")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 11
Health-related quality of life outcomes and economic burden of inflammatory bowel disease in Japan
Authors Yamabe K, Liebert R, Flores N, Pashos CL
Received 11 July 2018
Accepted for publication 15 November 2018
Published 12 March 2019 Volume 2019:11 Pages 221—232
DOI https://doi.org/10.2147/CEOR.S179892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Kaoru Yamabe,1 Ryan Liebert,2 Natalia Flores,2 Chris L Pashos3
1Healthcare Policy and Access, Takeda Pharmaceutical Company Limited, Nihonbashi, Chuouku, Tokyo 103-8668, Japan; 2Health Outcomes Research, Kantar Health, New York, NY 10010, USA; 3Global Outcomes and Epidemiology Research, Data Sciences Institute, Takeda Pharmaceuticals International Inc., Cambridge, MA, 02139, USA
Purpose: Previous Japanese studies have not compared health-related quality of life (HRQoL), work productivity and activity impairment, health care resource utilization (HRU), and costs in inflammatory bowel disease (IBD) patients with non-IBD controls, leading to insufficient evidence regarding IBD’s true burden. The aim of this study was to examine the impact of IBD on patient-reported outcomes and costs among Japanese adults (≥18 years).
Patients and methods: This retrospective cross-sectional study used data from the 2012–2014 Japan National Health and Wellness Survey (N=83,505). HRQoL (SF-36v2), work productivity and activity impairment (work productivity and activity impairment-General Health Questionnaire), HRU, and annual costs were compared between respondents with IBD (n=441) and non-IBD controls (n=82,944), and within IBD subtypes (Crohn’s disease [CD] and ulcerative colitis [UC]) using chi-square and ANOVA tests.
Results: Mental Component Summary (MCS), Physical Component Summary (PCS), and health state utility (Short-Form-6 Dimensions [SF-6D]) scores were significantly lower in IBD respondents than in controls (differences of 2.2 points, 2.6 points, and 0.041 points, respectively; all P<0.001). However, only differences in SF-6D scores reached the minimally important difference threshold. Furthermore, IBD-diagnosed respondents reported greater absenteeism, presenteeism, overall work productivity loss and activity impairment, and HRU than controls (all P<0.001). Consequently, direct and indirect costs were 3-fold and 1.5-fold higher in IBD-diagnosed respondents than in controls (both, P<0.001). Additionally, CD-diagnosed respondents had lower MCS, PCS, and SF-6D scores (all P<0.01) and higher direct costs (P<0.001) than UC-diagnosed respondents.
Conclusion: IBD and its subtype CD were associated with lower HRQoL, greater impairment to work and non-work activities, HRU, and costs among Japanese adults. This reinforces the general consensus that IBD patients, specifically those diagnosed with CD, require support from their family and society to combat the disease.
Keywords: activity impairment, costs, health care resource utilization, health-related quality of life, inflammatory bowel disease, work productivity impairment
Introduction
Inflammatory bowel disease (IBD) is a chronic and recurrent gastrointestinal condition believed to result from complex interactions between genetic and environmental factors that result in intestinal inflammation. IBD primarily consists of Crohn’s disease (CD), a relapsing transmural disease that can cause inflammation across the entire gastrointestinal tract, and ulcerative colitis (UC), a relapsing nontransmural disease that causes inflammation only in the colon.1
Previously, IBD was considered to be a “Western” disorder, since it was more prevalent among those populations, relative to Asians.2 A systematic review of studies conducted through 2010 found UC and CD prevalence rates to be higher in Western nations than in Asia and the Middle East (as high as 505 vs 168.3 per 100,000 and up to 322 vs 67.9 per 100,000 for UC and CD, respectively).3 Nevertheless, it is now known that cases of IBD have been steadily increasing in Asia mostly due to an increase in consumption of a “Western” diet4 and improvements in the living environment, with the latter reducing natural immunity according to the hygiene hypothesis.5 In Japan, the prevalence of UC and CD increased 3.5-fold (from 18.1 to 63.6 per 100,000 persons) and 3.0-fold (from 5.9 to 21.1 per 100,000 persons), respectively, between 1991 and 2005.5,6 More recent data from 2013 showed an additional increase to 121.9 and 30.1 per 100,000 persons, respectively.4
IBD can negatively impact an individual’s health-related quality of life (HRQoL), work productivity and daily activities and can increase economic burden and health care resource utilization (HRU). A Japanese patient-reported survey showed that IBD symptoms, such as bleeding, cramps, and exhaustion, were associated with impairments to social and interpersonal interactions.7 Other studies have also documented the difficulties experienced by Japanese patients with IBD; for example, patients with IBD had a poor HRQoL (measured using the Short-Form 8-Item Health Survey [SF-8]), and patients with CD had worse HRQoL than those with UC.8
In addition to poor HRQoL, patients with IBD also face difficulties in their work life. Previous studies from Japan showed lower mean annual income and employment among those with IBD, compared with non-IBD controls.8,9 Moreover, Japanese IBD patients often took leave from work for medical visits or due to extreme fatigue, which may have caused them to be discriminated against by their colleagues or even held back in their career.7 Furthermore, patients with IBD have high HRU and incur considerable costs. A prior study showed that patients with IBD had a higher number of hospitalizations, emergency room (ER) visits, and health care provider visits than non-IBD controls, resulting in higher direct and indirect costs in patients with IBD.10 Thus, the collective evidence demonstrates the substantial burden attributed to IBD, which highlights the need for effective long-term treatment and disease management.
Although the impact of IBD on HRQoL has been measured in Japan, these prior studies have utilized either a translated version of a European questionnaire7 or a shortened standard questionnaire (ie, SF-8).8 Moreover, studies of employment or work-related issues in Japanese patients with IBD have focused only on the factors affecting employment,9 such as overall motivation to work,11,12 or have qualitatively evaluated the impact of IBD on work outcomes.7 However, none of them have assessed multiple HRQoL parameters, including physical and mental functioning, and the impact of IBD on work productivity. Furthermore, there is a lack of research estimating HRU and costs among Japanese patients diagnosed with IBD in the general adult population.
Objectives
The current study examined the impact of IBD on HRQoL, work productivity and activity impairment, HRU, and costs associated with IBD among Japanese adults. In addition, HRQoL outcomes and associated costs were also compared between the IBD subtypes, CD and UC.
