")
Back to Journals » International Medical Case Reports Journal » Volume 13
Heroin Intoxication Through Damaged Skin in a 7-Year-Old Girl
Authors Delirrad M , Sedokani A
Received 22 April 2020
Accepted for publication 19 August 2020
Published 26 August 2020 Volume 2020:13 Pages 379—382
DOI https://doi.org/10.2147/IMCRJ.S259326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Mohammad Delirrad,1 Amin Sedokani2
1Department of Forensic Medicine and Toxicology, School of Medicine, Urmia University of Medical Sciences, Urmia, Iran; 2Cardiology Department, Medical Faculty, Urmia University of Medical Sciences, Urmia, Iran
Correspondence: Amin Sedokani Cardiology Department, Medical Faculty
Urmia University of Medical Sciences, 17 Sharivar St, Urmia 571478334, Iran
Tel +98 44 3237 5907
Fax +98 44 3237 2917
Email [email protected]
Abstract: Transdermal opioid intoxication has only been reported for pharmaceutical fentanyl and buprenorphine patches. Here, we report a rare case of heroin poisoning through damaged skin. A seven-year-old girl with an impaired level of consciousness and difficulty breathing was brought to a local hospital about one hour after burning with boiling water. She had a small second-degree burn on the right elbow. Clinicians were initially unable to obtain any reliable history from relatives about the cause of altered mental status. However, with a clinical suspicion of opioid poisoning, naloxone therapy started, and the patient was moderately improved. She underwent a coma workup; then she was referred to a tertiary care hospital. Further investigation revealed that after the burning, the mother left home to seek for a burn ointment from a neighbor, and the heroin-dependent father sprinkled some heroin powder over the burned area. Heroin was absorbed through the damaged skin and poisoned the child unintentionally. After three days of clinical management, the patient was discharged from the hospital in good condition without any complications. Heroin can be absorbed through damaged skin and cause poisoning. Diagnosis requires strong clinical suspicion, and an appropriate naloxone therapy may be life-saving.
Keywords: heroin, opioid poisoning, damaged skin, transdermal absorption, naloxone
Introduction
Heroin (diamorphine or diacetylmorphine) is a highly addictive semisynthetic opioid made from morphine.1 Intoxication by opioids may occur through ingestion, inhalation, or injection. Among opioids, transdermal poisoning has only been reported for fentanyl and buprenorphine pharmaceutical patches.2,3 Here, we present a rare case of heroin poisoning through damaged skin.
Case Presentation
A seven-year-old girl was burnt by boiling water at home in a rural place in the Northwest of Iran. The burnt area was on the right elbow. Her mother left home to take a burn ointment from the neighbor and rubbed it over the burnt area. An hour later, the mother brought the girl to the local city hospital with an impaired level of consciousness and difficulty breathing. The family provided no more history than the burn. A general practitioner and afterward, a pediatrician visited the patient. She was unconscious without responding to any painful stimuli, had pinpoint pupils and apneustic respirations (respiratory rate: 6 per minute). Other vital signs were stable (pulse rate 90 bpm, blood pressure: 90/60 mmHg, and body temperature 36.5 °C). An oval shape second-degree burnt area with the dimensions of 3 cm × 4 cm (approximately 0.25% of the body surface area) was seen over the posterolateral aspect of the right elbow covered with a burn ointment (Zinc oxide 30% plus Fish oil 50%). With a clinical suspicion of opioid poisoning, intravenous (IV) naloxone 0.2 mg was injected four times at 2 to 5 minutes intervals (total dose: 0.8 mg), and the level of consciousness of the patient was improved. The burn site was washed using normal saline, and the burn dressing resumed. Nonetheless, considering other differential diagnoses, the essential laboratory examinations, including a brain computed tomography (CT) scan without contrast, and a lumbar puncture were performed. Then, the patient was referred to a tertiary care pediatric hospital located in the center of the province for further management.
Four hours later, the patient arrived at the destination hospital emergency room, and she was immediately admitted to the pediatric intensive care unit. A pediatric resident and a toxicologist visited the patient. She was in a light coma (just poorly respond to painful stimuli) and had meiotic pupils and apneustic respirations. Her level of consciousness and breathing became better after receiving a bolus of 0.8 mg IV naloxone. Other treatments for the patient included: fluid therapy, continuous naloxone infusion (0.01 mg/kg/hour for 24 hours), ranitidine (50 mg IV every 12 hours), ceftriaxone (900 mg IV every 12 hours), and topical silver sulfadiazine 1% ointment (every 12 hours on the burnt area).
Laboratory studies of the patient are summarized in Table 1. Furthermore, a chest x-ray and a brain CT scan were unremarkable.
