")
Back to Journals » Clinical Interventions in Aging » Volume 15
Hemodynamic Effects of a Multidisciplinary Geriatric Rehabilitation Program
Authors Pagonas N, Bauer F, Zappe L, Seibert FS , Rohn B, Klimek C, Wirth R , Gotzmann M, Babel N, Westhoff TH
Received 24 November 2019
Accepted for publication 1 May 2020
Published 30 June 2020 Volume 2020:15 Pages 1035—1043
DOI https://doi.org/10.2147/CIA.S239844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Nikolaos Pagonas,1,2,* Frederic Bauer,1,* Laura Zappe,1 Felix S Seibert,1 Benjamin Rohn,1 Christiane Klimek,3 Rainer Wirth,3 Michael Gotzmann,4 Nina Babel,1 Timm H Westhoff1
1University Hospital Marien Hospital Herne, Department of Internal Medicine I, Ruhr-University Bochum, Bochum, Germany; 2University Hospital Brandenburg, Department of Cardiology, Brandenburg Medical School, Brandenburg an der Havel, Germany; 3University Hospital Marien Hospital Herne, Department of Geriatrics, Ruhr-University Bochum, Bochum, Germany; 4University Hospital St Josef Hospital Bochum, Cardiology, Ruhr University Bochum, Bochum, Germany
*These authors contributed equally to this work
Correspondence: Timm H Westhoff
University Hospital Marien Hospital Herne, Department of Internal Medicine I, Ruhr-University Bochum, Bochum, Germany
Email [email protected]
Background: Geriatric rehabilitation programs primarily aim at an increase of mobility and functional autonomy of the elderly. The cardiovascular effects of these programs, however, remain elusive. Since regular physical exercise is associated with numerous beneficial cardiovascular effects including a reduction of blood pressure (BP), the present prospective study investigates the hemodynamic effects of a representative standardized rehabilitation program.
Methods: A total of 74 subjects who were hospitalized in a German university hospital for geriatric rehabilitation were enrolled in the study. Peripheral BP, central aortic BP, 24h-ambulatory BP, heart rate and pulse wave velocity as a measure of arterial stiffness were assessed at admission and before discharge from the hospital. The program contained 4– 5 sessions of physical activity of individualized intensity per week (≥ 30 min/session, eg, walking, cycling, stair rising).
Results: The mean age of the study population was 82.4± 6.9 years; all patients suffered from arterial hypertension (stage 2– 3) with a median number of three antihypertensive drugs. The most frequent cause for admission was injurious falls. The mean duration of the rehabilitation program was 17 days and comprised at least 20 physical activity sessions including occupational therapy. The program led to a significant improvement of mobility (Timed Up & Go 29.5± 18.5 vs 19.1 ± 9.3 s, p< 0.001) and Barthel index of activities of daily living score (46.6± 19.1 vs 69.8± 16.5, p< 0.001). Peripheral systolic BP decreased from 135.4± 19.0 mmHg at baseline to 129.0± 18.4 mmHg at follow-up (p=0.03), whereas peripheral diastolic BP, central aortic BP, 24h-ambulatory BP, heart rate and pulse wave velocity as a measure of arterial stiffness were not significantly altered (p> 0.05 each).
Conclusion: The present representative standardized geriatric rehabilitation program was able to improve mobility, which showed a mild effect on systolic BP but did not affect 24h-ambulatory BP.
Keywords: exercise, rehabilitation program, geriatric, blood pressure, hypertension
Introduction
Physical exercise on a regular basis induces multiple beneficial cardiovascular effects including a reduction of blood pressure (BP).1 It is therefore strongly recommended as a basic lifestyle modification by current hypertension guidelines.2,3 In normotensives, regular exercise reduces systolic BP by 3–5 mmHg and diastolic BP by 2–3 mmHg. In hypertensives, this effect is more pronounced yielding a mean reduction of 7 mmHg systolic and 5 mmHg diastolic.4,5 With regard to the advanced arteriosclerotic wall changes, comorbidities and limited physical fitness skepticism was expressed whether elderly patients could achieve relevant changes of BP as well. In the past years, however, we and others have shown that aerobic exercise is able to reduce BP even in the elderly.6–8 Noteworthy, even subjects with increased arterial stiffness and isolated systolic hypertension demonstrated a significant benefit in BP control.6 Data on the necessary intensity of exercise training in the elderly, however, are sparse.