Patients and methods
Sample
This retrospective cross-sectional study used pooled data collected from respondents (≥18 years old) of the annually fielded 2012–2014 Japan National Health and Wellness Survey (NHWS; N=83,505), covering a wide range of comorbid conditions in addition to those not reporting any comorbidity.13 Although respondents are not targeted for repeat recruitment, 6,489 respondents completed the survey multiple times. However, only the most recent data for each respondent were used. Potential NHWS respondents were recruited from an opt-in online panel maintained by Lightspeed Research using stratified random sampling to mirror age and gender distributions in the general adult population in Japan. Participants who satisfied the below criteria were eligible for the study: 1) able to read and understand Japanese, 2) able to operate a computer to access the online survey, 3) resided in Japan, 4) aged ≥18 years, and 5) willing to provide informed consent to participate. After providing explicit informed consent via online agreement during initial screening, the respondents completed a confidential self-administered online survey. The NHWS was self-reported in nature and did not include any sensitive questions; therefore, it was exempted from review by the Pearl Institutional Review Board (Indianapolis, IN, USA). The study data will be provided for non-commercial use upon request.
Measures
IBD status
Respondents who self-reported an IBD diagnosis (CD, UC, or CD and UC) were included in the IBD group. The respondents who did not self-report an IBD diagnosis, but may have had some other diseases, were included in the non-IBD control group.
Demographic and health characteristics
Demographic measures included age (continuous), gender (male or female), education (university degree or less than a university degree), annual household income (<¥3,000,000, ¥3,000,000 to <¥5,000,000, ¥5,000,000 to <¥8,000,000, ≥¥8,000,000, or declined to answer), and health insurance status (national health insurance, social insurance, late-stage elderly insurance, other insurance, or no insurance).
Health characteristics were measured using data on smoking status (current smoker, former smoker, or never smoked), exercise behavior (do not exercise or exercise regularly), alcohol use (currently consume alcohol or abstain), body mass index category (using the WHO’s recommendation for Asian populations:14 underweight [<18.5 kg/m2], acceptable risk [18.5 to <23.0 kg/m2], increased risk [23.0 to <27.5 kg/m2], high risk [≥27.5 kg/m2], or decline to provide weight) and the Charlson Comorbidity Index (CCI).15 The CCI measures the degree of comorbidity burden on the individual due to the presence of specific and pre-selected comorbidities. Each self-reported comorbidity in the CCI is weighted, and these values are then summed across conditions to generate a total score; greater comorbidity burden is indicated by a higher CCI score.
Health-related quality of life
Physical Component Summary (PCS), Mental Component Summary (MCS), and Short-Form-6 Dimensions (SF-6D) health utility scores from the Medical Outcomes Study Short-Form 36-Item Health Survey version 2 (SF-36v2) were used to assess HRQoL.16,17 MCS and PCS are the two main summary scores that reflect all the SF-36v2 domains. They are normed to the US general population (M=50.00, SD=10.00) and can range from 0 to 100. For the SF-6D, health utility scores can range from 0 to 1. On each of these measures, higher scores signify better HRQoL. Minimally important differences (MIDs) for the MCS/PCS and SF-6D were represented by 3 and 0.041 points, respectively.16,18
Work Productivity and Activity Impairment
Impairment in work productivity and daily activities was assessed using the Work Productivity and Activity Impairment-General Health (WPAI-GH) questionnaire.19 Four domains (absenteeism, presenteeism, overall work impairment, and activity impairment) were assessed by the WPAI-GH, and scores were represented as percentages, with higher values indicating greater impairment due to the patient’s health in the past 7 days. Only currently employed respondents (full-time, part-time, or self-employed) provided data on absenteeism, presenteeism, and overall work impairment; all respondents provided data on activity impairment.
Health care resource utilization
HRU was defined by the self-reported number of health care provider visits, ER visits, and hospitalizations in the past 6 months.
Costs
Indirect and direct costs were estimated from the available NHWS data. Hourly wage rates from the Japan Basic Survey on Wage Structure, 2011,20 were integrated with information from the WPAI-GH using the Lofland method21 to calculate annual indirect costs. Each employed respondent’s annual wage was estimated by multiplying median weekly wage rates (as noted above) by the number of work weeks in a year (52 weeks). To calculate direct costs, the number of health care provider visits, ER visits, and hospitalizations over 6 months were multiplied by 2 (to estimate the annual number of visits), and further multiplied by the corresponding unit cost for each type of visit, which was obtained from the literature.22 For hospitalizations, the cost per day was obtained from the literature, and the number of hospitalizations for each respondent was obtained from the NHWS. To align them, we multiplied the cost per day by the average number of days hospitalized, as reported by the Organization for Economic Cooperation and Development.23
Analyses
Statistical Analysis System v9.3 was used to perform statistical analyses. Outcomes for individuals were compared across IBD status (diagnosed group vs control group) and IBD subgroup (UC vs CD).
Treatment of outliers and extraneous controls
The sample was examined for potential outliers and extraneous controls before analysis (ie, respondents without IBD whose mean values on the covariates were outside the range for the same covariates in the IBD group). There were no potential outliers identified, based on the distribution of covariates. However, there were extraneous controls that were identified based on age. The maximum age for the IBD group was 82 years old; therefore, individuals in the control group >82 years old were removed. The final study sample consisted of 83,385 respondents.
Independent group comparisons
Differences in demographics and health characteristics were examined by IBD status, as well as within CD and UC IBD subtypes. These results served to identify differences between those with IBD and controls and informed the selection of the covariates for multivariable analyses. Significant differences between the groups (P<0.05, two-tailed) for categorical and continuous outcome variables were determined using chi-square and one-way ANOVA tests, respectively.
Creation of sample weights
Baseline differences in sample size, demographics, and health characteristics between the IBD and control groups were minimized using propensity score weighting. The weights were estimated using the Toolkit for Weighting and Analysis of Non-equivalent Groups.24 Based on the independent group comparisons, the variables that differed significantly (P<0.05, two-tailed) were placed into generalized boosted models to predict IBD presence and to balance the study groups. One-, two-, and three-way interaction terms were tested in the models. The weighted samples provide a whole number that reflects the entire original sample, albeit with individual respondents counted as full or partial respondents to the extent that they are similar to, or different from, respectively, the sample of patients with IBD.