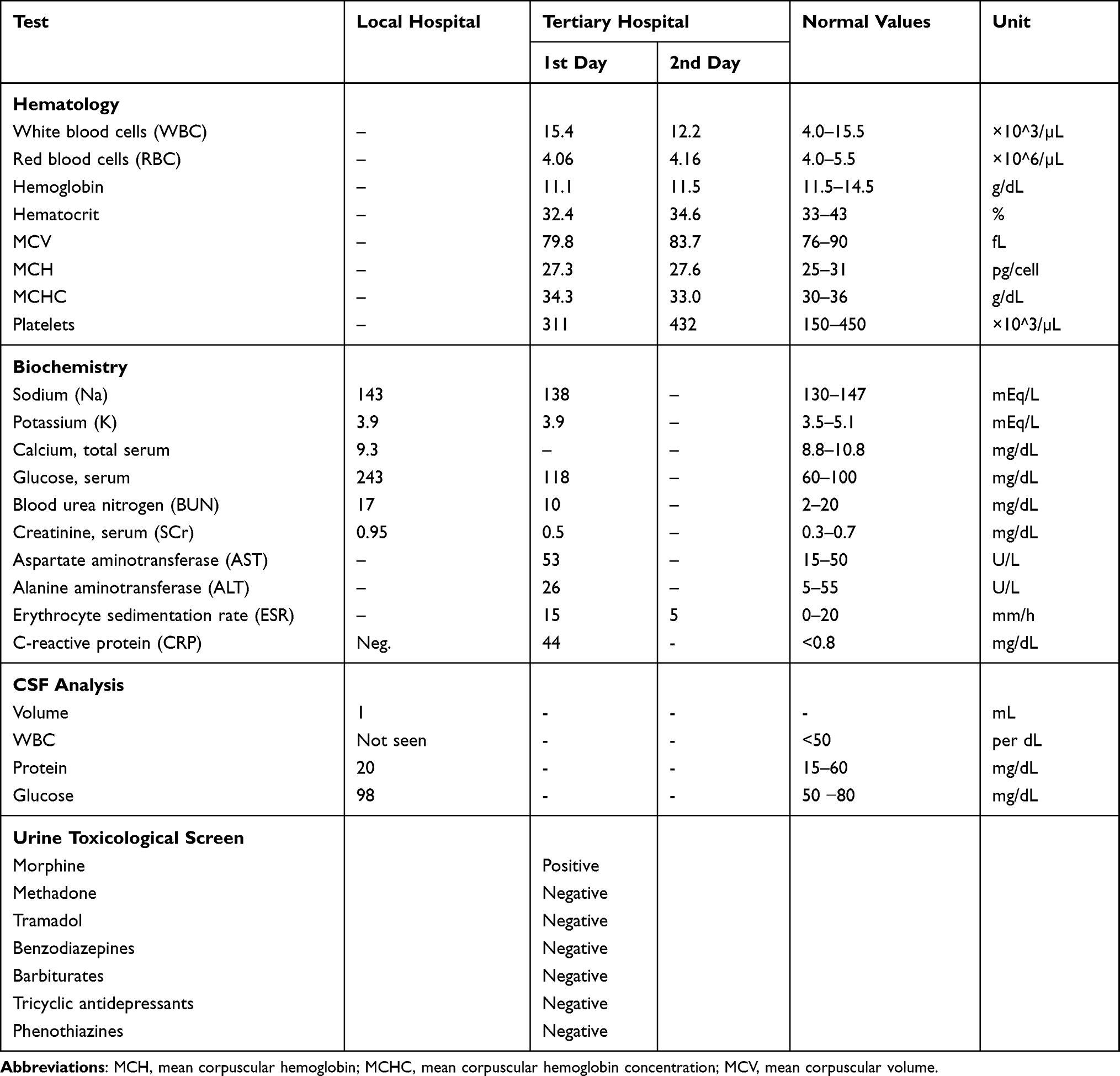 |
Table 1 Laboratory Findings of the Patient (7-Year-Old Girl) Who Accidentally Intoxicated by Heroin Sprinkled on Burnt Skin |
Initially, clinicians were unable to obtain any reliable information from the patient’s parents about the circumstances of intoxication. Further investigation revealed that after burning, the mother left home to seek for a burn ointment from the neighbors, and the patient was left alone with her heroin-dependent father. By observing the agitation of his daughter, the father sprinkled some heroin powder over the burnt area. Then the mother, unaware of everything, rubbed the burn ointment on the burn. Heroin gradually penetrated the damaged skin and led to the unintentional poisoning of the child. On the third day of hospitalization, the patient was discharged in good condition without any complications.
Discussion
We reported an unusual case of heroin empoisoning through the damaged skin. The doctors initially diagnosed the probable opioid intoxication in the local hospital, and the patient’s general condition improved after the injection of naloxone as an antidote. However, during the four-hour route to the destination hospital, they forgot to schedule for naloxone maintenance therapy. The relatively short duration of action of naloxone (20 to 90 min) must be borne in mind, because a severely-depressed patient may recover after a single dose of naloxone and appear healthy, only to relapse into a coma after 1–2 hours when naloxone effect dissipates.4,5
After IV injection or snorting, the duration of action of heroin is usually short (half-life 3–6 minutes) because it rapidly reacts to its metabolites (6-monoacetyl morphine, morphine, morphine-3-glucuronide, and morphine-6-glucuronide). However, the elimination of the metabolites depends on many factors such as the route of administration, dose, body weight, the time elapsed since the last dose, and inter-individual pharmacokinetics.5 Although it is not precisely clear, similar metabolism may occur in the body after the transdermal absorption of heroin.
