Campbell-Sills and Stein made a series of empirical modifications, resulting in a unidimensional scale of ten items that exhibited excellent psychometric properties that correlated highly with the original version (r=0.92).22 Each item is rated on a 0–4 scale, with high scores reflecting high levels of resilience. The Chinese version of the CD-RISC 10 has proven to be reliable and effective.23 Cronbach’s α coefficient for this scale in this study was 0.911.
Data Analysis
Descriptive statistics are given as means ± SD or frequencies (percentages). Associations between demographics and the K10 and resilience were initially explored. Then, LPA was performed to identify latent subgroups pertaining NGNSs’ mental health.24 It began with a one-class model and continued until fit indices could not be significantly improved. For determining the number of latent subgroups, Akaike information criterion (AIC),25 Bayesian information criterion (BIC),26 sample size–adjusted BIC,27 and entropy were utilized as indicators. The Lo–Mendell–Rubin likelihood-ratio test and bootstrapped likelihood ratio test were used to test whether the introduction of an additional category (ie, latent group) contributed to a significant change compared to the previously derived model.28 Also, k-means clustering was applied to confirm the LPA-derived profiles. After the optimal LPA model had been determined, univariate and multivariate regression was used to detect relationships between latent classes of mental health and demographics and resilience. Potential covariates with P<0.2 on univariate analysis were included in multivariate regression.29 In addition, false discovery–rate calculations were performed to control for type I errors on multivariate regression. Then, GAM analysis was performed to estimate nonlinear associations between resilience and mental health. Lastly, we divided mental health profiles into dichotomous outcomes — positive group (coded 0) and negative group (coded 1) — and classified resilience scores into low resilience, medium resilience, high resilience, and very high resilience to further examine associations between resilience and mental health. Mplus 8.3, SPSS 26.0, and Empower Stats 2.2 were used for all statistical analyses.
Ethics
