")
Back to Journals » Cancer Management and Research » Volume 14
Health-Related Quality of Life of Patients with Metastatic Pancreatic Cancer: A Systematic Literature Review
Authors Yoo HK , Patel N, Joo S, Amin S, Hughes R, Chawla R
Received 1 July 2022
Accepted for publication 13 November 2022
Published 6 December 2022 Volume 2022:14 Pages 3383—3403
DOI https://doi.org/10.2147/CMAR.S376261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bilikere Dwarakanath
Hyun Kyoo Yoo,1 Nikunj Patel,2 Seongjung Joo,3 Suvina Amin,2 Rowena Hughes,4 Rajinder Chawla5
1Health Economics & Payer Evidence AstraZeneca, Cambridge, UK; 2Oncology Business Unit, AstraZeneca, Gaithersburg, MD, USA; 3MRL, Center for Observational & Real-World Evidence (CORE), Oncology, Merck Sharp & Dohme LLC, a Subsidiary of Merck & Co., Inc, Rahway, NJ, USA; 4AccuScript Consultancy, Reading, Berkshire, UK; 5AccuScript Consultancy, Ludhiana, Punjab, India
Correspondence: Hyun Kyoo Yoo, Global Value, Access and Pricing, Alexion, AstraZeneca Rare Disease, City House, 130 Hills Road, Cambridge, CB2 1RE, UK, Email [email protected]
Background: Metastatic pancreatic cancer (mPaC) has a poor prognosis and available treatments provide only moderate improvements in survival. Preserving or improving health-related quality of life (HRQoL) is therefore an important treatment outcome for patients with mPaC. This systematic review identified HRQoL data in patients with mPaC before and after treatment, compared these with data from the general population, and reported the effects of different mPaC treatments on HRQoL.
Methods: Searches were performed in Embase, PubMed, and the Cochrane Library from January 2008 to May 2021, and the articles identified were screened for HRQoL data in patients with mPaC. Abstracts from relevant congresses were also manually searched. Publications included were randomized controlled trials and observational studies written in English that reported HRQoL data for adult patients with non-resectable mPaC who were on or off treatment.
Results: Thirty relevant publications were identified and HRQoL scores were collected. Overall, baseline mean scores from the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30), 5-dimension EuroQol questionnaire (EQ-5D), and Functional Assessment of Cancer Therapy-General (FACT-G) for newly diagnosed and previously treated patients with mPaC were worse than those of the general population. Baseline scores were generally better for previously treated patients than for newly diagnosed patients, indicating that mPaC treatments preserve or improve HRQoL. Identified publications also reported changes in HRQoL following first- or subsequent-line chemotherapy. When reported, 10 studies found improvements in overall HRQoL compared with baseline scores, four reported no changes in overall HRQoL after treatment, and six found deteriorations in overall HRQoL.
Conclusion: Patients with mPaC had worse HRQoL than the general population. Available anti-cancer therapies can improve or preserve HRQoL.
Keywords: health-related quality of life, metastatic pancreatic cancer, symptoms
Introduction
Pancreatic cancer is an aggressive malignancy associated with a poor prognosis, in part due to its late diagnosis. It usually progresses to locally advanced or metastatic disease while still asymptomatic, and as a result, fewer than 20% of patients have a resectable tumor at diagnosis.1 Five-year overall survival (OS) for metastatic pancreatic cancer (mPaC) is approximately 3% and median OS is often less than 1 year.2
Current treatment options for mPaC provide only moderate improvements in survival compared with palliative care and are associated with significant toxicity. For patients with a good performance status (eg Eastern Cooperative Oncology Group Performance Status [ECOG PS] of 0 or 1) and a favorable comorbidity profile who wish to receive aggressive therapy, guidelines recommend the oxaliplatin-containing regimen FOLFIRINOX (leucovorin, fluorouracil, irinotecan, and oxaliplatin) or nanoparticle albumin-bound (nab)-paclitaxel plus gemcitabine (GEM), known as nPG.1,3 The pivotal PRODIGE-4/ACCORD-11 trial showed that patients receiving FOLFIRINOX had a significant OS benefit compared with those receiving GEM alone4 while the MPACT trial showed that patients receiving nPG had significantly longer median OS than those receiving GEM alone.5 Treatment with FOLFIRINOX or nPG has an associated increase in toxicity compared with GEM;4,5 therefore, for patients with a worse performance status (ECOG PS of 2) or comorbidities that prevent the use of more aggressive regimens, the standard of care is GEM monotherapy, which may be combined with capecitabine or erlotinib.1,3
Improvements in OS in mPaC are currently limited, with recommended treatments providing an OS increase of 6–11 months. Thus, providing adequate symptom control and preserving or improving health-related quality of life (HRQoL) are important therapeutic goals that benefit patients and their caregivers. mPaC is often associated with abdominal pain, appetite loss, and weight loss, with the toxicities of chemotherapy adding to this burden. To understand the HRQoL of patients with mPaC and how available treatments affect this, a systematic literature review of studies investigating HRQoL in patients with mPaC was performed. The aims of this study were (a) to summarize the HRQoL of newly diagnosed and previously treated patients with mPaC and compare this with data for the general population and (b) to report the effects of treatment on the HRQoL of patients with mPaC.
