")
Back to Journals » International Journal of General Medicine » Volume 14
Hemodynamic Characteristics of Patients with Myocardial Injury and Cardiogenic Shock Caused by Severe COVID-19-Related Pneumonia
Authors Liu Y, Chen Y, Chen J, Kuang Y, Tan N, Jiang K, Peng S, Hu C
Received 20 August 2021
Accepted for publication 30 November 2021
Published 14 December 2021 Volume 2021:14 Pages 9647—9655
DOI https://doi.org/10.2147/IJGM.S334442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yongjun Liu,1,* Yuee Chen,2,* Jie Chen,3 Yukung Kuang,4 Niandi Tan,5 Ke Jiang,6 Shuihui Peng,7 Chunlin Hu2
1Department of Critical Care Medicine, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, Province Guangdong, People’s Republic of China; 2Department of Emergency Medicine, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, Province Guangdong, People’s Republic of China; 3Department of Critical Care Medicine, Dongguan People’s Hospital, Dongguan, Province Guangdong, 523059, People’s Republic of China; 4Division of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, Province Guangdong, People’s Republic of China; 5Department of Gastroenterology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China; 6Department of Thoracic Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 7Department of Pharmacy Intravenous Admixture Services, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, Province Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunlin Hu
Department of Emergency Medicine, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, Province Guangdong, People’s Republic of China
Email [email protected]
Shuihui Peng
Department of Pharmacy Intravenous Admixture Services, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, Province Guangdong, People’s Republic of China
Email [email protected]
Objective: To observe hemodynamic characteristics in a series of patients with myocardial injury caused by severe COVID-19-related pneumonia.
Materials and Methods: We continuously collected clinical data from severe COVID-19-related pneumonia patients from the West Campus of Union Hospital in Wuhan and Dongguan People’s Hospital in Dongguan to explore the prevalence of myocardial injury and hemodynamic characteristics after circulatory failure. Doppler ultrasound and PiCCO2 were used to evaluate the hemodynamics of each patient, and arterial blood gas analysis was performed at the same time. Pearson correlation analysis was used to clarify the relationship between the parameters.
Results: A total of 376 patients were observed during the study period. Eighty-seven patients had myocardial injury after admission, and the mean time of myocardial injury after admission was 6 (2, 30) days, from which 16 patients developed hemodynamic instability and 15 died of cardiogenic shock or combined with MODS. Cardiac echocardiography found that the LVEF of all patients was in the normal range and that diastolic function was slightly to moderately impaired. The PiCCO2 data showed that the GEF was significantly decreased in all patients. The dpmx was in normal range. EVLWI, SVRI and GEDI were significantly increased in most patients. Pearson correlation analysis showed that cTNI was significantly related to BNP at hemodynamic instability (r = 0.662, p = 0.005); GEF was related to EVLWI (r = − 0.572, p = 0.021) and LAC (r = 0.692, p = 0.003); and EVLWI was affected by LVEF (r = − 0.564, p = 0.023), LVDF (r = − 0.734, p = 0.001) and PVPI (r = − 0.524, p = 0.037).
Conclusion: Hemodynamic status after myocardial injury and cardiogenic shock caused by severe COVID-19-related pneumonia was characterized by cardiac preload and increased EVLWI, accompanied by a decline in GEF.
Keywords: COVID-19, PiCCO2, myocardial injury, hemodynamic instability
Introduction
Coronavirus disease 2019 (COVID-19) is a global epidemic. While most patients recover, those with severe illnesses, especially elderly patients, have higher mortality rates.1,2 COVID-19 is a systemic disease that damages various systems throughout the body. There are many underlying diseases in elderly patients. Since the emergence of the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), COVID-19 combined with the underlying conditions has resulted in aggravation of the disease and increased mortality. SARS-CoV-2 infects host cells through angiotensin-converting enzyme 2 (ACE2) receptors, leading to COVID-19-related pneumonia while also causing acute myocardial injury and chronic damage to the cardiovascular system.3 Myocardial injury associated with SARS-CoV-2 occurred in 5 of the first 41 patients diagnosed with COVID-19 in Wuhan, China, which mainly manifested as an increase in high-sensitivity cardiac troponin I (hs-TnI) levels (>28 pg/mL).4 In another report of 138 patients with COVID-19 in Wuhan, 36 patients with severe symptoms were treated in the intensive care unit (ICU).5 The levels of biomarkers of myocardial injury were significantly higher in patients treated in the ICU than in those not treated in the ICU, suggesting that patients with severe symptoms often have complications involving acute myocardial injury.4 However, the effects of myocardial injury on patients’ hemodynamics is still unclear.