There are multiple advantages in choosing propensity score analyses over traditional regression-based approaches for covariate adjustment. For example, propensity score estimates avoid misspecification of the treatment effect model and allow the covariates to be independent of potentially influencing the estimated treatment effect. This is possible because propensity score estimates, unlike regression, are not derived from modeling of the outcome variables.25
The higher efficiency and precision of machine learning models – due to their efficient exploration of interactions and consequent ability to explain more potential variance in the data – such as generalized boosted models, enables their application in scenarios requiring multiple levels of treatment. These models estimate the propensity score and weight to be applied by performing several iterations of multiple regression trees. A major benefit of this model over regression-based alternatives is the program’s ability to undergo modifications, as required, to achieve the optimum propensity score model. The Toolkit for Weighting and Analysis of Nonequivalent Groups package also enables users to assess the quality of the propensity score weights estimated from generalized boosted models.24
Multivariable analyses
Weighted generalized linear models (GLMs) were performed to further adjust baseline differences that remained after weighting, to estimate the economic burden of IBD on health and economic outcomes, and to test whether any statistically significant (P<0.05, two-tailed) differences existed between the two study groups on the outcomes of interest. Only covariates that differed significantly post-weighting (age and CCI score) were included in the GLMs. For the HRQoL (MCS, PCS, and SF-6D health state utilities) data, a normal distribution for the error terms and an identity link function were used. For impairment to work and non-work activities, HRU, and direct/indirect costs variables, a negative binomial distribution with a log-link function was used to fit the data, which helped account for the skewed distribution of these variables. Estimated means, standard errors, CIs, and P-values were calculated for each dependent variable.
Ethics approval
Pearl Institutional Review Board (Indianapolis, IN, USA) approved the study.
Results
Demographics
A total of 83,385 respondents were included in the study analyses. On average, they were 47.5 years old, 50.6% were male, and 39.4% were not currently employed. The sample had an average CCI score of 0.14 (Table 1).
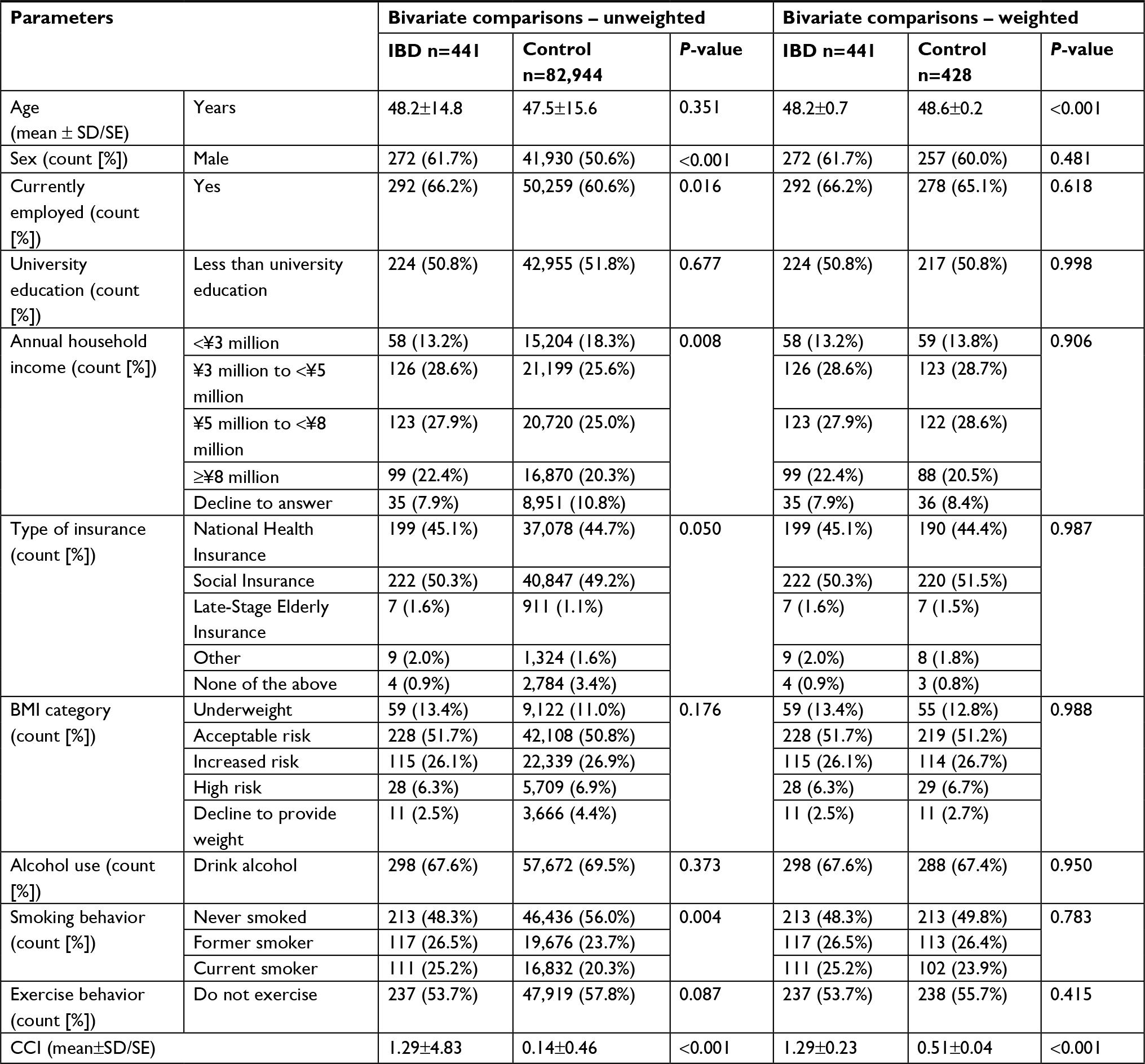 | Table 1 Comparison of demographics and health characteristics between patients with IBD and controls Notes: SDs and SEs are provided for the unweighted and weighted comparisons, respectively. Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; IBD, inflammatory bowel disease; SE, standard error. |
Health-related outcomes before matching
The IBD group was significantly more likely than non-IBD controls to be male (P<0.001), employed (P=0.016), and current smokers (P=0.004) and to have higher income (P=0.008), and CCI score (M=1.29 vs 0.14, P<0.001; Table 1). There were no significant differences between study groups in other demographics and health characteristics.
The IBD group had significantly lower MCS (44.7 vs 47.8), PCS (49.5 vs 53.4), and SF-6D (0.71 vs 0.76; for all, P<0.001) scores, with the difference in scores exceeding the MIDs for all the measures. IBD respondents also reported significantly higher absenteeism (9.3% vs 3.0%), presenteeism (29.6% vs 20.1%), overall work impairment (33.4% vs 21.7%), and activity impairment (30.0% vs 22.0%) than the control group (for all, P<0.001). Additionally, respondents with IBD had a significantly higher number of health care provider visits (11.8 vs 4.5), ER visits (0.9 vs 0.1), and hospitalizations in the past 6 months (2.9 vs 0.5), as well as higher annual per-patient (APP) direct (¥3,558,388 vs ¥637,329) and indirect (¥1,580,075 vs ¥980,639) costs than non-IBD controls (for all, P<0.001; Tables 2 and 3).