Materials and Methods
A systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.6 Searches were performed in Embase, PubMed, and the Cochrane Library including articles published from January 2008 to May 2021 and using search terms for mPaC and HRQoL (see search strings in Supplementary Tables 1–6). Searches were restricted to publications in English. A first round of searches was conducted on 17 April 2019, with update searches carried out on 14 May 2021. Results of the two sets of searches were combined for analysis. Search results were screened for publications reporting HRQoL in patients with mPaC on or off treatment. Manual searches were performed for abstracts presented at the following annual conferences for 2016–2021: the American Society of Clinical Oncology Annual Meeting, the American Society of Clinical Oncology Gastrointestinal Cancers Symposium, the European Society for Medical Oncology Annual Congress, the European Society for Medical Oncology World Congress on Gastrointestinal Cancer, the International Association of Pancreatology annual conference, the International Society for Pharmacoeconomics and Outcomes Research Europe conference, the International Society for Pharmacoeconomics and Outcomes Research US conference, and the International Conference on Hepatobiliary and Pancreatic Disorders.
Inclusion and exclusion criteria for studies to incorporate in this systematic review were developed ahead of performing the searches and were based on population, intervention, comparators, outcomes, study design, study period, publication type (ie primary or secondary publications and congress abstracts), and language (Table 1). Randomized controlled trials and observational studies were included if they involved HRQoL data for patients aged over 18 years with non-resectable mPaC. Studies were required to be published in English, and case reports, case series, systematic or narrative reviews, and editorials were excluded.
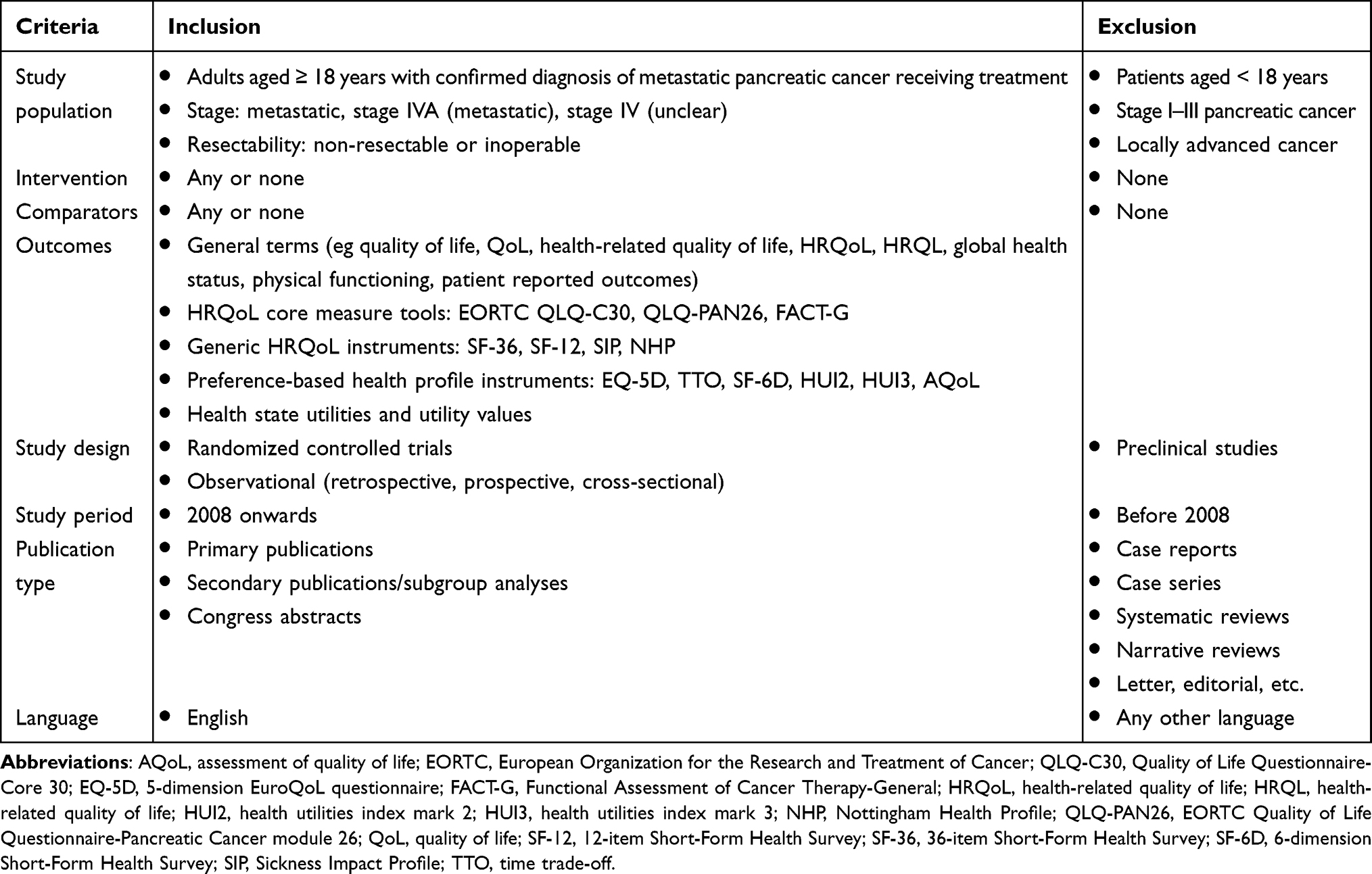 |
Table 1 Eligibility Criteria Used in the Systematic Screening Strategy to Identify Publications Relating to HRQoL |
