")
Back to Journals » International Journal of General Medicine » Volume 15
Healthcare Utilization Disparities Among Lung Cancer Patients in US Hospitals During 2010–2014: Evidence from the US Hispanic Population’s Hospital Charges and Length of Stay
Authors Kim SJ, Medina M , Delgado R, Miller A , Chang J
Received 12 November 2021
Accepted for publication 26 January 2022
Published 9 February 2022 Volume 2022:15 Pages 1329—1339
DOI https://doi.org/10.2147/IJGM.S348159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sun Jung Kim,1– 3,* Mar Medina,4,* Rigoberto Delgado,5 Anastasia Miller,5 Jongwha Chang5
1Department of Health Administration and Management, College of Medical Science, Soonchunhyang University, Asan, Republic of Korea; 2Center for Healthcare Management Science, Soonchunhyang University, Asan, Republic of Korea; 3Department of Software Convergence, Soonchunhyang University, Asan, Republic of Korea; 4School of Pharmacy, University of Texas at El Paso, El Paso, TX, USA; 5Department of Healthcare Administration, College of Business, Texas Woman’s University, Denton, TX, USA
*These authors contributed equally to this work
Correspondence: Jongwha Chang, Tel +1940-898-2899
, Email [email protected]
Purpose: There is a lack of research focused on understanding the differences in the healthcare utilization of lung cancer patients between ethnic groups. This study aims to characterize disparities in healthcare utilization for Hispanic lung cancer patients compared to non-Hispanic patients.
Methods: National Inpatient Sample was used to identify nationwide lung cancer patients (n=141,675, weighted n=702,878) from 2010 to 2014. We examined the characteristics of the study sample by race (Hispanic vs non-Hispanic) and its association with healthcare utilization, measured by discounted hospital charges and length of stay. Multivariate survey regression models were used to identify predictors by racial groups.
Results: Among 702,878 lung cancer patients, 5.1% were Hispanic. Descriptive statistics showed that Hispanics have higher hospital charges and length of stay. Survey regression results also suggested that Hispanic lung cancer patients were associated with higher hospital charges (26.6%) and length of stay (3.5%) than non-Hispanic lung cancer patients. Subgroup analysis displayed a similar trend to the full model.
Conclusion: Healthcare utilization disparities may exist for lung cancer Hispanic patients due to insurance status and early detection. Thus, our findings support providing financial assistance and targeted programs for minority patients. Future health policy consideration should be given to those vulnerable populations where limited healthcare resources are available.
Keywords: lung cancer, Hispanic patients, NIS sample, healthcare utilization
Introduction
Lung cancer remains a leading cause of death in the United States as the second most common cancer.1 In 2018, there were 218,520 new lung cancer cases, and it was the leading cause of cancer death that year.2 That same year, 10,183 lung cancer cases were from Hispanic patients, and 5540 Hispanic patients died.2 Comparatively, there were 23,417 new lung cancer Black patients, 1353 new cases in American Indian and Alaskan natives, and 6590 new cases in Asian and Pacific Islander patients.2 Despite advances in screening, treatment, and tobacco prevention, lung cancer attributed to over 1.8 million worldwide deaths in 2018 and was about 23.5% of all cancer deaths in 2019 in the United States.1 Worldwide, in 2020, there were 2,206,771 new lung cancer cases and 1,796,144 new lung cancer deaths, second in both categories only to female breast cancer.3 Lung cancer also has the highest cancer mortality rate in men worldwide.3 By 2021, the estimated number of new lung cancer cases in the United States will be 12.4% of all cancer cases and contribute to 21.7% of cancer deaths.4
From 2011 to 2017, the 5-year survival rate of lung cancer in the United States was 21.7%, and 34.4% of new cases occurred in patients aged 65–74.5 Notably, most patients are diagnosed at late stages, with 56% of lung cancer cases having already metastasized,5 contributing to sub-par survival rates compared to other cancers.6 Early detection is ideal, but current screening tests have not been effective at catching the early stages of lung cancer.6,7 As a result, patients no longer can undergo surgery or curative treatment at later stages of the disease and are often treated with chemotherapy.8 Significantly, minority patients are more often diagnosed at such late stages, thus decreasing survival rates.9 Such aggressive end-of-life treatment has been known to affect cancer patients’ quality of life with negligible effects on survival improvement.10 More significant research is required to pinpoint lung-cancer patient-specific health needs by race and ethnicity.11
Racial disparities in the United States have affected access to healthcare and lung cancer screening, treatment, and survival rates.9,12 Hispanic patients are less likely to receive cancer treatment for leading cancers in the United States, including lung cancer.11 Further, race and ethnicity have been correlated with differences in socioeconomic status.9,12,13 Low socioeconomic status inhibits healthcare access, screening, and treatment before and during the disease.12 Socioeconomic status affects residence, and a high proportion of Hispanic people live in highly polluted areas – another risk factor for lung cancer.12 Lung cancer remains the leading cause of cancer death in Hispanic men,14 despite advancements in tobacco control.15 Considerable tobacco control has led to a decline in lung cancer-related deaths with greater educational outreach on the risks of nicotine, the legal smoking age, and cancer prevention.15
Lung cancer cost in the United States is estimated at $20.1 billion and is expected to rise by over 30% by 2030 because of an aging population and costly new therapies.16 In 2017, the average monthly cost of terminal lung cancer in the final 6 months of life was $12,987.17 Aggressive end-of-life care has become more prevalent for lung cancer patients, increasing cost.18 While cheaper hospice options have also increased, they are often utilized too late to lower costs.18 Most end-of-life care for cancer patients comes from hospitalizations, and racial minorities are more likely to be cared for in emergency rooms, intensive care units, and inpatient facilities.18 Hispanic patients tend to visit the ER and ICU more and receive more aggressive chemotherapy towards their end of life than non-Hispanic white patients.18
Further, in 2019, the Hispanic population had the most significant percentage of uninsured people at 16.7% compared to 5.2% of non-Hispanic white being uninsured.19 The disparity in insurance coverage for Hispanic patients has limited their access to health and mental health services.20,21 Lack of insurance can drive patients, notably ethnic minorities, to be treated in emergency rooms rather than private offices.22 Further exacerbating the lack of access, Hispanic patients often face language barriers, low education rates, and a lack of providers with similar cultural and ethnic backgrounds.23 In addition, cancer screening is more deficient in minority patients, possibly due to insurance as even Medicaid screening coverage varies by state and does not guarantee lung cancer screening.20
As Medicaid physician fees are cut or frozen, fewer patients visit their doctors, and more Medicaid patients turn to a hospital or emergency room care, which are obligated to treat without regard to insurance status.24 Primary care physicians often do not accept Medicaid patients for various reasons, like decreased reimbursement compared to private insurance.25 Higher Medicaid fees tend to increase the amount of Medicaid patients seen by a primary care physician.26
There is a lack of research focused on understanding the differences in the healthcare utilization of lung cancer patients between ethnic groups. With lung cancer being a leading cause of cancer death in the United States and among Hispanic male patients, it is essential to determine how Hispanic patients are affected by the rising healthcare costs. Such research can pave the way for economic programs targeting low-income minority cancer patients and further highlight the connection between ethnicity, low socioeconomic status, and the burden of cancer. This study aims to characterize disparities in healthcare utilization as measured by discounted hospital charges and length of stay for Hispanic lung cancer patients compared to non-Hispanic patients.