The present study is part of the BRNC (ChiCTR2000038693) program and was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine (ZYYEC-ERK [2020] 132). Participants allowed us to use their data for academic research and publication. All participants provided informed consent, and the study was conducted in accordance with the Declaration of Helsinki.
Results
Sample Characteristics
Demographics and profession-related characteristics are presented in Table S1. The sex ratio of men to women was 1:4.76 and the mean age 22.21±1.27 years. Mean scores on the K10 and CD-RISC 10 were 22.63±8.18 and 25.14±5.64, respectively. Relationships between demographic characteristics and the K10 and CD-RISC 10 are presented in Figure 2A.
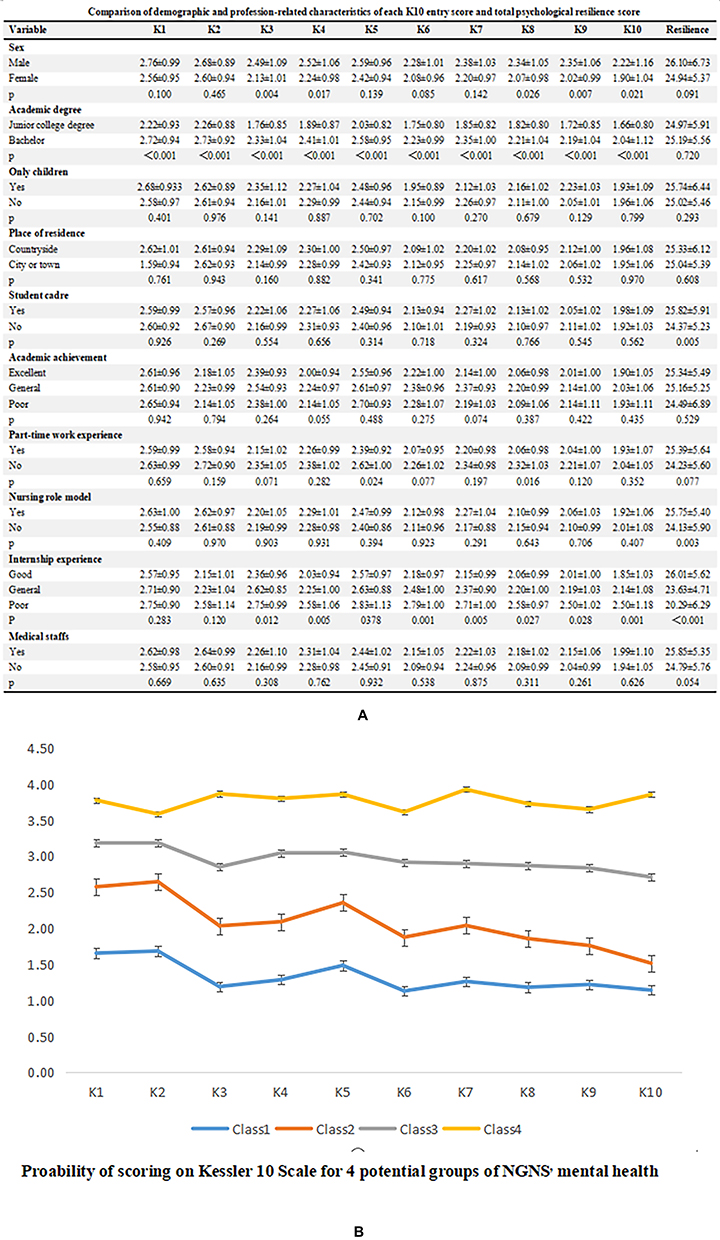 |
Figure 2 (A, B) Relationship between demographic characteristics, K10, and CD-RISC 10 and probability of scoring on K10 for four potential groups of newly graduated nurses’ mental health. |
Latent Profile Analysis of Mental Health
Figure 3A shows that log-likelihood, AIC, BIC, and adjusted BIC values decreased in line with an increasing number of categories. This indicated that a four-class model (C1, C2, C3, C4) had the optimal fitting indicators, with an entropy value of 0.915 (classification accuracy >96%). The subgroups were classified as lowest (28.0%), lower middle (36.4%), upper middle (26.1%), and highest (9.5%), and are further explained in Figure 2B. Classification probabilities for the most likely latent class membership (column) by latent class (row) are presented in Table S2. The k-means clustering analysis confirmed the LPA-based findings (κ=0.947, 95% CI 0.923–0.971; Table S3).
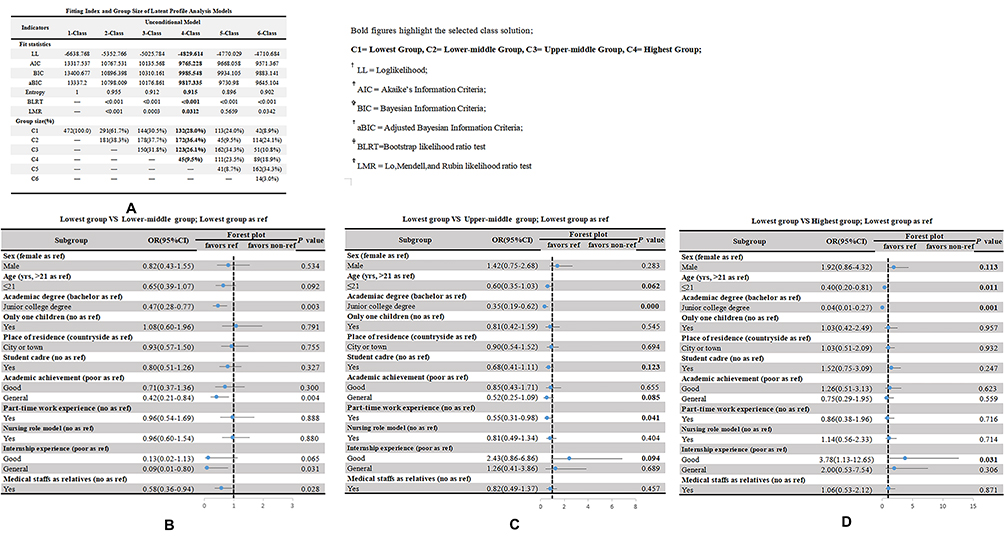 |
Figure 3 (A-D) Fitting index and group size of latent profile–analysis models and univariate logistic regression results for predicting external features on the four-class pattern. Abbreviation: CI, confidence interval. Note: Bold figures highlight statistical significance on univariate logistic regression. |
Univariate Logistic Regression Analysis
Figure 3B shows that for the lowest group vs the lower-middle group, age (OR 0.65, P=0.092), academic degree (OR 0.467, P=0.003), general academic achievement (OR 0.42, P=0.004), good internship experience (OR 0.13, P=0.065), general internship experience (OR 0.09, P=0.031), and medical staff as relatives (OR 0.58, P=0.028) were significant predictors of NGNSs’ mental health profiles. Figure 3C shows that for the