Screening based on title and abstract was performed independently by two researchers with input from a senior researcher in cases of disagreement. Following initial title and abstract screens, full publications were obtained and these were also screened by two researchers with similar resolution of disagreement. Congress proceedings and bibliographies of included articles were searched by a single researcher. Data from included publications were extracted by one researcher and were reviewed by a second researcher. Reported mean values for the HRQoL instruments were used to compare findings of the included publications. The risk of bias in individual studies was assessed using the Newcastle–Ottawa scale. The quality of studies was scored based on three categories: selection of study groups, comparability of groups, and ascertainment of outcomes of interest. Additional non-systematic ad hoc searches were performed in PubMed to obtain mean HRQoL reference values for comparing the HRQoL of patients with mPaC with that of the general population.
HRQoL Instrument Definitions
EORTC QLQ-C30 and QLQ-PAN26
The QLQ-C30 evaluates five functional scales (physical, role, emotional, cognitive, and social), nine symptom scales (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties) and a GHS scale, each scored on a scale from 0 to 100, with higher GHS and functional scores indicating better HRQoL and higher symptom scores indicating greater symptom burden.7 The QLQ-PAN26 is an appendix module of the QLQ-C30 that includes 26 pancreatic cancer-specific items covering the domains of symptoms, adverse events, and emotional issues.8 For all items except satisfaction with healthcare, a higher score reflects worse HRQoL.
FACT-G and FACT-Hep
The FACT-G is a 27-item self-report instrument that assesses four domains of HRQoL – physical (seven items), social (seven items), emotional (six items), and functional (seven items). Each item is scored on a 5-point scale ranging from 0 (not at all) to 4 (very much). The final score is the sum of these domain scores, with a possible total score greater than 100.9 The specific tool for assessing hepatobiliary and pancreatic diseases, FACT-Hep, is the sum of the FACT-G score plus an additional disease-specific module (18 items).10
EQ-5D-5L
The EQ-5D-5L is composed of five dimensions – mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.11 Each dimension is measured in five levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. Patients are asked to self-assess and select the most accurate statement describing their condition for each scale. The scale ranges from 0 to 1, with higher scores indicating better HRQoL.
