")
Back to Journals » International Journal of Women's Health » Volume 7
Hemostatic assessment, treatment strategies, and hematology consultation in massive postpartum hemorrhage: results of a quantitative survey of obstetrician-gynecologists
Authors James A, Cooper DL , Paidas MJ
Received 29 May 2015
Accepted for publication 19 August 2015
Published 4 November 2015 Volume 2015:7 Pages 873—881
DOI https://doi.org/10.2147/IJWH.S89573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Andra H James,1 David L Cooper,2 Michael J Paidas3
1Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, Duke University, Durham, NC, 2Novo Nordisk Inc., Princeton, NJ, 3Department of Obstetrics, Gynecology, and Reproductive Sciences, Yale Women and Children’s Center for Blood Disorders and Preeclampsia Advancement, Yale University, New Haven, CT, USA
Objective: To assess potential diagnostic and practice barriers to successful management of massive postpartum hemorrhage (PPH), emphasizing recognition and management of contributing coagulation disorders.
Study design: A quantitative survey was conducted to assess practice patterns of US obstetrician-gynecologists in managing massive PPH, including assessment of coagulation.
Results: Nearly all (98%) of the 50 obstetrician-gynecologists participating in the survey reported having encountered at least one patient with “massive” PPH in the past 5 years. Approximately half (52%) reported having previously discovered an underlying bleeding disorder in a patient with PPH, with disseminated intravascular coagulation (88%, n=23/26) being identified more often than von Willebrand disease (73%, n=19/26). All reported having used methylergonovine and packed red blood cells in managing massive PPH, while 90% reported performing a hysterectomy. A drop in blood pressure and ongoing visible bleeding were the most commonly accepted indications for rechecking a “stat” complete blood count and coagulation studies, respectively, in patients with PPH; however, 4% of respondents reported that they would not routinely order coagulation studies. Forty-two percent reported having never consulted a hematologist for massive PPH.
Conclusion: The survey findings highlight potential areas for improved practice in managing massive PPH, including earlier and more consistent assessment, monitoring of coagulation studies, and consultation with a hematologist.
Keywords: acquired hemophilia, blood coagulation disorders, disseminated intravascular coagulation, von Willebrand disease
Introduction
Deaths from postpartum hemorrhage (PPH) occur as a result of a suboptimal clinical response to massive hemorrhage, whether due to limited or absent resources in developing countries or to poor coordination of resuscitative efforts in developed countries,1 and usually occur in the setting of coagulopathy. The most common causes of massive PPH are obstetric bleeding (uterine atony, retained placenta) or surgical bleeding (lacerations and incisions);2–7 but with massive PPH from any of these causes, women may develop a dilutional coagulopathy due to resuscitation with crystalloids or acute consumptive coagulopathy and disseminated intravascular coagulation (DIC).
Alternatively or additionally, a preexisting coagulation disorder, either acquired or congenital, may underlie immediate or delayed postpartum bleeding.5 Acquired coagulation disorders that may occur during or after pregnancy and contribute to PPH include quantitative platelet disorders8 such as HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome or immune thrombocytopenic purpura; acute liver failure of pregnancy resulting in reduced liver synthetic function;5 and acquired hemophilia.9 Acquired hemophilia is a rare (incidence, 1–1.5 per million)10 acquired coagulopathy characterized by alloantibodies against coagulation factors, most often factor VIII, that is associated with pregnancy in 2%–29% of cases9–14 and occurs in otherwise healthy women without a personal or family history of bleeding. Acquired hemophilia is notable for its potential to cause delayed postpartum bleeding in the mother (up to 117 days after delivery)9 and the baby, via transplacental transfer of maternal alloantibodies.9,15–17 Congenital coagulation disorders that may contribute to PPH include von Willebrand disease (VWD), hemophilia carriage, and factor XI deficiency; rare bleeding disorders such as factor II (prothrombin) and VII deficiencies and fibrinogen disorders; and the severe platelet function disorders Glanzmann’s thrombasthenia and Bernard–Soulier syndrome. All have higher than expected rates of PPH.18 Of these inherited bleeding disorders, VWD is the most common resulting from a quantitative or qualitative defect in von Willebrand factor (VWF). The rise in VWF and factor VIII levels during pregnancy may protect against immediate PPH in type I VWD (quantitative defect), but in general, the risk for PPH is increased threefold for women with VWD.19 Whereas it is relatively uncommon that a preexisting congenital or acquired coagulopathic condition is the primary or sole cause of PPH,8 failure to recognize the presence of such a condition at the time of delivery or in the postpartum period may impair attempts to control bleeding.
With the exception of limited summary data from administrative databases, clinical guidelines, and the results of another recently published survey,20 there are few data about how obstetrician-gynecologists manage massive PPH, especially with regard to hemostatic assessment and engagement of hematologic specialists. In the other recently published PPH management survey, fewer than half of patients with PPH managed by obstetrician-gynecologists ever had a hematologic evaluation.20 The purpose of this study was to assess potential diagnostic and practice barriers to successful management of massive PPH resulting from the most common to the rarest causes, including experience with PPH associated with bleeding disorders.