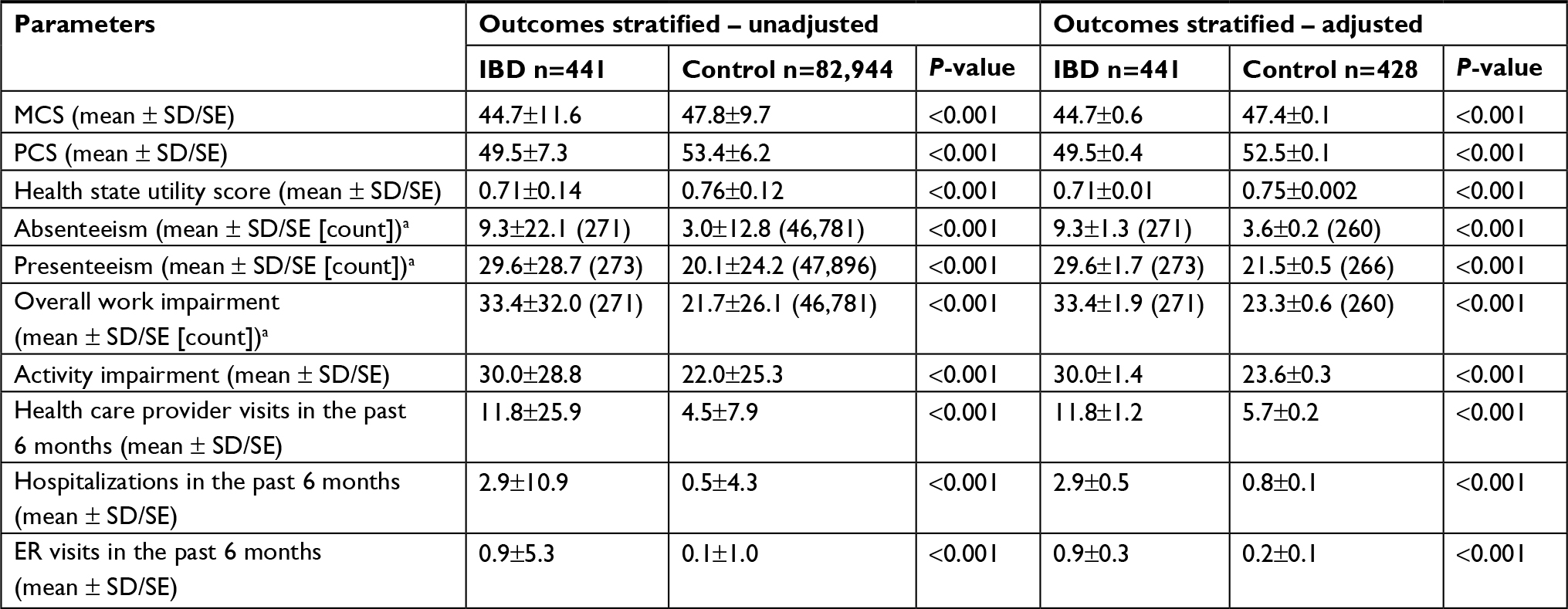 | Table 2 Effect of IBD on HRQoL, impairment to work and non-work activities, and HRU – bivariate analysis Notes: aNumber of patients. SDs and SEs are provided for the unweighted and weighted comparisons, respectively. Abbreviations: ER, emergency room; HRQoL, health-related quality of life; HRU, health care resource utilization; IBD, inflammatory bowel disease; MCS, mental component summary; PCS, physical component summary; SE, standard error. |
 | Table 3 Effect of IBD on direct and indirect costs – bivariate analysis Notes: aNumber of patients. SDs and SEs are provided for the unweighted and weighted comparisons, respectively. Abbreviations: APP, annual per-patient; ER, emergency room; IBD, inflammatory bowel disease; SE, standard error. |
Health-related outcomes after matching
After weighting, only age and CCI scores were significantly different between the groups (for both, P<0.001; Table 1).
In the weighted sample, the IBD group reported significantly lower HRQoL (MCS: 44.7 vs 47.4, PCS: 49.5 vs 52.5, and SF-6D: 0.71 vs 0.75), with the difference in the latter two scores reaching the MID. IBD respondents also reported higher absenteeism (9.3% vs 3.6%), presenteeism (29.6% vs 21.5%), overall work impairment (33.4% vs 23.3%), and activity impairment (30.0% vs 23.6%) than the non-IBD control group (for all, P<0.001). Additionally, patients with IBD had a significantly higher number of health care provider visits (11.8 vs 5.7), ER visits (0.9 vs 0.2), and hospitalizations in the past 6 months (2.9 vs 0.8) than non-IBD controls, resulting in significantly higher direct (¥3,558,388 vs ¥1,033,987) and indirect (¥1,580,075 vs ¥1,081,572) costs (for all, P<0.001; Tables 2 and 3).
Multivariable analysis
The results observed were consistent even after controlling for age and CCI in GLMs. Patients with IBD had significantly lower HRQoL (MCS: 45.1 vs 47.3, PCS: 50.2 vs 52.8, and SF-6D: 0.71 vs 0.75), with only the difference in SF-6D scores meeting the MID, and significantly higher absenteeism (8.1% vs 3.1%), presenteeism (28.1% vs 20.7%), overall work impairment (32.0% vs 22.4%), and activity impairment (28.4% vs 22.8%; for all, P<0.001), compared with the non-IBD control group. The IBD group also had a significantly higher number of health care provider visits (7.4 vs 4.5), ER visits (0.3 vs 0.1), and hospitalizations in the past 6 months (2.1 vs 0.6) than controls, resulting in significantly higher direct (¥2,563,141 vs ¥808,467) and indirect (¥1,546,610 vs ¥1,067,331) costs (for all, P<0.001; Tables 4 and 5).
