")
Back to Journals » International Medical Case Reports Journal » Volume 14
Hepatitis C Virus Reactivation Following COVID-19 Vaccination – A Case Report
Authors Lensen R , Netea MG, Rosendaal FR
Received 9 July 2021
Accepted for publication 21 August 2021
Published 29 August 2021 Volume 2021:14 Pages 573—576
DOI https://doi.org/10.2147/IMCRJ.S328482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Ruud Lensen, 1 Mihai G Netea, 2, 3 Frits R Rosendaal 4
1Cordaan Health Care Organization, Amsterdam, the Netherlands; 2Department of Internal Medicine and Radboud Center for Infectious Diseases, Radboud University Medical Center, Nijmegen, the Netherlands; 3Department of Immunology and Metabolism, Life and Medical Sciences Institute, University of Bonn, Bonn, Germany; 4Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, the Netherlands
Correspondence: Ruud Lensen
Cordaan Health Care Organization, Amsterdam, the Netherlands
Tel +31204356300
Email [email protected]
Purpose: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection impacted morbidity and mortality during the pandemic of 2020– 2021. A number of anti-COVID-19 vaccines have been developed with an unprecedented speed. While these vaccines have good efficacy and are safe, the experience with their use is limited and hence the knowledge of rare side effects. Identifying rare complications is important for future safe use of these vaccines.
Materials and Methods: Here, we report a case of a 82-year old patient with dementia who was admitted to a nursing home in the Netherlands. After vaccination with COVID-19 vaccination, physical examinations and lab tests were performed.
Results: She had a reactivation of hepatitis C infection after vaccination with the mRNA-based Pfizer–BioNTech COVID-19 vaccine. This reactivation manifested with jaundice, loss of consciousness, hepatic coma and death.
Conclusion: This reactivation of hepatitis C virus after vaccination with the Pfizer–BioNTech COVID‑19 vaccine suggests a need for critical consideration of individuals with prior HCV infection and considered for COVID-19 vaccination.
Keywords: SARS-CoV-2, hepatitis C, virus reactivation, COVID-19 vaccination
A Letter to the Editor has been published for this article.
Corrigendum for this paper has been published
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection (Covid-19) emerged as a pandemic at the beginning of 2020.1 Several vaccines against Covid-19 have been developed with unprecedented speed, some of them using novel technologies such as mRNA-based approaches. While large Phase 3 trials provided evidence for efficacy and safety, registration of post-licensing is crucial for future safe use of these novel technologies. Here, we report a case of a hepatitis C virus reactivation following COVID-19 vaccination using the mRNA-based anti-COVID19 vaccine produced by BioNTech/Pfizer.
Materials and Methods
A 82 years old woman with dementia [Alzheimer’s disease] was admitted to a nursing home in the Netherlands in 2020. Her medical history included hepatitis C infection [2007], hepatitis B infection [1980], diabetes mellitus type 2 [2005], essential hypertension [2001], osteoarthritis [2007], portal hypertension with esophageal varices [2015], hepatic cirrhosis with thrombocytopenia, and allergy to wasp sting [2014]. She had slightly increased liver enzymes [AST, ALT, GGT, ALP], but normal bilirubin [since 2011]. The patient never tested positive for COVID - 19.
On 21 February 2021, the patient was vaccinated against COVID-19 using Pfizer–BioNTech COVID‑19 vaccine [first dose]. During the first two days after the first vaccination, no symptoms or signs were observed.
Results
On day 3 after vaccination jaundice, somnolence and chills were noticed. On clinical examination there was an obvious jaundice of skin and sclerae; her consciousness was decreased. Rectal temperature 38.1C, heart rate 92 bpm, oxygen saturation 95% [no dyspnea], blood pressure 105/93 mmHg. Two hours later rectal temperature was 37.4C, consciousness was somewhat improved, whereas other vital signs remained abnormal. Color of urine and feces was normal. Blood glucose levels were normal.
Between day 4 and 10 the patient consciousness improved and the jaundice cleared.
After day 10 of follow-up manifest jaundice again increased, accompanied by severe pain in the upper right abdomen, irradiating to the upper left abdomen, followed by loss of consciousness, coma and death on day 23. Hepatitis C was confirmed by the blood test. Patient refused treatment with hepatitis C medication.