Materials and methods
Study design
This was a quantitative survey of the practice patterns of a cohort of obstetrician-gynecologists with respect to the management of massive PPH and recognition of bleeding disorders, undertaken as a part of a more comprehensive case-based survey of multiple specialties.21 The survey aimed to assess respondents’ practices with regard to treatment strategies, hemostatic assessment and monitoring, and hematology consultation in the setting of PPH, as well as participants’ prior clinical experience with bleeding disorders. Since the practice patterns of obstetrician-gynecologists are unique, the survey questions were specifically addressed to those practice patterns (distinct from the case study used for other specialists), and the responses from the cohort of obstetrician-gynecologists were not compared to the responses of other specialties.
Setting
All surveys were completed over a 2-week period from January 14, 2010 to January 28, 2010. The time frame was dictated by the budget and the needs of the larger study, in addition to meeting the goal of 50 completed surveys for each specialty group.
Participants
This study was exempt from Institutional Review Board approval since the survey procedures did not elicit private, protected information or biological specimens, and responses were recorded in a way that did not link back to the physicians who completed the survey. Any disclosure of the responses outside of the research could not reasonably place the physician subjects at risk of criminal or civil liability or be damaging to their financial standing (which could include loss of insurability or employability) or reputation. The obstetrician-gynecologists surveyed were a subset of a larger group of physicians specializing in hematology, hematology/oncology, emergency medicine, geriatrics, internal medicine, rheumatology, critical care medicine, and general surgery who were randomly sampled from the American Medical Association Physician Masterfile. From this sample, physicians who were already part of the Harris Interactive Online Physician Panel were invited to participate in the survey by email. Physicians who were not part of the panel were invited to participate via first-class mail. The invitation included a URL address and password to log on to the survey site, where invitees first encountered a series of questions to determine eligibility for participation in the survey.21 Eligible obstetrician-gynecologists were required to have an active obstetrics practice. Upon confirmation of eligibility, participants completed the approximately 10-minute-long online survey.
Survey instrument
For obstetrician-gynecologists, the survey questionnaire centered on PPH and included questions about definitions and management of PPH; thresholds for obtaining coagulation laboratory studies; the frequency of and rationale for hematology consultation; and prior clinical experience with bleeding disorders. The rest of the physicians completed different surveys about different bleeding issues: one for all of the physicians in medical specialties21 and another for the general surgeons.22
Analysis
The survey was designed to assess potential diagnostic and practice barriers. To ensure sufficient feedback to generate reasonable hypotheses about obstetrician-gynecologists’ stated practice patterns for subsequent testing in face-to-face interviews, a sufficient number of obstetrician-gynecologists was recruited to accrue 50 complete responses. To ensure that the findings were representative of all of the obstetrician-gynecologists surveyed, data were weighted for sex, years in practice, and region.
Results
A total of 50 obstetrician-gynecologists, the first 50 who responded, participated in the survey. The mean age of respondents was 51.0 years and they had an average (median) of 19.4 (21) years in practice. The majority (60%) reported between 100 and 200 deliveries per year. Detailed demographic and professional information about the participants is shown in Table 1.
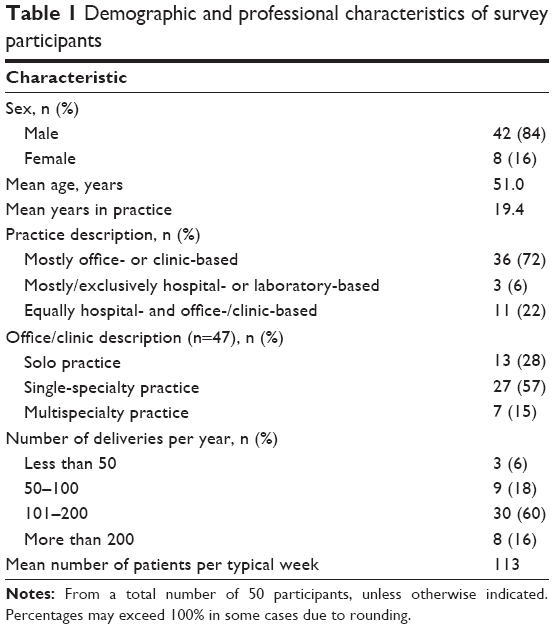 | Table 1 Demographic and professional characteristics of survey participants |
All obstetrician-gynecologists surveyed reported having encountered at least one patient with PPH in the past 5 years, and nearly all (98%) reported having specifically encountered a patient with what they defined as “massive” or “severe” PPH in that time frame. The majority (64%) of the respondents defined massive hemorrhage as more than 2,000 mL blood loss; approximately one-quarter (26%) as more than 1,500 mL blood loss; 6% as more than 1,000 mL blood loss; and another 4% as “other”. Potential strategies for managing PPH are summarized in Figure 1. With respect to uterotonics, all (100%) of the obstetrician-gynecologists surveyed reported having used methylergonovine, 82% misoprostol, and 52% carboprost tromethamine (Figure 1A). With respect to surgical management, 90% reported having used hysterectomy, 62% B-Lynch or similar compression sutures, and 54% arterial embolization (Figure 1B). All (100%) reported having used packed red blood cells (PRBCs), 88% fresh frozen plasma (FFP), 74% cryoprecipitate, and 26% recombinant clotting factor in the management of PPH (Figure 1C).
