")
Back to Journals » International Journal of General Medicine » Volume 13
Hematology Reference Intervals for Healthy Adults of the City of Sulaymaniyah, Iraq
Authors Abdullah DA , Mahmood GA, Rahman HS
Received 17 July 2020
Accepted for publication 14 August 2020
Published 25 November 2020 Volume 2020:13 Pages 1249—1254
DOI https://doi.org/10.2147/IJGM.S270800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dana Ahmed Abdullah,1 Gizing Anwar Mahmood,2 Heshu Sulaiman Rahman3,4
1Department of Pathology, College of Medicine, University of Sulaimani, Sulaymaniyah 46001, Republic of Iraq; 2Directorate of Health, Sulaymaniyah 46001, Republic of Iraq; 3Department of Physiology, College of Medicine, University of Sulaimani, Sulaymaniyah 46001, Republic of Iraq; 4Department of Medical Laboratory Sciences, College of Health Sciences, Komar University of Science and Technology, Sarchinar District, Sulaymaniyah 46001, Republic of Iraq
Correspondence: Heshu Sulaiman Rahman
Department of Physiology, College of Medicine, University of Sulaimani, Sulaymaniyah, Republic of Iraq
Tel +964 7726159598
Email [email protected]
Background: Hematology laboratory analyses are essential in the diagnosis of and making decisions on clinical cases. Hematology results are only meaningful when reference made to a normal range of values for a particular population. These values are affected by race, diet, and lifestyle the society.
Objective: To establish the hematological reference values for adult residents of the city of Sulaymaniyah, Iraq.
Methods: Blood samples collected from 1133 healthy males and female volunteers were analyzed for complete blood count, serum iron, and vitamin B12 concentrations. After applying the exclusion criteria, the hematology results from 762 individuals comprising 313 males and 449 males were included in the study.
Results: The mean red blood cell count, hemoglobin concentration, hematocrit, and serum iron concentration were higher in males than females while the neutrophil and platelet counts and plateletcrit were higher in females than males.
Conclusion: This study for the first time recorded hematological reference intervals for residents of the city of Sulaymaniyah.
Keywords: hematology, serum iron, vitamin B12, reference interval, city of Sulaymaniyah
Introduction
The normal ranges for blood parameters vary significantly among those reported because of the high diversity in the characteristics of samples within and between populations. Thus, the range of values of the blood cell parameters for the normal and abnormal cases may overlap, making the differentiation of marginal values for the normal and pathological states problematic. Other factors that can produce inconsistencies in the establishment of the range of normal values include nationality, diet, and lifestyle of the individuals providing blood samples. For these reasons, there is no true normal, thus, the terms “normal value” and “normal range” have been replaced by reference values and the reference range, respectively. In diagnostic testing, reference limits are also used to represent data obtained from measurements on the reference population.1
Proper and accurate reference intervals are vitally important for the medical assessment of patients. The reference interval is defined as the interval between 2 values in which 95% of the results for apparently healthy individuals would fall, usually this implies between 2.5 and 97.5 percentiles of the distribution of test results for a reference population. Ideally, each laboratory should establish its databank of reference values that takes account of all variables affecting blood parameters. This is particularly true for diagnostic laboratories were the results of a patient’s test is expressed and interpreted relative to the normal range of values.2
The Clinical and Laboratory Standards Institute (CLSI) recommends that the establishment of a reference interval of a laboratory to be done by testing at least 120 samples from non-diseased individuals for each gender and age group.2 If this is not possible, the laboratory can adopt by transference verified reference intervals established by a different method. If the analyte is tested in the laboratory, it can also adopt another laboratory’s or the manufacturer’s reference interval.3
This study aims to establish the normal hematology reference intervals for residents of the city of Sulaymaniyah, Iraq.
Methods
Study Location
This study conducted between December 2018 and June 2019, recruited 1133 healthy individuals aged 18 to 95 years. All participants provided informed consent to participate in this study from various health, educational, and social centers in the Sulaymaniyah city, Northern Iraq.
Pre-Analytical and Analytical Phases
The pre-analytical and analytical phases of our study were conducted according to the recommendations of the International Federation of Clinical Chemistry Laboratory Medicine (IFCC-LM) and the Clinical and Laboratory Standards Institute (CLSI).2 The study was performed following the Declaration of Helsinki and approved by the College of Medicine, University of Sulaimani, Sulaymaniyah, Iraq with the approval number of COM/UNIVSUL/2018/1140.
