")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Hepatitis C Virus Infections in Patients with Hemophilia: Links, Risks and Management
Authors Spanoudaki A , Papadopoulos N , Trifylli EM , Koustas E, Vasileiadi S, Deutsch M
Received 18 July 2022
Accepted for publication 5 October 2022
Published 10 October 2022 Volume 2022:15 Pages 2301—2309
DOI https://doi.org/10.2147/JMDH.S363177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anastasia Spanoudaki,1,* Nikolaos Papadopoulos,2,* Eleni-Myrto Trifylli,2 Evangelos Koustas,2 Sofia Vasileiadi,1 Melanie Deutsch1
1 2nd Academic Department of Internal Medicine, Hippokration General Hospital of Athens, Medical School of National & Kapodistrian University of Athens, Athens, Greece; 2 1st Department of Internal Medicine, 417 Army Share Fund Hospital, Athens, Greece
*These authors contributed equally to this work
Correspondence: Nikolaos Papadopoulos, 1st Department of Internal Medicine, 417 Army Share Fund Hospital, Ravine 14-16 str, Athens, 11521, Greece, Tel +302117100671, Email [email protected]
Abstract: Haemophilia is a rare, hereditary bleeding disorder. Clotting factor concentrates were a revolutionary treatment which changed the life of people with haemophilia. However, early generation of clotting factor concentrates, without viral inactivation procedures in the manufacturing process, led to an increased risk of transmission of blood-borne viral infections, mainly due to hepatitis C virus and human immunodeficiency virus. As only 20% of HCV-infected patients clear the infection naturally, chronic HCV infection constitutes a serious health problem and a major cause of chronic liver disease in this group of patients. Fortunately, the use of viral inactivation procedures in the plasma-derived factor concentrates manufacturing process and the availability of alternative treatment options, led to a significant reduction of transfusion-associated viral infections. The advent of multiple, orally administrated, highly effective direct-acting antivirals (DAAs) is changing the natural history of HCV infection in patients with haemophilia as these drugs have an excellent safety profile and achieve very high sustained virological response rates, similar to the general population. Eradication of HCV-infection in patients with haemophilia is feasible via micro-elimination projects.
Keywords: hepatitis C virus, haemophilia, direct-acting antivirals, micro-elimination projects
Introduction
Chronic hepatitis C (CHC) is a severe public health problem and a significant cause of chronic liver disease.1 Approximately 80% of patients with acute disease slowly progress to chronic infection. These patients are at a higher risk for cirrhosis, end-stage liver disease (ESLD), and hepatocellular carcinoma (HCC).2 In 2020, the global prevalence of viraemic hepatitis C virus (HCV) infection was estimated at 56.8 million infections worldwide. Although this number represents a decrease compared to the estimated prevalence in 2015, the global HCV elimination target stated by the World Health Organization (WHO) by 2030 appears challenging.3 In order to overcome the difficulties arising from the high number of affected individuals and the different patterns of risk for the disease across sub-populations and geographic areas, the concept of micro-elimination has been introduced. This involves breaking down national elimination targets into targets focused on smaller subgroups. These tailored interventions can accelerate the implementation of prevention and treatment strategies in specific sub-populations and settings.4 As HCV has a blood-borne transmission, transfusion-dependent subjects such as patients with bleeding disorders are theoretically at a significant risk of viral acquisition. However, due to the application of effective prevention plans and the universal screening of blood products and blood-derived clotting factors, HCV infection has significantly decreased in this special group of patients during the last two decades.5 Nevertheless, this is the case in industrialized countries, whereas in developing countries, the prevalence of HCV infection still remains high due to the inadequate application of universal precautions in health care.6
Bleeding disorders include especially haemophilia which represents rare, hereditary X-linked disorders caused by the deficiency or dysfunction of coagulation factor VIII (haemophilia A) or IX (haemophilia B). Bleeding manifestations are roughly proportional to the degree of factor deficiency in plasma.7 The prevalence of haemophilia (per 100,000 males) is 17.1 cases for all severities of haemophilia A and 3.8 cases for all severities of haemophilia B. The expected number of patients with haemophilia worldwide is 1125 000, of whom 418 000 have a more severe clinical phenotype.8 Until 1990, before the existence of viral inactivation procedures and the advent of alternative treatment options, the majority of patients with haemophilia were treated with unsafe plasma-derived factor concentrates. As a result, most patients acquired HCV infection.9,10 A subset of patients also acquired transfusion-associated co-infection with the human immunodeficiency virus (HIV) which results in a more accelerated course of CHC.11 In HCV mono-infected patients, rates of progression to end-stage liver disease (ESLD) are similar to that in HCV-positive individuals in the general population. The management of CHC in patients with haemophilia (either mono or coinfected) is not different from that of individuals without haemophilia.12
In this article, we aimed to review comprehensively the data regarding the links, the risks and the management of HCV infection in patients with haemophilia.