Pulse indicator continuous cardiac output (PiCCO) monitoring technology is the combined application of pulse contour continuous cardiac output measurement and transpulmonary temperature dilution cardiac output measurement technology, which can systematically monitor the hemodynamic status of patients.6,7 This study used PiCCO to monitor the hemodynamic changes after myocardial injury in a series of patients with severe coronavirus disease-related pneumonia, which will help doctors make treatment decisions.
Materials and Methods
All patients were confirmed to have SARS-CoV-2 infection by real-time reverse transcription polymerase chain reaction (RT–PCR) and were admitted to a designated hospital (West Campus of Union Hospital, Huazhong University of Science and Technology in Wuhan, and Dongguan People’s Hospital ICU in Dongguan). We prospectively collected and analyzed data obtained from electronic medical records, including clinical charts, nursing records, laboratory findings, and chest X-rays, from February 8 to April 7, 2020.
Cardiac injury was diagnosed if serum levels of the cardiac biomarker hs-TnI were >28 pg/ml4 or if new abnormalities were shown on electrocardiography and echocardiography. COVID-19-related myocardial injury showed noncharacteristic ECG changes, such as ST segment deviation, presystole, atrioventricular block or sinus tachycardia. All patients were screened for clinical chest pain symptoms and electrocardiographic changes to rule out acute myocardial infarction (AMI). The ECG of AMI was mainly ST segment changes with positioning characteristics, mainly ST segment elevation, followed by the high cusp and inversion of T wave, and finally the formation of pathological Q wave. The changes in the ST segment were divided into ST segment elevation myocardial infarction (STEMI) and nonST segment elevation myocardial infarction (NSTEMI).
Echocardiograms
Ejection fraction was measured by quantitative 2-D methodology, as previously reported.8 Diastolic function was assessed by pulse wave Doppler examination of mitral flow, pulmonary venous flow, and Doppler imaging of the medial mitral annulus.8 Diastolic dysfunction was graded on a four-point ordinal scale: 1) normal; 2) mild diastolic dysfunction = abnormal relaxation without increased LV end-diastolic filling pressure (decreased E/A ratio <0.75); 3) moderate or “pseudonormal” diastolic dysfunction = abnormal relaxation with increased LV end-diastolic filling pressure (E/A 0.75 to 1.5, deceleration time >140 ms, plus 2 other Doppler indices of elevated end-diastolic filling pressure); 4) or severe diastolic dysfunction = advanced reduction in compliance, (ie, markedly increased stiffness) with restrictive filling (E/A ratio of >1.5, deceleration time <140 ms, and Doppler indices of elevated LV end-diastolic filling pressure).
Hemodynamic Measurements
The patients were placed in a supine position. The right femoral artery was dissected and a 6F arterial catheter inserted to measure blood pressure and cardiac output by means of a femoral arterial thermodilution system (PiCCO2, Pulsion Medical Systems, Munich, Germany). PiCCO2 is a combined application of pulse contour analysis and the thermodilution method for pulse indicator continuous cardiac output (PiCCO) technology, which can comprehensively evaluate the patient’s hemodynamic status. PiCCO2 can monitor the following indicators: 1. Indicators of cardiac output, such as cardiac output (CO) and stroke volume (SV); 2. Indicators of blood volume, such as global end diastolic volume (GEDV), intrathoracic blood volume (ITBV), stroke volume variation (SVV), and pulse pressure variation (PPV); 3. Indicators of organ function, such as extravascular lung water (EVLW) and pulmonary vascular permeability index (PVPI); 4. Indicators of vascular resistance, such as systemic peripheral vascular resistance (SVR) and arterial blood pressure (AP); 5. Indicators of cardiac function, such as cardiac function index (CFI), global ejection fraction (GEF), and left ventricular contraction index (dPmx).
Continuous hemodynamic surveillance was initiated using arterial pulse contour analyses with transpulmonary thermodilution calibration. At least three boluses of iced (<8 °C) 0.9% saline were injected through the central venous catheter into the right internal jugular vein, and the thermodilution curve was used to estimate hemodynamic variables. Triplicate consecutive injections for calibration were performed at setup, repeated every eight hours, or more frequently if indicated by changes in the special condition.
Statistics
Continuous variables were expressed as medians (interquartile ranges [IQRs]) and compared using the Mann–Whitney U-test. Pearson correlation analysis was used to analyze the relationship between different variables. Statistical analyses were performed using SPSS software, version 13.0 (IBM Corporation, Armonk, NY, USA).
