")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Healthcare Worker Experience and the Challenges in Screening for Intimate Partner Violence Among Women Who Use Antiretroviral Therapy and Other Health Services in Wolaita Zone, Ethiopia: A Phenomenological Study
Authors Meskele M , Khuzwayo N, Taylor M
Received 13 July 2020
Accepted for publication 7 September 2020
Published 30 September 2020 Volume 2020:13 Pages 1047—1059
DOI https://doi.org/10.2147/JMDH.S269940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mengistu Meskele,1,2 Nelisiwe Khuzwayo,3 Myra Taylor1
1School of Nursing and Public Health, Discipline of Public Health, Durban, KwaZulu-Natal, South Africa; 2School of Public Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 3School of Nursing and Public Health, Discipline of Rural Health, University of KwaZulu-Natal, Durban, South Africa
Correspondence: Mengistu Meskele Email [email protected]
Background: Intimate partner violence is a crime against humanity. This study aimed to explore the experiences and challenges in screening for intimate partner violence among women who use antiretroviral therapy and other health services in Wolaita Zone in Ethiopia.
Methods: A descriptive phenomenological qualitative study design was used, and 16 in-depth interviews were conducted with healthcare workers from 19 health facilities who were providing healthcare services in Wolaita Zone. We selected participants purposively until data saturation was reached. Colaizzi’s descriptive phenomenological method was used for the data analysis, and the Open Code software was used to assist with the data coding. We maintained the scientific rigour of credibility, transferability, dependability, and confirmability.
Results: Analysis of the study data identified the following five themes: type of IPV identified by HCWs among women, provider-related barriers, healthcare system barriers, patient-level barriers, and providers’ recommendations for improvements. Issues that emerged from these findings were a gap in medico-legal report provision, absence of a separate record-keeping for IPV cases, lack of client follow-up, absence of routine assessment of violence for women who have injuries, and lack of specific coordination with an external organisation. Moreover, the absence of staff training, weak referral systems, and a shortage of necessary medical equipment challenged IPV screening.
Conclusion: This study has shown that there are healthcare provider and health system challenges relating to screening clients for intimate partner violence in Wolaita Zone. Provision of separate record-keeping of intimate partner violence cases in the healthcare facilities, standardising the medico-legal reporting system, improving women’s access to education, and executing more gender-equitable policies, are needed. Moreover, the inclusion of intimate partner violence-specific policy frameworks in national legislation is necessary.
Keywords: healthcare workers, intimate partner violence, screening, Wolaita Zone
Background
Intimate partner violence (IPV) is a challenging public health problem that affects the health of women in different ways. Intimate partner violence “refers to any behaviour within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship”.1 The World Health Organization (WHO) multi-country study showed that 13–61%; 4–49%; 6–59%; and 20–75% of women reported ever having experienced physical, severe physical, sexual, and emotional violence, respectively.1 The adverse health effects ranged from physical injury, to emotional harm, disability, mental health problems, suicide, and even death.1,2 Intimate partner violence entails different forms of violence that aim at exerting control over an intimate partner. The most visible are injuries sustained from physical assault. However, some victims disguise evidence of these injuries by wearing less revealing clothes or by denying an attack has happened.3
The World Health Organization’s international study shows that in different countries, there are multiple challenges at different levels of the health systems while screening for IPV. Among these difficulties concerning IPV screening, the service providers’ attitudes and their lack of knowledge about IPV were significant challenges. Besides these, non-inclusion of IPV-specific training in the national medical curricula, lack of coordination among various actors, and a lack of departments involved in planning integrated services also affected a country’s response.4 The WHO study stated the importance of the health sectors to ensure the efficient provision of healthcare related services to victims of IPV.4 It also emphasized the vital policies and practices for IPV screening which could aim to integrate responses to violence, into the existing services in low- and middle-income countries.4
Studies have, however, revealed a low rate of IPV screening by healthcare workers (HCWs), ranging from 1.5% to 12% in primary care settings.5,6 The identified challenges of IPV screening by HCWs are lack of provider education on IPV, the shortage of time to screen for IPV, the absence of effective IPV interventions, client reluctance to disclose their experiences of violence, and their fear of the perpetrators.5,6 Similarly, a study conducted in the north-eastern United States showed a low rate of IPV/sexual violence screening at 15%.7 Moreover, a study conducted in Tanzania also showed that lack of adequate resources, ethical dilemmas, staff competency, lack of consultation rooms, and healthcare worker views that IPV screening was a waste of time, were systemic limitations for IPV screening.8
In Ethiopia, more than one in three ever-married women (35%) reported that they had experienced IPV inflicted by their husband or partner at some point in time. This finding showed that the rate of IPV was high in Ethiopia. Intimate partner violence in Ethiopia is, therefore of great concern from the perspectives of economics, health, and human rights.9,10 In a study conducted in East Gojam Zone in Ethiopia, the majority of nurses had not received training on the detection of IPV.11 However, there is limited information concerning healthcare worker experiences of screening for IPV in the country. Therefore, this study aimed to explore healthcare workers’ experience of screening for IPV among the special population group of women living with HIV, using antiretroviral therapy, and accessing other health services in Wolaita Zone in Ethiopia.
Methodology
Study Area and Setting
We conducted the study in Wolaita Zone, which is in southern Ethiopia. Most of the people in this area speak Wolaita, the native language. The total population is 2,473,190, of whom 578,726.46 [23.4% of the total population] are women of reproductive age.12 From the 19 health facilities we included in this study, we recruited a total of 16 HCWs for the interviews. We chose the special population, women living with HIV and following ART. We have noticed that violence leads to HIV infection and we wanted to investigate these experiences; as well as IPV screening among this population groups that were previously not studied in Ethiopia.