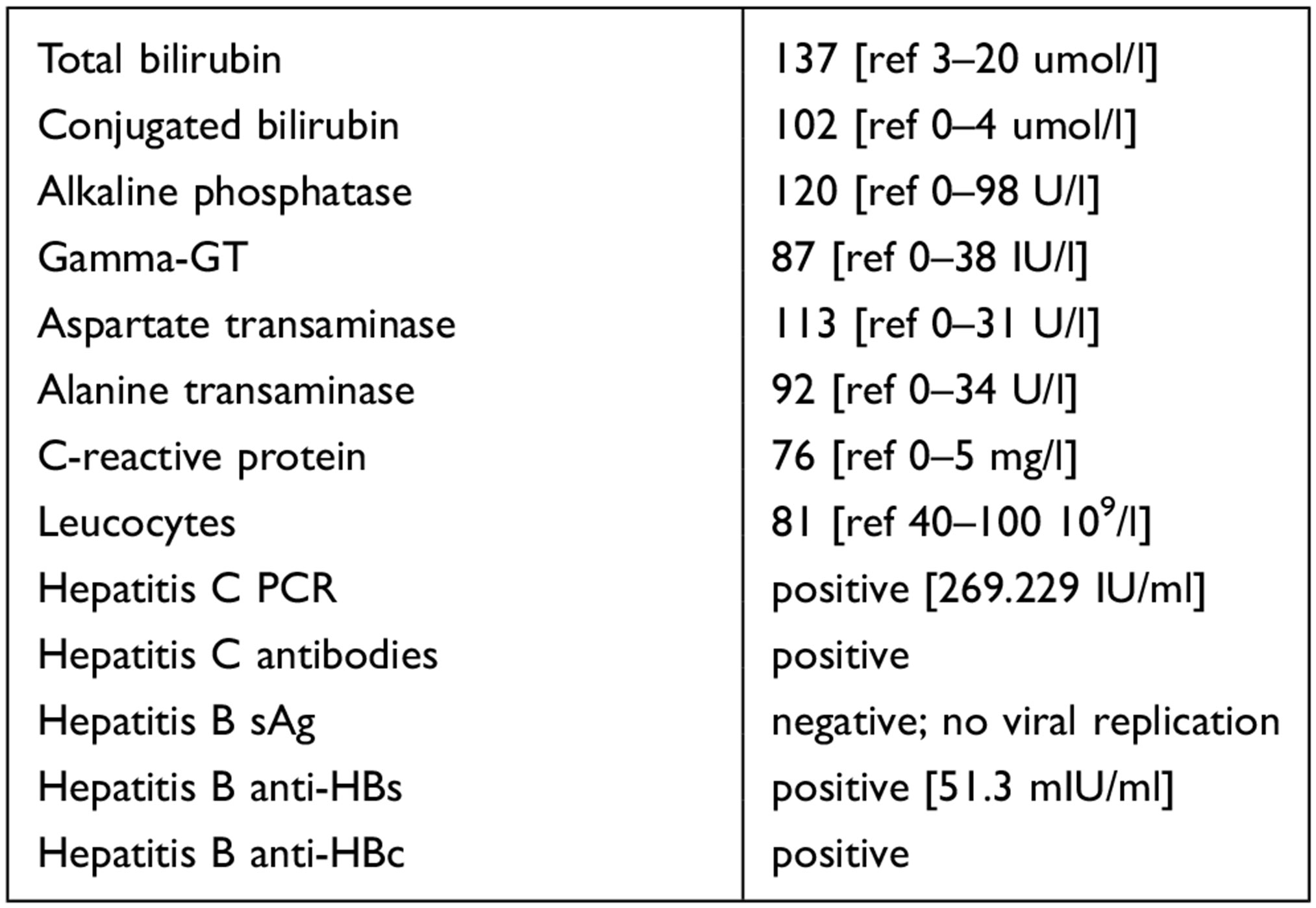
Blood test on day 5 showed:
 |
|
A second blood test on day 14 showed a decrease of bilirubin and CRP levels, but a further increase of liver enzymes AST, ALT and ALP.
Discussion
An 82-year old woman with multiple morbidities had reactivation of hepatitis C infection after vaccination with the mRNA-based Pfizer–BioNTech COVID-19 vaccine. Injection of fragments of mRNA that encode viral antigens induces a long-term immune response against COVID-19. Most frequently occurring side effects are mild, with transient fatigue and headache being the most common, followed by (in order of frequency): pain and swelling at the injection site, muscle aches, chills, joint pain, fever [more common after the second dose] and allergic reactions.2,3 However, the short-term experience with this new type of vaccines needs to be complemented by careful observation of the population after large-scale introduction of the vaccine, in order to monitor the occurrence of rare side effects.
In our patient a strong increase in HCV load occurred a few days after vaccination. While we cannot exclude a coincidental occurrence of the HCV load increase by chance after the vaccination, a causal relationship seems likely given the close temporal proximity of vaccine administration and the elevated HCV. An alternative explanation is that she used oxycodone, which may induce cholestasis and thereby possibly viral reactivation. However, low-dose (5 mg daily) oxycodone had been already started six weeks before vaccination, i.e. without a close temporal proximity to HCV reactivation.