Results
General Information
A total of 376 patients were observed during the study period, and all of the patients met the diagnostic criteria of severe COVID-19. According to the COVID-19 pneumonia diagnosis and treatment plan, trial version 7, patients with severe COVID-19 require oxygen inhalation to maintain SpO2 > 93% (Figure 1). Twenty-five patients with myocardial injury at admission were excluded, and 3 patients experienced myocardial injury during hospitalization, which was identified as acute myocardial infarction by the research team and was also excluded. Eighty-seven patients had myocardial injury after admission, with a mean time of myocardial injury after admission of 6 (2, 30) days and a mean time of discharge of 21 (11, 60) days, during which 16 patients developed hemodynamic instability. Vasoactive drugs were needed to maintain the mean arterial pressure above 70 mmHg, only 1 of these 16 patients survived and was discharged, and the remaining 15 died of cardiogenic shock or combined with MODS (Table 1). Three of fifteen patients who died received ECMO to support cardiopulmonary failure.
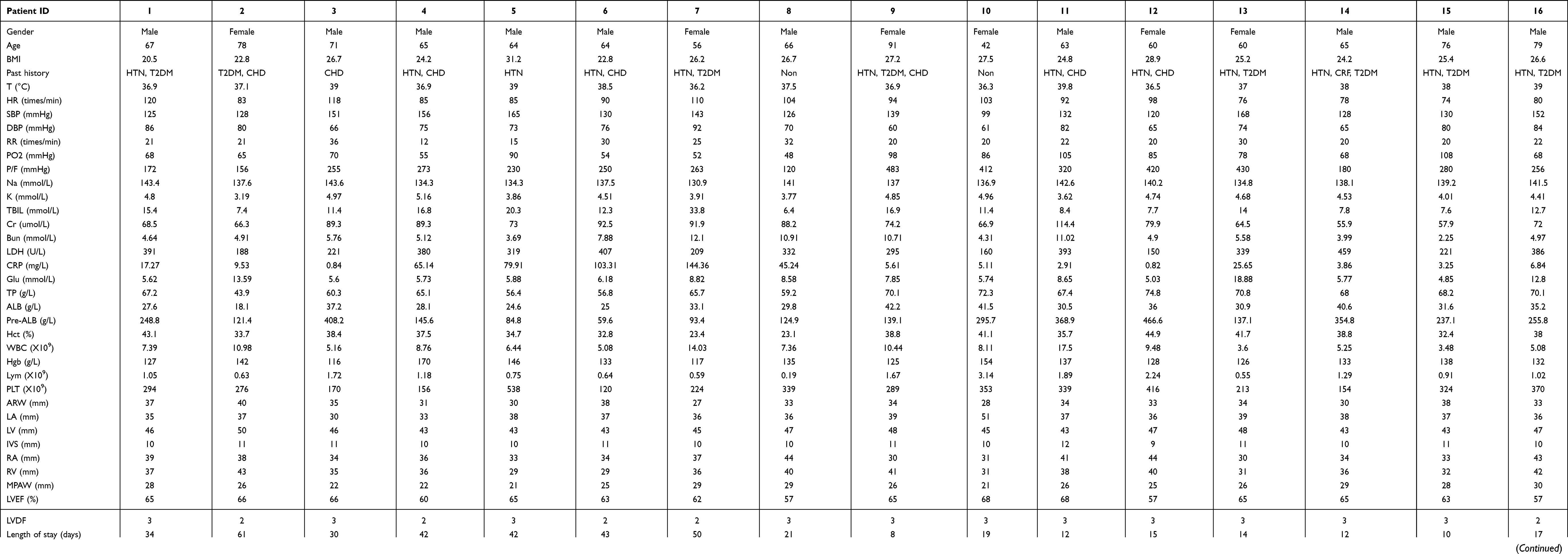 |
Table 1 The General Information of the Patients |
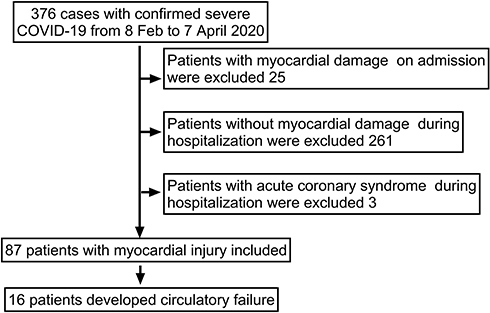 |
Figure 1 Patients recruitment flow-chart. |
Myocardial injury continued to progress, and the levels of cTNI, Myo, CK-MB, and pro-BNP progressively increased, and were significantly higher than those at admission (Table 2).