Inclusion Criteria
The participants were healthy adults, regardless of ethnicity and religion, of various socioeconomic and professional groups, who were residents of the Sulaymaniyah city.
Exclusions Criteria
Excluded from this study are individuals with any of the following characteristics: pregnant, lactating, smoker, alcoholic, donated blood in the last 6 months, sick with major diseases such as cancer, undergoing chemotherapy, renal disease, hypertension, diabetes mellitus, family history of thalassemia, with skin tattoo, diarrhea in the past 2 weeks, or had been vaccinated in the last 4 weeks. Also exclude from the study were individuals with the following test results: hemoglobin (Hb) concentration <10 g/dL (2.5% of the normal population have Hb concentration lower than this value), white blood cell (WBC) count <3.0 or >12.0 × 109 cells/L, serum iron <50 or >150 µg/dL, erythrocyte sedimentation rate (ESR) >25 mm/hour for male or >35 mm/hour for female, vitamin B12 concentrations <190 pg/mL, and serum iron concentrations <50 µg/dL.
The above exclusion criteria were applied after physical examinations of the participants and performed laboratory tests to exclude these abnormalities.
Blood Sampling
Blood sampling was done according to the CLSI guidelines2 for complete blood count and biochemical analyses to determine serum iron and vitamin B12 concentrations. To avoid the effect of diurnal variations on blood parameters and the effect of physical exercise, sampling was done in the morning between 9:00 am - 12:00 pm. Approximately, 5.0 mL blood sample was withdrawn from the antecubital vein into K3-EDTA or clot activator gel tubes (BD Vacutainer® tubes from Becton, Dickinson, United Kingdom). The blood samples were analyzed on the same day and within 6 hours of collection. All analyses were done at the Sulaymaniyah Public Laboratory, Sulaymaniyah city, Northern Iraq.
Hematological Analysis
Complete blood count (CBC) was performed using the automated hematological analyzer (Orphee Mythic 22 CT– 5Diff, Switzerland) to analyze for red blood cell (RBC) count, hemoglobin (Hb) concentration, hematocrit (Hct), mean cell volume (MCV), mean cell hemoglobin (MCH), mean cell hemoglobin concentration (MCHC), RBC distribution width (RDW), white blood cell (WBC) count, WBC differential count (including neutrophils, eosinophils, basophils, lymphocytes, and monocytes), platelet counts, and plateletcrit (PCT).
Biochemical Analysis
Serum from blood samples in clot activator gel tubes was subject to iron and vitamin B12 estimation using the Elecsys kits (Roche Diagnostics, United Kingdom) and a chemistry analyzer using Cobas e411 and c11chemistry analyzer (Roche Diagnostics Ltd, United Kingdom).
Statistical Analysis
The data were analyzed using IBM SPSS 20.0 (Illinois, Chicago, USA). The studied groups were distributed according to age (18–39 years, 40–59 years, and 60–95 years) for both sexes. The distribution of variables was determined using Kolmogorov–Smirnov test. Quantitative variables were expressed as mean ± standard deviation, and the 2.5th and 97.5th percentiles were used as the limits for the reference intervals. Statistically significant was defined by p < 0.05.
Results
Seven hundred and sixty-two (762) blood samples, comprising of 313 from males and 449 females, were subjected to hematological and biochemical analyses. The results of these analyses are presented in Table 1. The mean age of males was slightly higher than female participants. The mean platelet, neutrophil counts, and PCT were higher in females than males, while the RBC count, Hb concentration, hematocrit, and serum iron concentration were higher in males than females (p=0.001).