lowest group vs the upper-middle group, age (OR 0.60, P=0.062), academic degree (OR 0.35, P<0.0001), student-cadre experience (OR 0.68, P=0.123), general academic achievement (OR 0.52, P=0.085), part-time work experience (OR 0.55, P=0.041), and good internship experience (OR 2.43, P=0.094) were significant predictors of NGNSs’ mental health profiles. Figure 3D shows that that for the lowest group vs the highest group, sex (OR 1.92, P=0.113), age (OR 0.40, P=0.011), academic degree (OR 0.04, P=0.001), and good internship experience (OR 3.78, P=0.094) were significant predictors of NGNSs’ mental health profiles.
Multivariate Logistic Regression Analysis
Table S4-1 shows that for the lowest group vs the lower-middle group, resilience (OR 0.91, P<0.0001), academic degree (OR 0.39, P<0.0001), general academic achievement (OR 0.34, P=0.004), good internship experience (OR 0.08, P=0.023), and general internship experience (OR 0.07, P=0.016) were significant predictors of mental health after adjusting for the effects of confounders. Table S4-2 shows that for the lowest group vs the upper-middle group, resilience (OR 0.84, P<0.0001), academic degree (OR 0.26, P<0.0001), and general academic achievement (OR 0.34, P=0.011) were significant predictors of mental health profiles after adjusting for the effects of confounders. Table S4-3 shows that for the lowest group vs the highest group, resilience (OR 0.90, P<0.0001), and academic degree (OR 0.03, P=0.001) were significant predictors of mental health after adjusting for the effects of confounders.
Generalized Additive Model Analysis
Resilience was nonlinearly associated with mental health (Figure 4A). When resilience scores were <17, resilience was positively associated with mental health, while this association became negative when they were >17. Figure 4B shows that NGNSs with a medium level of psychological resilience were 0.438 times less likely to have mental health problems than those with a low level of psychological resilience and that NGNSs with a high level of psychological resilience were 0.164 times less likely to have mental health problems than those with a mild level of psychological resilience, while NGNSs with a very high level of psychological resilience were 0.182 times less likely to have mental health problems than those with a mild level of psychological resilience (all P<0.001).