Links
Until the 1960s, the only available treatment for haemophilia patients was the transfusion of fresh blood or fresh frozen plasma (FFP). These replacement methods were of poor clinical efficacy, poorly tolerated in terms of volume overload and carried the risk of HCV transmission. A first step forward was the demonstration in 1964 by Judith Pool that cryoprecipitation of fresh-frozen plasma was able to concentrate FVIII and was more efficient than FFP as replacement therapy for haemophilia A.7,13 However, the treatment of a bleeding episode would require several units of cryoprecipitate and multiple infusions, further increasing the risk of viral transmission. Commercially fractionated factor concentrates were introduced in the 1970s and represented a significant improvement in patients’ treatment.14 These concentrates have proved to be highly infectious as being produced from large donations’ pools. Especially, batches manufactured from blood originating from commercial source plasma clinics with paid donors and located near areas with a high prevalence of illicit drug use had higher HCV seropositivity compared to batches issued from volunteer donors.15
In the late 1970s through the mid-1980s, directly related to the increasing use of fractionated factor concentrates, the frequency of post-transfusion hepatitis also increased. The infective agent involved was at that time termed non-A, non-B hepatitis since HCV was not yet discovered. It was later established that HCV was the causative agent of >90% of these cases of post-transfusion hepatitis.16 At around the same period, in 1983, the recognition of human immunodeficiency virus (HIV) transmission to blood-product recipients accelerated the efforts to apply adequate measures in order to prevent transmission of infectious agents via transfusions.17 As a result, in 1985, several companies introduced viral inactivation procedures for hemophilia blood products and by 1987 these procedures were uniformly used. The implementation of primary measures such as donor selection and screening of individual donations and plasma pools for serologic markers and nucleic acids for blood‐borne viruses has been proved effective in reducing the risk of transfusion-transmitted infections (TTIs).17,18 The approval of the first recombinant human factor VIII in 1992 and recombinant factor IX in 1997 was a significant breakthrough in the treatment of patients with hemophilia.19 The production of the first generation of recombinant products required albumin for stabilization, which although considered safe, was still derived from human plasma. Recently developed recombinant products are formulated without any human proteins.18 Latest advances in haemophilia treatment include nonfactor products that act by enhancing coagulation or inhibiting anticoagulant pathways and are also totally deprived of viral transmission risk.20 The use of virucidal and viral exclusion steps in the plasma-derived factor concentrates manufacturing process and the availability of recombinant products and nonfactor treatments virtually eliminated the risk of TTIs. Although safe and efficacious factor products are widely available in Europe and North America, this is not the case in developing countries where patients with haemophilia may still receive transfusions of non-virus inactivated blood components, such as FFPs and cryoprecipitate.21 As a result, these patients continue to be vulnerable to hepatitis viruses and HIV transmission.22
Risks
The percentage of spontaneous HCV clearance in haemophilia patients is lower than in other HCV populations, probably due to the high prevalence of HIV co-infection, which decreases the probability of viral clearance.23 The main risks related to chronic HCV infection concern the progression to ESLD (defined as the occurrence of cirrhosis, bleeding oesophageal varices or liver-related death) and the development of HCC. Cirrhosis can occur in up to 20% of chronically infected patients, and of those with cirrhosis, 1–5% per year will develop HCC.2 A multicenter study from the Netherlands and the UK assessed the occurrence of ESLD in 863 HCV-infected patients with inherited bleeding disorders, of whom 91% suffered from haemophilia. During a median infection duration of 31 years. 81% developed CHC; 13% of chronically infected patients developed ESLD, and 3% were diagnosed with HCC.24 These numbers are higher than reported in another study which describes the natural history of a very large number (1818 patients) of HCV-infected patients with haemophilia, during a much shorter, however, period of follow up (median 12 years). 8% of this cohort developed ESLD, with only two reported HCC cases.25 Although these are the largest cohorts studying the natural course of CHC in patients with haemophilia, it should be underlined that they were conducted before the era of the direct-acting antiviral agents used for the treatment of CHC, which have dramatically changed the natural course of the disease.
The progression of liver disease and the development of HCC seem to be related to multiple risk factors such as a longer history of infection, presence of HCV genotype 1, HIV coinfection, and lifestyle characteristics such as alcohol abuse and the presence of the metabolic syndrome.11,26 The progression to ESLD is also negatively associated with antiviral treatment success.24
A long history of infection increases the risk of developing ESLD from a hazard ratio of 0.10/100 person-years in the first 10 years of infection to 0.90 after more than 20 years of infection.26 HCV genotype also seems to play a role in liver disease progression, although different studies have shown controversial results. Among haemophilia patients with CHC, the most common genotype was genotype 1 (65–70%).21 This is not unexpected, as genotype 1 is the virus mainly detected in people with risky behaviors, who were the primary donors for factor concentrates manufactured in the USA before 1985.15 Several studies suggest more rapid disease progression in patients with genotype 1 HCV infection.27–29 On the contrary, other studies indicate the absence of an association between genotype and liver disease progression.25,30
Before the advent of highly active antiretroviral treatment (HAART), antiretroviral regimens were highly hepatotoxic and contraindicated in patients with liver failure, resulting in worse prognosis in HCV/HIV-coinfected patients. HCV was an independent predictor of worse prognosis in HIV-infected hemophiliacs.31–33 The use of HAART has significantly improved the prognosis of HIV infection. As a result, liver disease is now the primary cause of morbidity in co-infected patients. HIV-coinfection was associated with an increased rate of progression of CHC to ESLD and HCC.31 Prospective studies reveal substantial differences between HCV mono-infected and HCV/HIV co-infected patients.25,34,35 An Israelian study compared patients with haemophilia and other bleeding disorders who were either HCV mono-infected, HCV/HIV co-infected, or non-HCV infected. Overall and liver-related 10-year survival were: 82.1 and 89.3%, 95.3 and 99.2 and 100% for HCV/HIV co-infected, HCV mono-infected, and non-infected haemophilia patients, respectively.34 In addition, HCV RNA levels are increased in HIV-positive patients with hemophilia, hastening the progression of liver disease.36 Co-infection is thus considered an independent risk factor for progression to ESLD.