BRE 43 QOL
The BRE 43 QOL is similar to the QLQ-C30 and asks questions regarding basic performance status, associated health issues, pain level, mental status, and treatment effect on family and social life. There are 45 questions assessing different aspects of HRQoL, with scores ranging from 1 (not at all) to 4 (very much), and two questions evaluating overall HRQoL, with scores ranging from 1 (very poor) to 7 (excellent).
KPS and ZPS
The KPS is a physician-rated scale that classifies patients according to their functional impairment, ranging from 0 (dead) to 100 (well-functioning).12 The ZPS also describes patients’ level of functioning according to their ability to care for themselves; this scale ranges from 0 (perfect health) to 5 (dead).
Results
Identified Studies and HRQoL Instruments
A total of 30 articles assessing the HRQoL of patients with mPaC met the inclusion criteria (Figure 1).4,13–41 These publications reported results from 27 different studies published between 2008 and 2021 (summarized in Table 2). Twenty-nine of the 30 references were full-text publications, and one was a conference abstract. There were 10 randomized controlled trials,4,15,17,18,20,23,27,28,38,39 three single-arm trials,19,22,33 one prospective study,25 nine prospective observational studies,13,16,21,29,32,34,36,37,41 three retrospective observational studies,30,31,40 and one cross-sectional study.35 The studies included data from newly diagnosed and/or previously treated patients with mPaC. As assessed using the Newcastle–Ottawa scale, from the 27 identified studies, 17 (63.0%) had a low