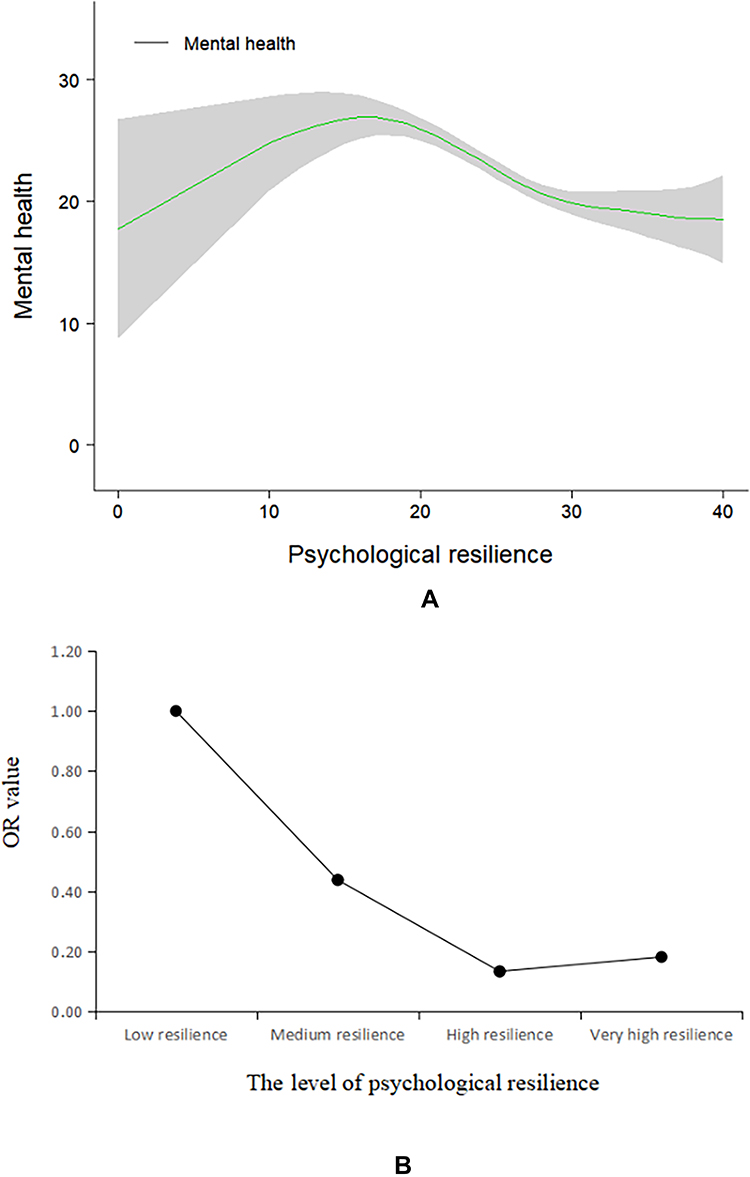 |
Figure 4 Curve-fitting and curvilinear regression results. |
Discussion
NSs experience significantly more stress, anxiety, sleep disturbances, and stress-related disorders than the general student population.30 Therefore, it is important to understand the mental health of NGNSs and contributing factors so as to develop proactive interventions. Although many studies have investigated mental health in NSs or nurses, a majority have focused on the prevalence of mental health problems,1,5 and the heterogeneity of mental health profiles have been less explored. The results in the current study demonstrated the heterogeneity of mental health profiles in the NGNSs sampled, consistent with Ma and Lai.31 Profession-related covariates were also used for a better understanding of mental health profiles in NGNSs, eg, internship experience and medical staff as relatives. Type of degree differentiated these four mental health profiles from one another, with NGNSs with a bachelor’s degree more prone to be in the highest-risk mental health subgroup than those with a junior college degree. This may be attributed to high self-expectation. In addition, delayed recruitment or reduced job opportunities in tertiary hospitals due to the high number of coronavirus patients in 2020 may also have exacerbated mental health issues, consistent with Moxham et al’s findings.32
Individual-based LPA was performed to provide new insights into associations between resilience and mental health profiles in NGNSs. Mental health was negatively associated with psychological resilience only in NGNSs with moderate and high resilience levels, which was inconsistent with previous studies.33–35 This phenomenon was also identified in Pakalniškienė et al’s research.36 Potential reasons for this are that at the time of our enrollment, NGNSs had returned to school from their clinical internship and were preparing their dissertations while simultaneously dealing other stressors, such as employment, education, and marriage. As such, NGNSs with low resilience levels may have had a turbulent mental status, making it difficult to recognize the relationship between resilience and mental health. Also, the small sample of NGNSs with low resilience (<17) may be another possible reason, and this issue should be further verified in future research. Medical staffs are quite different from other professionals, and the CD-RISC 10 may not have captured some resilience characteristics in the current study. A new resilience instrument specific to nurses or physicians should be developed and validated in future research, as pointed out in other resilience-based research.37–42
A nonlinear relationship was identified that had not been fully explored in previous studies. On GAM, analysis, a significant threshold effect was revealed between high- and very high–resilience subgroups, indicating that proactive intervention approaches should be undertaken for NGNSs with moderate levels to achieve optimal cost-effectiveness. These findings suggest that it is feasible to incorporate resilience-target intervention into mental health–enhancement programs for FNSs at high risk of emotional distress. There already exist some resilience-enhancing programs for NSs. For example, Chow et al developed a resilience-building program for 195 NSs that had a beneficial impact on nursing undergraduates.43 In addition, resilience-based interventions have also been trialed on patients. For example, Ye et al developed the program Be Resilient to Breast Cancer to promote breast cancer patients’ resilience, resulting in increased quality of life and hope.44–47 These successful programs could be adapted and utilized for NGNSs.