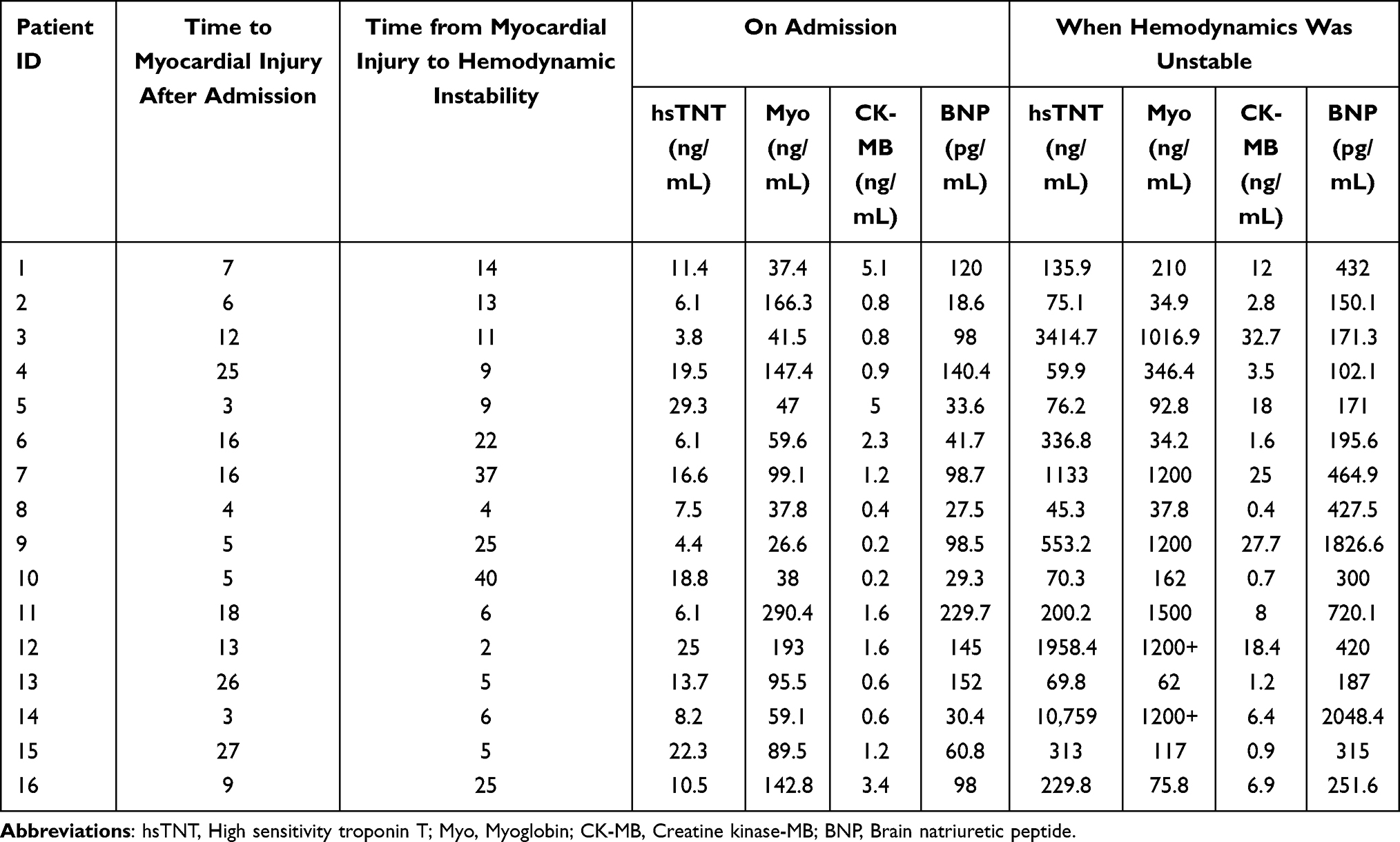 |
Table 2 Time to Myocardial Injury and Hemodynamic Instability After Admission |
After hemodynamic instability, we used bedside echocardiography to evaluate the cardiac function of the patients (Table 1). The LVEF of all patients was in the normal range, and diastolic function was slightly to moderately impaired. All patients had a history of hypertension and mild ventricular septal hypertrophy (9–11 mm). At almost the same time, we used PiCCO2 to monitor the hemodynamics of the patients. The PiCCO2 data are shown in Table 3, and the artery blood analysis results are shown in Table 4. The results showed that the GEF (reflecting the whole cardiac systolic function) was significantly decreased in all patients. The dpmx (reflecting left ventricular systolic performance) was close to the normal range, and SVRI (reflecting cardiac afterload) was significantly increased, which may be related to the use of vasoactive drugs, while GEDI (reflecting volume load) was significantly increased in most patients. ELWI (reference value 3–7 mL/kg) was significantly increased in all patients.