Regarding lifestyle risk factors, alcohol abuse, defined as an intake of more than 20 units of alcohol per week, independently increased the risk of developing ESLD in the multicentre study from the Netherlands and the UK (HR 4.34).24 The role of metabolic factors in fibrosis progression in patients with chronic hepatitis C seems particularly important.37 Especially in genotype 3 infected patients, steatosis is considered a risk factor for fibrosis progression.38 However, it has not yet been studied as a risk factor in the analyses of large cohorts of HCV-infected haemophilia patients.24
As HCC is the leading cause of cancer in patients with CHC, it constitutes a significant risk for infected haemophilia patients.39 The higher prevalence of HCC in HCV-infected haemophilia patients in comparison to the general population and its more aggressive course in this patient group have long been observed.40,41 A recent American study analyzed hospital discharge data regarding HCC, between 1998 and 2014. One hundred forty-four men suffering from HCC, with or without haemophilia, were identified. Adjusted rates of HCC increased 3-fold in patients with haemophilia during the study period compared to 1.7 fold increase in patients without haemophilia, although this difference was not statistically significant. Furthermore, HCV was the primary predictor for HCC in haemophilia patients in multivariate logistic regression.42 Another study from the Netherlands, assessing the all‐cause and cause‐specific mortality in 1031 patients with hemophilia from 2001 to 2018, found increased mortality from HCC in HCV-infected haemophilia patients compared to the general male population.43
Management
The high rates of chronic infection and progression of liver disease in haemophilia patients infected with HCV made viral eradication crucial for this particular group of patients. The first treatments to be offered to these patients were the same as the ones indicated for the general population and included interferon (IFN) monotherapy, IFN with the addition of ribavirin, an oral antiviral drug, and later the replacement of IFN by pegylated IFN (PEG-IFN).44 In 2006, a review of 35 studies, including 1151 haemophilia patients, assessed the response-rate to the abovementioned regimens. HIV-negative and treatment naïve patients had sustained virological response (SVR) rates of 22% with IFN monotherapy, 43% with IFN plus ribavirin and 57% when treated with PEG-IFN plus ribavirin. Treatment results appeared to be similar to those observed at the general population.44 In HIV/HCV co-infected haemophilia patients, however, data are limited, showing a higher efficacy of PEG-INF plus ribavirin compared to IFN plus ribavirin or IFN monotherapy, with lower SVR rates.45,46
IFN-based treatments showed multiple limitations; their efficacy was insufficient, especially regarding patients with genotype 1 infection.47 IFN-based treatments also had significant side effects leading to reduced adherence to therapy, need for dose reduction, and frequent discontinuation. Patients most commonly experienced neuropsychiatric disorders such as irritability and severe fatigue. IFN also caused bone-marrow depression, flu-like symptoms, and autoimmune syndromes.48 The expected side-effects frequently led patients to decline treatment.49
The introduction of direct-acting antiviral agents (DAAs) revolutionized the management of chronic HCV infection.50 The first regimen, approved for treatment-naive patients with HCV genotype 1 infection, was called “triple therapy” and consisted of the protease inhibitors (PI) telaprevir or boceprevir, combined with PEG-IFN and ribavirin. “Triple therapy” led to high SVR rates of about 30% more than standard PEG-IFN-ribavirin regimens.51 In 2016, a study including DAAs in treating HCV patients with haemophilia was published. Fifty-one patients with haemophilia were treated with lambda-IFN, ribavirin, and daclatasvir. 90% among them achieved SVR12.52 The introduction of IFN-free and ribavirin-free regimens resulted in early HCV suppression and further revolutionized HCV-treatment.53 Nowadays, DAAs are divided into four classes based on their mechanism of action and their target in the viral replication cycle: nonstructural (NS) proteins 3/4A protease inhibitors (-previr), NS5B nucleoside polymerase inhibitors and NS5B non-nucleoside polymerase inhibitors (-buvir); and NS5A inhibitors (-asvir).54,55 Fixed combinations of the abovementioned DAAs lead to viral eradication in more than 98% of treated HCV patients.51 Although patients with haemophilia were not included in initial major studies on DAAs, there are studies confirming their efficacy in this specific group of patients. These studies include limited numbers of patients but still offer data on treating these patients with DAAs.