Design
The design for this study is a descriptive phenomenological qualitative one. This design helped us to gain the essence of the lived experiences and allowed detailed descriptions of the HCWs’ IPV screening and the barriers that they experienced.13 In descriptive phenomenology, the perception of researchers is set aside or bracketed, to obtain the real experience of the participants.14 In this study, the meaning attributed to the 16 purposively selected HCWs were not influenced by the researchers’ experiences and beliefs.14
Selection of the Study and Sample
We selected the HCWs (medical doctors, nurses, health officers, and midwives) purposively. We interviewed those who were providing healthcare services in the 19 health facilities (both private and government) until saturation of ideas was reached and no new information was presented. In doing this, we conducted 16 in-depth interviews.
Data Collection and Procedures
The data collection for this study took place from October to November 2018. We adapted the interview guides from the World Health Organization’s (WHO) document on researching violence against women15 (Supporting file_section 1). We included the interview guides based on the challenges of HCWs’ IPV screening, the role of HCWs, follow-up care, documentation and medico-legal report provision. The guides included the following questions. What are the most common types of abuse that you identify? Do you or your staff members routinely ask questions to determine if the patient was a victim of family violence? Why? How? What instruments do you use for the examination? How often? What tests or examinations do you routinely perform when a woman indicates that she has been the victim of violence? What are the challenges in screening for abuse? Were you trained to screen for abuse? What types of abuse do you detect? Do women disclose, without being asked, the abuse they experienced? What is the procedure for obtaining an official report from the medical examiner? Do you have a way of keeping records of cases? Is there a form and procedure for recording them? Do you or your staff provide follow-up care to women who have been victims of family violence? Are there mechanisms for referring them to other institutions? Do you think the record-keeping system is adequate to identify women affected by family violence, refer them to the appropriate services, and provide timely follow-up services?
The principal investigator conducted face-to-face, in-depth interviews by using the local languages of the HCWs, Wolaita and Amharic. During the meetings, the investigator probed to get further clarity from the participants. Two experienced research assistants supported the principal investigator with note-taking and digital recordings during the interviews. To maintain the privacy of the healthcare workers, we conducted in-depth discussions at the participants’ offices or their preferred venue.
Trustworthiness
We maintained the scientific rigour and trustworthiness of the data collection based on five criteria16 Credibility: To ensure that the study reflected the participants’ views, the principal investigator spent time in the field and collected the data from the healthcare workers. The results’ section provides verbatim quotes to document the participants’ perspectives, and we undertook peer debriefing after each of the interviews. Transferability: We provided thick descriptions to allow readers to determine whether or not the findings were transferable to their context. Dependability: The research team conducted an audit trail with the supervisor and co-supervisor to ensure that the analysis was grounded in the data and that the findings would be consistent and stable over time. Confirmability: Applying the audit trail (the primary researcher maintained detailed procedural records of the research process) helped us assess the accuracy of the results and truthfulness of the participants’ perspectives. Reflexivity: The results show that the principal researcher thought about himself and the participants, and continuously recorded, as a way to offset predetermined thinking about the research that might interfere with the data analysis. By doing so, we aimed to prevent our motives, perspectives, experiences, backgrounds and prior hypotheses influencing the data interpretation.
Data Analysis
We used the seven steps set in Colaizzi’s descriptive phenomenological method, which is used in health science research, for the data analysis.17 The steps are 1) Familiarisation (reading all the participants’ data and familiarising oneself with the data); 2) Identifying significant statements (recognising the pertinent statements related to the phenomenon); 3) Formulating meanings (identifying the meanings close to the event with the researchers bracketing their knowledge about the meaning); 4) Clustering themes (clustering the meanings into themes); 5) Developing an exhaustive description (writing complete and inclusive explanations of the phenomena, including all the themes that were developed); 6) Producing the fundamental structure (ensuring that the reports cover the essentials); 7) Seeking verification of the underlying structure (returning the primary structure statements to all the participants for confirmation). We used Open Code software for the data analysis, and we used the Consolidated criteria for Reporting Qualitative research (COREQ) Checklist, for maintaining the quality of data.
Ethical Consideration
Ethical clearance was obtained from the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (BREC Ref No: BE387/18) and from Wolaita Sodo University Institutional Review Board (IRB), Ref No: WSU15/04/147 (12 Sep. 2018). Permission was also obtained from Wolaita Zone Health Department and the respective healthcare facilities. Written, informed consent was received from individual participants. The participant informed consent included the publication of anonymized responses. Permission also was obtained for audio recording, and in cases where the participants refused permission to record, notes were taken instead, and the results were incorporated into the other data. Each interview took 50 minutes, and before beginning, the purpose of the research was communicated. This study maintained the confidentiality and privacy of the participants. To this end, they were conducted at the participant’s offices, and nothing was written on any part of the results that could reveal their identities. It was the participant’s right to interrupt or withdraw their participation at any time without penalty or loss of benefits, but this did not occur.
Results
Overall, we conducted a total of 16 in-depth interviews among HCWs with different educational backgrounds. Six (37.5%) were females, while the other 10 (62.5%) were males. Healthcare workers involved in this study were aged between 24 and 42 years. They had different roles and responsibilities at their respective healthcare facilities such as ART focal person, emergency department leader, outpatient worker, obstetrics and gynaecology department coordinator, and mother and child health (MCH) clinic workers (Table 1).