Materials and Methods
Data Collection
The 2010–2014 National Inpatient Sample (NIS) database was used to obtain a population-based estimate for nationwide patients with lung cancer. This was the available dataset in possession when we were conducting this research. Among all 2010–2014 NIS samples (N=37,312,324), as shown in Figure 1, we first identified a primary diagnosis of lung cancer (n=156,180) using the International Classification of Diseases Ninth Revision, Clinical Modification (ICD-9-CM) codes for lung cancer. Then, after patients with missing variables were excluded, we finally obtained patients with lung cancer (n=141,675).
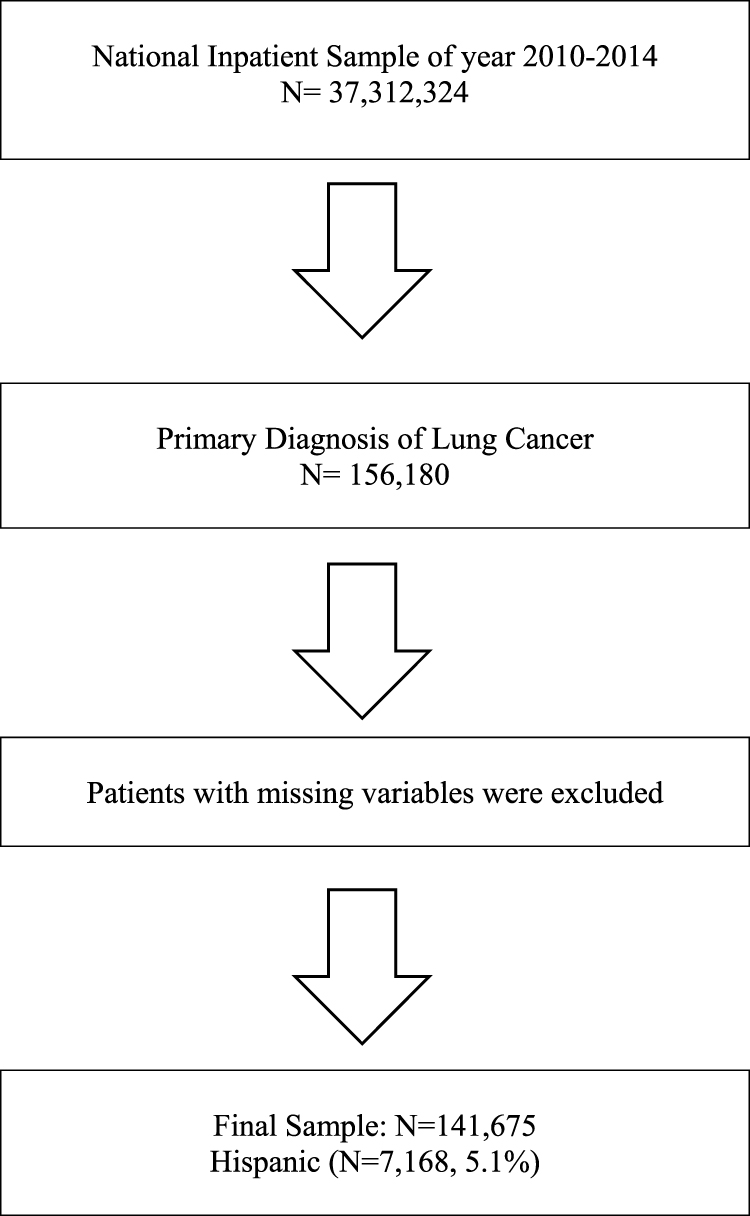 |
Figure 1 Flow chart of patient sample selection. |
Variables
The primary outcome of this study was to investigate the difference in hospital charges and length of stay for Hispanic vs Non-Hispanic patients. Total hospital charges were calculated after adjusting the annual inflation rate using Centers for Medicare and Medicaid Services estimates.27 Due to the skewing of distribution for hospital charges and length of stay, we conducted the natural log of those variables.