The efficacy and safety of the combination of sofosbuvir (SOF)/ledipasvir (LDV) plus ribavirin was studied in 14 patients with bleeding disorders (11/14 had haemophilia) infected with HCV genotype 1. They all achieved SVR12 with a mild profile of adverse events in 93% of them, mainly fatigue, headache, nausea, and insomnia.56 The combination of SOF/LDV was also evaluated in patients with bleeding disorders and genotype 1 or 4 infection, including treatment-experienced cirrhotic patients with genotype 1 infection. SOF with the addition of ribavirin was studied in patients with bleeding disorders and genotype 1 or 4 infection. Overall, 120 patients were treated. 91% among them suffered from haemophilia, and 22% were HIV coinfected. SVR12 rate was 99% (98/99) in patients with genotype 1 or 4 infection; 100% (5/5) in treatment-experienced cirrhotic patients with genotype 1 infection; 100% (10/10) in patients with genotype 2 infection; and 83% (5/6) in patients with genotype 3 infection. Treatment was well tolerated.57
Treatment with elbasvir (EBR)/grazoprevir (GZR) for 12 weeks, in patients with sickle cell anemia, thalassemia, haemophilia A/B or von Willebrand disease and HCV infection was assessed in the randomized, placebo-controlled Phase III C-EDGE IBLD study. Forty-seven of the 107 included patients suffered from haemophilia A/B or von Willebrand disease. 89.4% among them achieved SVR12 with favourable tolerability. The study also evaluated the presence of NS5A resistance-associated substitutions (RASs) among patients with genotype 1a infection, which was associated with significantly lower SVR rates.58
Another study evaluated the response of 30 haemophilia patients to different DAA treatments (SOF/LDV, daclatasvir (DCV)/asunaprevir (ASN), SOF plus ribavirin). SVR rates were 100% for eight patients with genotype 1a and 1b who received SOF/LDV for 12 weeks; 91% for 11 treatment-naïve patients with genotype 1b who received DCV/ASN for 24 weeks; 85.7% for seven treatment-experienced genotype 1b patients treated with DCV/ASN for 24 weeks; and 100% for four patients with genotype 2a/2b who received sofosbuvir plus ribavirin for 12 weeks. Serious adverse events leading to treatment discontinuation were not reported.59
The safety and efficacy of DAAs in HCV/HIV co-infected patients was evaluated in several studies. However, data regarding co-infected haemophilia patients were limited. A study from Japan included 27 HCV/HIV co-infected patients with bleeding disorders, 92% of whom had haemophilia. Genotype 1 and genotype 4 patients were treated with SOF/LDV, genotype 2 patients with SOF plus ribavirin, and genotype 3 patients with DCV/SOF. The SVR12 rate was 100%. However, it was noted that the occurrence of adverse events as well as the efficacy of combination antiretroviral therapy (cART) need to be closely observed in this group of patients.60 A retrospective analysis including 12 HCV/HIV co-infected haemophilia patients treated with different regimens (DCV/SOF, SOF/velpatasvir (VEL), SOF/PEG-IFN/ribavirin, SOF/ribavirin), showed an SVR24 rate of 91.7%. One patient failed treatment with SOF/PEG-IFN/ribavirin but achieved SVR with DCV/ASN for 12 weeks. Authors underlined the importance of surveillance regarding drug–drug interactions between DAAs and cART.61
Real-world studies of patients with haemophilia treated with DAAs confirm their efficacy. The most extensive real-world study included 200 haemophilia patients treated with different DAA regimens in two large Italian Hemophilia Treatment Centers. Patients showed an SVR-12 rate of 99% with no significant side effects. Forty patients among them were HCV/HIV co-infected.62
Smaller real-life data from different countries have been published. A case report from the Netherlands described two HCV genotype 1a/HIV coinfected patients with haemophilia and non-compensated cirrhosis, who received DCV/SOF for 24 weeks and both achieved SVR12.63 A study from Germany regarding 18 patients with inherited bleeding disorders and chronic HCV genotype 1 infection treated with DAAs reported an SVR-12 in 17/18 patients, without severe side effects.64