risk of bias (7–9 points), nine (33.3%) had a high risk of bias (4–6 points), and none had a very high risk of bias (0–3 points) (Table 2). The conference abstract did not present sufficient information for determining the risk of bias using the Newcastle–Ottawa scale.
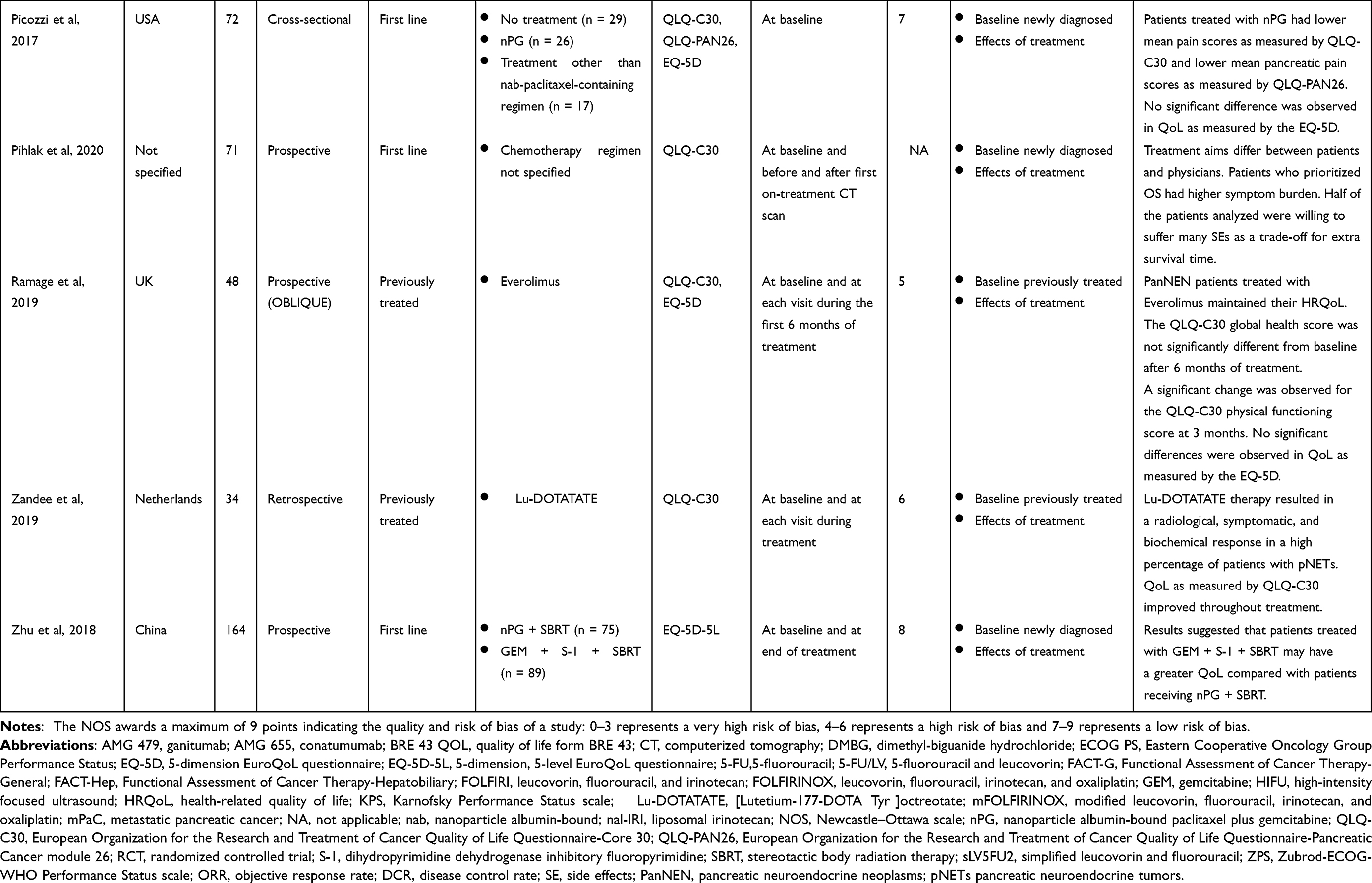 |
Table 2 Overview of Studies Evaluating the HRQoL of Patients with mPaC |
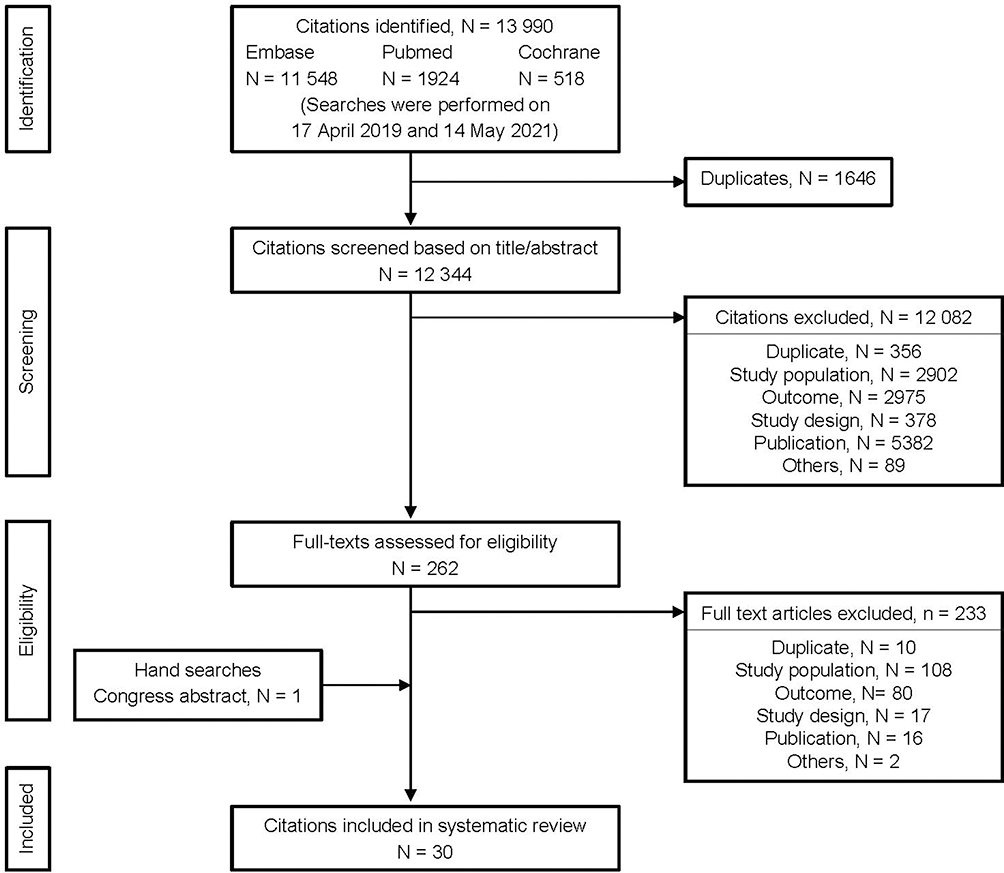 |
Figure 1 Preferred reporting items for systematic reviews and meta-analysis for the systematic review. |
HRQoL was assessed using the European Organization for the Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-Core 30 (QLQ-C30) in 20 studies, the EORTC Quality of Life Questionnaire-Pancreatic Cancer module 26 (QLQ-PAN26) in three studies, the Functional Assessment of Cancer Therapy-General (FACT-G) in one study, the Functional Assessment of Cancer Therapy-Hepatobiliary (FACT-Hep) in three studies, the 5-dimension EuroQoL questionnaire (EQ-5D) or the 5-dimension, 5-level EuroQoL questionnaire (EQ-5D-5L) in four studies, the quality of life form BRE 43 (BRE 43 QOL) in one study, the Karnofsky Performance Status scale (KPS) in two studies, and the Zubrod-ECOG-WHO Performance Status scale (ZPS) in one study (see Methods for comprehensive definitions7–12). Baseline HRQoL scores were reported for newly diagnosed patients in 10 studies and for previously treated patients in eight studies, and one study recorded baseline HRQoL scores for both newly diagnosed and previously treated patients. In total, 26 studies investigated the effects of treatment on HRQoL.