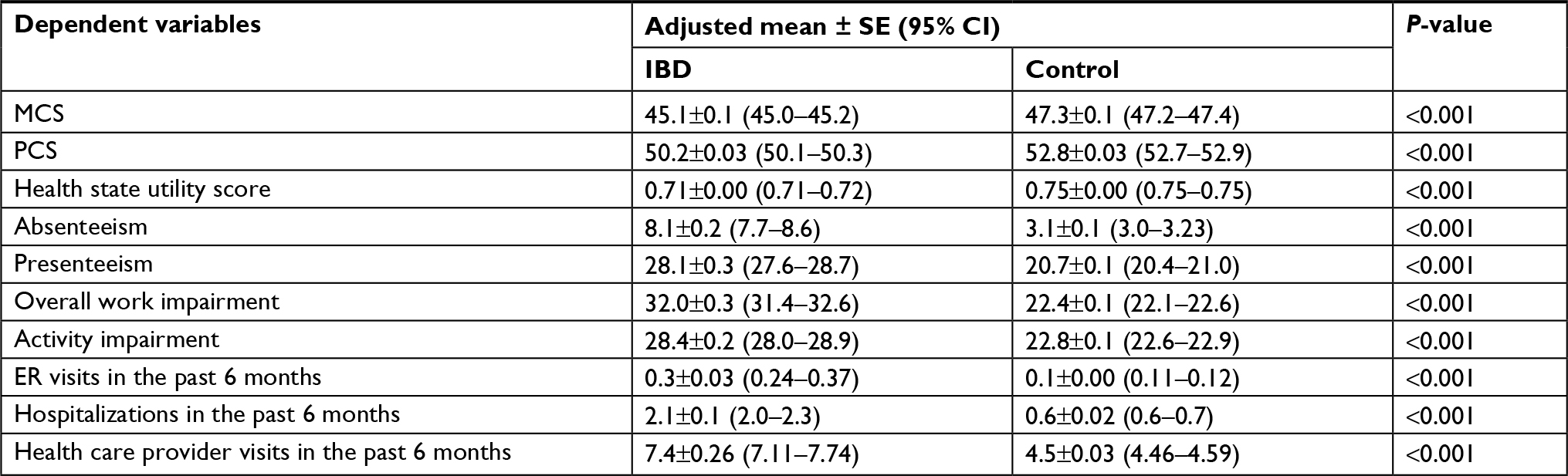 | Table 4 Association of IBD with HRQoL, impairment to work and non-work activities, and HRU – multivariable analysis Abbreviations: ER, emergency room; HRU, health care resource utilization; IBD, inflammatory bowel disease; MCS, mental component summary; PCS, physical component summary; SE, standard error. |
 | Table 5 Effect of IBD on direct and indirect costs – multivariable analysis Abbreviations: APP, annual per-patient; ER, emergency room; IBD, inflammatory bowel disease; SE, standard error. |
Comparison of health-related outcomes among the IBD subtypes
Nine respondents from the 441 IBD-diagnosed respondents were not included in the CD vs UC analyses because they reported both CD and UC. Demographic and health characteristics between the UC- and CD-diagnosed respondents are presented in Table 6.
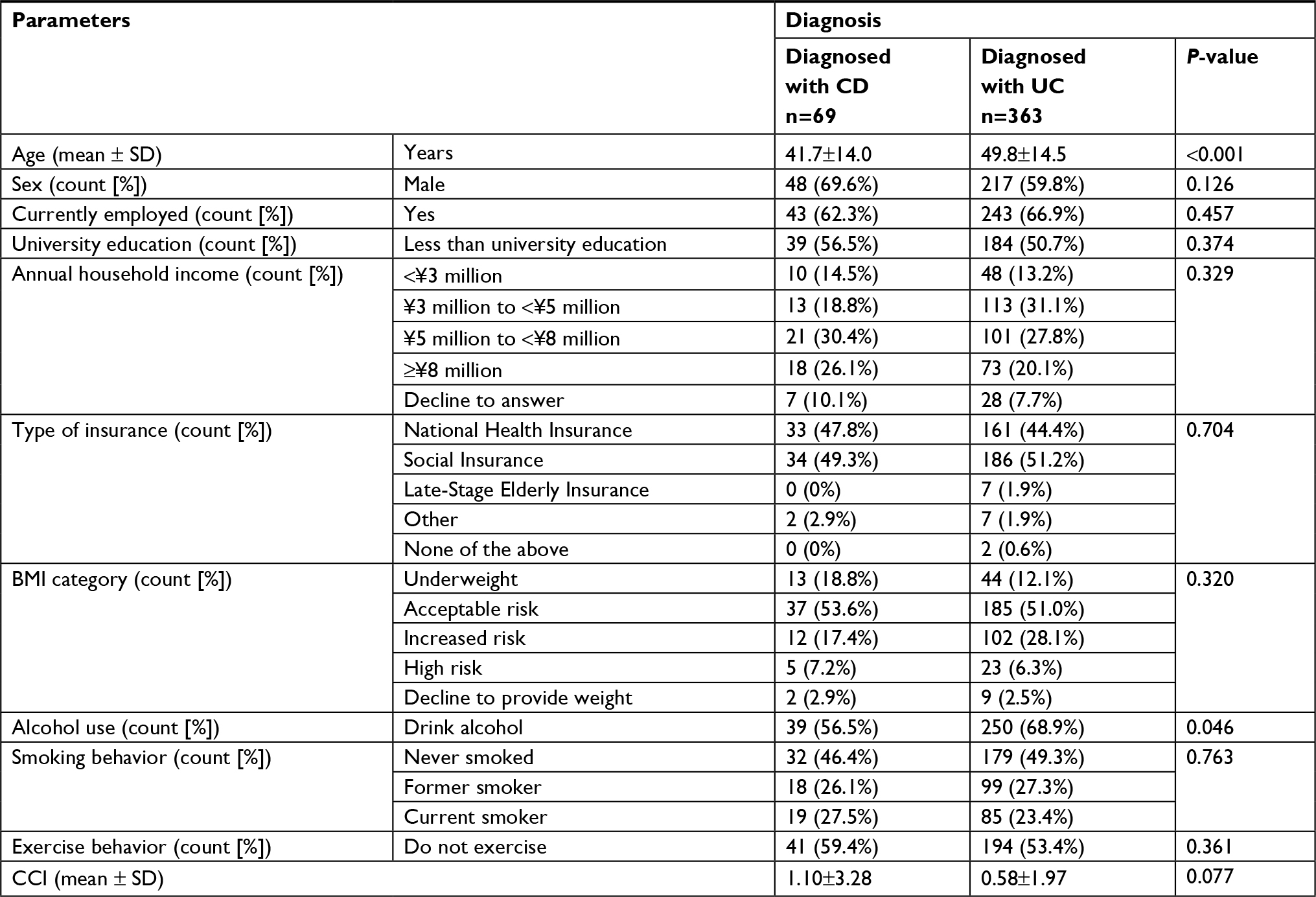 | Table 6 Comparisons for sociodemographics and health characteristics for the respondents diagnosed with UC or CD, while excluding those respondents diagnosed with both Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; CD, Crohn’s disease; UC, ulcerative colitis. |
The worse HRQoL of CD-diagnosed respondents was evident by their significantly lower MCS (41.4 vs 45.7; P=0.004), PCS (47.6 vs 50.2; P=0.005), and SF-6D scores (0.67 vs 0.72; P=0.002), compared with UC-diagnosed respondents, with the difference among the groups for MCS and SF-6D exceeding the MID. Although not significantly different, respondents with CD reported higher absenteeism, presenteeism, overall work impairment, and activity impairment than respondents with UC. Direct costs (¥7,533,257 vs ¥2,135,095; P<0.001) were significantly higher in respondents with CD than in those with UC. However, health care provider visits, ER visits, and indirect costs were similar between the two groups (Tables 7 and 8).