In a small case series from India, seven patients with bleeding disorders, 4 of them with haemophilia, were treated with DCV/SOF achieving an SVR-12 rate of 100%.65 Forty-three Japanese patients with haemophilia and genotype 1 or 4 HCV were treated with SOF/LDV for 12 weeks. Twenty among them were HIV-positive. SVR-12 rates were 100% in HIV-negative and 90% in HIV-positive patients. SVR rate was significantly lower in patients with cirrhosis (p = 0.005).66
In a retrospective study from northern Greece aiming to report the effects of chronic HCV in patients with inherited bleeding disorders, 74 patients suffering from chronic HCV. Treatment with DAAs (IFN-free) was implemented in three treatment-experienced patients with either DCV/SOF or SOF/simeprivir. All three patients achieved SVR12, with no significant side effects.67 A study from Slovenia reported an SVR rate of 98% among 63 HCV-infected patients with bleeding disorders, treated with IFN-including and IFN-free regimens. In total, 26 DAAs regimens were used, leading to an overall SVR rate of 88%. Slovenia is the first country to report the micro-elimination of HCV in the sub-population of patients with bleeding disorders.68
Eighty-five patients with hereditary bleeding disorders and HCV infection received different DAA regimens in Belgium. The SVR rate, measured in 84 among them, was 91.6%.69 A Portuguese retrospective analysis of a single-center cohort of HCV-infected haemophilia patients included 73 patients followed for 22 years. Among them, two treatment-naïve and 14 treatment-experienced patients were treated with DAAs, with an overall SVR-12 rate of 100%.10 An Iranian, bicentric, retrospective study reported the treatment results of 147 patients with hereditary bleeding disorders (132 of whom suffered from haemophilia) and CHC. Six (4,1%) patients were HCV/HIV co-infected and 37 (25.2%) had cirrhosis. All of them were treated with SOF-based IFN-free regimens. Of the 132 patients who completed treatment and were evaluated for SVR12, all achieved SVR.70
A retrospective, single-center study including 26 haemophilia patients with CHC infection was carried out in the Clinical Center of Vojvodina, in the northern region of Serbia. Nine of them received DAA regimens with an SVR rate of 100%. Authors report no patients with active HCV infection in the region’s haemophilia registry after 2020, making the Province of Vojvodina, a paradigm of successful micro-elimination strategy in the subpopulation of patients with haemophilia.71
An overview of studies reporting IFN-free treatment efficacy in inherited bleeding disorders is shown in Table 1. The results of the above mentioned studies underline the effectiveness and safety of DAAs for treating HCV infection in patients suffering from haemophilia and other bleeding disorders. The management of chronic hepatitis C in haemophilia patients and the indications for treatment are the same as in the population without haemophilia, based on published guidelines such as the updated recommendations of the European Association for the Study of the Liver (EASL).12
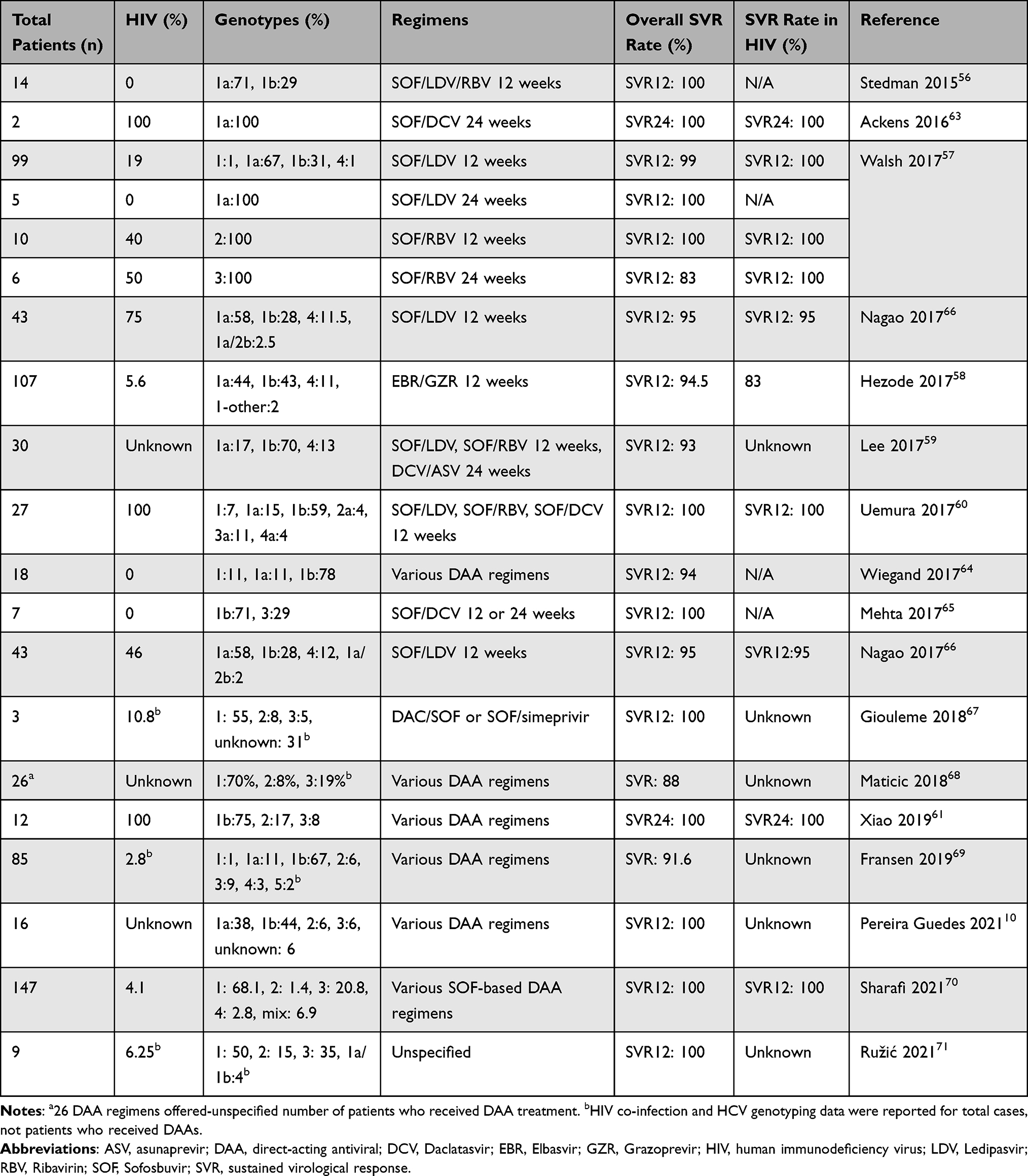 |
Table 1 Treatment of Hepatitis C Virus Infection with DAAs in Patients with Inherited Bleeding Disorders |
Some authors report concerns regarding the clinical benefit of HCV eradication in haemophilia patients remains unclear. A study from Japan compared the clinical outcomes of SVR in HCV patients with (n = 78) and without (n = 621) haemophilia and found no difference in the incidence of liver-related disease or overall death. There was also no significant difference in the cumulative incidence of HCC between the two groups.72 Although more data are needed regarding the impact of HCV cure in this subgroup of patients, in terms of public health and taking into account the WHO goal of HCV elimination up to 2030 treating all patients with HCV and inherited bleeding disorders represents an important step forward.