For the general population, a total of 19 publications reporting HRQoL data from various geographical regions were identified from non-systematic searches. HRQoL was assessed using QLQ-C30 in 10 publications (15 European countries, Canada, the USA, Australia, and Colombia),42–51 FACT-G in three publications (Sweden and the USA),52–54 and the 5-dimension, 3-level EuroQoL questionnaire and EQ-5D-5L in six publications (Canada, the USA, Australia, Brazil, Hong Kong, and Vietnam).55–60 Supplementary Table 7 summarizes publications reporting HRQoL data for the general population.
Baseline HRQoL Scores of Patients with mPaC and the General Population
QLQ-C30
Based on the results of 15 studies that measured mean baseline QLQ-C30 global health status (GHS) for patients with mPaC, individuals with newly diagnosed disease had lower mean QLQ-C30 GHS scores (range, 41.7–63.2)14–16,20,24,25,35,36 than those reported for the general population (range, 66.1–77.1).42–51 Among studies assessing QLQ-C30 GHS for previously treated patients,13,16,19,26,29,32,37,39 some found mean scores that were lower than those of the general population (43.8–58.3 vs 66.1–77.1) and some that were similar to those of the general population (70.4–75.0 vs 66.1–77.1, Figure 2). Mean baseline scores for all functional scales (physical, emotional, role, social, and cognitive function) of newly diagnosed patients, when reported,14–16,20,24,25,35,36 were also generally lower than those of the general population42–51 (Figure 2). Scales showing the greatest decrease in function compared with the general population were emotional (41.7–74.4 vs 73.9–87.6), role (59.2–66.4 vs 80.8–92.3), and social (63.2–73.4 vs 84.8–92.7). Scores for the other two functional scales, physical (71.5–86.7 vs 81.7–92.2) and cognitive (66.7–83.3 vs 83.5–91.2), also showed impairment compared with the general population. For previously treated patients, scales with scores showing an overall poorer HRQoL compared with the general population across the different studies were social (56.3–77.3 vs 84.8–92.7) and role (53.2–76.0 vs 80.8–92.3) function, except for in one study, by Ueno et al39 (Figure 2). Among studies providing QLQ-C30 GHS scores for functional scales for previously treated patients, some found lower scores and others similar scores compared with the general population. In some studies, mean scores were reported that were higher than those of the general population for emotional (56.5–91.7 vs 73.9–87.6), social (56.3–100.0 vs 84.8–92.7), and cognitive (69.4–100.0 vs 83.5–91.2) function scales.