Geriatric rehabilitation programs aim primarily at an improvement of the mobility and functional autonomy of the elderly individual. They therefore contain predefined minimum numbers of supervised physical activity sessions (4–5/week, overall ≥20) of individualized intensity for a period of 2–3 weeks. The program consists of aerobic training (bicycle ergometer, stair rising), isometric training and occupational therapy. Whereas there is convincing evidence for the benefits in mobility, it remains elusive whether these training sessions are able to induce a measurable effect on BP and arterial function. Do the exercise intensity, the number of sessions and the duration of the overall program suffice to induce hemodynamic effects? In addition to peripheral BP, it would be interesting to know, whether there are effects on central BP. Since the CAFE trial, a sub-study of ASCOT, it has increasingly been recognized that central aortic BP has a higher prognostic impact on stroke than peripheral BP.9
Geriatric rehabilitation programs primarily aim at an improvement of the mobility and functional autonomy of the elderly individual. Over a period of 2–3 weeks, they encompass 10–15 sessions of physical activity. Patients are usually admitted for cardiovascular problems like stroke, or skeletal problems including osteoporosis, osteoarthritis and knee/hip replacements. Whereas there is convincing evidence for the benefits in mobility, it remains elusive whether these training sessions are able to induce measurable hemodynamic effects as well, eg, on BP and arterial function.
The primary hypothesis of the present prospective study was that a standardized multidisciplinary geriatric rehabilitation inpatient program is able to reduce peripheral systolic BP. Moreover, the study investigates the effect on central aortic BP, 24h-ambulatory BP (ABP), heart rate, and pulse wave velocity (PWV) as a measure of arterial stiffness in a German university hospital.
Materials and Methods
Study Design and Protocol
Patients were recruited from the geriatric ward of a German university hospital. Inclusion criteria were: Admission to the Department of Geriatrics for a standardized rehabilitation program in an inpatient setting, written informed consent. Exclusion criteria: Inability to participate in the program in an adequate manner for cognitive (dementia, delirium) or physical reasons; surgical contraindications for mobilization.
The standardized geriatric rehabilitation program comprised at least 20 physical activity sessions including aerobic training, isometric training and occupational therapy. The aerobic exercise included an individualized mixture of bicycle ergometer, gait training and stair climbing for 30 min per day. In patients who were not able to walk, isometric strength training of the lower limb was performed instead of walking and stair climbing. Both trainings were supervised by a physiotherapist. The target was to perform exercise at a level similar to the Borg Scale 13 (somewhat hard). The Borg scale ranges from 6 to 20 with “6” corresponding to a “very, very light effort” and “20” corresponding to “exhaustion”. The occupational sessions were conducted by an occupational therapist for 30 min per day and included mainly training of basic activities of daily living.
The investigation took part in a real-life setting of a geriatric acute care ward. With regard to the huge variability of physical performance in elderly participants, the determination of exercise intensity necessitated a strong individualization. Therefore, training intensity was guided by the level of perceived exertion and not eg lactate levels. Medical staff intended, as mentioned above, a training intensity corresponding to level 13 of the Borg scale.
The overall program had duration of two to three weeks. Peripheral BP, central aortic BP, 24h-ABP, heart rate and PWV as a marker of arterial stiffness were measured before and after the standardized rehabilitation program. Baseline parameters were assessed within the first 2 days of the program, follow-up examinations at least 2 hours with most of them being performed the day after the final session. A significant change of systolic peripheral BP from baseline to follow-up was defined as the primary endpoint.
Patients’ characteristics including reason for admission to the rehabilitation program and concomitant diseases are presented in Table 1. The number of antihypertensive drugs for each patient ranged from 1 to 5 (median 3). Thirty-four subjects (45.9%) fulfilled the criteria of resistant hypertension (peripheral blood pressure ≥140/90 mmHg despite three or more antihypertensive agents, one of which was a diuretic).10 Antihypertensive medication contained diuretics, calcium-channel blockers, β-blockers, ACE inhibitors, AT1 blockers, alpha-blockers, moxonidine, and clonidine. In order to minimize the bias of compliance concerning antihypertensive drug intake during the study, all the patients were insistently and repeatedly requested to take care of an accurate drug intake. Written informed consent was obtained from all participants before inclusion in the study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee at the Ruhr-University Bochum (April 22nd, 2015). Data were collected from May 2015 to April 2016.