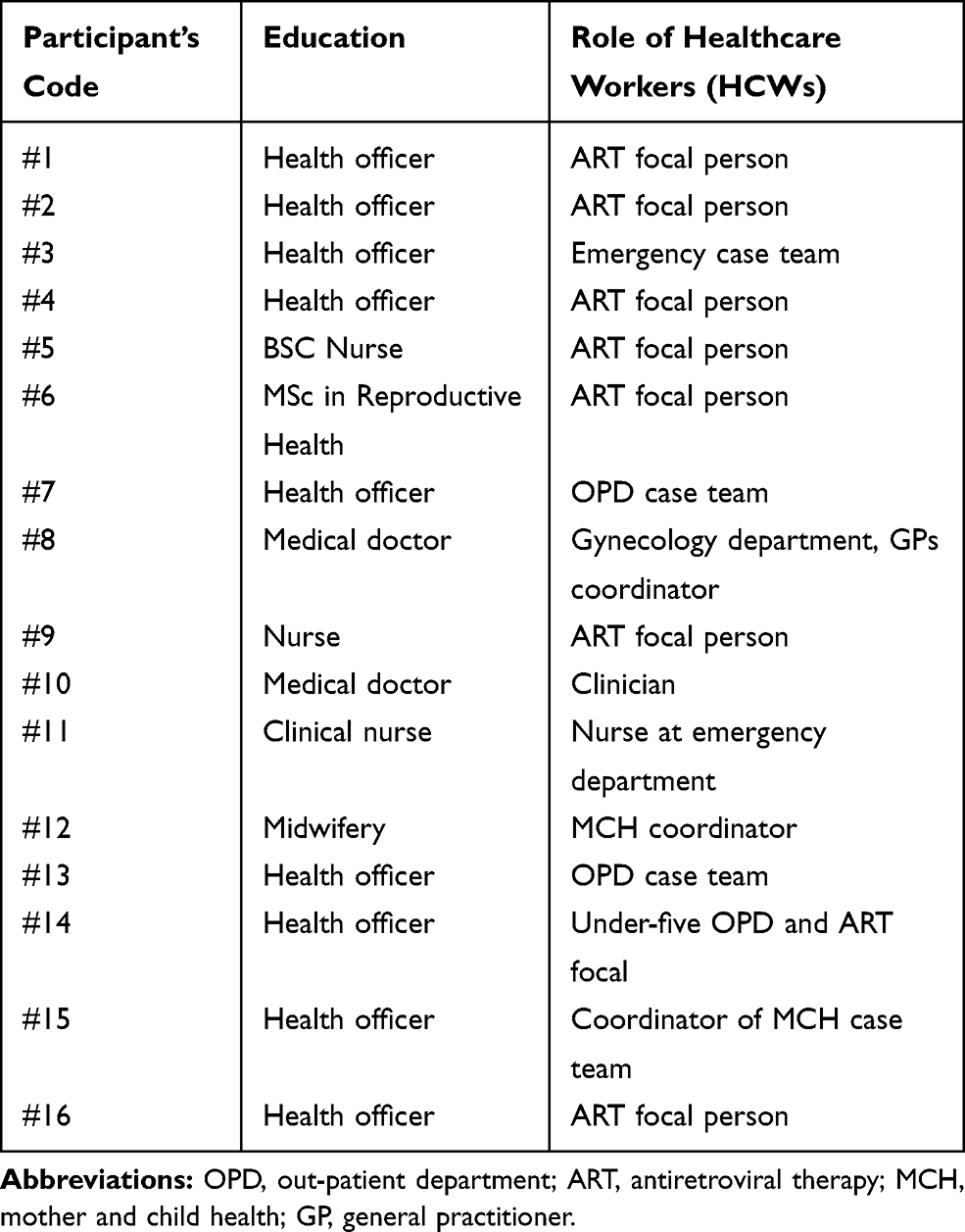 |
Table 1 Socio-Demographic Features of Healthcare Workers in Wolaita Zone in Ethiopia, November–December 2018 |
Themes
Analysis of the study data identified the following five themes: Types of IPV identified by HCWs among women; provider related barriers; healthcare system barriers; patient-level barriers; and providers’ recommendations for improvements (Supporting file_section 2).
Theme 1. Types of IPV Identified by HCWs Among Women
Most HCWs reported that they observed two to three IPV cases per month. However, few healthcare facilities reported more than five to ten IPV cases per month. According to the report from the HCWs, most of the women were visiting their clinic after physical violence trauma, followed by rape. However, they reported that sexual violence victims visited their clinic infrequently. Healthcare workers discussed the reason for fewer incidents of sexual violence being reported to them. They reasoned that this was because the women did not as openly disclose sexual abuse as they did physical abuse.
Healthcare workers reported traumatic experiences of violence that they usually see when screening victims of IPV. These included physical, sexual, and psychological cases of violence. Most HCWs indicated that in mostly, they screen many physical abuse victims and also other victims that experienced traumatic rape. Few health providers reported that instances of violence were uncommon in their facilities.
One of the HCWs Explained
For example, I have seen during my examinations a woman with a head injury, pregnant women who miscarried, and hair follicles removed during a fight. I observed during my physical examination that a man beat his spouse in her birth canal, and I referred her sample [case] to Black Lion Hospital. Usually, women hide such cases. I know a woman who has been suffering from pain for six years due to the violence that she experienced from her husband (HCW, #6)
Another HCW Stated
When I was working in the emergency department, I saw physical violence cases. I also observed a husband who stabbed his wife with a knife. I haven’t seen any other sexual violence cases. I remember a sexual violence case where four people raped the 28-year-old woman. She was unconscious when she visited [was brought to] our clinic. (HCW, #5)
Another HCW Stated
There were women on ART who disappeared from their follow-up. When I searched for the reasons in detail, I identified that most of them were discordant, and they disappeared due to stigma/violent pressure from their partners. (HCW, #6)
Theme 2. Provider Related Barriers
Training
According to the HCWs, most of them had not received on-the-job training on gender-based violence, and it was one of the significant challenges that hindered them in screening cases of abuse. They also highlighted that the lack of training limited them in providing the required quality of care for clients. However, there were very few trained as only one healthcare provider from a private hospital had received training on gender-based violence.
I was not trained and also no one [else is] trained on gender-based violence in this hospital. (HCW, #4)
We did not get training, but there are some staff who were working in the youth-friendly health service who got training. There is also a training manual there. (HCW, #13)
I didn’t train on gender-based violence, but I tend to receive training in gender-based violence. (HCW, #3)
Medico-Legal Issues
Most of the HCWs reported that they offered a medico-legal certificate at the client’s request. However, some of them said that the provision of the medico-legal story of their patient was the responsibility of senior staff, and it was one of the significant challenges for clients to receive it timeously. Moreover, most of the HCWs reported their difficulty in reporting sexual violence after a rape case. The HCWs mentioned various factors that influence screening and provision of the accurate medico-legal report to the victims of IPV. Most healthcare providers explained that rape survivors delay seeking medical help to the degree that on their arrival in the health facility when HCWs conduct a physical examination, they do not find new lacerations or bleeding. The challenge arises when health providers are expected to give a medico-legal report in court.