Conclusions
In the last two decades, the use of viral inactivation procedures in the manufacturing process of plasma-derived factor concentrates and the availability of recombinant products and nonfactor treatments have practically led to almost no new cases of transfusion-associated HCV infections in haemophilia patients. However, older generations of patients with haemophilia, already suffering from CHC, are in danger of ESLD and HCC. The use of DAAs has made HCV eradication possible, even for patients considered “difficult to treat”, such as HIV/HCV coinfected or genotype 1 infected patients. The WHO HCV elimination goal for 2030 is feasible in patients with haemophilia and other bleeding disorders, via micro-elimination projects.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Carmo RA, Martins ML, Chaves DG, Dezanet LNC. Prevalence and risk factors associated with hepatitis C among Brazilian male patients with haemophilia: a long‐term follow‐up. Haemophilia. 2019;25(3):447–455. doi:10.1111/hae.13728
2. Taherkhani R, Farshadpour F. Epidemiology of hepatitis C virus in Iran. World J Gastroenterol. 2015;21(38):10790–10810. doi:10.3748/wjg.v21.i38.10790
3. Blach S, Terrault NA, Tacke F, et al. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol. 2022;7(5):396–415. doi:10.1016/S2468-1253(21)00472-6
4. Lazarus JV, Wiktor S, Colombo M, Thursz M. EASL international liver foundation. Micro-elimination - a path to global elimination of hepatitis C. J Hepatol. 2017;67(4):665–666. doi:10.1016/j.jhep.2017.06.033
5. Jang TY, Lin PC, Huang CI, et al. Seroprevalence and clinical characteristics of viral hepatitis in transfusion-dependent thalassemia and hemophilia patients. PLoS One. 2017;12(6):e0178883. doi:10.1371/journal.pone.0178883
6. Roudot-Thoraval F. Epidemiology of hepatitis C virus infection. Clin Res Hepatol Gastroenterol. 2021;45(3):101596. doi:10.1016/j.clinre.2020.101596
7. Mannucci PM. Hemophilia therapy: the future has begun. Haematologica. 2020;105(3):545–553. doi:10.3324/haematol.2019.232132
8. Iorio A, Stonebraker JS, Chambost H, et al. Establishing the prevalence and prevalence at birth of hemophilia in males. Ann Intern Med. 2019;171(8):540–546. doi:10.7326/M19-1208
9. Pipe SW. New therapies for hemophilia. Hematology Am Soc Hematol Educ Program. 2016;2016(1):650–656. doi:10.1182/asheducation-2016.1.650
10. Pereira Guedes T, Garrido M, Kuttner Magalhães R, et al. Long-term follow-up of a Portuguese single-centre cohort of persons with haemophilia and hepatitis C virus infection. PJG. 2021;28(2):79–86. doi:10.1159/000510023
11. Rumi MG, Di Marco V, Colombo M. Management of HCV-related liver disease in hemophilia and thalassemia. Semin Liver Dis. 2018;38(2):112–120. doi:10.1055/s-0038-1655774
12. Pawlotsky JM, Negro F, Aghemo A, et al. EASL recommendations on treatment of hepatitis C: final update of the series☆. J Hepatol. 2020;73(5):1170–1218. doi:10.1016/j.jhep.2020.08.018
13. Pool JG, Shannon AE. Production of high-potency concentrates of antihemophilic globulin in a closed-bag system. N Engl J Med. 1965;273(27):1443–1447. doi:10.1056/NEJM196512302732701
14. Murphy N, O’Mahony B, Flanagan P, et al. Progression of hepatitis C in the haemophiliac population in Ireland, after 30 years of infection in the pre-DAA treatment era. Haemophilia. 2017;23(5):712–720. doi:10.1111/hae.13244
15. James RC, Mustard CA. Geographic location of commercial plasma donation clinics in the United States, 1980–1995. Am J Public Health. 2004;94(7):1224–1229. doi:10.2105/AJPH.94.7.1224
16. Tobler LH, Busch MP. History of posttransfusion hepatitis. Clin Chem. 1997;43(8 Pt 2):1487–1493. doi:10.1093/clinchem/43.8.1487
17. Klamroth R, Gröner A, Simon TL. Pathogen inactivation and removal methods for plasma-derived clotting factor concentrates: plasma Concentrate Pathogen Safety. Transfusion. 2014;54(5):1406–1417. doi:10.1111/trf.12423
18. Teitel JM. Viral safety of haemophilia treatment products. Ann Med. 2000;32(7):485–492. doi:10.3109/07853890009002024
19. Swiech K, Picanço-Castro V, Covas DT. Production of recombinant coagulation factors: are humans the best host cells? Bioengineered. 2017;8(5):462–470. doi:10.1080/21655979.2017.1279767
20. Nogami K, Shima M. New therapies using nonfactor products for patients with hemophilia and inhibitors. Blood. 2019;133(5):399–406. doi:10.1182/blood-2018-07-820712
21. Isfordink CJ, Erpecum KJ, Valk M, Mauser‐Bunschoten EP, Makris M. Viral hepatitis in haemophilia: historical perspective and current management. Br J Haematol. 2021;195(2):174–185. doi:10.1111/bjh.17438
22. Ghosh K, Ghosh K. Management of haemophilia in developing countries: challenges and options. Indian J Hematol Blood Transfus. 2016;32(3):347–355. doi:10.1007/s12288-015-0562-x
23. Zhang M, Rosenberg PS, Brown DL, et al. Correlates of spontaneous clearance of hepatitis C virus among people with hemophilia. Blood. 2006;107(3):892–897. doi:10.1182/blood-2005-07-2781
24. Fransen van de Putte DE, Makris M, Fischer K, et al. Long-term follow-up of hepatitis C infection in a large cohort of patients with inherited bleeding disorders. J Hepatol. 2014;60(1):39–45. doi:10.1016/j.jhep.2013.08.010
25. Goedert JJ, Eyster ME, Lederman MM, et al. End-stage liver disease in persons with hemophilia and transfusion-associated infections. Blood. 2002;100(5):1584–1589.