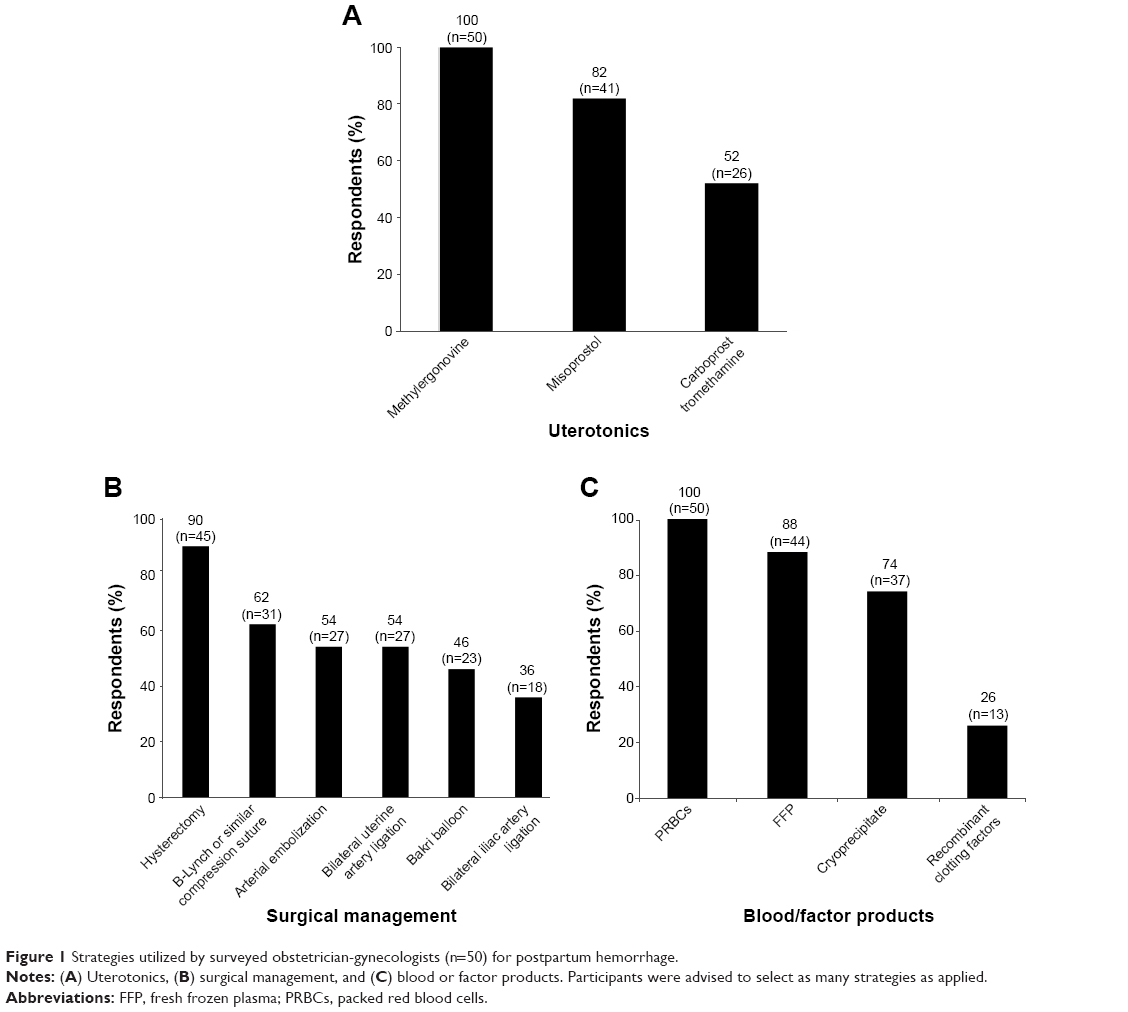 | Figure 1 Strategies utilized by surveyed obstetrician-gynecologists (n=50) for postpartum hemorrhage. |
Common thresholds for rechecking a “stat” complete blood count (CBC) in a patient with PPH included a drop in blood pressure (82%), ongoing visible bleeding (76%), and tachycardia (68%; Table 2). Nearly half of respondents reported that blood losses of 1,000 mL (48%) or 1,500 mL (40%) would prompt immediate rechecking of the CBC; only 32% would have rechecked a CBC after 2,000 mL blood loss (Table 2). The most common threshold for checking coagulation studies (defined in the question as prothrombin time, activated partial thromboplastin time [aPTT], and international normalized ratio) was ongoing visible bleeding (84%; Table 3). Only 4% of respondents reported that they would not routinely order coagulation studies.