Limitations
Several limitations should be considered. First, NGNSs from two universities may not be representative, and the findings of the current study should be validated in a larger sample with students from different backgrounds. Second, causality cannot be established due to the cross-sectional nature of this study, and a longitudinal study for the association between resilience and mental health should be performed. An ongoing 2-year follow-up assessment on this BRNC cohort will provide more insights. Third, several potential confounders, ie, social support, hope, and family function, were not considered and included in regression analysis due to study restrictions, which would surely have affected the relationship between resilience and mental health. These variables can be considered in future studies.
Conclusion
There exists heterogeneity in NGNSs’ mental health. Negative and nonlinear associations between psychological resilience and mental health can only be confirmed in NGNSs with moderate and high resilience levels.
Ethics
The current study is part of the Be Resilient to Nursing Career (ChiCTR2000038693) program and was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine (ZYYEC-ERK [2020] 132).
Funding
This research was funded by grants from the National Natural Science Foundation of China (71904033), Humanity and Social Science Youth Foundation of Ministry of Education of China (19YJCZH227), Humanity and Social Science Foundation of Department of Education of Guangdong Province (2020WTSCX009), Humanity and Social Science Foundation of Guangzhou (2021GZGJ57), and Humanity and Social Science Foundation of Guangzhou University of Chinese Medicine (2020SKXK01, 2021SKYB07).
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Seabra PRC, Lopes JMO, Calado ME, Capelas ML. A national survey of the nurses’ mental health - the case of Portugal. Nurs Forum. 2019;54(3):425–433. doi:10.1111/nuf.12350
2. World Health Organization. State of the world’s nursing 2020: investing in education, jobs and leadership report. Available from: https://apps.who.int/iris/bitstream/handle/10665/331677/9789240003279-eng.pdf.
3. Galderisi S, Heinz A, Kastrup M, Beezhold J, Sartorius N. A proposed new definition of mental health. Propozycja nowej definicji zdrowia psychicznego. Psychiatr Pol. 2017;51(3):407–411. doi:10.12740/PP/74145
4. Cheung T, Wong SY, Wong KY, et al. Depression, anxiety and symptoms of stress among baccalaureate nursing students in Hong Kong: a cross-sectional study. Int J Environ Res Public Health. 2016;13(8):779. doi:10.3390/ijerph13080779
5. Zeng Y, Wang G, Xie C, Hu X, Reinhardt JD. Prevalence and correlates of depression, anxiety and symptoms of stress in vocational college nursing students from Sichuan, China: a cross-sectional study. Psychol Health Med. 2019;24(7):798–811. doi:10.1080/13548506.2019.1574358
6. Anderson K, Priebe S. Concepts of resilience in adolescent mental health research. J Adolesc Health. 2021;69(5):689–695. doi:10.1016/j.jadohealth.2021.03.035
7. Tanji F, Kodama Y. Prevalence of psychological distress and associated factors in nursing students during the COVID-19 pandemic: a cross-sectional study. Int J Environ Res Public Health. 2021;18(19):10358. doi:10.3390/ijerph181910358