We adjusted for various patient-level confounders that other previous researchers used to investigate healthcare utilization using NIS.28–30 Patient characteristics included age, race, annual median household income, primary payer (Medicare, Medicaid, Self-Pay/No Charge, Other, Private insurance), number of comorbidities, the severity of illness using all-patient refined diagnosis-related group (APRDRG-number of coexisting medical conditions that are not directly related to lung cancer), and whether the patient received surgery, radiation, chemotherapy.
Statistical Analysis
To represent all lung cancer patients, sampling weights were applied to all statistical analyses. First, we examined the characteristics of the final dataset, which included patient characteristics by racial groups (Hispanic vs non-Hispanic). Patient characteristics were presented as weighted frequency (percentage) or means (SD). To investigate groups, Rao-Scott Chi-Square tests were used for categorical variables.
Then, we investigated how racial differences were associated with discounted hospital charges and length of stay using multivariate survey linear regression analysis. Finally, we conducted a subgroup analysis where we ran the models multiple times to investigate each subgroup’s association. All subgroup models were performed by adjusting all other variables. All analyses were conducted using SAS statistical software (version 9.4; SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided and statistical significance was determined at p-value <0.05.
Results
Patient Characteristics and Descriptive Statistics
A total 141,675 lung cancer patients were identified in the 2010–2014 NIS data (weighted n=702,878, Table 1). Among them, 7168 (weighted n=35,823, 5.1%) were Hispanic patients. The general characteristics of patient characteristics are presented in Table 1.
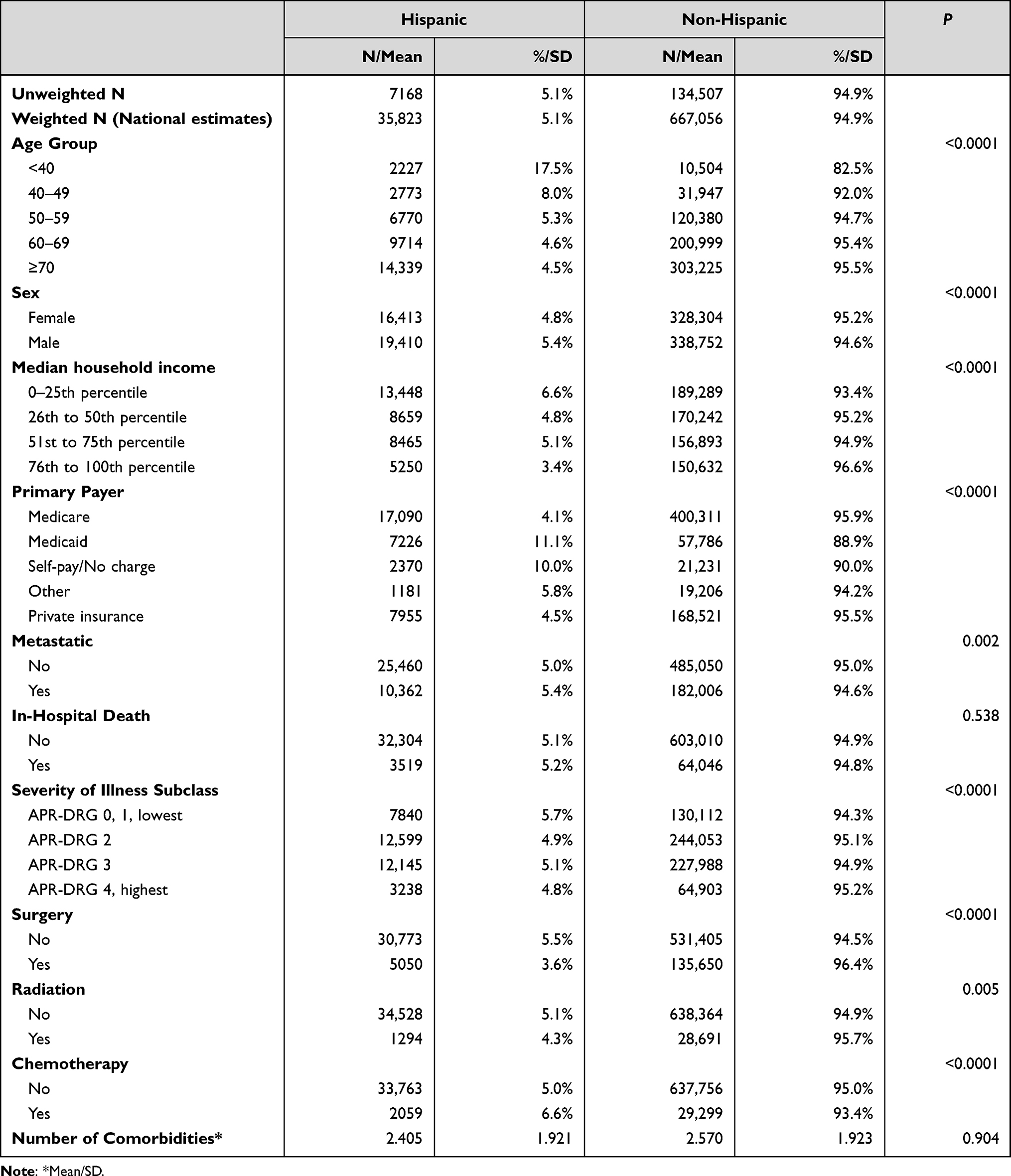 |
Table 1 General Characteristics of Patient Sample |
Table 2 shows different racial groups’ temporal trends of hospital charges and length of stay among lung cancer patients during 2010–2014. Overall mean discounted hospital charges and length of stay were $73,941 and 6.82 days for Hispanic patients and $60,378 and 6.48 days for non-Hispanic patients. Thus, although hospital charges were discounted, hospital charges were somewhat increased in the Hispanic population; however, the length of stay was not volatile during the study period.