One of the HCWs Explained This Thus
Sometimes, we may not observe any sign of physical injury, even if they are affected by physical abuse. We have to report it medico-legally, but we couldn’t. Some women who had previous sexual experience come to our clinic and report their rape; however, we couldn’t observe the recent signs of laceration or bleeding of rape. We observe only an old scar, but women report they have no previous sexual experience. It is the biggest challenge when women take the case to court; the report can’t help them. I have seen 18-year-old lady two weeks back who reported a rape case and no previous history of sexual experience. During the physical examination, I observed that the hymen did not tear recently, and I saw an old scar. I haven’t even written her report. She denies it, and the examination report is different from her report. Both physical and sexual violence cases are difficult to report. (HCW, #8)
Another HCW Explained Thus
Since the issue is medico-legal, it puts pressure on the care providers. The victims ask you to over-report while their counterparts ask to under-report the level of damage. (HCW, #10)
Disclosure of physical violence, but not on sexual abuse was explained by another HCW thus:
Yes, women disclose physical violence cases, but they don’t disclose sexual violence cases, but we probe them. (HCW, #11)
Theme 3. Healthcare System Barriers
According to healthcare workers, there are many health system-related problems in testing for IPV. Among these, HCWs reported that there was no separate record-keeping, nor were there registration mechanisms for IPV cases, IPV specific referral systems, or follow-up care for IPV victims. A few HCWs also reported that there was a shortage of medical equipment such as HIV kits, pregnancy kits, ultrasound, and x-ray machines to diagnose IPV. Moreover, HCWs explained that there was no collaboration with external organisations established to prevent IPV cases. Furthermore, HCWs also reported that there was a gap in providing medico-legal reports timeously for their clients. Besides this, HCWs confirmed that it is challenging to do follow-up and routine assessments of IPV clients, because of poor record-keeping.
Follow-Up
HCWs reported that they did not follow up on their clients who were victims of IPV. Moreover, they were not routinely asking questions of patients who were victims of family violence.
One of the HCWs Explained
No follow-up for the IPV affected clients. I do not know if there exists any registration book. Since emergency surgeons manage cases, they know about it. I don’t know whether they have a follow-up or not. (HCW, #3)
There is a shortage of material/equipment. For example, there is a shortage of HIV test kits as well as pregnancy test kits. Also, there was a shortage of equipment for haemoglobin and haematocrit tests. We usually refer such cases due to the shortage of such equipment. (HCW, #12)
Record-Keeping
Healthcare workers also mentioned that there was a gap in the issuing of medico-legal certificates to their clients. The scenario was explained thus:
Only senior physicians write a medico-legal report, and a formal letter with an institutional stamp in a sealed envelope will be sent directly to the requesting legal body, whether to the police or justice office. There is a gap in providing timely medical reports. (HCW, #10)
A Healthcare Provider Also Explained
We don’t have a separate register for violence. We manage them as any other case. I don’t think that the record-keeping is adequate because there is no one trained on gender-based violence, and we do not start to give sufficient services. Also, we don’t have ultrasound and x-ray [machines]. We consider a case as a violence case based on the client’s report, and there is no other device to detect the violence case. (HCW, #7)
There is no form for keeping records of violence cases separately. I don’t think that the record-keeping system is adequate. It is [would be] good if there is [was] a separate registration book. We don’t do screening routinely of the women who are the victims of family violence. I routinely ask them when they come in for their monthly follow-up. (HCW, #2)
We don’t register it separately; rather, we register it as a trauma case in the Health Management Information System (HMIS). (HCW, #4)
Lack of Inter-Sectoral Support
No organisation or person is working on partner violence except the women’s and children’s affairs office. The women’s and children’s affairs office did not come to me, and I did not go to them. (HCW, #2)
There are no organizations specifically working in gender-based violence. Also, many non-governmental organizations are working in other health programs, but not specifically on gender-based violence. (HCW, #15)
Theme 4. Client-Level Barriers
HCWs reported that disclosure related problems, inequality of power between women and men, female beliefs concerning male rights to abuse women, and fear and stigma were patient level barriers to screen IPV. Most of the HCWs reported that women do not disclose their history of abuse unless they are asked by the HCWs. They explained that women were trying to hide their violence experiences because they feared the social challenges. Moreover, they reported that this situation affected HIV-positive women’s adherence to medication, its discontinuation, and family intrigue among all the women. Healthcare workers also said that women’s absence of income limits their disclosure and decisions about an exit plan. This is because they fear that a husband could withdraw his wife’s financial support if he heard about her complaint. Similarly, they reported that there is male dominance in Wolaita society. The same action was feared if husbands became aware of their wives’ disclosure to others about the abuse they experienced. The participant expressed this issue in this way:
One of the challenges is that women who faced sexual violence or rapes do not report their case appropriately due to fear and cultural sensitivity. It makes the screening of sexual violence difficult even though it exists. (HCW, #2)
HIV Disclosure
Mostly in our clinic, women do not disclose due to the fear of the consequence of disclosure. Some women do not have an income, and they fear that if they divorce, they have no place else to go. (HCW, #6)
Most of the time, women don’t disclose their cases without being asked. They have a fear of social stigma. They also fear the confidentiality of their status. (HCW, #9)
One of the HCWs Also Mentioned That
Most men hide their test result from their spouse. They take ART from other health facilities or us, and they don’t want to bring their wives. Some women have a fear of disclosing their status to their husbands. I usually appoint them to bring their husbands, and we screen them together. Then we inform [them of] their test results together. It is to safeguard their marriage. (HCW, #2)
Culture Promoting Male Superiority
Most of the HCWs explained that there is inequality between men and women. They said that women hide reports regarding their issue of violence to male HCWs because of the fear of male dominance. Healthcare workers also reported that husbands’ violent behaviour occurred after consuming alcohol and from having multiple sexual partners. Moreover, they said that women had no decision-making power.