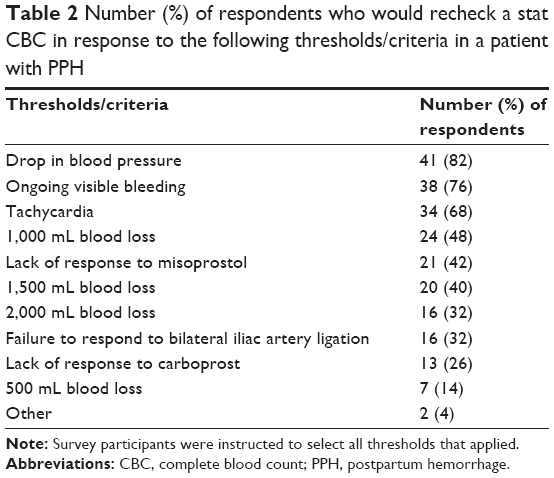 | Table 2 Number (%) of respondents who would recheck a stat CBC in response to the following thresholds/criteria in a patient with PPH |
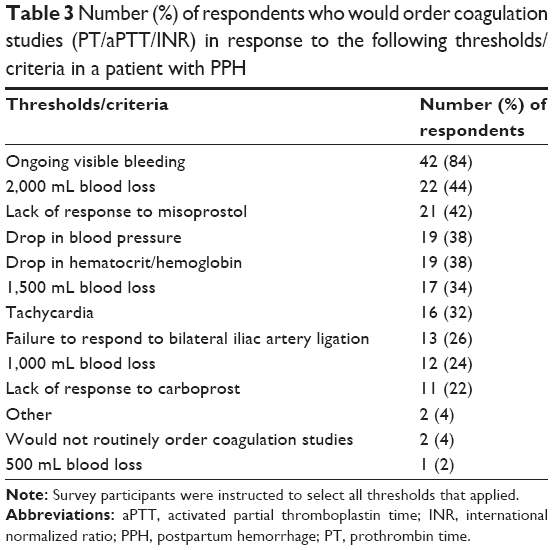 | Table 3 Number (%) of respondents who would order coagulation studies (PT/aPTT/INR) in response to the following thresholds/criteria in a patient with PPH |
The vast majority (92%) of obstetrician-gynecologists reported that the centers or hospitals with which they were affiliated performed most coagulation laboratory studies on site. A majority (62%) of respondents reported that they did not send coagulation laboratory studies out for analysis, while 24% reported sending at least some coagulation studies out to a central laboratory and 14% out to a regional center or academic hospital.
Forty-two percent of obstetrician-gynecologists surveyed reported never having consulted a hematologist for PPH (Figure 2A). A slightly smaller percentage (34%) reported having consulted a hematologist one or two times for this purpose. Of several potential options, the most common reasons for considering consultation with a hematologist (n=29) included abnormal coagulation studies that were not normalizing with administration of FFP or cryoprecipitate (86%, n=25/29), worsening abnormal coagulation studies (86%, n=25/29), and suspicion of DIC (72%, n=21/29; Figure 2B). More than half (52%) of obstetrician-gynecologists reported having previously discovered an underlying bleeding disorder in a patient with PPH. DIC (88%, n=23/26), VWD (73%, n=19/26), and platelet disorders (58%, n=15/26) were the most commonly reported diagnoses, followed by lupus anticoagulant (misinterpreted as a bleeding disorder by the respondents, but not actually a bleeding disorder, 23%, n=6/26) and “other” bleeding disorders (15%, n=4/26). Only one of the obstetrician-gynecologists surveyed reported having ever encountered a patient with acquired hemophilia.