Together with the diagnosis of opioid intoxication, the doctors considered other differential diagnoses in the local hospital and performed a brain CT scan, a lumbar puncture, and probably used hypertonic dextrose. As a result, the patient’s serum and cerebrospinal fluid glucose were high. As well as, in our hospital, the patient had leukocytosis and a positive C reactive protein (CRP) and received antibiotics with suspicion of infection.
Considering the banning of poppy cultivation in Iran, dietary use is infrequent, and the child has no history of eating poppy seeds or opium. Therefore, the positive qualitative urine immunoassay screen for morphine was related to heroin. Unfortunately, the urinary assay for 6-monoacetyl morphine, which is specific for heroin, was not available in our hospital.
While most opioids are not well- absorbed from intact skin, but percutaneous absorption of drugs (eg, morphine) will significantly increase if the epidermal barrier is damaged or diseased.6 Especially, young children with burns and infants with extensive skin disease (particularly eczema) may be at higher levels of risk.
Among opioids, there are only fentanyl and buprenorphine that possess ideal characteristics for transdermal delivery. It means they are small molecules (molecular weight: 336.5 and 467.6 g/mol, respectively) with high lipophilicity.3,6,7 Hence, there are numerous descriptions of fatal and non-fatal intoxication of transdermal fentanyl. As well as, there is only one report of buprenorphine overdose by using transdermal patches.2,3,8 Another study evaluated a new morphine patch for transdermal administration.9
Although heroin is a small lipophilic molecule (MW: 369.4g/mol), to the best of our knowledge, transdermal heroin intoxication has never been reported in the literature. Our patient has been the first case report of heroin poisoning through the damaged skin that was fortunately diagnosed and appropriately treated. In many situations like the reported case, the diagnosis of opioid intoxication requires strong clinical suspicion. In other words, taking a precise history, using confirmatory urine toxicological screen, and an appropriate naloxone therapy could be life-saving.
Whether covering the burnt area with the burn ointment in our patient may lead to more entrapment, and absorption of heroin transdermally is unclear for us. However, the possibility of transdermal absorption as a new route for pharmaceutical heroin deserves attention in further investigations.
Ethical Statement
The patient’s parents had the opportunity not to accept the study. The patient’s parents both provided written informed consent for the case details to be published and the patient’s personal information remained confidential. There was no cost or harm to the patient for the study. All of the stages of the study were under supervision and confirmation of the ethical committee of Taleghani Teaching hospital and Urmia Medical Sciences University.
Funding
This study (case report) has no kind of funding.
Disclosure
The authors report no kind of conflict of interest in this report.
References
1. Akhgari M, Etemadi-Aleagha A, Jokar F. Street level heroin, an overview on its components and adulterants. In: Neuropathology of Drug Addictions and Substance Misuse. Preedy VR, editor. 867877. Elsevier Inc; 2016:chap 81.
2. Nara A, Yamada C, Saka K, et al. A fatal case of poisoning with fentanyl transdermal patches in Japan. J Forensic Sci. 2019;64(6):1936–1942. doi:doi:10.1111/1556-4029.14127
3. Magdalan J, Merwid-Lad A. Transdermal buprenorphine intoxication. Clin Toxicol. 2008;46(9):915–916. doi:doi:10.1080/15563650701834672
4. Nelson LS, Howland MA. Opioid Antagonists. In: Goldfrank’s Toxicologic Emergencies. Hoffman RS, Nelson LS, Goldfrank LR, Howland MA, Lewin NA, Smith SW, editors.
5. Rzasa Lynn R, Galinkin JL. Naloxone dosage for opioid reversal: current evidence and clinical implications. Ther Adv Drug Saf. 2018;9(1):63–88. doi:doi:10.1177/2042098617744161
6. Leppert W, Malec-Milewska M, Zajaczkowska R, Wordliczek J. Transdermal and topical drug administration in the treatment of pain. Molecules. 2018;23(3):681. doi:doi:10.3390/molecules23030681
7. Pathan H, Williams J. Basic opioid pharmacology: an update. Br J Pain. 2012;6(1):11–16. doi:doi:10.1177/2049463712438493
8. Bartram U, Schmidt R. [Transdermal intoxication through broken opioid ampules: accidental intoxication in a paramedic]. Der Anaesthesist. 2020;69(2):122–125. doi:doi:10.1007/s00101-020-00732-7.
9. Inui N, Kato T, Uchida S, et al. Novel patch for transdermal administration of morphine. J Pain Symptom Manage. 2012;44(4):479–485. doi:doi:10.1016/j.jpainsymman.2011.10.022
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.