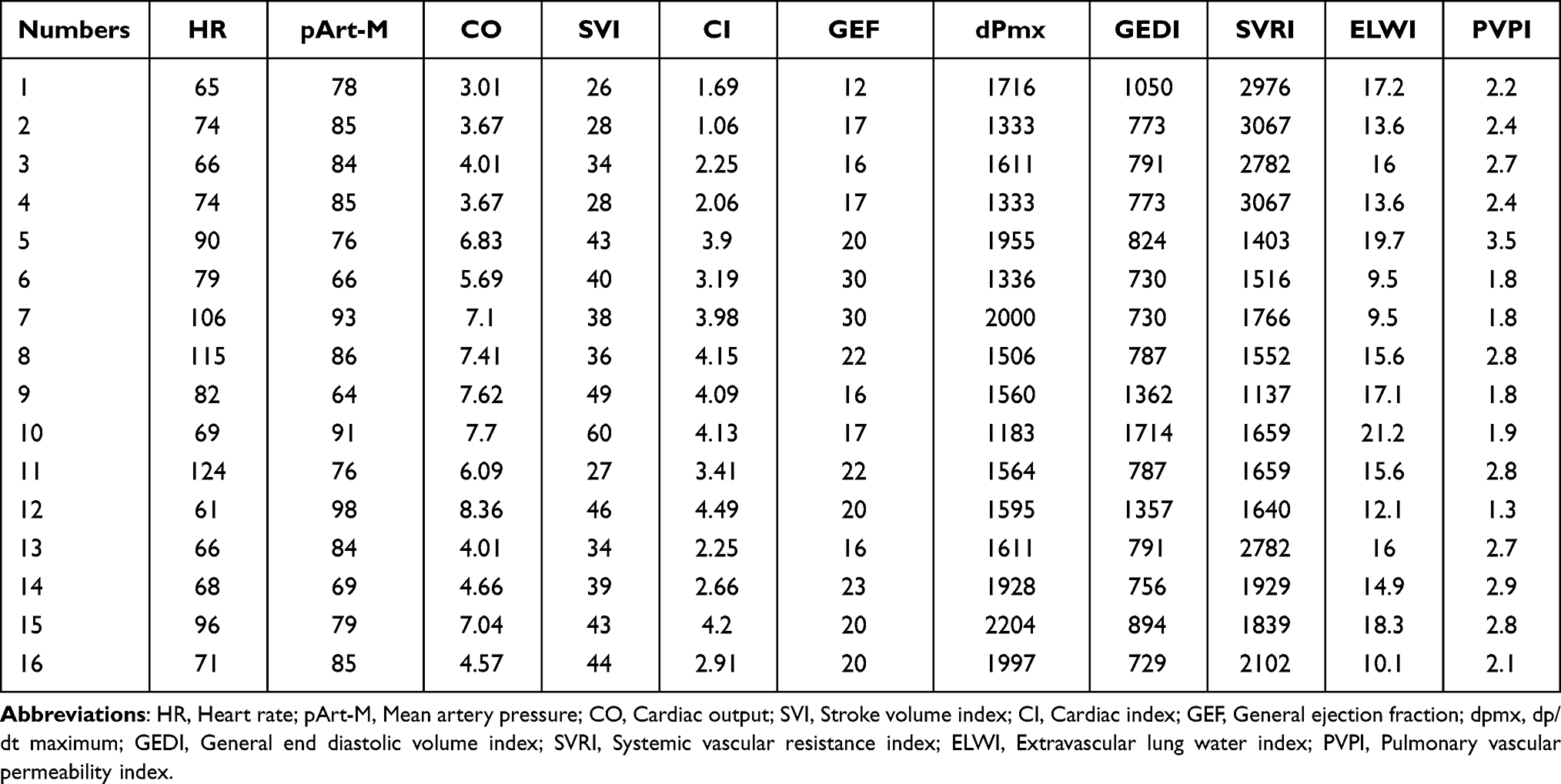 |
Table 3 Parameters Monitored by PiCCO When Hemodynamics Was Unstable |
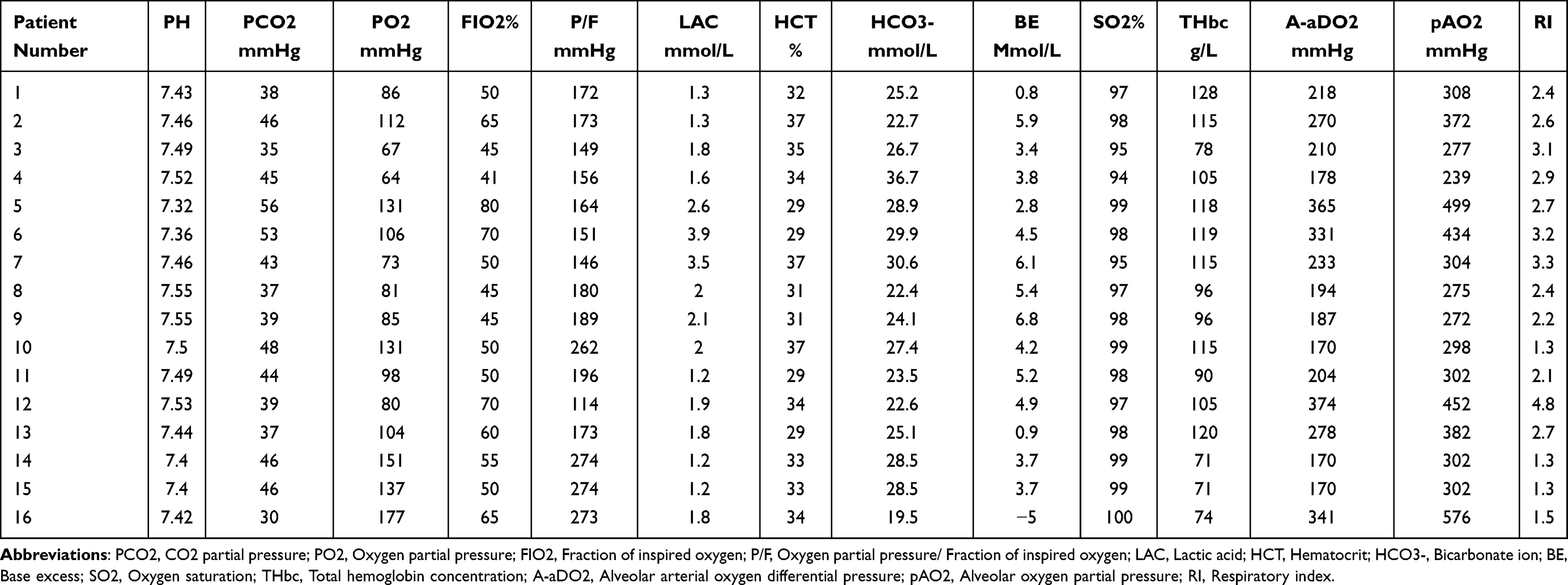 |
Table 4 The Arterial Blood Gas Analyses of Patients by GEM Premier 3500 at Hemodynamics Unstable |
Pearson correlation analysis was used to analyze the relationship between all variables. cTNI was significantly related to BNP at hemodynamic instability (r=0.662, p=0.005). GEF was related to ELWI (r=−0.572, p=0.021) and LAC (r=0.692, p=0.003). ELWI was affected by LVEF (r=−0.564, p=0.023), LVDF (r=−0.734, p=0.001) and PVPI (r=−0.524, p=0.037). For related analysis of other parameters, see the Supplementary Materials.
Discussion
In this study, we conducted continuous observations of 376 critically ill patients. Eighty-seven of the 376 (23.1%) patients developed myocardial injury after admission, 16 of those 87 (18.4%) patients developed circulatory failure and required the use of vasoactive drugs, and 3 patients also received ECMO due to cardiopulmonary failure. At the same time, we also used bedside ultrasound and PiCCO2 to evaluate the hemodynamics of the patients. We found that the patient’s EVLWI was significantly increased.