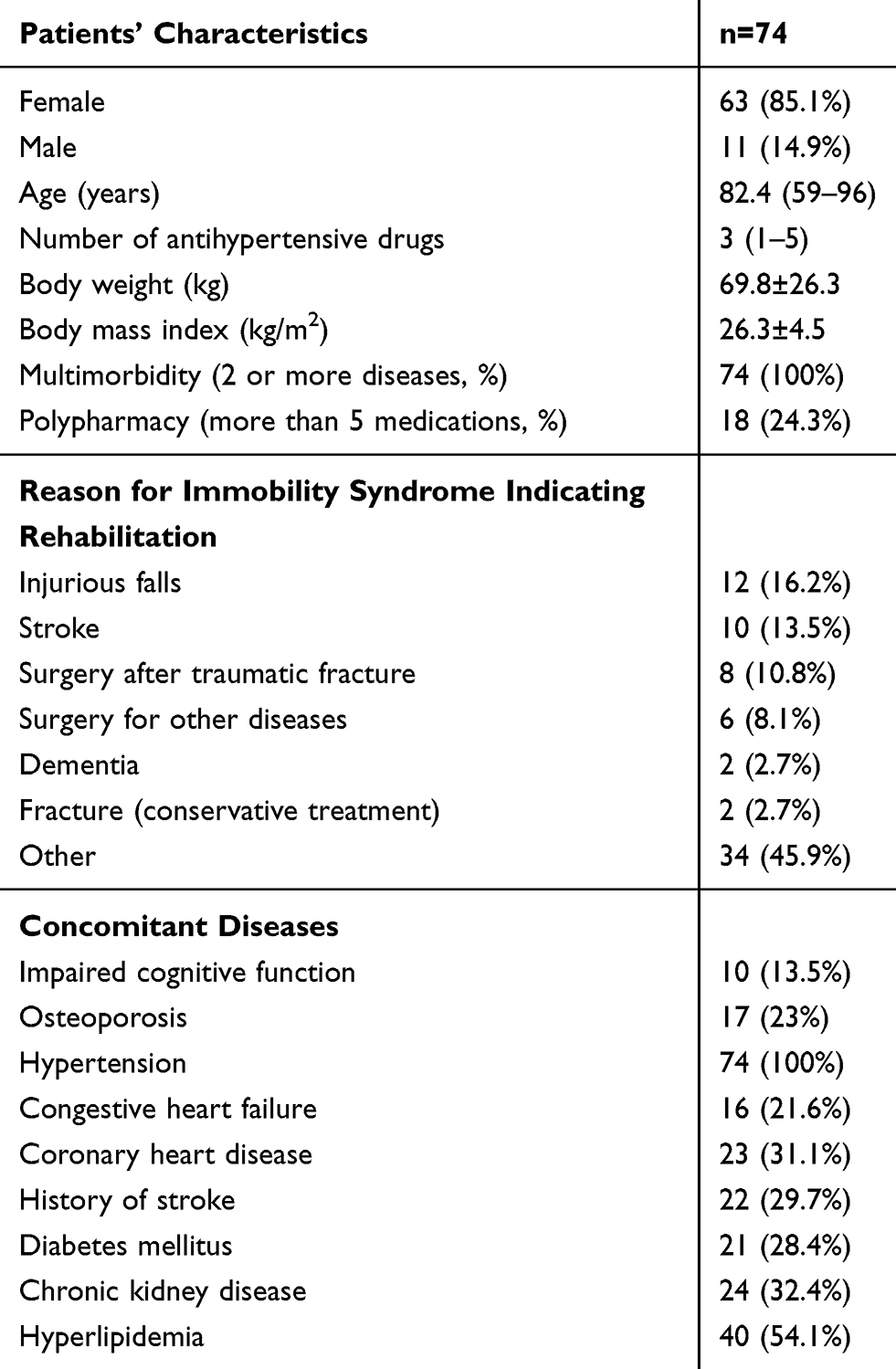 |
Table 1 Study Population |
Assessment of Mobility and Daily Life Competences
A geriatric assessment was routinely performed after admission and before discharge in every patient taking part in the geriatric rehabilitation program. Mobility was assessed by the Timed Up & Go test.11 In this test, the subject is requested to stand up from the chair, walk a predefined distance, turn around, walk back, and sit down again. An older adult who takes ≥12 seconds to complete the test is regarded at risk for falling. The ability to perform daily life activities was assessed by the German version of the Barthel index of activities of daily living score.12 This score summarizes the subject’s competences in, eg, food intake, bathing, dressing, bladder control, and mobility. If the subject is able to perform all these activities by himself, the maximal score is 100.
Assessment of Hemodynamic Parameters
Peripheral BP was measured with an automated oscillometric device (OMRON Healthcare Co., Kyoto, Japan). Assessments of BP were performed as single measurements after >5 min of rest. 24h-ABP monitoring was performed using Spacelabs 90,207 monitors (Spacelabs, Redmond, Washington, USA). Intervals between single measurements were set to be 20 min during daytime (6 a.m. to 10 p.m.) and 30 min during nighttime (10 p.m. to 6 a.m.). Central aortic BP and PWV were assessed by the SphygmoCor device (AtCor MedicalR, Sydney, Australia) as recommended and published previously.13,14 Briefly, recording of radial pressure waveforms was performed by a high-fidelity micromanometer placed on the tip of a hand-held tonometer (Millar InstrumentsR, Houston, USA), which was positioned above the radial artery. Pulse waves were recorded for 12 s. In accordance with the manufacturer’s recommendations several recordings were taken if needed in order to accomplish recommended quality control criteria, namely a quality index ≥80%. Transformation of peripheral pressure waveforms was performed by means of a generalized transfer function, which had been previously validated by intra-arterially measured pressure waves.15,16 Calibration of the recorded pressure waveforms was performed using the brachial systolic and diastolic BP values. PWV was calculated from measurements of pulse transit time and the distance travelled between two recording sites as “PWV = distance/transit time”. An electrocardiogram (ECG) was used to determine the start of the pulse-wave. The mean of 12 s of tonometer recorded pulse-waves at the radial and carotid artery were used to determine the arrival of the pulse-wave at the peripheral recording site (aortic PWV). The distance was measured between the recording sites and the suprasternal notch. The mean value of three consecutive measurements was used for statistical analysis.