One of the HCWs Explained Further
Since most women live under the influence of men, they don’t tell us. Usually, men have more than one partner, and they treat one of the women in a better way, but they mistreat the other woman. There is violence, but they don’t tell us. I have seen a case where both the husband and wife came after fighting. (HCW, #3)
Healthcare workers explained that women believed that a man has a natural right to abuse women, to insult them and force sex. Hence, they hide their abuse; this made the screening process very difficult for healthcare workers, who believe that to avert this mindset, awareness creation is needed.
One of the HCWs Explained Thus
In our community, it is believed that men are above women in marriage. Some men exploit women financially; however, they did not consider it as violence. Forcing women for sex without their consent is not believed to be violence. Insulting wives is also not considered as violence. There is a saying: ‘If a man does not insult and beat women, he is not a man.’ Women also consider this as men’s natural behaviour. (HCW, #3)
Women don’t think that they are equal to men; they always believe in male dominance and give priority to males. Females don’t feel that they are equal to men in any matters like decision making. Therefore, training on gender equality should be given in all circumstances. (HCW, #16)
Theme 5: Provider Recommendations for Improvements
Most of the HCWs mentioned different IPV prevention strategies. Among these was a need for improved legal, community, and spiritual support for the violence victims and involving males in programs of violence prevention. They reported the need for collaboration with other stakeholders in the violence prevention programs, capacity building of staff through in-service training, the importance of treating clients with respect and dignity, the need for a separate unit or clinic to treat gender-based violence victims together, and improving the equality of women and men through women’s empowerment. Most of the HCWs also mentioned awareness creation, and that efforts to establish the economic independence of women should be aggressively made.
Women’s Empowerment
For me, the most important intervention is empowering women. The government should empower women in every aspect. The concerned bodies should educate women to the level of men, and the economic and social gap between men and women should be minimized. (HCW, #1)
HCWs suggested that in cases where women do not know how to get help from legal, local, and religious leaders, the HCWs should be able to guide women in that regard. Moreover, HCWs reported that consulting seniors, and linking the victims with local and religious leaders might help resolve the conflicts.
Community and Partner Participation
When they report physical violence, we assess the level of damage, and if the problem is significant, we consult our seniors. If she decides to take the case to court, community elders, or to the church and women do not know the process; we guide them. (HCW, #2)
Most HCWs highlighted the importance of the participation of husbands and wives together in education programs aimed at violence prevention. Moreover, they emphasized that special education programs should be established for male partners to tackle their violent behaviours, such as excessive alcohol drinking and extra-marital sexual relationships, which lead couples into conflicts.
I believe that education should be given for husband and wife together on the roles and responsibilities of both. The responsibility of women is so heavy, and husbands don’t think that they have the responsibility of raising their children and preparing food. They should be advised how to support their wives in all activities as well as in sharing responsibility. (HCW, #2)
The study participants explained that collaboration with different stakeholders, for instance, legal services, schools and health facilities, is essential. Additionally, they highlighted the importance of educating men, ensuring proper documentation and reporting of violence cases, and aggressively improving the referral systems. One of the participants stated:
The health facilities should work with legal services, schools, and others. If we integrate the work, we can be effective. We should also educate men and make them responsible. We usually focus on women, and we neglect men in different areas. Gender-based violence education should be implemented independently in schools and other institutions. Reporting, documentation, and referral systems should be strengthened. (HCW, #3)
Role of HCWs
According to the participants, HCWs provide care and respect for the victims of violence and treat these clients compassionately. As most HCWs reported, routine assessment of IPV with women with injuries from violence, counselling of both women and men together and respectfully approaching clients, was an excellent strategy for treating clients. Besides this, addressing the IPV problem, and support and advice from the case manager and adherence counsellor should be beneficial to prevent marriage dissolution and violence. One of the participants was of the opinion
It is better if HCWs provide compassionate care. It depends on the behaviour of individuals. No matter how good the healthcare worker, if he/she does not respect the clients, the clients are not willing to disclose their violence experience. Therefore, there should be rapport/good relations between the two. (HCW, #14)
HCWs should see violence cases as if it happened to them. They should give the victim good care and ease their psychological feelings. If we mistreat them, they may not come to us because of our behaviour. (HCW, #3)
It is good if we educate young girls about violence, at school. We can also give education to local media. Fliers can also transmit a lot of information. (HCW, #8)
A few HCWs mentioned the need for special legislation and policy to treat IPV cases in separate clinics, at the given health facilities. They also pointed out that the economic gap between women and men should be minimized, and that there is a need for decentralizing the programs to all facilities, and mainstreaming IPV prevention into schools and other social spaces. Moreover, they highlighted the need for particular prevention strategies such as community-based interventions, a focal person at health facilities for IPV, the establishment of clubs working on IPV, and home-to-home visits and follow-up education through health extension workers.
The government has a poor focus on violence cases, and it is good if they form a special unit for better follow-up, reporting, and psychiatric or psychosocial management. For example, TB and HIV have a separate system, and it is good if violence has a similar separate unit with trained healthcare workers. It is also good to have a reporting and recording system. (HCW, #8)
Discussion
This research identified IPV screening challenges at the different levels of the health system, and from the perspectives of HCWs and their clients. The current study also proposed different prevention strategies. The findings in Wolaita Zone confirmed the results of the WHO and other studies.2,5,6 However, the significant results that emerged from the current study were about the delays in medico-legal reporting for the victims, the absence of separate record-keeping for IPV cases, the absence of referral systems for IPV victims, and a lack of follow-up care for IPV-affected women.