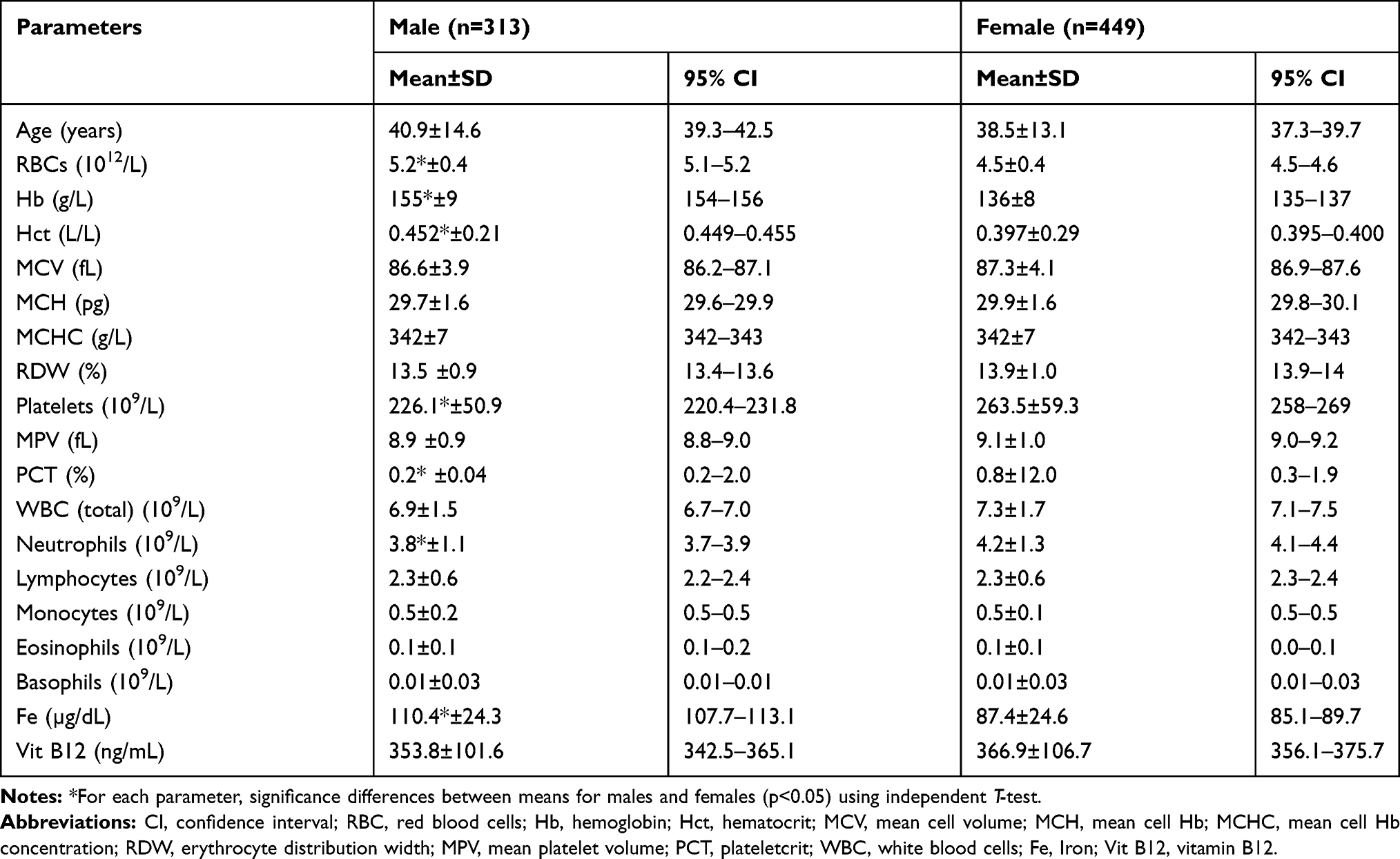 |
Table 1 Reference Intervals for Hematological and Serum Biochemical Parameters for Male and Female Adults |
Data from the male and female cases were divided into 3 different age subgroups (18–39, 40–59, and 60–95 years). Only Hb value was statistically significant (p=0.01) among age groups of males in which it decreased with increasing of age (Table 2). However, this difference was not seen in female age groups (Table 3).
 |
Table 2 Differences in the Reference Intervals Among Adult Males Classified by Age at 2.5 and 97.5 Percentiles |
 |
Table 3 Differences in the Reference Intervals Among Adult Females Classified by Age at 2.5 and 97.5 Percentiles |
Discussion
Complete blood cell count is the most frequently requested laboratory analysis by a clinician for the diagnosis and follow-up of clinical cases.4 The determination of the pathological states of patients is based on the comparison with reference values or reference interval for the normal population.5 The establishments of these reference intervals are dependent on the pre-analytical and analytical methods used to obtain the values. Several inherent factors can cause variability in the values, which include age, sex, weight, environment, race and ethnic origin, biorhythms, pregnancy, nutritional state, lifestyle, medication, and tobacco and alcohol consumption.6 Thus, a set of reference intervals developed by a laboratory in a particular region of the world may not be applicable for use in other laboratories elsewhere.