Sample Size Estimation
Based on previous studies on exercise in hypertension, we expected the intervention to result in a decrease of peripheral systolic BP of at least 5 mmHg.7,17–19 This difference was considered to be clinically relevant. A sample size of 71 has 80% power to detect this difference assuming that the common standard deviation is 15 mmHg in a paired t-test with a two-sided p<0.05. We estimated the drop-out rate to be 5% leading to an overall sample size of 74 patients.
Statistical Analysis
Numeric data are presented as mean ± standard deviation, number of antihypertensive drugs as median and range. Data were tested for normal distribution by the Kolmogorov–Smirnov test. Changes of numeric parameters from baseline to follow-up were analyzed using a paired two-tailed Student’s t-test in case of normal distribution and a Wilcoxon signed-rank test in case of lacking normal distribution. P<0.05 was regarded significant. All statistical analysis was done using SPSS Statistics 21 (SPSS Inc, Chicago, Illinois, USA).
Results
The study population comprised 74 subjects with a mean age of 82.4±6.9 years. The most frequent reason for admission to the rehabilitation program was injurious falls (16.2%), followed by stroke (13.5%), and surgery after fracture (10.8%). Table 1 summarizes the epidemiological data, reason for admission to rehabilitation, and concomitant diseases of the population. The participants showed a high level of comorbidity, functional impairment and disability with 100% having hypertension, 21.6% congestive heart failure, 31.1% coronary heart disease, and 28.4% diabetes. Assessment of mobility at baseline revealed a strongly impaired state with a mean Timed Up & Go of 29.5±18.5 s and a poor Barthel index of daily living score (46.6±19.1). All except of 9 patients completed the rehabilitation program (Supplement Figure 1, flow Figure).
Figure 1 and Table 2 illustrate the individual hemodynamic parameters before and after the program. Figure 2 shows the development of functional parameters. The program was associated with a significant improvement in mobility: The duration of the Timed Up & Go test significantly decreased from 29.5±18.5 s to 19.1±9.3s (p<0.001). Moreover, the Barthel index of activities of daily living score significantly increased from 46.6±19.1 to 69.8±16.5 (p<0.001) indicating an improvement in daily life competences and less dependence from external help. As shown in Table 2, baseline peripheral BP was 135.4±19.0 mmHg systolic and 