Types of IPV
As far as the types of IPV identified by HCWs are concerned, physical violence trauma was most common, followed by rape. However, HCWs reported that sexual violence cases visited their clinic infrequently. These findings are supported by the WHO global and regional estimates, South African studies and EDHS 2016 reports, confirming the findings that higher numbers of women in Ethiopia (25%) experienced physical violence, while fewer (10%) experienced sexual abuse.18–20 A probable explanation for these findings is that the women did not as openly disclose sexual abuse as they did physical abuse. It may also be due to the women’s fear of blame and shame in speaking of sexual violence issues, whereas this is not the case for physical trauma. The body of literature also revealed that victims do not even report their abuse to friends, the police, and others, because they do not trust others, and do not think the police will help them.1 Therefore, capacity building is needed to equip HCWs to counsel and assess their clients wisely to allow them to disclose the level of their abuse.
Provider Related Barriers and Training
The findings of this study show that there are many healthcare worker-related challenges for screening IPV in Wolaita Zone. The literature revealed that a considerable gap exists in HCW in-service training, and there is an absence of specific education regarding IPV cases.5,21,22 Therefore, we suggest on-the-job training of staff and the establishment of IPV-specific education for HCWs in Wolaita Zone. However, contrary to our findings, earlier studies found another challenge was the attitude of HCWs towards performing IPV screening, which was seen as an unreasonable activity.21 Moreover, the body of literature has shown the lack of provider education regarding IPV, the lack of time, and the lack of effective interventions for IPV cases.5 The WHO report recommended that HCWs should give adequate time to examine IPV cases.23 In the current study, HCWs had not received any training about IPV. Therefore, we suggest that the government of Ethiopia should give due attention to on-the-job training for IPV screening.
Moreover, there is a need for HCWs to be trained to help women to develop a safety plan as the best strategy to prevent violence. Women who have experienced IPV are likely to have fears about their safety, but women may not expect that violence will happen again. HCWs need training to teach their client that IPV is not likely to stop on its own. Violence tends to continue and may become worse. Therefore, assessing and planning for safety is an ongoing process.23
The literature highlighted the need for HCWs to be open-minded, ready to listen to their clients, unhurried, and to respect confidentiality.24 The HCWs in this study, however, did not meet this recommendation of WHO’s IPV prevention strategy.25 Therefore, we suggest that HCWs should give particular emphasis by taking adequate time in screening IPV at all healthcare facilities. Despite all the challenges reported by the HCWs, there has been little information about the clients’ difficulty in obtaining medico-legal reports from their service providers after IPV screening. The lack of IPV patient follow-up is another concern needing attention. The concerned body in the country should provide specialized training for staff and initiate follow-up care for clients; for example, home visits. The victims of IPV may have different requirements from other healthcare patients since they require a response to their emotional needs - they may also be frightened and need reassurance and support. Women may not need physical, but emotional care instead, and they may require this on an ongoing basis.23
Healthcare System Challenges
Concerning health system-related challenges to screening for IPV, the health facilities in Wolaita Zone had several problems, including the absence of separate record-keeping for IPV, the absence of a referral system for IPV, and a lack of follow-up care for IPV victims. Comparable to the results of the current study, a north-eastern United States study also showed that there were health system-related challenges for IPV screening. However, the health system challenges in the present research are different from the United States’ study. In that investigation, there was a limited time for patient visits, absence of a screening strategy in the health system, and clinicians were so busy with other activities that they took no responsibility for IPV screening.26 The discrepancy in these studies could be due to the economic and health system structural differences between the two countries. The findings of a Togo study is similar to the current result since none of the victims had been referred to local organizations to receive appropriate support27 Our study found that there were, in fact, no local organizations to support violence prevention. Furthermore, the body of literature showed that only 15.8% of victims were referred for IPV assistance by HCWs.28 The current study found a shortage of medical equipment, which is in line with research in Tanzania.8 The current study findings also showed that there was no collaboration with external organizations to prevent IPV and that a gap existed in the medico-legal reporting system, match a study in Serbia,21 in which there was a weak support network for screening IPV. This is despite the body of literature in the WHO document revealing a need for immediate referral and the need for resources to treat IPV victims.23 Therefore, Ethiopia has to arrange medico-legal reporting and referral systems for counselling victims in the short term. In addition, establishing external collaboration with stakeholders who work on gender-based violence in the medium term, and ensuring all the necessary medical equipment to screen IPV cases, is required for the longer term.
The women/partner-related challenges in our study revealed that the clients chose not to disclose their history of abuse to the HCWs. This is because women fear the potential social challenge after their disclosure. Similarly, an earlier study revealed that patient non-disclosure of their abuse was one of the IPV screening challenges.5 Another study also revealed that only half of the women disclosed their IPV experience to HCWs.29 The strategy for the non-disclosure is that HCWs should not pressure women, but give them time to decide what they are willing to disclose. When clients disclose their abuse to HCWs, they need to receive emotional counselling and treatment support, and HCWs should also advise women on a strategy to protect themselves from the perpetrators. Disclosure of HIV status appears to place women at increased risk of IPV, and IPV may prevent them from regular attendance to obtain ART. IPV is not the common medical reason women seek health care more than trauma, car accidents and other emergency cases. However, gender-based violence, and particularly physical violence and sexual violence cases do visit the health facilities in Ethiopia. It is one of the prevalent health problems that may affect the health of women negatively. Women may require counselling, trauma care, and other examinations related to their specific cases.