8. Hart PL, Brannan JD, De Chesnay M. Resilience in nurses: an integrative review. J Nurs Manag. 2014;22(6):720–734. doi:10.1111/j.1365-2834.2012.01485.x
9. Wang L, Xu B, Gu Y, Zhu J, Liang Y. The mediating and moderating effects of resilience on the relationship between perceived stress and depression in heroin addicts. J Community Psychol. 2019;47(3):495–503. doi:10.1002/jcop.22133
10. Yu J, Chae S. The mediating effect of resilience on the relationship between the academic burnout and psychological well-being of medical students. Korean J Med Educ. 2020;32(1):13–21. doi:10.3946/kjme.2020.149
11. Hou T, Zhang T, Cai W, et al. Social support and mental health among health care workers during Coronavirus Disease 2019 outbreak: a moderated mediation model. PLoS One. 2020;15(5):e0233831. doi:10.1371/journal.pone.0233831
12. Howell KH, Miller-Graff LE, Schaefer LM, Scrafford KE. Relational resilience as a potential mediator between adverse childhood experiences and prenatal depression. J Health Psychol. 2020;25(4):545–557. doi:10.1177/1359105317723450
13. Rees CS, Breen LJ, Cusack L, Hegney D. Understanding individual resilience in the workplace: the international collaboration of workforce resilience model. Front Psychol. 2015;6:73. doi:10.3389/fpsyg.2015.00073
14. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equ Model. 2014;21(2):263–279. doi:10.1080/10705511.2014.882690
15. Xie J, Liu M, Zhong Z, et al. Relationships among character strengths, self-efficacy, social support, depression, and psychological well-being of hospital nurses. Asian Nurs Res. 2020;14(3):150–157. doi:10.1016/j.anr.2020.06.002
16. Guo YF, Cross W, Plummer V, Lam L, Luo YH, Zhang JP. Exploring resilience in Chinese nurses: a cross-sectional study. J Nurs Manag. 2017;25(3):223–230. doi:10.1111/jonm.1245
17. Mark G, Smith AP. Occupational stress, job characteristics, coping, and the mental health of nurses. Br J Health Psychol. 2012;17(3):505–521. doi:10.1111/j.2044-8287.2011.02051.x
18. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/s0033291702006074
19. Zhou CC, Chu J, Wang TT, et al. Reliability and validity of 10-item Kessler Scale (K10) Chinese version in evaluation of mental health status of Chinese population. Chin J Clin Psychol. 2008;16(6):627Y629.
20. Behera S, Paluri SSSL, Mishra A. Mental health status of students pursuing professional training: a questionnaire-based study. J Educ Health Promot. 2021;10:399. doi:10.4103/jehp.jehp_1340_20
21. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
22. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
23. Ye ZJ, Qiu HZ, Li PF, et al. Validation and application of the Chinese version of the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) among parents of children with cancer diagnosis. Eur J Oncol Nurs. 2017;27:36–44. doi:10.1016/j.ejon.2017.01.004
24. Boduszek D, Debowska A, Willmott D, Jones AD, DeLisi M, Kirkman G. Is female psychopathy linked with child abuse? An empirical investigation using a person-centered approach. J Child Sex Abus. 2019;28(6):708–725. doi:10.1080/10538712.2019.1592272