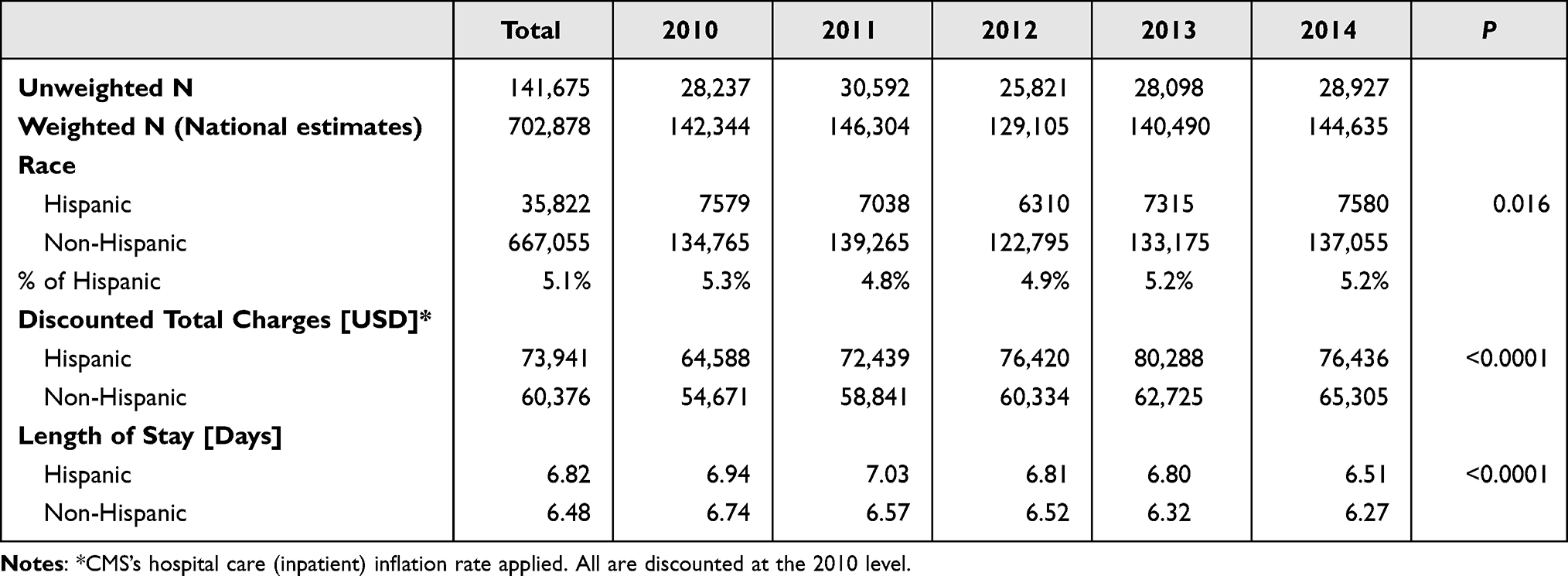 |
Table 2 Temporal Trend of Healthcare Utilization Among Lung Cancer Patients: Hispanic vs Non-Hispanic |
Association of Racial Difference with Hospital Charges and Length of Stay
The associations of racial difference with discounted total hospital charges and LOS from survey logistic regression models are shown in Table 3. After controlling for all other variables, hospitalization of the Hispanic population was associated with a statistically significant increase in hospital charges (β =0.266, p<0.001), which means 26.6% higher discounted total costs than non-Hispanic patients. Furthermore, length of stay was associated with a statistically significant increase (β =0.035, p<0.001) in Hispanic patients, which means 3.5% higher length of stay than non-Hispanic patients.
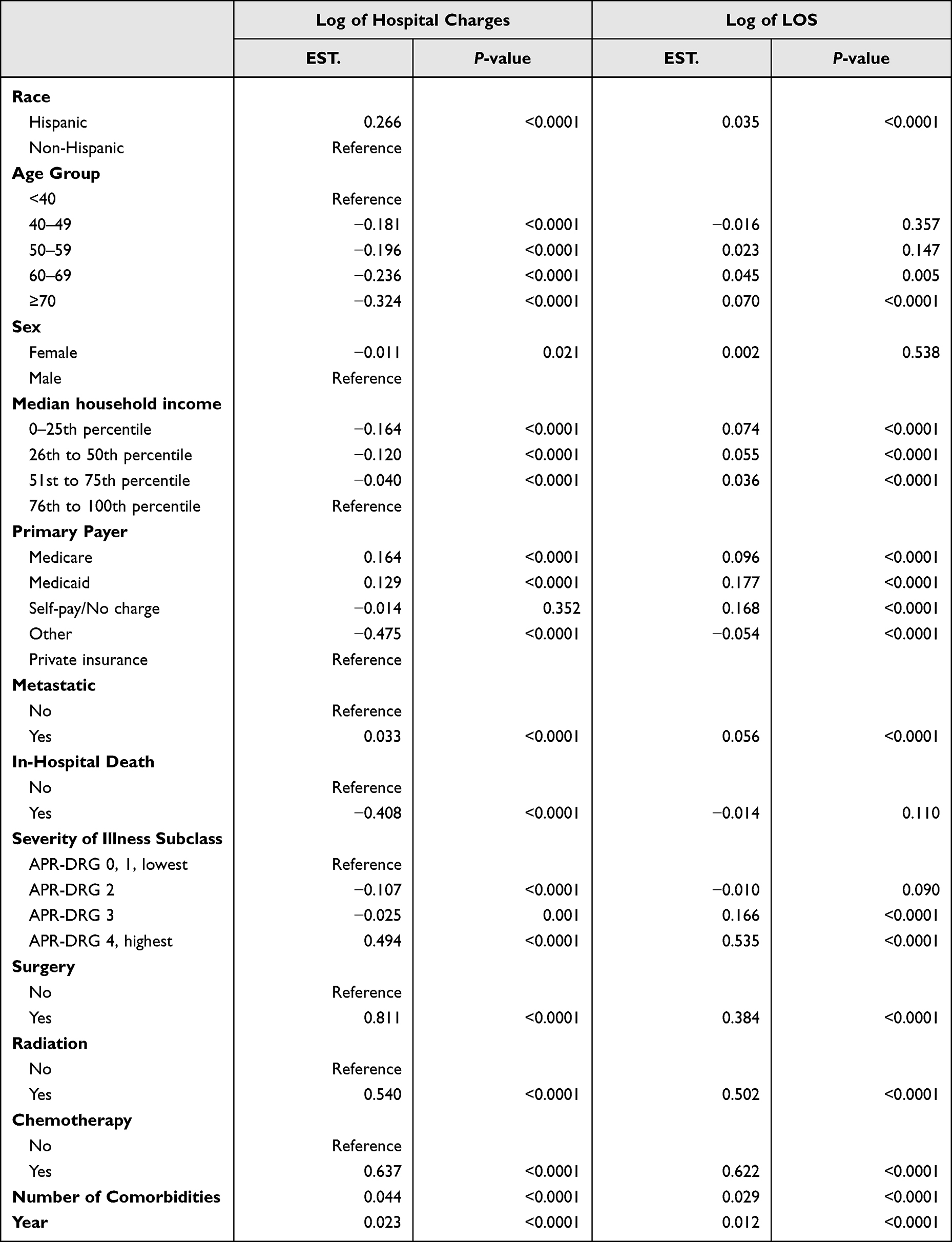 |
Table 3 Results of Survey Regression Models: Log Transformed Hospital Charges and LOS by Racial Groups |
Higher hospital charges were also associated with lower age, male, high income, metastatic stage, surgery, radiation, chemotherapy, etc. Higher length of stay was associated with older age, lower income, metastatic stage, surgery, radiation, and chemotherapy.
Results of Subgroup Analysis
Table 4 shows the association of racial groups with discounted total hospital charges and length of stay for each subgroup in the model. The results in the table are Hispanic patients’ hospital charges and length of visit for each subgroup compared with non-Hispanic patients. Results in the subgroup analysis were aligned with the full model, which we assume higher hospital charges and length of stays were presented in all Hispanic patient groups. Hispanic patients over 40 years old were associated with higher discounted total costs, while longer length of stay was associated with Hispanic patients over 60 years old. This trend carries over all other confounders including sex, income, and payer, as the Hispanic population was associated with higher discounted total charges for all those factors. A few groups did not have statistically significant differences in terms of length of stay, including female, income, and different types of payers. The severity of illness subclass was not statistically significant; however, many subgroups did show a higher length of stay for the Hispanic population.
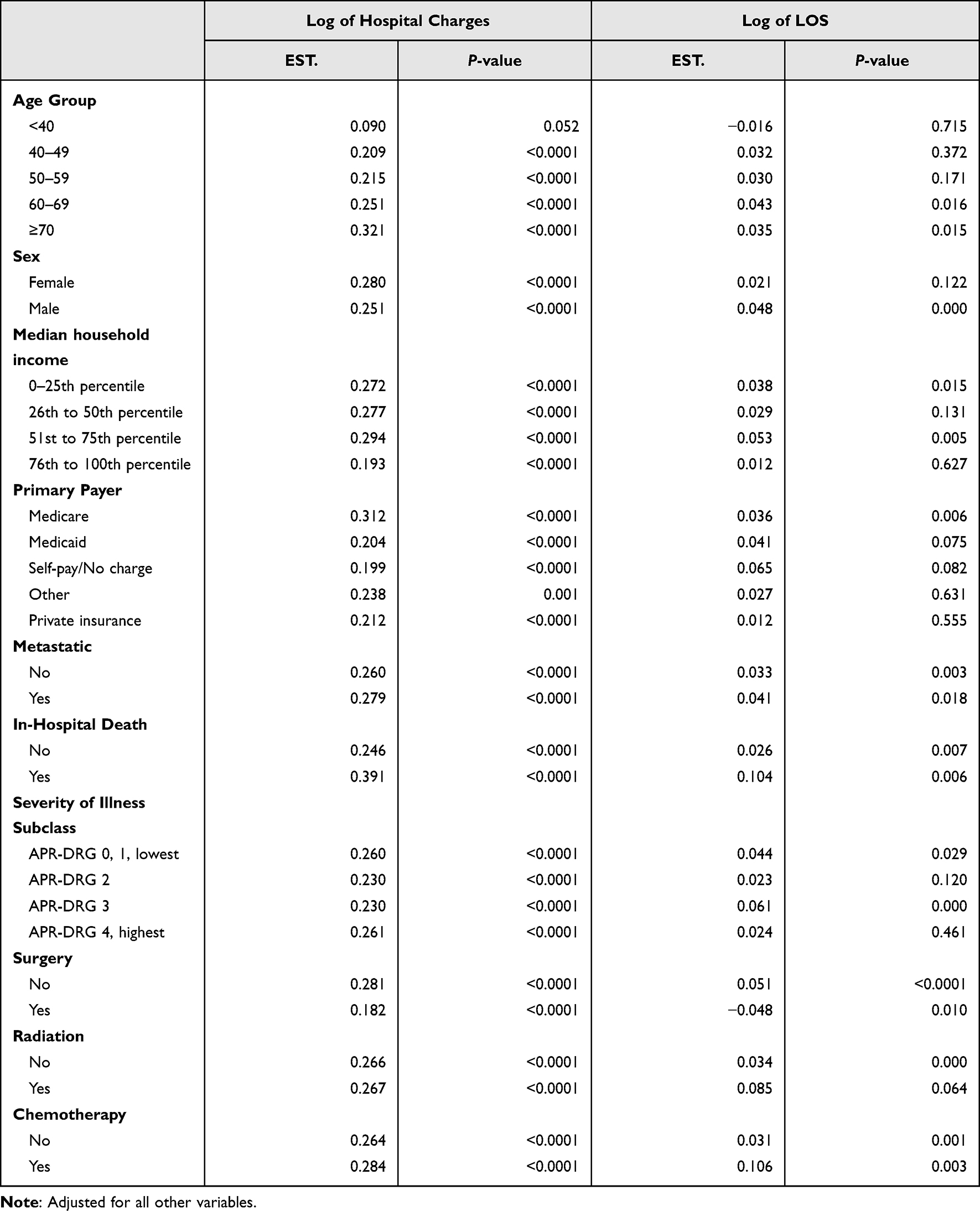 |
Table 4 Results of Subgroup Analysis |
Discussion