Client Level Concerns and Follow-Up Care
This study suggests the need for the provision of follow-up care and information on the effects of violence on women’s and children’s health, and as was indicated in the literature23 Besides this, our research found that the inequality of power between women and men and women’s mindset in accepting a man’s natural right to abuse women were IPV screening challenges related to the clients. There is a need to change these perceptions in the Wolaita communities. HCWs have a counselling role in this regard, which they should enact during IPV screening at their clinic. The government of Ethiopia should train their HCWs regarding IPV through specific on the job training. There is also a need for a referral system to link clients to more specialized counselling. This finding matches a study in Bangladesh in which attitudes toward wife-beating, and men who believed wife-beating to be acceptable, were risk factors for IPV.2,30 Additionally, the current study is similar to another study in which male dominance, low social and economic status of women, gender inequality, and men having multiple partners were all factors that challenged IPV screening.2,25
Strategies to Prevent IPV
In our study, regarding the proposed interventions and strategies for the prevention of violence, HCWs suggested a number of different prevention strategies. A feasible short-term strategy is addressing the need for spiritual support, and male involvement in the programs of violence prevention. In the medium term, HCWs also suggested that the government should enhance legal services and empowerment of women. These results are supported by an earlier study by the WHO, in which changing laws that discriminate against women, increasing their access to education, implementing more gender-equitable policies, and reducing acceptance of violence were stated as IPV prevention strategies.2,25 The current study also revealed the need for collaboration with other stakeholders, staff training, and treatment of clients with respect. These findings have also been reported previously where the need for collaboration with other stakeholders, advocacy and awareness creation, integration of services, and the use of behavioural change communication for social change, was found to be important.2 For instance, the involvement of the law office in developing IPV-specific laws, the involvement of the health sector in implementing and treating the cases, and involvement of the psychological and social work departments in counselling IPV victims are considered crucial. Specific laws for IPV are not yet developed and in practice in developing countries; however, the findings of this study suggest the need for a separate unit to treat gender-based violence victims. This would be made feasible by allocating the HCWs who are trained to deal with IPV.
Moreover, our study found the need for different documentation of IPV cases in the healthcare management system. A survey in Togo revealed that screening of IPV in healthcare facilities should be systematic.27 This could make it easier to access the available data for implementers and in the intervention of IPV cases. Also suggested by HCWs is the need for resources for IPV prevention. Similarly, the body of literature strongly suggests availing possible resources (crisis centres, helplines, social workers, support groups, legal support, mental health counsellors, and psychologists) in a particular health system, to manage IPV victims.23 Therefore, we suggest that the collaboration and the availability of the various resources mentioned here should tackle IPV.
Furthermore, the HCWs confirmed that IPV is a public health problem that is exacerbated by male dominance in the society, by alcohol consumption, and discordant HIV test results, a finding in line with other literature.23,31 Therefore, a comprehensive strategy to reduce alcohol consumption in Wolaita society is needed.25 Among the specific approaches which may help to curtail alcohol drinking is for men to record in writing reasons to reduce drinking (e.g. for improved health and sleep) and keeping a diary of drinking habits for three to four weeks; in addition, avoiding keeping alcohol in the home, choosing drink-free days, and deciding not to accept peer pressure is also suggested.32
Strengths and Limitations
Our study has the following three strengths. Firstly, we attempted to put our knowledge and personal biases aside. This means that in the descriptive phenomenological design, the meaning of the research findings was not influenced by our belief systems and experiences. This bracketing also supported the validity of interpretation. Secondly, a profound and detailed understanding of IPV screening challenges were identified and illustrated in the results. Thirdly, the HCWs appear to have contributed well to the study in their support and interest, in that they revealed a delay in medico-legal reporting to the victims, an absence of separate record-keeping for IPV cases, and the lack of follow-up care for IPV and the lack of specific laws for gender-based violence prevention.
However, we can also consider a possible limitation of this study. Although we tried to maintain pure bracketing in placing our presumptions aside, it may, in reality, be difficult to ensure complete bracketing and avoid researcher-induced bias entirely. We also cannot generalize the qualitative finding to other settings.
Conclusions
This study has shown that there is healthcare worker, health system, and client-related IPV screening challenges in Wolaita Zone for women who have injuries or conditions that they suspect may be related to IPV. The issues that emerged from the findings are the gap in medico-legal report provision, absence of separate record-keeping for IPV cases, lack of client follow-up, absence of routine assessment of violence victims, and lack of specific coordination with an external organization. Moreover, the absence of staff training, a weak referral system, and shortages of necessary medical equipment were other challenges. In the Wolaita Zone, among the types of IPV, physical violence trauma was the most commonly reported abuse, followed by rape. Therefore, we recommend the need for improvement in separating record-keeping systems in health facilities, explicit provision of the medico-legal report to clients, improving women’s access to education, and executing more gender-equitable policies. Moreover, the need for an active community and religious leader interventions, involving males in programs of violence prevention, creating a network of support with stakeholders, the inclusion of IPV-specific policy frameworks in the national legislation, and compassionate care is imperative. Additionally, further study with more focus on IPV screening challenges in other parts of the country is suggested.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We obtained ethical approval from the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (BREC Ref No: BE387/18) and the Institutional Review Board approval from Wolaita Sodo University under the Ref No: WSU15/04/147 (12 Sep. 2018). Written consent was obtained from individual participants.
Acknowledgments
We thank the University of KwaZulu-Natal (UKZN), South Africa, for the grant they provided to conduct this research. Our gratitude also goes to data collectors, supervisors, and study participants. We also like to thank Dr. Bereket Yakob, former UKZN student, for the provision of books that helped us on the process of developing design and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Authors’ Information
MM is a Ph.D. candidate at the school of Nursing and Public Health, University of KwaZulu-Natal, South Africa.
NK is a lecturer (Ph.D.) in the School of Nursing and Public Health, University of KwaZulu-Natal, South Africa.
MT is an honorary professor in the School of Nursing and Public Health, University of KwaZulu-Natal, South Africa.
Funding
The University of KwaZulu-Natal, College of Health Science, has funded this research.
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. WHO. Understanding intimate partner violence: fact sheet. 2014. [Cited February 01, 2020]. Available from: apps.who.int/iris/bitstream/10665/77432/1/WHO_RHR_12.36_eng.pdf.
2. WHO. Understanding and addressing violence against women. 2012. [Cited April 20, 2020]. Available from: https://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf;jsessionid=98664A6A2E6FFFEEDE092E584616E006?sequence=1.
3. Lopes C, Hons B. Intimate partner violence: a helpful guide to legal and psychosocial support services. S Afr Med J. 2016;106(10):966–968.
4. Colombini M, Susannah Mayhew WC. Health-Sector Responses to Intimate Partner Violence in Low- and Middle-Income Settings: A Review of Current Models, Challenges and Opportunities. WHO; August, 2008:577–656.