ELWI is one of the indicators reflecting the severity of extravascular lung water in patients with severe sepsis, which is closely related to the prognosis of patients. The factors affecting EVLWI are pulmonary and cardiogenic. Early autopsy studies found that in patients with severe COVID-19-related pneumonia, the alveolar capillaries were congested, capillary leakage caused fibrin exudation and fibrin precipitation to form a transparent membrane, the accumulation of monocytes in the alveolar cavity and the accumulation of squamous metaplasia of lung epithelial cells.9 Pearson correlation analysis showed that ELWI was significantly related to LVEF (r=−0.564, p=0.023), LVDF (r=−0.734, p=0.001) and PVPI (r=−0.524, p=0.037). Metaplastic alveolar epithelial cells may also be one of the sources of EVLWI, which is different from the phenomenon previously observed in patients with severe ARDS.10–12 Whether EVLWI can predict the prognosis of patients with COVID-19-related pneumonia needs to be confirmed through further research. The increase in ELWI was related to the decrease in left ventricular diastolic function or the increase in nonvascular water sources in the lung. The increase in ELWI will inevitably affect gas exchange in the lung, leading to the occurrence of hypoxemia. Blood gas analysis showed that the difference in oxygen partial pressure in the alveolar air and artery increased significantly, indicating the disorder of oxygen diffusion.