When considering the high healthcare utilization of lung cancer, it is essential to characterize how different ethnic groups, like Hispanics, are impacted by the financial burden of this disease. In this study, we have illuminated the disparity felt by Hispanic lung cancer patients in healthcare utilization, represented by their length of hospital stays and hospital charges. Hispanic patients paid between an estimated $10–18,000 more than non-Hispanic patients during the study years. On average, Hispanic patients paid $13,565 more than non-Hispanic patients between 2010 and 2014. Considering that Hispanic patients accounted for only 5.1% of the patients during the study period, the $13,000 price tag discrepancy is jarring. Further, in 2020, the Hispanic population had a median household income of $55,321, which is more than $10,000 less than the median US household income for 2020 of $67,521.31 Thus, when compared to non-Hispanic whites, who have a median household income above the national median at $74,912, the financial cost of lung cancer disproportionally burdens Hispanic families.31
With the average cost at the end of life for lung cancer patients in the United States around $12,000,17 Hispanic patients are paying an average of $3000 more than the national average. Hispanic patients typically have lower socioeconomic backgrounds, a known limitation for healthcare access,9,12 and a risk factor for lung cancer.12 The discrepancy in end-of-life costs for Hispanic patients can be an undue, increased burden. Most patients were also in the 0–25th percentile for median household income in both test groups. Thus, there is a significant financial disparity for Hispanic lung cancer patients despite similarities in economic backgrounds to non-Hispanic patients.
Insurance status is also an essential factor for healthcare access,20,21 and our study found that most Hispanic and non-Hispanic patients were insured through Medicare, Medicaid, or private insurance. Medicare was the largest insurance group in total. One possible reason for the increased cost in Hispanic patients may have come from the use of Medicaid. Medicaid does not guarantee lung cancer screenings,20 and patients with Medicaid are often barred from primary care physician offices because of decreased reimbursement, moving patients towards emergency rooms and hospitals for treatment.22,24,25 The lack of screening has been implied in our study as most patients had higher severity of illness, demonstrating a lack of early screening and prevention. The increased cost for Hispanic patients seen in the current study may reflect increased emergency room visits, ICU stays, inpatient treatment, and aggressive chemotherapy treatment – trends more commonly seen in minority patients.8,9,22
Length of stay between Hispanic and non-Hispanic lung cancer patients had a minor variation; however, Hispanic patients across the study period did have a greater length of stay in hospitals. Furthermore, increased length of stay may also be connected to increased hospital use.22,24 Thus, Hispanic lung cancer patients are hospitalized for more extended periods and are paying more for care despite similarities in financial backgrounds and disease severity compared to non-Hispanic patients. Patients with longer lengths of stay tended to be of lower income. Considering that Hispanic patients tend to be of lower socioeconomic classes,9,12,13 the trend of more extended stays for poorer patients again highlights a financial burden targeting the Hispanic population.