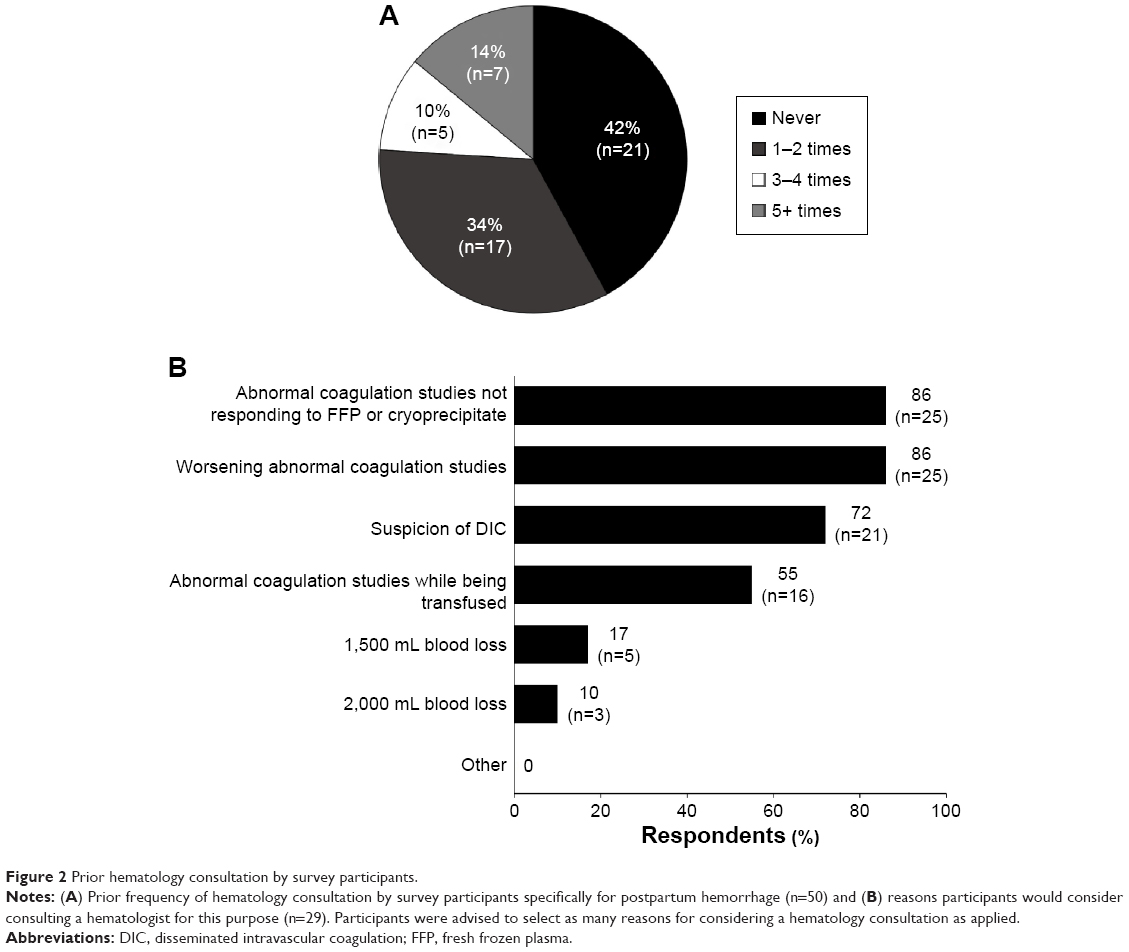 | Figure 2 Prior hematology consultation by survey participants. |
Discussion
We found that all survey participants reported having had experience with the management of PPH within the prior 5 years and that nearly all reported having had experience, specifically, with what they defined as massive PPH. This is not surprising, since the majority of participants attended between 100 and 200 deliveries per year and the published incidence of massive obstetric hemorrhage ranges from 0.15% to 2.7% of pregnancies.5 Whereas most participants identified massive PPH as correlating with a blood-loss volume of 2,000 mL or more, the variability among survey respondents in defining this condition is reflected in the literature, in which massive PPH has been variably defined based on such factors as blood-loss volume, the need for transfusion of blood products (most often PRBCs), presence of coagulopathy, or some combination thereof.5 Recently, a multidisciplinary panel of internationally recognized experts on PPH emphasized the ongoing nature of bleeding in their definition of PPH, defining severe persistent (ongoing) PPH as “active bleeding >1,000 mL within the 24 hours following birth that continues despite the use of initial measures including first-line uterotonic agents and uterine massage.”23
Hematologic laboratory assessment in PPH
The most common reasons obstetrician-gynecologists in this survey would have repeated a stat CBC included ongoing visible bleeding and changes in vital signs suggesting evolving hemodynamic instability. Fewer than half would have repeated a CBC for thresholds based on blood volume lost or insufficient response to either uterotonics or bilateral iliac artery ligation. The value of hematocrit measurement in an acutely bleeding patient may be limited, as drops in hematocrit may not immediately correlate with the magnitude of blood loss;24 however, inconsistent assessment and follow-up of hemoglobin concentration were noted in a retrospective analysis of 38 maternal deaths due to PPH in France and were identified as potential areas for improvement in the critical-care management of women with PPH.2
Fewer than half of obstetrician-gynecologists in the survey would have relied on specific blood loss volumes as a threshold for obtaining hematologic laboratory studies. Given that visual estimates of blood loss are often inaccurately low,24–26 intensified surveillance and more aggressive management should, perhaps, occur at lower than usual blood-volume thresholds when relying on visual estimates.24 Underestimation of blood loss appears to be greatest (by up to 50%) when volumes exceed 1,000 mL.24,26 A recently evaluated visual aid depicting known volumes of blood on obstetric materials may improve the accuracy of blood-loss estimation by obstetric providers with varying years of experience.26 It has been suggested that blood loss exceeding 1,000 mL should prompt mobilization of additional resources for managing PPH.27 Ongoing heavy bleeding with an estimated blood loss of 1,500 mL or more should prompt initiation of the local massive blood-loss protocol.6,28 Such protocols have been the standard of care in the United Kingdom for years, but were not universally implemented at the time of this survey and are only now being widely adopted in the United States. In contrast, hemodynamic parameters may underestimate the extent of blood loss in women with PPH, who may tolerate blood loss better because of normal intrapartum physiological changes.29,30
The majority (84%) of obstetrician-gynecologists in this survey would have ordered coagulation studies for ongoing visible bleeding. Fewer than half of respondents chose any other scenario (blood volume lost, hemodynamic parameters, hemoglobin measurements, or failed response to initial treatments) as a threshold for ordering coagulation studies. Nearly 4% (n=2/50) of obstetrician-gynecologists in this survey would not have ordered coagulation studies, despite the majority of all respondents reporting that coagulation studies were performed on-site at their institution. The explanation for this finding may be the obstetrician-gynecologists’ reliance on anesthesiologists and, in cases of intensive care unit transfer, intensivists to assess and manage any coagulopathy associated with PPH.