74.3±12.4 mmHg diastolic. Assessment of central aortic systolic BP was successful in 67% of the subjects at baseline and turned out to be 137.4±18.4 mmHg. Forty subjects (54%) had a 24h-ABP both before and after the rehabilitation program. Mean baseline 24h-ABP was 133.4±19.4/75.8±8.6 mmHg. Mean heart rate was 64.6±11.4/min with 57% of the subjects being administered beta-blockers. Arterial stiffness was high with a mean PWV of 11.2±2.5 m/s.
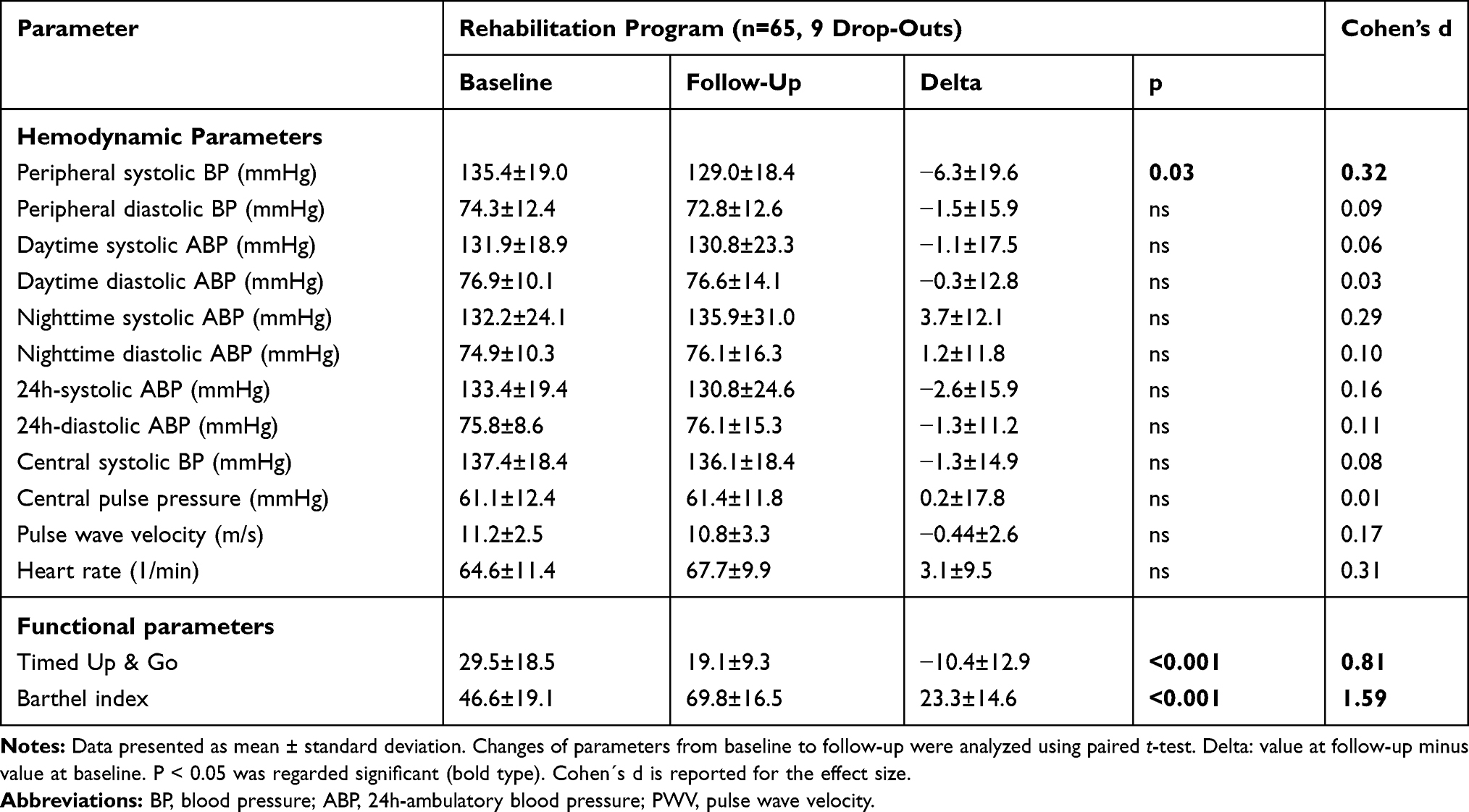 |
Table 2 Hemodynamic and Functional Parameters Before and After the Geriatric Rehabilitation Program |
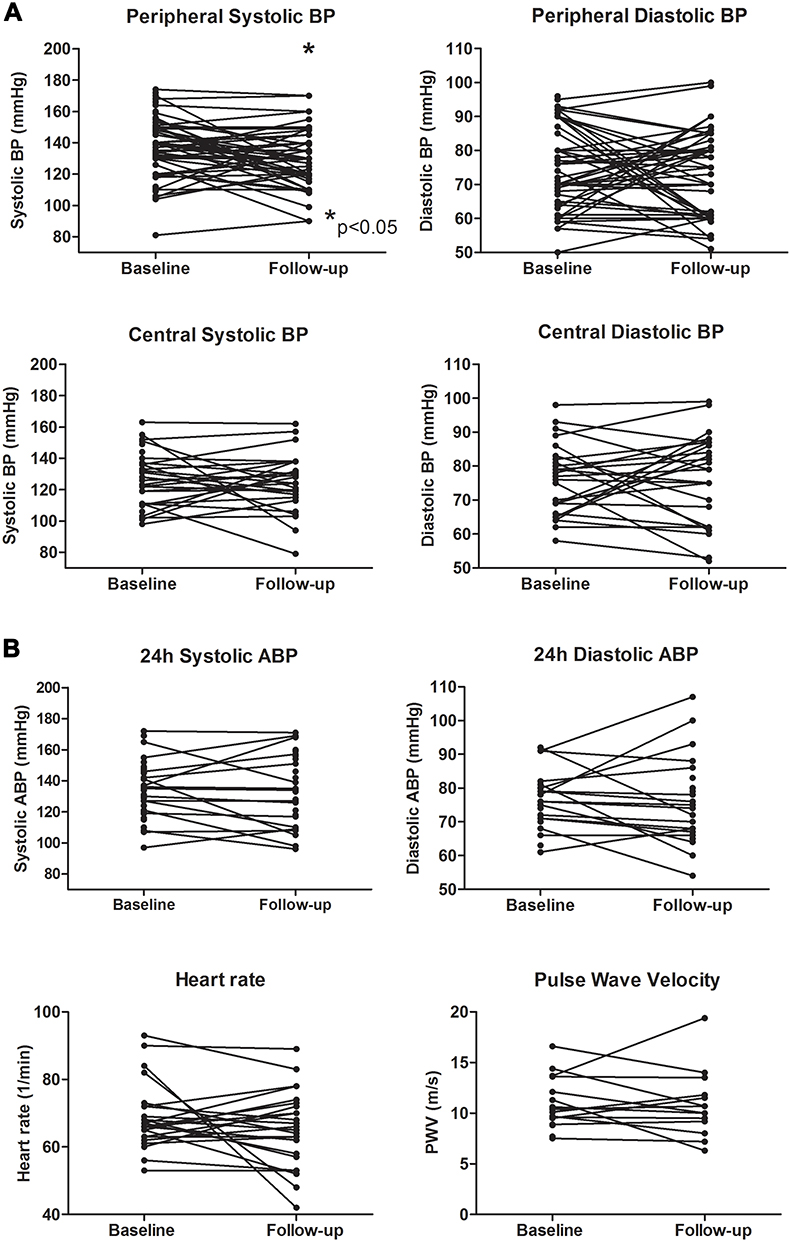 |
Figure 1 Individual hemodynamic parameters before (baseline) and after (follow-up) the geriatric rehabilitation program. (A) Peripheral and central aortic blood pressure (BP), (B) 24h-ambulatory blood pressure (ABP), heart rate and pulse wave velocity (PWV). |
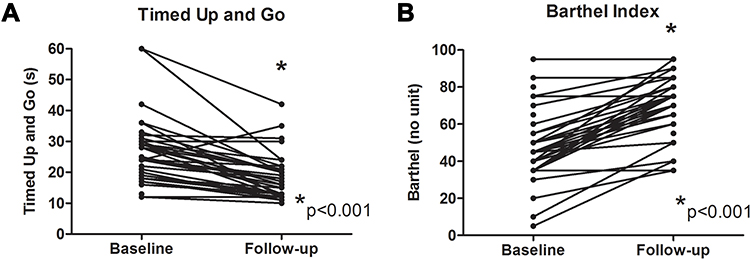 |
Figure 2 Individual functional parameters before (baseline) and after (follow-up) the geriatric rehabilitation program. (A) Timed Up & Go and (B) Barthel index. |
At follow-up, peripheral systolic BP had decreased by 6.3±19.6 mmHg to 129.0±18.4 mmHg (p=0.03). By dividing patients into 2 groups, based on blood pressure at baseline: controlled hypertension (<140/90mmHg) and uncontrolled hypertension (≥140/90mmHg) was demonstrated that only the uncontrolled group did have a significant reduction of the systolic blood pressure (from 150.8±10.3 to 134.4±19, p<0.001) with no change of the diastolic blood pressure (p>0.05). In older patients with controlled hypertension on baseline no change of the blood pressure was seen (p>0.05). Peripheral diastolic BP, central aortic systolic BP, 24h-ABP, and heart rate were not significantly different from baseline parameters after completion of the rehabilitation program (p>0.05 each). Arterial stiffness as measured by PWV was not significantly affected either (p>0.05 each).
In 13 subjects antihypertensive medication was intensified (n=8) or replaced by another medication (n=5) during rehabilitation. After exclusion of these subjects the peripheral systolic blood pressure still tended to be decreased from 136.4±19.8 to 130.6±19.2 mmHg, but the effect failed to reach statistical significance (p=0.06). In analogy to the overall study population, peripheral diastolic BP, central aortic systolic BP, 24h-ABP, heart rate, and PWV did not significantly change from baseline to follow-up (p>0.05 each, Supplement Table 1).