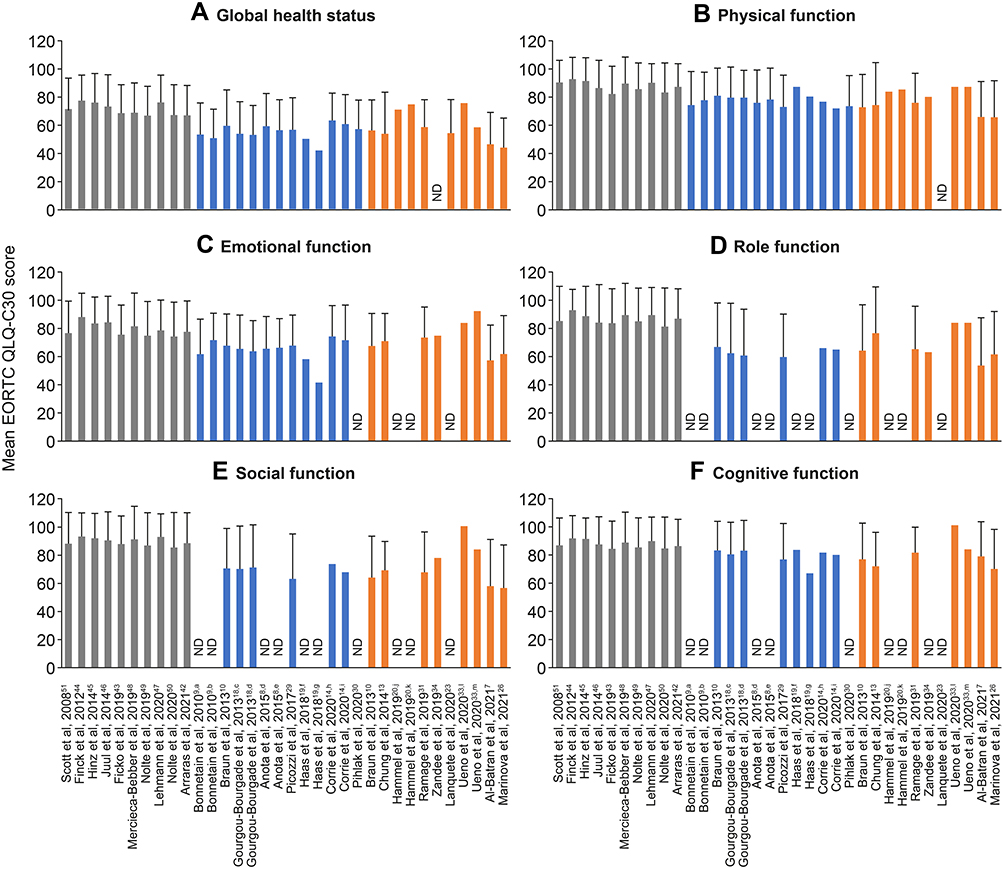 |
Figure 2 Baseline EORTC QLQ-C30 GHS/functional scores for the general population and newly diagnosed and previously treated patients with mPaC. Mean EORTC QLQ-C30 scores are shown for global health status (A), physical function (B), emotional function (C), role function (D), social function (E), and cognitive function (F). Higher scores indicate better health status and functioning. Gray bars represent reference values for the general population, blue bars represent data for newly diagnosed patients and orange bars represent data for previously treated patients. Error bars represent standard deviations. Treatment regimens: a5-FU/cisplatin followed by GEM; bGEM followed by 5-FU/cisplatin; cFOLFIRINOX; dGEM; eFOLFIRI plus GEM; fGEM plus erlotinib; gGEM plus erlotinib followed by FOLFIRINOX; hnab-paclitaxel plus GEM administered concomitantly; inab-paclitaxel plus GEM administered sequentially; jmaintenance olaparib; kplacebo; lnal-IRI plus 5-FU/LV; m5-FU/LV. Abbreviations: EORTC QLQ-C30, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; 5-FU, 5-fluorouracil; 5-FU/LV, 5-fluorouracil and leucovorin; FOLFIRI, leucovorin, fluorouracil, and irinotecan; FOLFIRINOX, leucovorin, fluorouracil, irinotecan, and oxaliplatin; GEM, gemcitabine; GHS, global health status; mPaC, metastatic pancreatic cancer; nab, nanoparticle albumin-bound; nal-IRI, liposomal irinotecan. |
A generally greater symptom burden was reported in patients with mPaC than in the general population42–51 for both newly diagnosed and previously treated patients13–16,19,20,24–26,32,35–37,39,40 (Figure 3). The most severe baseline symptom scores (ie higher mean scores) reported for newly diagnosed and previously treated patients compared with the general population were for pain (newly diagnosed patients, 33.3–66.7; previously treated patients, 14.9–46.7; general population, 13.6–27.6), fatigue (newly diagnosed patients, 33.3–55.6; previously treated patients, 27.3–51.4; general population, 14.0–31.9), appetite loss (newly diagnosed patients, 34.1–51.7; previously treated patients, 12.1–44.6; general population, 4.4–10.1), and insomnia (newly diagnosed patients, 35.7–47.1; previously treated patients, 14.6–43.6; general population, 12.6–28.3). Constipation (newly diagnosed patients, 23.9–38.7; previously treated patients, 10.9–27.8; general population, 5.2–15.3), financial difficulties (newly diagnosed patients, 9.4–31.3; previously treated patients, 17.0–31.6; general population, 5.1–11.3), diarrhea (newly diagnosed patients, 12.1–29.4; previously treated patients, 8.3–36.7; general population, 4.9–10.4), dyspnea (newly diagnosed patients, 14.9–22.4; previously treated patients, 9.8–33.7; general population, 6.0–19.7), and nausea/vomiting (newly diagnosed patients, 14.3–17.0; previously treated patients, 7.3–17.2; general population, 2.0–6.2) were worse for newly diagnosed and previously treated patients than for the general population. Although the symptom burden was generally greater for previously treated patients than for the general population, it was generally less severe in this group than in newly diagnosed patients, with the exception of financial difficulties (Figure 3).