Assessment for coagulopathy in PPH is important not only to exclude preexisting bleeding diatheses but also, and more often, to identify an acquired coagulopathy resulting from massive hemorrhage.5 The reported incidence of massive PPH accompanied by coagulopathy ranges from 0.15% to 0.5%.5 Despite the potential contribution of hemostatic disorders to PPH, in the aforementioned French study of maternal deaths due to PPH, coagulation tests were performed in only 20 of the 38 women, despite on-site clinical laboratory support in 30 (76%) cases.2 Global tests of hemostasis such as thromboelastometry or thromboelastography can provide potentially valuable information in real time at the patient’s bedside.31 Thromboelastography has been reported to have decreased the use of FFP and platelets in the setting of massive transfusion,32 but it has not been adequately studied in obstetric hemorrhage and may have limited predictive value, according to recent guidelines from the European Society of Anesthesiology.33
Prior experience with bleeding conditions
It was surprising that DIC was the most common bleeding diathesis previously encountered by obstetrician-gynecologists. The explanation for this finding may be that most VWD is mild type I, which does not usually pose a significant bleeding challenge at the time of delivery. More than half of respondents reported having encountered platelet disorders in women with PPH. Platelet disorders that may present during pregnancy encompass a broad range of acquired and inherited quantitative and qualitative platelet defects. However, not all are clinically significant, many (especially severe qualitative platelet disorders) are rare, and some inherited disorders may be diagnosed before an affected woman becomes pregnant.8 Approximately one in five (23%, n=6/26) of respondents identified lupus anticoagulant as a bleeding disorder that they previously encountered in the setting of PPH, yet lupus anticoagulant is typically associated with thrombosis rather than bleeding.34 However, lupus anticoagulant may confound the diagnosis of coagulation factor inhibitors if an abnormal coagulation study (typically an isolated prolonged aPTT) or reduced factor levels are attributed to lupus anticoagulant, whether erroneously35 or in the presence of a coexisting lupus anticoagulant and coagulation factor inhibitor.36–39 Whereas the small percentage of obstetrician-gynecologists who had ever encountered acquired hemophilia may be expected in light of the rarity of the condition (even in postpartum women), this finding nevertheless highlights the fact that, like most non-hematologists, most obstetrician-gynecologists lack experience with the condition and thus may not recognize the signs and symptoms of acquired hemophilia or consider the diagnosis in affected patients. At one of the authors’ institutions (AHJ), a patient recently presented 2 months postpartum with delayed PPH due to acquired hemophilia, which was recognized based upon abnormal aPTT. She was subsequently managed jointly by obstetrics and hematology.
Hematology consultation for PPH
In this survey, 34% of obstetrician-gynecologists reported having consulted a hematologist for PPH only once or twice in their career; 42% of these respondents had never consulted a hematologist for this purpose. Yet, nearly all respondents had occasion to manage what they defined as massive PPH in the previous 5 years. It is possible that this finding relates again to reliance on anesthesiologists and, in cases of intensive care unit transfer, intensivists to assess and manage any coagulopathy associated with PPH. Nevertheless, this finding may reveal an opportunity to involve a hematologist sooner (ie, before having to intervene surgically or transfer the patient to a higher level of care) to optimize diagnostic evaluation and management, particularly with regard to the use of blood products and other resources. Furthermore, prompt and accurate identification of any acquired or undiagnosed congenital bleeding disorder underlying PPH is critical.