5. Waalen J, Goodwin MM, Spitz AM, Petersen R, Saltzman LE. Screening for intimate partner violence by health care providers. Barriers and interventions. Am J Prev Med. 2000;19(4):230–237. doi:10.1016/S0749-3797(00)00229-4
6. Agency for Health care Research and Quality. Intimate Partner Violence Screening: fact Sheet and Resources. April. 2015. [Cited May 02, 2020]. Available from: https://www.ahrq.gov/ncepcr/tools/healthier-pregnancy/fact-sheets/partner-violence.html.
7. Suther Land MA, Hutchinson MK. Intimate partner and sexual violence screening practices of college health care providers. Appl Nurs Res. 2018;39:217–219. doi:10.1016/j.apnr.2017.11.031
8. Laisser RM, Nyström L, Lindmark G, Lugina HI, Emmelin M. Screening of women for intimate partner violence: a pilot intervention at an outpatient department in Tanzania. Glob Health Action. 2011;4(1):7288. doi:10.3402/gha.v4i0.7288
9. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016 [Cited April 24, 2020]. Available from: http://evaw-global-database.unwomen.org/-/media/files/un%20women/vaw/vaw%20survey/1%20ethiopia%20dhs%202016.pdf?vs=4831.
10. Yitbarek K, Woldie M, Abraham G. Time for action: intimate partner violence troubles one-third of Ethiopian women. PLoS One. 2019;14(5):e0216962. doi:10.1371/journal.pone.0216962
11. Zeleke H, Mengistu D, Alem G. Assessment of nurses’ preparedness and identify barriers to care women exposed to intimate partner violence in East Gojjam Zone, Ethiopia, 2014. Nurs Care. 2015;4(250):2167–1168.
12. From Wikipedia, the free encyclopedia. Wolayita zone. [Cited May 2, 2020]. Available from: https://en.wikipedia.org/wiki/Wolayita_Zone#Demographics.
13. Creswell JW. Research Design: Qualitative, Quantitative and Mixed Methods Approach. India: SAGE Publications, Inc.; 2014.
14. Rodriguez A, Smith J. Phenomenology as a healthcare research method. Evid Based Nurs. 2018;21(4). doi:10.1136/eb-2018-102990
15. Ellsberg M, Heise L. Researching Violence Against Women: A Practical Guide for Researchers and Activists. Washington DC, United States: World Health Organization, PATH;2005 [Cited May 2, 2020]. https://apps.who.int/iris/bitstream/handle/10665/42966/9241546476_eng.pdf;jsessionid=B12DC169268A966D579DECAAE9409DC2?sequence=1.
16. Billups F. The quest for rigor in qualitative studies: strategies for institutional researchers. 2014. http://subgroup.co/6a9er/.
17. Morrow R, Rodriguez A, King N. Colaizzi’s descriptive phenomenological method. Psychologist. 2015;28(8):643–644.
18. Central Statistical Agency/CSA/Ethiopia and ICF. Ethiopia Demographic and Health Survey, 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016. [Cited May 24, 2020]: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.
19. WHO. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. WHO. 2013 [Cited April 24, 2020]. Available from: https://www.who.int/reproductivehealth/publications/violence/9789241564625/en/.
20. Bernstein M, Phillips T, Zerbe A, et al. Intimate partner violence experienced by HIV-infected pregnant women in South Africa: a cross-sectional study. BMJ Open. 2016;6(8):e011999. doi:10.1136/bmjopen-2016-011999
21. Djikanovic B, Celik H, Simic S, Matejic B, Cucic V. Health professionals’ perceptions of intimate partner violence against women in Serbia: opportunities and barriers for response improvement. Patient Educ Couns. 2010;80(1):88–93. doi:10.1016/j.pec.2009.09.028
22. Sprague S, Madden K, Simunovic N, et al. Barriers to screening for intimate partner violence. Women's Health. 2012;52(6):587–605.
23. WHO. Health Care for Women Subjected to Intimate Partner Violence or Sexual Violence: A Clinical Handbook. September, 2014.
24. Usta J, Antoun J, Ambuel B, Khawaja M. Involving the health care system in domestic violence: what women want. Ann Fam Med. 2012;10(3):213–220. doi:10.1370/afm.1336
25. WHO. Preventing intimate partner and sexual violence against women Taking action and generating evidence. World Health Organization and London School of Hygiene and Tropical Medicine; 2010 [Cited February 1, 2020]. Available from: https://www.who.int/violence_injury_prevention/publications/violence/9789241564007_eng.pdf.
26. D’Avolio DAJCNR. System issues: challenges to intimate partner violence screening and intervention. Clin Nurs Res. 2011;20(1):64–80.
27. Burgos-Soto J, Orne-Gliemann J, Encrenaz G, et al. Intimate partner sexual and physical violence among women in Togo, West Africa: prevalence, associated factors, and the specific role of HIV infection. Glob Health Action. 2014;7(1):23456. doi:10.3402/gha.v7.23456
28. Ballan MS, Freyer MB, Powledge L. Intimate partner violence among men with disabilities: the role of health care providers. Am J Men's Health. 2017;11(5):1436–1443. doi:10.1177/1557988315606966
29. Morse DS, Lafleur R, Fogarty CT, Mittal M, Cerulli C. “They told me to leave”: how health care providers address intimate partner violence. J Am Board Fam Med. 2012;25(3):333–342. doi:10.3122/jabfm.2012.03.110193
30. Johnson KB, Das MB. Spousal violence in Bangladesh as reported by men: prevalence and risk factors. J Interpers Violence. 2009;24(6):977–995. doi:10.1177/0886260508319368
31. Maeri I, El Ayadi A, Getahun M, et al. “How can I tell?” consequences of HIV status disclosure among couples in eastern African communities in the context of an ongoing HIV “test-and-treat” trial. AIDS Care. 2016;28(Suppl 3):59–66. doi:10.1080/09540121.2016.1168917
32. Harvard Health Publishing. 11 ways to curb your drinking [Internet]. Harvard University. March 14, 2020. Available from: https://www.health.harvard.edu/healthbeat/11-ways-to-curb-your-drinking.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.