Changes in the Timed Up & Go test and Barthel index remained significant (p<0.001, Supplement Table 1).
Discussion
The present study shows that a 2–3 weeks geriatric rehabilitation program provides a substantial improvement in mobility and additionally has a mild effect on peripheral BP in frail elderly patients. Systolic BP decreased by 5–6 mmHg. There was no effect on diastolic blood pressure, central aortic BP, 24h-ambulatory BP, heart rate and pulse wave velocity as a measure of arterial stiffness.
Physical exercise generally has a stronger impact on systolic than on diastolic blood pressure.20 This phenomenon is even more pronounced in isolated systolic hypertension, the typical form of hypertension in the elderly. Isolated systolic hypertension results from high aortic stiffness with reduced Windkessel function. Indeed, the present study in an 82-year-old population had both a PWV > 11 m/s and a pulse pressure >60 mmHg, both indicating substantially increased arterial stiffness. Since advanced arteriosclerosis encompasses peripheral arteries as the targets of most antihypertensive drugs as well, isolated systolic hypertension frequently constitutes a therapeutic challenge and requires a combination of multiple antihypertensive drugs. Accordingly, 46% of the present population suffered from resistant hypertension. Whereas the reduction of systolic office blood pressure by e g a calcium channel blocker is about 10–15 mmHg in the general population, it is markedly lower in the elderly population.21 Since the BP lowering effect is mediated at least in part by a modification of vascular tone as well. In this context, the decrease of 5–6 mmHg in the present study is still quite remarkable. Interestingly, these 5–6 mmHg resemble exactly the effect that has been demonstrated in prior trials on exercise in elderly hypertensives.7,22
The HYVET and the SPRINT-SENIOR trial showed impressively that a reduction of BP substantially reduces cardiovascular morbidity and mortality even in the (very) elderly.23,24 The most pronounced benefit is a reduction of hospitalizations for congestive heart failure.23,24 Moreover, a more intense antihypertensive regimen is able to reduce mild cognitive dysfunction and dementia.25 Although the SPRINT-SENIOR did not find an increased number of injurious falls, antihypertensive therapy – including aerobic exercise – in the elderly should “start low and go slow” with regular measurements of BP in an upright position in order to detect orthostatic dysregulation.