26. Posthouwer D, Makris M, Yee TT, et al. Progression to end-stage liver disease in patients with inherited bleeding disorders and hepatitis C: an international, multicenter cohort study. Blood. 2007;109(9):3667–3671. doi:10.1182/blood-2006-08-038349
27. Bruno S, Silini E, Crosignani A, et al. Hepatitis C virus genotypes and risk of hepatocellular carcinoma in cirrhosis: a prospective study. Hepatology. 1997;25(3):754–758. doi:10.1002/hep.510250344
28. Franchini M, Rossetti G, Tagliaferri A, et al. The natural history of chronic hepatitis C in a cohort of HIV-negative Italian patients with hereditary bleeding disorders. Blood. 2001;98(6):1836–1841. doi:10.1182/blood.v98.6.1836
29. Prati D, Capelli C, Zanella A, et al. Influence of different hepatitis C virus genotypes on the course of asymptomatic hepatitis C virus infection. Gastroenterology. 1996;110(1):178–183. doi:10.1053/gast.1996.v110.pm8536854
30. Minola E, Prati D, Suter F, et al. Age at infection affects the long-term outcome of transfusion-associated chronic hepatitis C. Blood. 2002;99(12):4588–4591. doi:10.1182/blood-2001-12-0192
31. Ioannou GN, Bryson CL, Weiss NS, Miller R, Scott JD, Boyko EJ. The prevalence of cirrhosis and hepatocellular carcinoma in patients with human immunodeficiency virus infection. Hepatology. 2013;57(1):249–257. doi:10.1002/hep.25800
32. Tagliaferri A, Rivolta GF, Iorio A, et al. Mortality and causes of death in Italian persons with haemophilia, 1990–2007. Haemophilia. 2010;16(3):437–446. doi:10.1111/j.1365-2516.2009.02188.x
33. Orman ES, Fried MW. Hepatitis C viral infection in patients with hemophilia and hemolytic disorders. Clin Liver Dis. 2012;1(3):95–97. doi:10.1002/cld.42
34. Maor Y, Schapiro JM, Bashari D, Martinowitz U. Survival of hepatitis C-infected haemophilia patients is predicted by presence of cirrhosis but not by anti-viral treatment. Ann Hepatol. 2014;13(6):753–761. doi:10.1016/S1665-2681(19
35. The Data Collection on Adverse Events of Anti-HIV Drugs Study Group. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D Study. Arch Intern Med. 2006;166(15):1632–1641. doi:10.1001/archinte.166.15.1632
36. Eyster ME, Fried MW, Di Bisceglie AM, Goedert JJ. Increasing hepatitis C virus RNA levels in hemophiliacs: relationship to human immunodeficiency virus infection and liver disease. Multicenter Hemophilia Cohort Study. Blood. 1994;84(4):1020–1023. doi:10.1182/blood.V84.4.1020.1020
37. Massard J, Ratziu V, Thabut D, et al. Natural history and predictors of disease severity in chronic hepatitis C. J Hepatol. 2006;44:S19–S24. doi:10.1016/j.jhep.2005.11.009
38. Westin J, Nordlinder H, Lagging M, Norkrans G, Wejstål R. Steatosis accelerates fibrosis development over time in hepatitis C virus genotype 3 infected patients. J Hepatol. 2002;37(6):837–842. doi:10.1016/S0168-8278(02)00299-4
39. Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings LW. Aging of hepatitis C virus (HCV)-infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression. Gastroenterology. 2010;138(2):
40. Tradati F, Colombo M, Mannucci PM, et al. A prospective multicenter study of hepatocellular carcinoma in Italian hemophiliacs with chronic hepatitis C. The study group of the association of Italian hemophilia centers. Blood. 1998;91(4):1173–1177.
41. Santagostino E, Colombo M, Rivi M, et al. A 6-month versus a 12-month surveillance for hepatocellular carcinoma in 559 hemophiliacs infected with the hepatitis C virus. Blood. 2003;102(1):78–82. doi:10.1182/blood-2002-10-3310
42. Thalappillil A, Ragni MV, Comer DM, Yabes JG. Incidence and risk factors for hepatocellular cancer in individuals with haemophilia: a national inpatient sample study. Haemophilia. 2019;25(2):221–228. doi:10.1111/hae.13668
43. Hassan S, Monahan RC, Mauser-Bunschoten EP, et al. Mortality, life expectancy, and causes of death of persons with hemophilia in the Netherlands 2001–2018. J Thromb Haemost. 2021;19(3):645–653. doi:10.1111/jth.15182
44. Posthouwer D, Mauser-Bunschoten EP, Fischer K, Makris M. Treatment of chronic hepatitis C in patients with haemophilia: a review of the literature. Haemophilia. 2006;12(5):473–478. doi:10.1111/j.1365-2516.2006.01317.x
45. Carrat F, Bani-Sadr F, Pol S, et al. Pegylated interferon alfa-2b vs standard interferon alfa-2b, plus ribavirin, for chronic hepatitis C in HIV-infected patients: a randomized controlled trial. JAMA. 2004;292(23):2839–2848. doi:10.1001/jama.292.23.2839
46. Torriani FJ, Rodriguez-Torres M, Rockstroh JK, et al. Peginterferon Alfa-2a plus ribavirin for chronic hepatitis C virus infection in HIV-infected patients. N Engl J Med. 2004;351(5):438–450. doi:10.1056/NEJMoa040842
47. Franchini M, Mengoli C, Veneri D, Mazzi R, Lippi G, Cruciani M. Treatment of chronic hepatitis C in haemophilic patients with interferon and ribavirin: a meta-analysis. J Antimicrob Chemother. 2008;61(6):1191–1200. doi:10.1093/jac/dkn119
48. Manns MP, Wedemeyer H, Cornberg M. Treating viral hepatitis C: efficacy, side effects, and complications. Gut. 2006;55(9):1350–1359. doi:10.1136/gut.2005.076646
49. Posthouwer D, Plug I, van der Bom JG, Fischer K, Rosendaal FR, Mauser-Bunschoten EP. Hepatitis C infection among Dutch haemophilia patients: a nationwide cross-sectional study of prevalence and antiviral treatment. Haemophilia. 2005;11(3):270–275. doi:10.1111/j.1365-2516.2005.01083.x
50. Xia H, Lu C, Wang Y, et al. Efficacy and safety of direct-acting antiviral therapy in patients with chronic hepatitis C virus infection: a real-world single-center experience in Tianjin, China. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.00710
51. Manns MP, Maasoumy B. Breakthroughs in hepatitis C research: from discovery to cure. Nat Rev Gastroenterol Hepatol. 2022;1–18. doi:10.1038/s41575-022-00608-8
52. Santagostino E, Pol S, Olveira A, et al. Daclatasvir/peginterferon lambda-1a/ribavirin in patients with chronic HCV infection and haemophilia who are treatment naïve or prior relapsers to peginterferon alfa-2a/ribavirin. Haemophilia. 2016;22(5):692–699. doi:10.1111/hae.12947
53. Younossi ZM, Stepanova M, Marcellin P, et al. Treatment with ledipasvir and sofosbuvir improves patient-reported outcomes: results from the ION-1, −2, and −3 clinical trials. Hepatology. 2015;61(6):1798–1808. doi:10.1002/hep.27724