Study strengths and limitations
The sample of obstetrician-gynecologists captured in this survey consisted of a cross-section of practicing, contemporary physicians. It is true that the participants elected to participate and those with an interest may have been more likely to respond to the invitation. The number of cases of DIC and other bleeding disorders managed is rather high, but the answers appear to have covered many years of practice; therefore, their responses may not be completely representative of all obstetrician-gynecologists. While the sample size was quite small, it was sufficiently large to generate reasonable hypotheses for subsequent qualitative analyses intended to explore the rationale behind participants’ responses, something that this quantitative survey could not capture. These data are consistent with findings of the parallel case-based survey including 402 physicians (~50 each) specialized in hematology, hematology/oncology, emergency medicine, geriatrics, internal medicine, rheumatology, and critical care medicine where there were also delays in interpretation of significantly abnormal coagulation assay results and a reluctance by non-hematologists to consult hematology, particularly by emergency medicine and critical care health care professionals.21
Conclusion
Early identification of coagulopathy – whether a preexisting coagulopathy or a “transient” dilutional or consumptive coagulopathy resulting from massive hemorrhage and subsequent resuscitation – may be essential to controlling bleeding and minimizing morbidity and mortality in massive PPH. Given reports of increased morbidity and mortality among insufficiently resuscitated women with PPH, early assessment of coagulation status in PPH, especially massive PPH, is justified and prudent. Early intervention and treatment of coagulopathy may be fertility-preserving and lifesaving. The results of this survey highlight potential areas for improved practice in the management of PPH, including development and implementation of algorithms or hospital protocols to assure earlier and more consistent assessment and monitoring of hematologic (including coagulation) laboratory indices and consultation with a hematologist, particularly in cases in which an acquired or previously undiagnosed inherited bleeding disorder may be a contributing cause.
Acknowledgments
The quantitative and qualitative research surveys described in this manuscript were completed by Harris Interactive, New York, NY, USA, under funding provided by Novo Nordisk Inc., Princeton, NJ, USA. Editorial assistance was provided by Lara Primak, MD, of ETHOS Health Communications in Newtown, PA, USA, with financial support from Novo Nordisk Inc., in compliance with international guidelines for Good Publication Practice.
Disclosure
Michael J Paidas has received research funding from Novo Nordisk. David L Cooper is an employee of Novo Nordisk Inc. Andra H James reports no conflicts of interest in this work.
References
Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066–1074. | ||
Bonnet MP, Deneux-Tharaux C, Bouvier-Colle MH. Critical care and transfusion management in maternal deaths from postpartum haemorrhage. Eur J Obstet Gynecol Reprod Biol. 2011;158(2):183–188. | ||
Borna S, Hantoushzadeh S. Acquired hemophilia as a cause of primary postpartum hemorrhage. Arch Iran Med. 2007;10(1):107–110. | ||
Brace V, Kernaghan D, Penney G. Learning from adverse clinical outcomes: major obstetric haemorrhage in Scotland, 2003–2005. BJOG. 2007;114(11):1388–1396. | ||
James AH, McLintock C, Lockhart E. Postpartum hemorrhage: when uterotonics and sutures fail. Am J Hematol. 2012;87 Suppl 1:S16–S22. | ||
Sheikh L, Najmi N, Khalid U, Saleem T. Evaluation of compliance and outcomes of a management protocol for massive postpartum hemorrhage at a tertiary care hospital in Pakistan. BMC Pregnancy Childbirth. 2011;11:28. | ||
Wise A, Clark V. Strategies to manage major obstetric haemorrhage. Curr Opin Anaesthesiol. 2008;21(3):281–287. | ||
Silver RM, Major H. Maternal coagulation disorders and postpartum hemorrhage. Clin Obstet Gynecol. 2010;53(1):252–264. | ||
Tengborn L, Baudo F, Huth-Kühne A, et al. Pregnancy-associated acquired haemophilia A: results from the European Acquired Haemophilia (EACH2) registry. BJOG. 2012;119(12):1529–1537. | ||
Collins PW, Hirsch S, Baglin TP, et al. Acquired hemophilia A in the United Kingdom: a 2-year national surveillance study by the United Kingdom Haemophilia Centre Doctors’ Oganisation. Blood. 2007;109(5):1870–1877. | ||
Kessler CM, Ludlam CA. The treatment of acquired factor VIII inhibitors: worldwide experience with porcine factor VIII concentrate. International Acquired Hemophilia Study Group. Semin Hematol. 1993;30(2 Suppl 1):22–27. | ||