25. Akaike H. Factor analysis and AIC. Psychometrika. 1987;52(3):317–332. doi:10.1007/BF02294359
26. Schwarz G. Estimating the dimension of a model. Annals of statistics. Psychometrika. 1978;6:461–464.
27. Sclove SL. Application of model-selection criteria to some problems in multivariate analysis. Psychometrika. 1987;52(3):333–343. doi:10.1007/BF02294360
28. Lo YT, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. doi:10.1093/biomet/88.3.767
29. Kang SJ, Cho YR, Park GM, et al. Predictors for functionally significant in-stent restenosis: an integrated analysis using coronary angiography, IVUS, and myocardial perfusion imaging. JACC Cardiovasc Imaging. 2013;6(11):1183–1190. doi:10.1016/j.jcmg.2013.09.006
30. Bartlett ML, Taylor H, Nelson JD. Comparison of mental health characteristics and stress between baccalaureate nursing students and non-nursing students. J Nurs Educ. 2016;55(2):87–90. doi:10.3928/01484834-20160114-05
31. Ma CM, Lai CC. Mental health profile and health-related behavior among Hong Kong Chinese university students. Health Psychol Open. 2018;5(2):2055102918786869. doi:10.1177/2055102918786869
32. Moxham LJ, Fernandez R, Kim B, Lapkin S, Ten Ham-baloyi W, Al Mutair A. Employment as a predictor of mental health, psychological distress, anxiety and depression in Australian pre-registration nursing students. J Prof Nurs. 2018;34(6):502–506. doi:10.1016/j.profnurs.2018.03.005
33. Osimo SA, Aiello M, Gentili C, Ionta S, Cecchetto C. The influence of personality, resilience, and alexithymia on mental health during COVID-19 pandemic. Front Psychol. 2021;12:630751. doi:10.3389/fpsyg.2021.630751
34. Bacchi S, Licinio J. Resilience and psychological distress in psychology and medical students. Acad Psychiatry. 2017;41(2):185–188. doi:10.1007/s40596-016-0488-0
35. Southwick SM, Charney DS. The science of resilience: implications for the prevention and treatment of depression. Science. 2012;338(6103):79–82. doi:10.1126/science.1222942
36. Pakalniškienė V, Viliūnienė R, Hilbig J. Patients’ resilience and distress over time: is resilience a prognostic indicator of treatment? Compr Psychiatry. 2016;69:88–99. doi:10.1016/j.comppsych.2016.05.010
37. Ye ZJ, Liang MZ, Li PF, et al. New resilience instrument for patients with cancer. Qual Life Res. 2018;27(2):355–365. doi:10.1007/s11136-017-1736-9
38. Ye ZJ, Liang MZ, Zhang HW, et al. Psychometric properties of the Chinese version of resilience scale specific to cancer: an item response theory analysis. Qual Life Res. 2018;27(6):1635–1645. doi:10.1007/s11136-018-1835-2
39. Ye ZJ, Zhang Z, Tang Y, et al. Development and psychometric analysis of the 10-item resilience scale specific to cancer: a multidimensional item response theory analysis. Eur J Oncol Nurs. 2019;41:64–71. doi:10.1016/j.ejon.2019.06.005
40. Ye ZJ, Zhang Z, Zhang XY, et al. State or trait? Measuring resilience by generalisability theory in breast cancer. Eur J Oncol Nurs. 2020;46:101727. doi:10.1016/j.ejon.2020.101727
41. Ye ZJ, Zhang Z, Tang Y, et al. Minimum clinical important difference for resilience scale specific to cancer: a prospective analysis. Health Qual Life Outcomes. 2020;18(1):381. doi:10.1186/s12955-020-01631-6
42. Liang MZ, Tang Y, Chen P, et al. New resilience instrument for family caregivers in cancer: a multidimensional item response theory analysis. Health Qual Life Outcomes. 2021;19(1):258. doi:10.1186/s12955-021-01893-8
43. Chow KM, Tang FWK, Tang WPY, Leung AWY. Resilience-building module for undergraduate nursing students: a mixed-methods evaluation. Nurse Educ Pract. 2020;49:102912. doi:10.1016/j.nepr.2020.102912
44. Ye ZJ, Liang MZ, Qiu HZ, et al. Effect of a multidiscipline mentor-based program, Be Resilient to Breast Cancer (BRBC), on female breast cancer survivors in mainland China-A randomized, controlled, theoretically-derived intervention trial. Breast Cancer Res Treat. 2016;158(3):509–522. doi:10.1007/s10549-016-3881-1
45. Ye ZJ, Qiu HZ, Liang MZ, et al. Effect of a mentor-based, supportive-expressive program, Be Resilient to Breast Cancer, on survival in metastatic breast cancer: a randomised, controlled intervention trial. Br J Cancer. 2017;117(10):1486–1494. doi:10.1038/bjc.2017.325
46. Ye ZJ, Zhang Z, Zhang XY, et al. Effectiveness of adjuvant supportive-expressive group therapy for breast cancer. Breast Cancer Res Treat. 2020;180(1):121–134. doi:10.1007/s10549-020-05526-4
47. Ye ZJ, Zhang Z, Tang Y, et al. Resilience patterns and transitions in the Be Resilient To Breast Cancer trial: an exploratory latent profile transition analysis. Psychooncology. 2021;30(6):901–909. doi:10.1002/pon.5668
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.