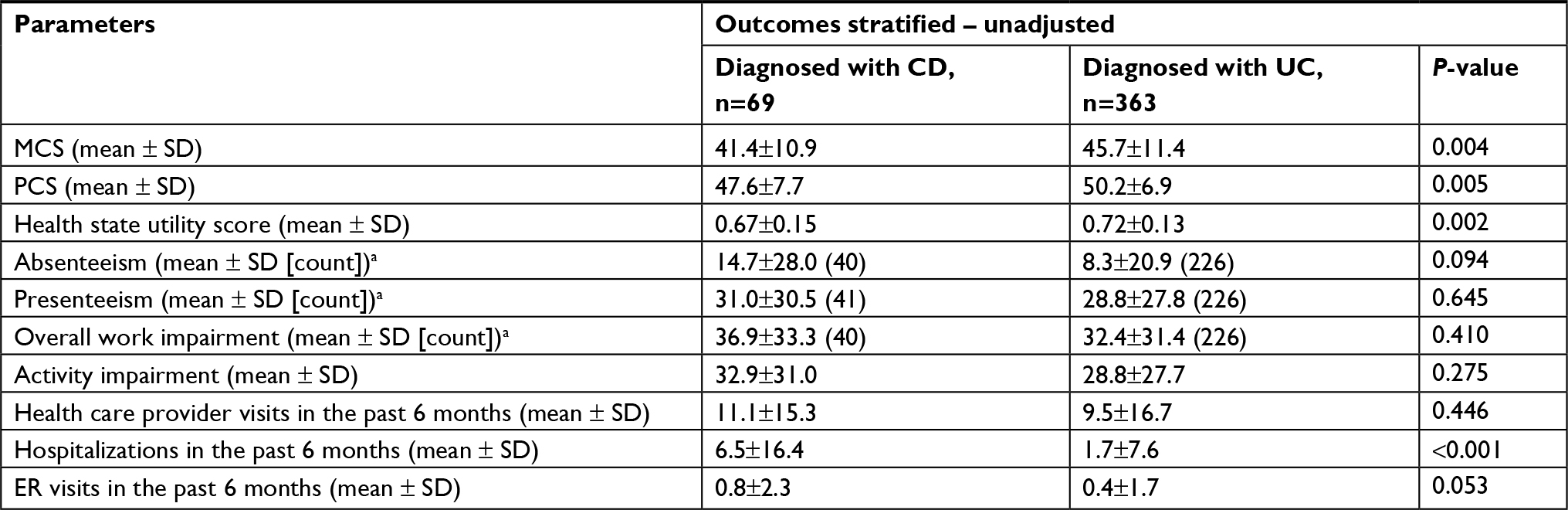 | Table 7 Patient-reported outcomes stratified by UC/CD diagnosis Note: aNumber of patients. Abbreviations: CD, Crohn’s disease; ER, emergency room; MCS, mental component summary; PCS, physical component summary; UC, ulcerative colitis. |
 | Table 8 Direct and indirect costs stratified by UC/CD diagnosis Note: aNumber of patients. Abbreviations: APP, annual per-patient; CD, Crohn’s disease; ER, emergency room; UC, ulcerative colitis. |
Discussion
In the current study, HRQoL in patients with IBD was affected by both worse mental and physical health status, compared with non-IBD controls who did not self-report IBD, but may have had other diseases. Furthermore, IBD patients exhibited higher absenteeism, presenteeism, activity impairment, and HRU, compared with non-IBD controls. In fact, differences in all patient-reported outcomes remained significant after propensity score weighting and further adjustment for confounders using GLMs, which provides strong support for the observed pattern of results. Among IBD subtypes, respondents diagnosed with CD had lower HRQoL than respondents with UC. The former also reported higher impairment to work and non-work activities and HRU than respondents diagnosed with UC.
The results observed in this study are in line with previous research.8,26,27 For example, a Japanese online survey study showed poorer HRQoL on several dimensions of the SF-8, including physical and social functioning, role physical, and emotional and mental health among patients with IBD, compared with controls. The study further reported poorer HRQoL outcomes among patients diagnosed with CD than among patients diagnosed with UC.8 Similar results were reported in a recent nationwide survey of patients with IBD from France using the Short-IBD Questionnaire and SF-36v2 to measure HRQoL.27 The MCS and PCS scores observed for IBD-diagnosed respondents in this study were 4.3 and 2.2 points higher than those reported in the French study (44.7 vs 40.4 and 49.5 vs 47.3, respectively). Additionally, the HRQoL outcomes of the CD- and UC-diagnosed respondents in the current study were relatively higher than those of the French study,27 implying slightly better HRQoL in Japanese patients with IBD. IBD was shown to have less impact on absenteeism, but a greater impact on presenteeism and activity impairment.27Similarly, a study by Zand et al26 in the US reported significantly higher presenteeism, but not absenteeism, in IBD patients than in controls. The results of both the aforementioned studies are in contrast to the current study wherein both presenteeism and absenteeism were significantly higher in patients with IBD than in controls. The discrepancies between these studies and the current study could be due to methodological differences. While the US study was prospective in nature and used healthy controls as a comparator,26 the French study was retrospective and assessed differences in outcomes between UC and CD patients, based on disease severity, and no control group was included.27 The current study did not show any significant difference in absenteeism, presenteeism, work productivity, and activity impairment when IBD subtypes were compared, possibly due to the five-fold difference in sample size. Further studies with a larger CD sample size could reveal statistically significant differences.
Respondents with IBD in the present study had a higher number of health care provider visits (1.6 times), hospitalizations (3.5 times), and ER visits (2.7 times) than the control group in the past 6 months. These results are consistent with those reported by Cohen et al,10 in which patients with UC in the US had significantly higher rates of hospitalization, ER visits, and prescription drug use. Consistent with a US study that analyzed HRU over 2 years,28 CD-diagnosed respondents in the current study reported a higher number of health care provider visits (1.2 times), hospitalizations (3.7 times), and ER visits (2.2 times) than UC-diagnosed respondents.