Finally, it should be considered that baseline systolic blood pressure was only 135 mmHg in the present population. Since the exercise-induced reduction of blood pressure increases with baseline blood pressure, an even more pronounced effect may be expected with higher initial blood pressure.6 A systolic BP reduction of 5 mmHg has to be regarded as clinically relevant, since it eg reduces the first incidence of fatal and nonfatal stroke by 29%.26 The lacking effect on PWV shows that the exercise program was not able to induce a measurable effect on the architecture of the arterial wall. This finding was not unexpected since arterial stiffness in the elderly is predominantly determined by the extent of arteriosclerosis.
The mechanisms underlying the exercise-induced effects on BP are incompletely understood. A reduction of sympathetic tone, an improvement of endothelium-dependent vasodilation, a reduction of reactive oxygen species, inflammation and arterial stiffness have been proposed to contribute to this phenomenon.27,28 The present study did not show an improvement of PWV as a measure of arterial stiffness. This is actually not surprising, since changes in the vascular architecture necessitate a substantially longer period of regular exercise.29 Moreover, there was no effect on 24h-ABP. It could therefore be speculated that the observed benefit in eventual BP corresponded to the so-called “post exercise hypotension” – a short period of reduced BP immediately after physical activity. To avoid the detection of post-exercise hypotension, however, measurements of eventual BP were performed at least 2 hours after the last physical activity session or the day after that. Whereas eventual BP readings were available in all the study participants, 46% refused another 24h-ABP or discontinued it after completion of the program. This may have contributed to the discrepancy between eventual and 24h-ABP readings. For the time being, it has to be stated that the study did not prove a long-term effect of the program on BP.
The lack of a more pronounced BP effect of the geriatric rehabilitation program is not unexpected. Geriatric rehabilitation programs are intended to primarily address functional deficits and thereby to improve balance, coordination, and mobility. These programs do not focus on cardiovascular effects of exercise training. Exercise intensity is usually low. As indicated by the baseline Timed Up & Go test, the age and the extent of comorbidities, the study population showed a substantially impaired mobility and physical capacity. With a mean age of 82 years and the documented comorbidities, our study population is quite representative for the patients in a geriatric rehabilitation program.
The present study is limited by several aspects: Peripheral BP was assessed by single measurements and training sessions were individualized to the patients’ condition. Therefore, there was a high variability of training intensity. This limitation was inevitable, however, since the study intended to investigate the cardiovascular effects in a real-life setting. For the same reason, there was no control group. Naturally, it is not possible to withhold physical exercise to a patient who is admitted for geriatric rehabilitation. Thus, it cannot finally be excluded that further factors including a regression to the mean phenomenon contribute to the decrease of BP.30 As a further limitation, not all the subjects agreed to perform an analysis of arterial function and 24h-ABP. Finally, the different time points of the follow-up examination (between 2 hours and 1 day after the last session) may influence the results as long as a residual effect of the last exercise session may still be detectable.
Conclusions
The present work constitutes the first prospective trial investigating the effects of a geriatric rehabilitation program on arterial function, peripheral and central aortic BP. It shows that a geriatric rehabilitation is able to provide mild cardiovascular benefits in addition to the improvement of the mobility and functional autonomy of older patients.
Abbreviations
BP, blood pressure; ABP, ambulatory blood pressure; PWV, pulse wave velocity.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brook RD, Appel LJ, Rubenfire M, et al. Beyond medications and diet: alternative approaches to lowering blood pressure: a scientific statement from the american heart association. Hypertension. 2013;61(6):1360–1383. doi:10.1161/HYP.0b013e318293645f