In addition, one might argue that there had been a sustained viral response after the onset of hepatitis C in 2007, which, however, did not cause jaundice. Rather, an inflammatory response to the vaccine (in combination with the presence of viral replication) could have been sufficient to cause decay of liver cells, leading to her symptoms and severity of the disease. However, after the episode of hepatitis C in 2007, no other episodes of jaundice or other symptoms of liver disease occurred, apart from a stable slight increase in liver enzymes. Moreover, an episode of pneumonia six months before the current episode was not followed by any of these liver symptoms. However, in the absence of HCV viral load measurements between 2007 and 2020, we cannot fully rule out this possibility.
The most likely explanation therefore is an HCV reactivation, caused by the COVID-19 vaccination. It is known for other vaccines that they can cause virus reactivation, especially in immunosuppressed patients and patients undergoing cancer treatment, eg as described for the herpes zoster subunit vaccine, causing reactivation of herpes zoster stromal keratitis.4 SARS-CoV-2 encoded proteins [and some anti-COVID-19 drugs] are able to induce reactivation of Kaposi’s sarcoma-associated herpesvirus.5
Hepatitis C virus reactivation has been described in patients receiving cancer treatments, in whom HCV reactivation occurred in 23% of patients.6 Another study revealed that psoriasis patients with hepatitis C infection were at risk for HCV reactivation with the use of biologic therapies.7
So far, no virus reactivations have been described after COVID-19 vaccination. We can only speculate on the mechanisms through which vaccination could have reactivated HCV. One possibility, as in the case of Kaposi sarcoma-associated herpesvirus, is that SARS-CoV-2 encoded proteins may cause reactivation of the hepatitis C virus. Alternatively, an indirect mechanism through induction of inflammation and cytokines, that would subsequently influence viral replication, is also possible.
Finally, from another perspective, a COVID vaccination followed by jaundice may reveal [by supplementary diagnostics] a previously unrecognized but now reactivated hepatitis C infection.
Conclusion
This study describes a case of hepatitis C reactivation following COVID-19 vaccination. The patient received no hepatitis C medication and died three weeks following COVID-19 vaccination of liver failure. No other cases with a history of HCV infection and cirrhosis with a similar fatal course following COVID-19 vaccination have been described. This suggests a need for critical consideration of individuals with prior HCV infection and considered for COVID-19 vaccination.
Abbreviations
ALP, Alkaline phosphatase; ALT, Alanine transaminase; anti-HBs, anti-hepatitis B surface; anti-HBc, anti hepatitis B core; AST, Aspartate transaminase; bpm, Beats per minute; COVID – 19, Coronavirus disease 2019; CRP, C-reactive protein; GGT, Gamma-glutamyltransferase; HCV, Hepatitis C virus; IU, International units; Ml, Millilitre; mRNA, messenger ribonucleic acid; PCR, Polymerase chain reaction; sAg, surface antigen; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available, due to the fact that they contain personal information, but are available from the corresponding author on reasonable request.
Ethics Approval and and Informed Consent
Ethics approval was not required and the patient’s next of kin gave her written consent to participate. Our study follows the principles of the Declaration of Helsinki.
Consent for Publication
Written informed consent was obtained from the patient’s next of kin for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal. The patient cannot be identified via the case report by fully anonymizing her.
Acknowledgments
We would like to thank all the staff at the Cordaan Health Care Organization for their approval for this submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There were no sponsors involved.
Disclosure
The authors report no conflicts of competing interest in this work.
References
1. World Health Organization. COVID-19 Public Health Emergency of International Concern (PHEIC) Global Research and Innovation Forum. World Health Organization; 2020.
2. Oliver SE, Gargano JW, Marin M, et al. The advisory committee on immunization practices’ interim recommendation for use of Pfizer-BioNTech Covid-19 vaccine - United States, December 2020. MMWR Morb Mortal Wkly Rep. 2020;69(50):1922–1924. doi:10.15585/mmwr.mm6950e2
3. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. doi:10.1056/NEJMoa2034577
4. Lehmann A, Matoba A. Reactivation of herpes zoster stromal keratitis after HZ/su adjuvanted herpes zoster subunit vaccine. Ophthalmology. 2018;125(11):1682. doi:10.1016/j.ophtha.2018.08.030
5. Chen J, Dai L, Barrett L, et al. SARS-CoV-2 proteins and anti-COVID-19 drugs induce lytic reactivation of an oncogenic virus. bioRxiv. 2020;4(1):1–6.
6. Torres HA, Hosry J, Mahale P, et al. Hepatitis C virus reactivation in patients receiving cancer treatment: a prospective observational study. Hepatology. 2018;67(1):36–47. doi:10.1002/hep.29344
7. Patterson AT. JAAD game changers: risk for hepatitis B and C virus reactivation in patients with psoriasis on biologic therapies: a retrospective cohort study and systematic review of the literature. J Am Acad Dermatol. 2020;82(2):532. doi:10.1016/j.jaad.2019.09.055
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.