IBD poses a large economic burden on the individual and society. Both the APP direct and indirect costs were found to be 3-fold and 1.5-fold higher for patients with IBD than for controls, respectively. The higher direct costs observed for those with IBD in this study were mainly driven by increased health care provider visits and hospitalization costs. These findings are similar to those of a US study that showed higher adjusted total direct and indirect costs for patients with IBD than for controls.10 Costs from health care provider visits could be high because of IBD symptom-related visits or due to the patients’ desire to talk about his/her general health and well-being. The latter is a distinct possibility, as patients with IBD who have poor HRQoL are more likely to be depressed27 and are also more likely to visit a mental health professional than the general population.29 Among IBD subtypes, CD-diagnosed respondents in the current study reported higher direct costs than UC-diagnosed respondents, which is consistent with a prior US study wherein patients diagnosed with CD had a higher number of health care visits and greater medication use.30 However, in contrast to a prior US study that analyzed insurance coverage of employees,31 indirect costs of CD-diagnosed respondents were observed to be higher than those of UC-diagnosed respondents. This could have occurred due to the difference in population and study time period (1999–2005 for the US study and 2012–2014 for the current study).
As shown in this study, IBD adversely affects HRQoL. However, comparisons with other diseases are essential to understand the true burden that IBD places on society. The 2017 data reported by Japanese Ministry of Health, Labour and Welfare (MHLW) states that cancer, with a death rate of 298.3 per 100,000 people, was the leading cause of death in Japan.32 However, as stated in Kantar Health’s Global Health and Wellness Report,33 cancer-afflicted Japanese adults reported higher HRQoL and lower work and activity impairment than IBD-afflicted respondents (MCS: 48.1 vs 45.1, PCS: 49.8 vs 50.2, overall work productivity impairment: 29.6% vs 32.0%, and activity impairment: 25.8% vs 28.4%). This shows that, while cancer causes higher mortality, IBD affects patients’ daily living more.
Treatment for IBD may potentially help to improve HRQoL, increase work productivity, and reduce activity impairment and costs. With the advent of novel biologics, like anti-tumor necrosis factor agents, patients can lead healthier lives. Indeed, new biologic agents, such as adalimumab, were found to improve HRQoL, increase work productivity, and reduce activity impairment.34 Similarly, treatment with infliximab improved HRQoL in Chinese patients with IBD.35 Apart from HRQoL, studies from the US and Spain have shown that usage of new biologic agents, such as infliximab and adalimumab, is associated with a lower HRU.36,37 Furthermore, infliximab was found to be beneficial, compared with cyclosporine, by reducing length of hospital stay and the associated costs in patients with severe UC.38 The reduction in HRU could be related to the lower disease severity achieved after administration of newer agents, such as infliximab, as shown by Waters et al.36
Although these new therapeutic agents are more effective than traditional therapies, it should also be noted that their cost is high. Studies have shown that overall economic burden increases when adalimumab or infliximab is used.37,38 However, the MHLW supports the use of such biologic treatments by means of a governmental grant; hence, the treatment decisions made by patients and their physicians in Japan are unlikely to be affected by the costs of these new medications.8
The strength of this study lies in the fact that this is the first large, nationwide study that utilized patient-reported outcomes data to assess multiple facets of disease burden, including HRQoL, impairment to work and non-work activities, HRU, and costs among Japanese adults diagnosed with IBD. Furthermore, comparing these parameters against controls (healthy and non-healthy) revealed the true burden of IBD in Japanese society.
Limitations
This study has a few important limitations. Survey responses were self-reported by participants and were not verified by electronic health records or physician charts. However, the survey was relatively low-stakes and benign, as questions were not designed to be intrusive or offensive. Survey responses were confidential, thereby reducing the incentive to misrepresent one’s reporting. As data were collected in 2012–2014, there is a need for follow-up with more recent data. While relevant demographic and health characteristics were controlled through weighting and multivariable models, we cannot exclude the possibility that other variables not included in these analyses may account for the observed pattern of results. Additionally, given the cross-sectional nature of the data, causal inferences cannot be made from the study results, and changes in the relationships between study variables over time could not be assessed. Although the NHWS is demographically representative of the adult population in Japan, the extent to which the IBD sample is representative of the general population of adults diagnosed with IBD in Japan could not be determined.
Conclusion
Overall, IBD was associated with poorer HRQoL and lower work productivity, as well as higher activity impairment, HRU, and APP direct and indirect costs. The direct health care costs of respondents with IBD are twice those incurred by controls, which has serious implications on future health care planning. Among IBD subtypes, CD-diagnosed respondents were more affected than UC-diagnosed respondents.
The findings of the current study reveal unmet needs among the IBD-diagnosed Japanese respondents, implying that reducing disease burden by means of more effective treatment strategies could potentially improve health and economic outcomes. Furthermore, the study results underscore the importance for health care systems in Asia, specifically in Japan, to preemptively invest sufficient resources in preparation for the burgeoning health and economic burden of IBD in this region.
Acknowledgments
The authors acknowledge Leo J Philip Tharappel and Ramu Periyasamy, PhD, Indegene Pvt Ltd. for assistance with literature review and writing, as well as Martine C. Maculaitis, PhD, for editing assistance on behalf of Kantar Health. This research was funded by Takeda Pharmaceutical Company Limited, Japan. Takeda utilized Kantar Health’s services to conduct this research, analyze the data, and prepare this manuscript. This paper was presented at the ISPOR 19th Annual European Congress as a poster presentation with interim findings. The poster’s abstract was published in “Research Poster Presentations” in the journal Value in Health: https://doi.org/10.1016/j.jval.2016.09.970.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Kaoru Yamabe, at the time of this study, was an employee of Takeda Pharmaceutical Company Limited. Ryan Liebert and Natalia Flores, at the time of this study, were employees of Kantar Health, a paid consultant of Takeda Pharmaceutical Company Limited. Chris L Pashos, at the time of this study, was an employee of Takeda Pharmaceuticals International, Inc. The authors report no other conflicts of interest in this work.