Both lengths of stay and the increased hospital charges were associated with a higher incidence of radiation and chemotherapy. Increased cost and differences in healthcare utilization are reflected in previous studies and have a strong connotation for Hispanic patients. Minority patients are often treated with more aggressive chemotherapy without improving their quality of life.8–10,18 Thus, the more aggressive treatment may increase cost and length of stay without improving outcomes and is a disparity more greatly seen in minorities like Hispanic patients.
The results of this study have demonstrated that Hispanic lung cancer patients, on average, utilize healthcare more than non-Hispanic patients. Notably, Hispanic lung cancer patients between 2010 and 2014 significantly spent 26.6% more on healthcare and were hospitalized 3.5% longer than non-Hispanic patients. This finding is significant because it denotes the financial barriers affecting Hispanic lung cancer patients. They may face an increased cost for more aggressive end-of-life treatment than non-Hispanic patients without seeing improvements in survival rates. Thus, our results support financial assistance programs for minority patients and more outstanding promotion of palliative care utilization to reduce the cost of treatment towards end-of-life.
To reduce the financial burden and increase the quality of end-of-life, palliative care should be considered. Palliative care usage has increased since 2000, and its positive effects on lung cancer patients have been well documented.32–35 Multiple studies have described the improvements to patient quality of life and mood improvement from end-of-life palliative care.32–35 Further, in one study, cancer patients who started palliative care earlier in their treatment had reduced healthcare usage near end-of-life, reflective of less intensive care yet more outstanding quality outcomes and reduced cost.32 As a result, there is a growing movement to integrate palliative care into treatment standards and discuss palliative treatment options earlier with cancer patients.32–35 The integration of palliative care, especially if programs can be tailored to meet the needs of minority patients, is significant because minority groups are less likely to utilize palliative care and hospice treatments due to language differences, religious beliefs, low health literacy, and lack of healthcare access.36 Targeted programs for minority groups like Hispanic patients should account for such differences and conduct outreach in multiple languages, with sensitivity to cultural and religious differences, and promote access to various services.