54. Kish T, Aziz A, Sorio M. Hepatitis C in a new era: a review of current therapies. P T. 2017;42(5):316–329.
55. Papadopoulos N, Argiana V, Deutsch M. Hepatitis C infection in patients with hereditary bleeding disorders: epidemiology, natural history, and management. Ann Gastroenterol. 2018;31(1):35–41. doi:10.20524/aog.2017.0204
56. Stedman CAM, Hyland RH, Ding X, Pang PS, McHutchison JG, Gane EJ. Once daily ledipasvir/sofosbuvir fixed-dose combination with ribavirin in patients with inherited bleeding disorders and hepatitis C genotype 1 infection. Haemophilia. 2016;22(2):214–217. doi:10.1111/hae.12791
57. Walsh CE, Workowski K, Terrault NA, et al. Ledipasvir-sofosbuvir and sofosbuvir plus ribavirin in patients with chronic hepatitis C and bleeding disorders. Haemophilia. 2017;23(2):198–206. doi:10.1111/hae.13178
58. Hézode C, Colombo M, Bourlière M, et al. Elbasvir/grazoprevir for patients with hepatitis C virus infection and inherited blood disorders: a phase III Study. Hepatology. 2017;66(3):736–745. doi:10.1002/hep.29139
59. Lee HW, Yoo KY, Won JW, Kim HJ. Direct acting antiviral agents in Korean patients with chronic hepatitis C and hemophilia who are treatment-naïve or treatment-experienced. Gut Liver. 2017;11(5):721–727. doi:10.5009/gnl17209
60. Uemura H, Tsukada K, Mizushima D, et al. Interferon-free therapy with direct acting antivirals for HCV/HIV-1 co-infected Japanese patients with inherited bleeding disorders. PLoS One. 2017;12(10):e0186255. doi:10.1371/journal.pone.0186255
61. Xiao H, Chen J, Wang J, Li J, Yang F, Lu H. Antiviral therapy for HCV in hemophilia A patients with HIV-1 co-infection. Medicine. 2019;98(30):e16524. doi:10.1097/MD.0000000000016524
62. Mancuso ME, Linari S, Santagostino E, et al. High rate of sustained virological response with direct-acting antivirals in haemophiliacs with HCV infection: a multicenter study. Liver Int. 2020;40(5):1062–1068. doi:10.1111/liv.14337
63. Ackens R, Posthouwer D. Treatment of chronic hepatitis C with direct acting antiviral agents in patients with haemophilia, end-stage liver disease and coinfected with HIV. Haemophilia. 2016;22(3):e223–e225. doi:10.1111/hae.12899
64. Wiegand J, Schiefke I, Stein K, Berg T, Kullig U, Ende K. Interferon-free treatment of chronic hepatitis C virus infection in patients with inherited bleeding disorders. Hamostaseologie. 2017;37(2):127–130. doi:10.5482/HAMO-16-05-0014
65. Mehta R, Kabrawala M, Nandwani S, et al. Daclatasvir-Sofosbuvir for treatment of hepatitis C virus in patients with inherited bleeding disorders. Indian J Gastroenterol. 2017;36(4):332–333. doi:10.1007/s12664-017-0777-x
66. Nagao A, Hanabusa H. Brief report: the impact of ledipasvir/sofosbuvir on HIV-positive and HIV-negative Japanese hemophilia patients with 1, 4, and Mixed-Genotype HCV. J Acquir Immune Defic Syndr. 2017;74(4):418–422. doi:10.1097/QAI.0000000000001271
67. Giouleme O, Paschos P, Katsoula A, Panteliadou K, Vakalopoulou S, Garipidou V. Hepatitis C infection in a Greek population with inherited bleeding disorders. Haemophilia. 2018;24(2):e74–e76. doi:10.1111/hae.13427
68. Maticic M, Lekše A, Kozinc M, et al. Micro-elimination of hepatitis C among patients with congenital bleeding disorders in Slovenia. J Hepatol. 2018;68:S193–S194. doi:10.1016/S0168-8278(18
69. Fransen L, D’hondt P, Bielen R, et al. Elimination of hepatitis C virus infection in patients with haemophilia in Belgium: a single‐centre experience. Haemophilia. 2019;25(6):1028–1034. doi:10.1111/hae.13829
70. Sharafi H, Behnava B, Azizi-saraji A, et al. Treatment of hepatitis C virus infection with direct-acting antiviral agent-based regimens in Iranian patients with hereditary bleeding disorders. Virol J. 2021;18(1):199. doi:10.1186/s12985-021-01659-0
71. Ružić M, Rajić N, Fabri M, et al. Implementation of microelimination strategy in eradication of chronic hepatitis C infection in patients with hemophilia in the Northern region of Serbia: is eradication possible? Mediterr J Hematol Infect Dis. 2021;13(1):e2021058. doi:10.4084/MJHID.2021.058
72. Inukai Y, Imai N, Yamamoto K, et al. The influence of hepatitis C virus eradication on hepatocarcinogenesis in patients with hemophilia. Ann Hepatol. 2022;27(1):100545. doi:10.1016/j.aohep.2021.100545
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.