Although the heart is not the main organ affected by COVID-19, the incidence of myocardial injury in severe COVID-19-related pneumonia patients is still high, and the mortality rate of patients with myocardial injury is significantly increased.13–15 Viral infectious sepsis can also cause MODS, autopsy-reported9,16 myocardial edema, weight gain and lymphocyte infiltration in the epicardium. Central CMC shows vacuolar degenerative changes without inflammatory cell infiltration.9 Studies have shown that myocardial edema affects myocardial energy metabolism efficiency and impairs the systolic and diastolic function of the heart.17,18 Sepsis myocardial injury caused by bacterial infection also affects myocardial remodeling,18,19 and whether myocardial injury caused by COVID-19 also leads to myocardial remodeling remains to be confirmed by future studies.
In this study, we observed that in most patients with impaired diastolic function, ventricular diastolic dysfunction can compromise the myocardial response to fluid load by increasing diastolic filling pressure and wall tension, simultaneously impairing microvascular flow and aggravating myocardial injury. Left ventricular diastolic dysfunction will lead to an increase in pulmonary capillary hydrostatic pressure, which tends to promote an increase in EVLWI. In addition, most of the patients have diseases that may potentially damage ventricular diastolic function, such as hypertension and coronary heart disease.
Therefore, the hemodynamics of COVID-19-related pneumonia are not exactly the same as those of sepsis, and it shows its particularity: (1) Pulmonary capillary permeability is not as high as that of sepsis. Pulmonary interstitial edema is not all water; it also includes changes in alveolar exudate organization and pulmonary interstitial fibrosis, which have been confirmed by autopsy. (2) PiCCO2 monitoring showed that the patient’s cardiac preload and ELWI increased, superimposed on hypoxia-induced pulmonary artery spasm, increased pulmonary artery resistance, and right heart dysfunction was induced, which was consistent with the findings of cardiac ultrasound. Therefore, patients have not lost a large amount of effective circulating blood volume, hence shock cannot be corrected by rehydration. Instead, it may lead to increased pulmonary hydrostatic pressure and extravascular lung water, which further aggravates the symptoms of hypoxia. A recent study compared the difference between ARDS caused by COVID-19 and nonCOVID-19; Shi’s20 study found that the values of EVLWi and PVPI in patients with COVID-19 ARDS increased significantly after the onset of disease, which was consistent with the severe alveolar injury caused by COVID-19, thereby correlating with the results of this study. The difference was that the condition of 16 patients in this study was more serious and GEF decreased significantly.
The current research has the following limitations. First, in this study, patients with myocardial injury were monitored by PiCCO after hemodynamic instability. Whether EVLWI increases after lung injury or when hemodynamic instability occurs after myocardial injury is still uncertain. Second, PiCCO is a very useful method of hemodynamic monitoring, and it is usually used for hemodynamic monitoring of critically ill patients; for patients with severe COVID-19-related pneumonia, if hemodynamic instability does not appear, there is no need to use PiCCO for monitoring, so in noncritically ill patients, whether they have elevated EVLWI is currently unknown. In future studies, we should improve the methods to accurately evaluate the right ventricular function of COVID-19 ARDS patients. More clinical evidence is needed to confirm whether impaired right ventricular function and increased EVLWI can reflect the severity of ARDS in patients with COVID-19?
Conclusions
The hemodynamic status after myocardial injury and cardiogenic shock caused by severe COVID-19-related pneumonia was characterized by cardiac preload and increased EVLWI accompanied by a decline in GEF.
Ethical Approval
The patients or the patients’ next of kin provided written informed consent to participate in this study. The data were anonymized or maintained with confidentiality. The publication of this study is in accordance with the Declaration of Helsinki. Ethical review and approval were not required for the observational study on human participants in accordance with the local legislation and institutional requirements by the National Health Commission of China and Ethics Commission of Union Hospital in Wuhan. The study is exempt from institutional review board approval.