References
Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. The Lancet. 2007;369(9573):1641–1657. | ||
Cheon JH. Genetics of inflammatory bowel diseases: a comparison between Western and Eastern perspectives. J Gastroenterol Hepatol. 2013;28(2):220–226. | ||
Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–54. | ||
Ng WK, Wong SH, Ng SC. Changing epidemiological trends of inflammatory bowel disease in Asia. Intest Res. 2016;14(2):111–119. | ||
Asakura K, Nishiwaki Y, Inoue N, Hibi T, Watanabe M, Takebayashi T. Prevalence of ulcerative colitis and Crohn’s disease in Japan. J Gastroenterol. 2009;44(7):659–665. | ||
Morita N, Toki S, Hirohashi T, et al. Incidence and prevalence of inflammatory bowel disease in Japan: nationwide epidemiological survey during the year 1991. J Gastroenterol. 1995;30(Suppl 8):1–4. | ||
Ueno F, Nakayama Y, Hagiwara E, Kurimoto S, Hibi T. Impact of inflammatory bowel disease on Japanese patients’ quality of life: results of a patient questionnaire survey. J Gastroenterol. 2017;52(5):555–567. | ||
Matsumoto T, Yanai S, Toya Y, Ueno M, Nakamura S. Internet-orientated Assessment of QOL and Actual Treatment Status in Japanese Patients with Inflammatory Bowel Disease: The 3I survey. J Crohns Colitis. 2015;9(6):477–482. | ||
Mahlich J, Matsuoka K, Nakamura Y, Sruamsiri R. The relationship between socio-demographic factors, health status, treatment type, and employment outcome in patients with inflammatory bowel disease in Japan. BMC Public Health. 2017;17(1):623. | ||
Cohen R, Skup M, Ozbay AB, et al. Direct and indirect healthcare resource utilization and costs associated with ulcerative colitis in a privately-insured employed population in the US. J Med Econ. 2015;18(6):447–456. | ||
Ito M, Togari T, Jeong Park M, Yamazaki Y. Difficulties at work experienced by patients with inflammatory bowel disease (IBD) and factors relevant to work motivation and depression. Jpn J Health Hum Ecol. 2008;74(6):290–310. | ||
Nasu A, Yamada K, Morioka I. Difficulties at work and work motivation of ulcerative colitis suffers. Sangyo Eiseigaku Zasshi. 2015;57(1):9–18. | ||
Kantar Health. National Health and Wellness Survey. Patient-Reported Healthcare Insights. New York: Kantar Health. Available from: http://www.kantarhealth.com/docs/datasheets/kh-national-health-and-wellness-survey.pdf. Accessed October 31, 2018. | ||
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. | ||
Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Maruish ME. User’s Manual for the SF36v2® Health Survey. 3rd ed. Lincoln: QualityMetric, Inc; 2011. | ||
Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ. 2002;21(2):271–292. | ||
Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res. 2005;14(6):1523–1532. | ||
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics.1993;4(5):353–365. | ||
Mhlw.go.jp [homepage on the Internet]. Tokyo: Basic Survey on Wage Structure. Ministry of Health Labour and Welfare of Japan; 2011. Available from: http://www.mhlw.go.jp/toukei_hakusho/toukei/. Accessed August 3, 2017.. | ||
Lofland JH, Pizzi L, Frick KD. A review of health-related workplace productivity loss instruments. Pharmacoeconomics. 2004;22(3):165–184. | ||
Ministry of Health Law. 2013 Fiscal Year Trends of Medical Expenses. Tokyo, Japan: Ministry of Health, Labor and Welfare; 2014. | ||
Organization for Economic Cooperation and Development (OECD). Length of Hospital Stay (Indicator). Available from: https://data.oecd.org/healthcare/length-of-hospital-stay.htm. Accessed March 12, 2018. | ||
Ridgeway G, Mccaffrey D, Morral A, Burgette L, Griffin BA. Toolkit for weighting and analysis of nonequivalent groups: a Tutorial for the TWANG Package. Santa Monica, CA: RAND corporation; 2017. | ||
McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat Med. 2013;32(19):3388–3414. | ||
Zand A, van Deen WK, Inserra EK, et al. Presenteeism in inflammatory bowel diseases: a hidden problem with significant economic impact. Inflamm Bowel Dis. 2015;21(7):1623–1630. | ||
Williet N, Sarter H, Gower-Rousseau C, et al. Patient-reported outcomes in a French Nationwide Survey of Inflammatory Bowel Disease Patients. J Crohns Colitis. 2017;11(2):165–174. | ||
van Deen WK, van Oijen MGH, Myers KD, et al. A nationwide 2010–2012 analysis of U.S. healthcare utilization in inflammatory bowel diseases. Inflamm Bowel Dis. 2014;20(10):1747–1753. | ||
Bhandari S, Larson ME, Kumar N, Stein D. Association of inflammatory bowel disease (IBD) with depressive symptoms in the United States population and independent predictors of depressive symptoms in an IBD population: A NHANES Study. Gut Liver. 2017;11(4):512–519. | ||
Kappelman MD, Rifas-Shiman SL, Porter CQ, et al. Direct healthcare costs of Crohn’s disease and ulcerative colitis in US children and adults. Gastroenterology. 2008;135(6):1907–1913. | ||
Gibson TB, Ng E, Ozminkowski RJ, et al. The direct and indirect cost burden of Crohn’s disease and ulcerative colitis. J Occup Environ Med. 2008;50(11):1261–1272. | ||
Mhlw.go.jp [homepage on the Internet]. Tokyo: outline of health, labour and welfare statistics. Director-general for statistics and information policy, Ministry of Health, Labour and Welfare of Japan; 2017. Available from: https://www.mhlw.go.jp/toukei/youran/aramashi/shibou.pdf. Accessed August 3, 2017. | ||
Kantar Health. The Global Health and Wellness Report; 2017. Available from: http://www.kantarhealth.com/docs/reports/final-2017-ghwr-full.pdf. Accessed March 12, 2018. | ||
Lichtiger S, Binion DG, Wolf DC, et al. The CHOICE trial: adalimumab demonstrates safety, fistula healing, improved quality of life and increased work productivity in patients with Crohn’s disease who failed prior infliximab therapy. Aliment Pharmacol Ther. 2010;32(10):1228–1239. | ||
Xu J, Lin H, Feng X, Tang M, Shen J, Ran Z. Different therapeutic approaches on quality of life in patients with inflammatory bowel disease. BMC Gastroenterol. 2014;14(1):199. | ||
Waters HC, Vanderpoel JE, Nejadnik B, et al. Resource utilization before and during infliximab therapy in patients with inflammatory bowel disease. J Med Econ. 2012;15(1):45–52. | ||
Saro C, Ceballos D, Muñoz F, et al. Resources utilization and costs the year before and after starting treatment with adalimumab in Crohn’s disease patients. Inflamm Bowel Dis. 2015;21(7):1631–1640. | ||
Löwenberg M, Duijvis NW, Ponsioen C, van den Brink GR, Fockens P, D’Haens GR. Length of hospital stay and associated hospital costs with infliximab versus cyclosporine in severe ulcerative colitis. Eur J Gastroenterol Hepatol. 2014;26(11):1240–1246. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.