There is currently no established set of reference values and intervals for hematological parameters that could be used in the diagnosis of illness in patients of the Kurdistan Region of Iraq. The current practice in the region is the use of references established by other laboratories in Western countries, values in brochures provided with diagnostic kits, and reported reference intervals in literature. Since these values are established elsewhere on populations with entirely different characteristics from the Kurds, reference to these values will certainly contribute to inaccuracies in disease diagnosis and clinical decisions.
To establish the reference range for the hematological parameter in our study, we recruited healthy adult males and females from the city of Sulaymaniyah, Kurdistan, Iraq. In this study, males were shown to have higher RBC parameter values than females, while females had higher WBC and platelet counts than males. These findings are similar to those reported in other countries such as Ghana,7,8 Turkey,9 Malaysia,10 China,11 and the United Kingdom.12 It is well known that the differences in RBC values between males and females are primarily due to the influence of the androgenic hormone on erythropoiesis and the menstrual blood loss in females.13
Based on the WBC counts in this study, it appears that females would be more resistant to infection and inflammation than males.14 However, contrary to our findings, studies in Ghana showed no difference in WBC parameters among sexes.7,8 It is expected that because of differences in race, diet, and lifestyle, the range of values will differ among countries as shown by the differences among the Africans, Caucasians, and Caribbeans.15 Even within the same country like the United States of America (USA), white Americans had higher Hct, Hb, MCV, and WBC counts than blacks.16 The Kurds in our study also showed higher mean RBC and platelet parameter values than Africans.14 After excluding contributions from genetic factors, this finding is expected because residents of Kurdistan are less afflicted with nutritional challenges and diseases than many countries of the African continent.
The reference intervals of WBC differential cell counts are identical in males and females except for the absolute neutrophil account which is higher in females than males. This result is consistent with the study conducted in the USA. The reasons for this difference might be attributed to higher non-pathologic or sub-clinical inflammatory states in healthy females than males. Generally, the absolute neutrophil count was significantly lower in the black population than in all of other groups.17
In respect to various age groups; in males, lower Hb, Hct, and platelet count were reported among older age groups compared to younger ages (18–39 vs. 40–59 vs. 60–95). This is mostly contributed to a decline in the hematopoietic activity with the age, which is in agreement with a recently conducted study in Morocco.18 This difference was not observed in the female’s population that might be contributed to the small sample size in our study compared to others.19
This is the first report on the establishment of reference intervals for hematological parameters for residents of the city of Sulaimaniyah, Iraq. The limitation of the study is that the compilation of data is not comprehensive. Other blood parameters should have been analyzed because they are of equal importance and essential blood parameters for disease diagnosis such as serum transferrin saturation (TS), serum ferritin, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). It is suggested the information would serve the medical community better had the study been extended to the whole country on a much large number of samples and all blood parameters relevant for disease diagnosis and prognosis and the determination of the effect of treatments.
Regarding the rest of Iraqi cities, we found some other researchers reported normal reference values, like that done in Hila of Babil about the normal reference ranges in neonatal cord blood.20
Conclusion
This is an initial study in the development of a comprehensive set of blood parameter reference intervals for residents of the city of Sulaymaniyah, Iraq. This study shows, because inherent sex differences, separate reference intervals should be used for males and females in the diagnosis of diseases.
Acknowledgments
The authors would like to appreciate the staff from General Sulaymaniyah Laboratory for their kind help and support as well as the Universiti Putra Malaysia (UPM) to provide publication fee for this research.
Disclosure
All authors of this manuscript declare no conflict of interest in this work.