This study has described various significant aspects of financial and treatment barriers targeting Hispanic patients; however, this research has limitations. First, this study used 2010–2014 data, which may not represent the current situation. Further research with more recent data is required. The national inpatient dataset utilized depends on ICD-9-CM codes, which may or may not have a restricted patient selection. The dataset also does not include clinical information like the cancer stage or pharmacologic treatments. Lung cancer patients at more advanced cancer stages are associated with higher healthcare spending and length of stay. Lack of information on advanced stages and spending or length of stay may weaken the result of this study. However, the study did contain control variables like APR-DRG, surgery, radiation, and chemotherapy, which may be used as a proxy role of patient stage status. Due to dataset limitations, substantial lung cancer risk factors like smoking, diet, and pollution were not included. Another limitation is that the dataset utilized does not describe if patients are treated in an outpatient or inpatient setting and the views patients or physicians have towards palliative care. Further research is required to determine how patient and physician perspectives on palliative care affect the delivery of palliative care and how it is associated with utilization and cost. The timing of palliative care delivery was also not captured and could be important for terminal lung cancer patients. Despite these limitations, our research is still generalizable to most deceased lung cancer patients in the United States because we utilized a well-sampled dataset with multiple study periods. Thus, our research denotes the benefits of palliative care for lung cancer patients and further discusses targeted minority end-of-life treatment.
Conclusion
This study has explored the targeting financial burden of lung cancer on the Hispanic population by identifying differences in healthcare utilization, represented by discounted hospital charges and length of hospital stay. On average, Hispanic patients spend more and are hospitalized longer than their non-Hispanic counterparts. This burden is felt on all levels of society as families suffer financial obstacles for treatment and society struggles to rectify racial health disparities. Previous research has discussed how disparities in healthcare utilization for Hispanic patients are caused by insurance status leading to lack of primary care providers, increased hospital use, lack of early screening, lower socioeconomic status, and exposure to pollution. Our findings reflect such disparities and illuminate the financial need of Hispanic lung cancer patients. In addition, past studies have characterized palliative care’s economic and quality of life benefits.32–35 Considering that our findings align with current economic and treatment disparities, trends for Hispanic lung cancer patients, our research promotes the early integration of palliative care in cancer treatment and calls for financial assistance programs for minority patients. Targeted programs and financial assistance will benefit the individual patient, their families, and the larger society as gaps in treatment and racial equality are narrowed.
Funding
This work was supported by the Soonchunhyang University Research Fund and BK21 FOUR (Fostering Outstanding Universities for Research, No. 5199990914048, Korean Ministry of Education).
Disclosure
The authors declare that they have no competing interests.
References
1. Schabath MB, Cote ML. Cancer progress and priorities: lung cancer. Cancer Epidemiol Biomarkers Prev. 2019;28(10):1563–1579. doi:10.1158/1055-9965.EPI-19-0221
2. U.S. Cancer Statistics Working Group. U.S. cancer statistics data visualizations tool, based on 2020 submission data (1999–2018). U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute; 2021. Available from: https://gis.cdc.gov/Cancer/USCS/#/AtAGlance/.
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
4. National Cancer Institute. Cancer stat facts: lung and bronchus cancer at a glance. SEER. Available from: https://seer.cancer.gov/statfacts/html/lungb.html.
5. National Cancer Institute. Cancer stat facts: lung and bronchus cancer survival statistics. SEER. Available from: https://seer.cancer.gov/statfacts/html/lungb.html.
6. Midthun DE. Early detection of lung cancer. F1000Res. 2016;5:739. doi:10.12688/f1000research.7313.1
7. Roointan A, Ahmad Mir T, Ibrahim Wani S, et al. Early detection of lung cancer biomarkers through biosensor technology: a review. J Pharm Biomed Anal. 2019;164:93–103. doi:10.1016/j.jpba.2018.10.017
8. Wintner LM, Giesinger JM, Zabernigg A, et al. Quality of life during chemotherapy in lung cancer patients: results across different treatment lines. Br J Cancer. 2013;109(9):2301–2308. doi:10.1038/bjc.2013.585
9. Bergamo C, Lin JJ, Smith C, et al. Evaluating beliefs associated with late-stage lung cancer presentation in minorities. J Thorac Oncol. 2013;8(1):12–18. doi:10.1097/JTO.0b013e3182762ce4
10. Saito AM, Landrum MB, Neville BA, Ayanian JZ, Earle CC. The effect on survival of continuing chemotherapy to near death. BMC Palliat Care. 2011;10(1):14. doi:10.1186/1472-684X-10-14
11. Zhang C, Zhang C, Wang Q, Li Z, Lin J, Wang H. Differences in stage of cancer at diagnosis, treatment, and survival by race and ethnicity among leading cancer types. JAMA Netw Open. 2020;3(4):e202950. doi:10.1001/jamanetworkopen.2020.2950
12. Zavala VA, Bracci PM, Carethers JM, et al. Cancer health disparities in racial/ethnic minorities in the United States. Br J Cancer. 2021;124(2):315–332. doi:10.1038/s41416-020-01038-6
13. Ellis L, Canchola AJ, Spiegel D, Ladabaum U, Haile R, Gomez SL. Racial and ethnic disparities in cancer survival: the contribution of tumor, sociodemographic, institutional, and neighborhood characteristics. J Clin Oncol. 2018;36(1):25–33. doi:10.1200/JCO.2017.74.2049
14. Miller KD, Goding Sauer A, Ortiz AP, et al. Cancer statistics for Hispanics/ latinos, 2018. CA Cancer J Clin. 2018;68(6):425–445. doi:10.3322/caac.21494
15. Jeon J, Holford TR, Levy DT, et al. Smoking and lung cancer mortality in the United States from 2015 to 2065. Ann Intern Med. 2018;169(10):684. doi:10.7326/M18-1250
16. Banegas MP, Hassett MJ, Keast EM, et al. Patterns of medical care cost by service type for patients with recurrent and de novo advanced cancer. Value Health. 2022;25(1):69–76. doi:10.1016/j.jval.2021.06.016
17. Sheehan DF, Criss SD, Chen Y, et al. Lung cancer costs by treatment strategy and phase of care among patients enrolled in medicare. Cancer Med. 2019;8(1):94–103. doi:10.1002/cam4.1896
18. Karanth S, Rajan SS, Sharma G, Yamal JM, Morgan RO. Racial-ethnic disparities in end-of-life care quality among lung cancer patients: a SEER-Medicare–Based Study. J Thorac Oncol. 2018;13(8):1083–1093. doi:10.1016/j.jtho.2018.04.014
19. U.S. Census Bureau. Figure 2. Percentage of people without health insurance coverage by selected characteristics: 2019; 2020. Available from: Census.gov.https://www.census.gov/content/dam/Census/library/visualizations/2020/demo/p60-271/figure2.pdf.