Acknowledgments
We gratefully acknowledge all the health care workers on the front line of the West campus of Union Hospital, Huazhong University of Science and Technology, the First Affiliated Hospital of Sun Yat-sen University, and all the patients involved in the study. This study was supported by funding from the Shenzhen Science and Technology R&D Fund (Grant No. JCYJ20160608142215491) and Guangdong Province Basic and Applied Basic Research Fund Project (Grant No. 2020A1515010120 and 2020A1515110919). The funders had no role in the study design, data collection, analysis, decision to publish, or the preparation of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
2. Wang L, He W, Yu X, et al. Coronavirus disease 2019 in elderly patients: characteristics and prognostic factors based on 4-week follow-up. J Infect. 2020;80(6):639–645. doi:10.1016/j.jinf.2020.03.019
3. Zheng YY, Ma YT, Zhang JY, Xie X. COVID-19 and the cardiovascular system. Nat Rev Cardiol. 2020;17(5):259–260. doi:10.1038/s41569-020-0360-5
4. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
5. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 Novel Coronavirus-infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
6. Michard F, Alaya S, Zarka V, Bahloul M, Richard C, Teboul JL. Global end-diastolic volume as an indicator of cardiac preload in patients with septic shock. Chest. 2003;124:1900–1908. doi:10.1378/chest.124.5.1900
7. Hofer CK, Furrer L, Matter-Ensner S, et al. Volumetric preload measurement by thermodilution: a comparison with transoesophageal echocardiography. Br J Anaesth. 2005;94:748–755. doi:10.1093/bja/aei123
8. Redfield MM, Jacobsen SJ, Burnett JC, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289(2):194–202. doi:10.1001/jama.289.2.194
9. Buja LM, Wolf DA, Zhao B, et al. The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities. Cardiovasc Pathol. 2020;48:107233. doi:10.1016/j.carpath.2020.107233
10. Pan P, Su LX, Zhou X, Long Y, Liu DW, Wang XT. Critical hemodynamic therapy oriented resuscitation helping reduce lung water production and improve survival. Chin Med J (Engl). 2019;132(10):1139–1146. doi:10.1097/CM9.0000000000000205
11. Boussat S, Jacques T, Levy B, et al. Intravascular volume monitoring and extravascular lung water in septic patients with pulmonary edema. Intensive Care Med. 2002;28(6):712–718. doi:10.1007/s00134-002-1286-6
12. Díaz-Rubia L, Ramos-Sáez S, Vázquez-Guillamet R, et al. Efficacy of an extravascular lung water-driven negative fluid balance protocol. Med Intensiva. 2015;39(6):345–351. doi:10.1016/j.medin.2014.07.008
13. Chen Q, Xu L, Zhu W, Ge J. Cardiovascular manifestations in severe and critical patients with COVID-19. Clin Cardiol. 2020;43(10):1054. doi:10.1002/clc.23422
14. Metkus TS, Sokoll LJ, Barth AS, et al. Myocardial injury in severe COVID-19 compared with non-COVID-19 acute respiratory distress syndrome. Circulation. 2021;143(6):553–565. doi:10.1161/CIRCULATIONAHA.120.050543
15. Puntmann VO, Carerj ML, Wieters I, et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from Coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(11):1265–1273. doi:10.1001/jamacardio.2020.3557
16. Fujioka M, Suzuki K, Iwashita Y, et al. Influenza-associated septic shock accompanied by septic cardiomyopathy that developed in summer and mimicked fulminant myocarditis. Acute Med Surg. 2019;6(2):192–196. doi:10.1002/ams2.394
17. Dongaonkar RM, Stewart RH, Geissler HJ, Laine GA. Myocardial microvascular permeability, interstitial oedema, and compromised cardiac function. Cardiovasc Res. 2010;87(2):331–339. doi:10.1093/cvr/cvq145
18. Desai KV, Laine GA, Stewart RH, et al. Mechanics of the left ventricular myocardial interstitium: effects of acute and chronic myocardial edema. Am J Physiol Heart Circ Physiol. 2008;294(6):H2428–34. doi:10.1152/ajpheart.00860.2007
19. Martin L, Derwall M, Al Zoubi S, et al. The septic heart: current understanding of molecular mechanisms and clinical implications. Chest. 2019;155(2):427–437. doi:10.1016/j.chest.2018.08.1037
20. Shi R, Lai C, Teboul JL, et al. COVID-19 ARDS is characterized by higher extravascular lung water than non-COVID-19 ARDS: the PiCCOVID study. Crit Care. 2021;25:186. doi:10.1186/s13054-021-03594-6
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.