Lak M, Sharifian RA, Karimi K, Mansouritorghabeh H. Acquired hemophilia A: clinical features, surgery and treatment of 34 cases, and experience of using recombinant factor VIIa. Clin Appl Thromb Hemost. 2010;16(3):294–300. | ||
Morrison AE, Ludlam CA, Kessler C. Use of porcine factor VIII in the treatment of patients with acquired hemophilia. Blood. 1993;81(6):1513–1520. | ||
Paidas MJ, Hossain N. Unexpected postpartum hemorrhage due to an acquired factor VIII inhibitor. Am J Perinatol. 2014;31(8):645–654. | ||
Kotani Y, Shiota M, Umemoto M, Koike E, Tsuritani M, Hoshiai H. Case of acquired hemophilia with factor VIII inhibitor in a mother and newborn. J Obstet Gynaecol Res. 2011;37(8):1102–1105. | ||
Lulla RR, Allen GA, Zakarija A, Green D. Transplacental transfer of postpartum inhibitors to factor VIII. Haemophilia. 2010;16(1):14–17. | ||
Ries M, Wölfel D, Maier-Brandt B. Severe intracranial hemorrhage in a newborn infant with transplacental transfer of an acquired factor VII:C inhibitor. J Pediatr. 1995;127(4):649–650. | ||
James AH. More than menorrhagia: a review of the obstetric and gynaecological manifestations of bleeding disorders. Haemophilia. 2005;11(4):295–307. | ||
Al-Zirqi I, Vangen S, Forsen L, Stray-Pedersen B. Prevalence and risk factors of severe obstetric haemorrhage. BJOG. 2008;115(10):1265–1272. | ||
Triche EW, Wehrum MJ, Paidas MJ. A survey of current treatment practices for postpartum hemorrhage by practicing obstetricians and hematologists. Open J Obstet Gynecol. 2014;4(6):279–293. | ||
Reding MT, Cooper DL. Barriers to effective diagnosis and management of a bleeding patient with undiagnosed bleeding disorder across multiple specialties: results of a quantitative case-based survey. J Multidiscip Healthc. 2012;5:277–287. | ||
Ma AD, Kessler CM, Al-Mondhiry HAB, Gut RZ, Cooper DL. US Experience with Recombinant Factor VIIa (rFVIIa) for Surgery and Other Invasive Procedures in Acquired Hemophilia: Analysis From the Hemophilia & Thrombosis Research Society Registry. Haemophilia. In press 2015. | ||
Abdul-Kadir R, McLintock C, Ducloy AS, et al. Evaluation and management of postpartum hemorrhage: consensus from an international expert panel. Transfusion. 2014;54(7):1756–1768. | ||
Rath WH. Postpartum hemorrhage – update on problems of definitions and diagnosis. Acta Obstet Gynecol Scand. 2011;90(5):421–428. | ||
Stafford I, Dildy GA, Clark SL, Belfort MA. Visually estimated and calculated blood loss in vaginal and cesarean delivery. Am J Obstet Gynecol. 2008;199(5):519.e1–e7. | ||
Zuckerwise LC, Pettker CM, Illuzzi J, Raab CR, Lipkind HS. Use of a novel visual aid to improve estimation of obstetric blood loss. Obstet Gynecol. 2014;123(5):982–986. | ||
Wise A, Clark V. Challenges of major obstetric haemorrhage. Best Pract Res Clin Obstet Gynaecol. 2010;24(3):353–365. | ||
Ahonen J, Stefanovic V, Lassila R. Management of post-partum hemorrhage. Acta Anaesthesiol Scand. 2010;54(10):1164–1178. | ||
Bonnet MP, Basso O. Prohemostatic interventions in obstetric hemorrhage. Semin Thromb Hemost. 2012;38(3):259–264. | ||
McLintock C, James AH. Obstetric hemorrhage. J Thromb Haemost. 2011;9(8):1441–1451. | ||
Huissoud C, Carrabin N, Audibert F, et al. Bedside assessment of fibrinogen level in postpartum haemorrhage by thrombelastometry. BJOG. 2009;116(8):1097–1102. | ||
Afshari A, Wikkelsø A, Brok J, Møller AM, Wetterslev J. Thrombelastography (TEG) or thromboelastometry (ROTEM) to monitor haemotherapy versus usual care in patients with massive transfusion. Cochrane Database Syst Rev. 2011;(3):CD007871. | ||
Kozek-Langenecker SA, Afshari A, Albaladejo P, et al. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2013;30(6):270–382. | ||
Kamal AH, Tefferi A, Pruthi RK. How to interpret and pursue an abnormal prothrombin time, activated partial thromboplastin time, and bleeding time in adults. Mayo Clin Proc. 2007;82(7):864–873. | ||
O’Connor CR, Reginato AJ, Ing JH, Keech JA. Prolonged activated partial thromboplastin time in systemic lupus erythematosus overlap syndrome: fatal bleeding due to factor VIII inhibitor. J Clin Rheumatol. 1995;1(1):57–59. | ||
Ballard HS, Nyamuswa G. Life-threatening haemorrhage in a patient with rheumatoid arthritis and a lupus anticoagulant coexisting with acquired autoantibodies against factor VIII. Br J Rheumatol. 1993;32(6):515–517. | ||
Lim S, Zuha R, Burt T, Chacko J, Scott R, Mainwaring CJ. Life-threatening bleeding in a patient with lupus inhibitor and probable acquired factor VII deficiency. Blood Coagul Fibrinolysis. 2006;17(8):667–671. | ||
Saxena R, Mishra DK, Kashyap R, Choudhry VP, Mahapatra M, Bhargava M. Acquired haemophilia – a study of ten cases. Haemophilia. 2000;6(2):78–83. | ||
Taher A, Abiad R, Uthman I. Coexistence of lupus anticoagulant and acquired haemophilia in a patient with monoclonal gammopathy of unknown signficance. Lupus. 2003;12(11):854–856. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.