20. Rivera MP, Katki HA, Tanner NT, et al. Addressing disparities in lung cancer screening eligibility and healthcare access. An official American thoracic society statement. Am J Respir Crit Care Med. 2020;202(7):e95–e112. doi:10.1164/rccm.202008-3053ST
21. Monnat SM. The new destination disadvantage: disparities in Hispanic health insurance coverage rates in metropolitan and nonmetropolitan new and established destinations. Rural Sociol. 2017;82(1):3–43. doi:10.1111/ruso.12116
22. Zhang X, Carabello M, Hill T, Bell SA, Stephenson R, Mahajan P. Trends of racial/ethnic differences in emergency department care outcomes among adults in the United States from 2005 to 2016. Front Med. 2020;7:300. doi:10.3389/fmed.2020.00300
23. Edward J, Morris S, Mataoui F, Granberry P, Williams MV, Torres I. The impact of health and health insurance literacy on access to care for Hispanic/Latino communities. Public Health Nurs. 2018;35(3):176–183. doi:10.1111/phn.12385
24. Decker SL. Changes in Medicaid physician fees and patterns of ambulatory care. Inquiry. 2009;46(3):291–304. doi:10.5034/inquiryjrnl_46.03.291
25. Pines JM, Zocchi M, Moghtaderi A, et al. Medicaid expansion in 2014 did not increase emergency department use but did change insurance payer mix. Health Aff. 2016;35(8):1480–1486. doi:10.1377/hlthaff.2015.1632
26. Decker SL. In 2011 nearly one-third of physicians said they would not accept new Medicaid patients, but rising fees may help. Health Aff. 2012;31(8):1673–1679. doi:10.1377/hlthaff.2012.0294
27. Mark TL, Levit KR, Vandivort-Warren R, Coffey RM, Buck JA. Trends in spending for substance abuse treatment, 1986–2003. Health Aff. 2007;26(4):1118–1128. doi:10.1377/hlthaff.26.4.1118
28. Yu KG, Shen JJ, Kim PC, et al. Trends of hospital palliative care utilization and its associated factors among patients with systemic lupus erythematosus in the United States From 2005 to 2014. Am J Hosp Palliat Care. 2020;37(3):164–171. doi:10.1177/1049909119891999
29. Hwang J, Shen JJ, Kim SJ, et al. Opioid use disorders and hospital palliative care among patients with gastrointestinal cancers. Medicine. 2020;99(25):e20723. doi:10.1097/MD.0000000000020723
30. Hwang J, Shen J, Kim SJ, et al. Ten-year trends of utilization of palliative care services and life-sustaining treatments and hospital costs associated with patients with terminally ill lung cancer in the United States from 2005 to 2014. Am J Hosp Palliat Care. 2019;36(12):1105–1113. doi:10.1177/1049909119852082
31. Shrider E, Kollar M, Chen F, Semega J. Income and poverty in the United States: 2020; September 14, 2021. Available from: Census.gov.https://www.census.gov/library/publications/2021/demo/p60-273.html.
32. Temel JS, Greer JA, El-Jawahri A, et al. Effects of early integrated palliative care in patients with lung and GI cancer: a randomized clinical trial. J Clin Oncol. 2017;35(8):834–841. doi:10.1200/JCO.2016.70.5046
33. Triplett DP, LeBrett WG, Bryant AK, et al. Effect of palliative care on aggressiveness of end-of-life care among patients with advanced cancer. J Oncol Pract. 2017;13(9):e760–e769. doi:10.1200/JOP.2017.020883
34. Isenberg SR, Lu C, McQuade J, et al. Impact of a new palliative care program on health system finances: an analysis of the palliative care program inpatient unit and consultations at Johns Hopkins Medical Institutions. J Oncol Pract. 2017;13(5):e421–e430. doi:10.1200/JOP.2016.014860
35. Huo J, Hong YR, Turner K, et al. Timing, costs, and survival outcome of specialty palliative care in medicare beneficiaries with metastatic non–small-cell lung cancer. J Oncol Pract. 2020;16(12):e1532–e1542. doi:10.1200/OP.20.00298
36. Mayeda DP, Ward KT. Methods for overcoming barriers in palliative care for ethnic/racial minorities: a systematic review. Palliat Support Care. 2019;17(6):697–706. doi:10.1017/S1478951519000403
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.