References
1. Castaneda C, Nalley K, Mannion C, et al. Clinical decision support systems for improving diagnostic accuracy and achieving precision medicine. J Clin Bioinforma. 2015;5(1):4–19. doi:10.1186/s13336-015-0019-3
2. Institute CLS. Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline. Wayne Pennsylvania U, editor; 2008.
3. Gilmour JW, Stevens WS, Gray C, de Souza M. Laboratory expansion to large-scale international HIV preventive vaccine trials. Curr Opin HIV AIDS. 2007;2(3):201–206. doi:10.1097/COH.0b013e3280eec77a
4. Troussard X, Cornet E, Bardet V, et al. Full blood count normal reference values for adults in France. J Clin Pathol. 2014;67(4):341–344. doi:10.1136/jclinpath-2013-201687
5. Zahid H, Meskini T, Yahyaoui A, Hadef R, Messaoudi N. The reference values of the CBC in the adult Moroccan Population a preliminary study in hematology and immunohematology Laboratory at the Rabat Military Hospital, Morocco. Int J Med Health Res. 2017;3(1):1522–1527.
6. Buchanan AM, Muro FJ, Gratz J, et al. Establishment of haematological and immunological reference values for healthy Tanzanian children in Kilimanjaro Region. Trop Med Int Health. 2010;15(9):1011–1021.
7. Dosoo DK, Kayan K, Adu-Gyasi D, et al. Haematological and biochemical reference values for healthy adults in the middle belt of Ghana. PLoS One. 2012;7(4):e36308. doi:10.1371/journal.pone.0036308
8. Addai-Mensah O, Gyamfi D, Duneeh RV, et al. Determination of haematological reference ranges in healthy adults in three regions in Ghana. Biomed Res Int. 2019;2019(2019):1–6. doi:10.1155/2019/7467512
9. Kabasakal E, Ergene Ü, Özlü C. Normal complete blood count reference intervals in the Turkish population: a prospective study. Hematol Transfus Int J. 2018;6(4):135–139. doi:10.15406/htij.2018.06.00169
10. Roshan T, Rosline H, Ahmed S, Rapiaah M, Wan Zaidah A, Khattak M. Hematological reference values of healthy Malaysian population. Int J Lab Hematol. 2009;31(5):505–512. doi:10.1111/j.1751-553X.2008.01068.x
11. Wu X, Zhao M, Pan B, et al. Complete blood count reference intervals for healthy Han Chinese adults. PLoS One. 2015;10(3):e0119669. doi:10.1371/journal.pone.0119669
12. Kelly A, Munan L. Haematologic profile of natural populations: red cell parameters. Br J Haematol. 1977;35(1):153–160.
13. Kueviakoe IM, Segbena AY, Jouault H, Vovor A, Imbert M. Hematological reference values for healthy adults in Togo. ISRN Hematol. 2011;2011:1–5. doi:10.5402/2011/736062
14. Jelkmann W. Regulation of erythropoietin production. J Physiol. 2011;589(6):1251–1258. doi:10.1113/jphysiol.2010.195057
15. Bain BJ. Ethnic and sex differences in the total and differential white cell count and platelet count. J Clin Pathol. 1996;49(8):664–666. doi:10.1136/jcp.49.8.664
16. Beutler E, West C. Hematologic differences between African-Americans and whites: the roles of iron deficiency and α-thalassemia on hemoglobin levels and mean corpuscular volume. Blood. 2005;106(2):740–745. doi:10.1182/blood-2005-02-0713
17. Hsieh MM, Everhart JE, Byrd-Holt DD, Tisdale JF, Rodgers GP. Prevalence of neutropenia in the US population: age, sex, smoking status, and ethnic differences. Ann Intern Med. 2007;146(7):486–492. doi:10.7326/0003-4819-146-7-200704030-00004
18. Bakrim S, Motiaa Y, Benajiba M, Ouarou A, Masrar A. Establishment of the hematology reference intervals in a healthy population of adults in the Northwest of Morocco (Tangier-Tetouan region). Pan Afr Med J. 2018;29(1):1–18. doi:10.11604/pamj.2018.29.169.13042
19. Al-Mawali A, Pinto AD, Al-Busaidi R, Al-Lawati RH, Morsi M, Haeckel R. Comprehensive haematological indices reference intervals for a healthy Omani population: first comprehensive study in Gulf Cooperation Council (GCC) and Middle Eastern countries based on age, gender and ABO blood group comparison. PLoS One. 2018;13(4):e0194497. doi:10.1371/journal.pone.0194497
20. Al-Marzoki JM, Al-Maaroof ZW, Kadhum AH. Determination of reference ranges for full blood count parameters in neonatal cord plasma in Hilla, Babil, Iraq. J Blood Med. 2012;3:113–118. doi:10.2147/JBM.S35895
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.