2. Williams B, Mancia G, Spiering W, et al., 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104.
3. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2018;138(17):e426–e483. doi:10.1161/CIR.0000000000000597
4. Pescatello LS, MacDonald HV, Lamberti L, Johnson BT. Exercise for hypertension: a prescription update integrating existing recommendations with emerging research. Curr Hypertens Rep. 2015;17(11):87. doi:10.1007/s11906-015-0600-y
5. Cornelissen VA, Fagard RH. Effects of endurance training on blood pressure, blood pressure-regulating mechanisms, and cardiovascular risk factors. Hypertension. 2005;46(4):667–675. doi:10.1161/01.HYP.0000184225.05629.51
6. Westhoff TH, Franke N, Schmidt S, et al. Too old to benefit from sports? The cardiovascular effects of exercise training in elderly subjects treated for isolated systolic hypertension. Kidney Blood Press Res. 2007;30(4):240–247. doi:10.1159/000104093
7. Dimeo F, Pagonas N, Seibert F, Arndt R, Zidek W, Westhoff TH. Aerobic exercise reduces blood pressure in resistant hypertension. Hypertension. 2012;60(3):653–658. doi:10.1161/HYPERTENSIONAHA.112.197780
8. Herrod PJJ, Doleman B, Blackwell JEM, et al. Exercise and other nonpharmacological strategies to reduce blood pressure in older adults: a systematic review and meta-analysis. J Am Soc Hypertens. 2018;12(4):248–267. doi:10.1016/j.jash.2018.01.008
9. Williams B, Lacy PS, Thom SM, et al. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the conduit artery function evaluation (cafe) study. Circulation. 2006;113(9):1213–1225. doi:10.1161/CIRCULATIONAHA.105.595496
10. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the american heart association professional education committee of the council for high blood pressure research. Hypertension. 2008;51(6):1403–1419. doi:10.1161/HYPERTENSIONAHA.108.189141
11. Podsiadlo D, Richardson S. The timed “up & go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
12. Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61–65.
13. Agabiti-Rosei E, Mancia G, O’Rourke MF, et al. Central blood pressure measurements and antihypertensive therapy: a consensus document. Hypertension. 2007;50(1):154–160. doi:10.1161/HYPERTENSIONAHA.107.090068
14. Seibert FS, Steltzer J, Melilli E, et al. Differential impact of belatacept and cyclosporine a on central aortic blood pressure and arterial stiffness after renal transplantation. Clin Transplant. 2014;28(9):1004–1009. doi:10.1111/ctr.12413
15. Karamanoglu M, O’Rourke MF, Avolio AP, Kelly RP. An analysis of the relationship between central aortic and peripheral upper limb pressure waves in man. Eur Heart J. 1993;14(2):160–167. doi:10.1093/eurheartj/14.2.160
16. Pauca AL, O’Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001;38(4):932–937. doi:10.1161/hy1001.096106
17. Arakawa K. Antihypertensive mechanism of exercise. J Hypertens. 1993;11(3):223–229. doi:10.1097/00004872-199303000-00001
18. Fagard RH. Exercise characteristics and the blood pressure response to dynamic physical training. Med Sci Sports Exerc. 2001;33(Supplement):S484–492. doi:10.1097/00005768-200106001-00018
19. Pescatello LS, Franklin BA, Fagard R, Farquhar WB, Kelley GA, Ray CA. American college of sports medicine position stand. Exercise and hypertension. Med Sci Sports Exerc. 2004;36(3):533–553. doi:10.1249/01.MSS.0000115224.88514.3A
20. Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, controlled trials. Ann Intern Med. 2002;136(7):493–503. doi:10.7326/0003-4819-136-7-200204020-00006
21. Messerli FH, Bangalore S, Bavishi C, Rimoldi SF. Angiotensin-converting enzyme inhibitors in hypertension: to use or not to use? J Am Coll Cardiol. 2018;71(13):1474–1482. doi:10.1016/j.jacc.2018.01.058
22. Stewart KJ, Bacher AC, Turner KL, et al. Effect of exercise on blood pressure in older persons: a randomized controlled trial. Arch Intern Med. 2005;165(7):756–762. doi:10.1001/archinte.165.7.756
23. Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358(18):1887–1898. doi:10.1056/NEJMoa0801369
24. Williamson JD, Supiano MA, Applegate WB, et al. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >/=75 years: a randomized clinical trial. JAMA. 2016;315(24):2673–2682. doi:10.1001/jama.2016.7050
25. Williamson JD, Pajewski NM, Auchus AP, et al., Group SMIftSR. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. 2019;321(6):553–561. doi:10.1001/jama.2018.21442
26. Pats collaborating group. Post-stroke antihypertensive treatment study. A preliminary result. Chin Med J. 1995;108(9):710–717.
27. Diaz KM, Shimbo D. Physical activity and the prevention of hypertension. Curr Hypertens Rep. 2013;15(6):659–668. doi:10.1007/s11906-013-0386-8
28. Moraes-Silva IC, Mostarda C, Moreira ED, et al. Preventive role of exercise training in autonomic, hemodynamic, and metabolic parameters in rats under high risk of metabolic syndrome development. J Appl Physiol. 2013;114(6):786–791. doi:10.1152/japplphysiol.00586.2012
29. Otsuki T, Namatame H, Yoshikawa T, Zempo-Miyaki A. Combined aerobic and low-intensity resistance exercise training increases basal nitric oxide production and decreases arterial stiffness in healthy older adults. J Clin Biochem Nutr. 2020;66(1):62–66. doi:10.3164/jcbn.19-81
30. Atkinson G, Taylor C. Normalization effect of sports training on blood pressure in hypertensive individuals: regression to the mean? J Sports Sci. 2011;29(6):643–644. doi:10.1080/02640414.2010.510848
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.