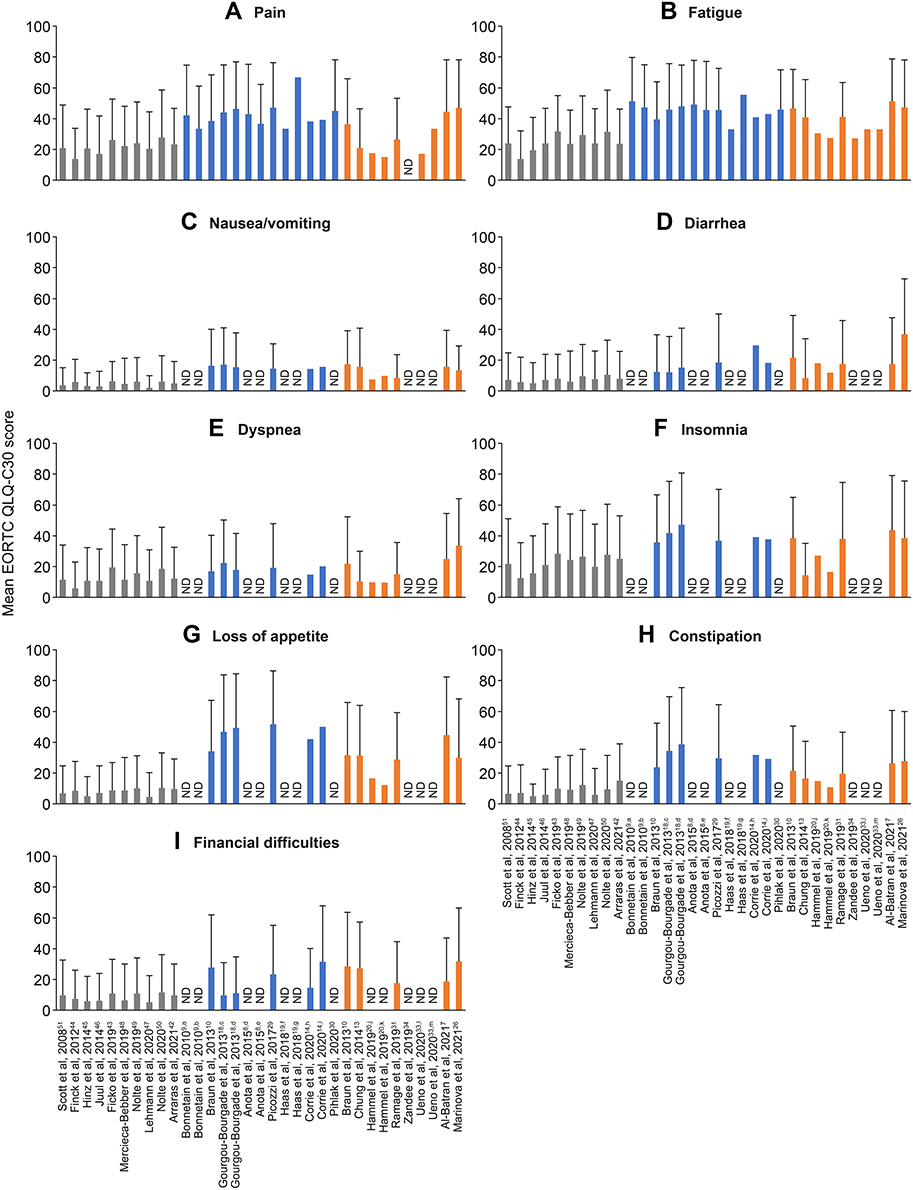 |
Figure 3 Baseline EORTC QLQ-C30 symptom scores for the general population and newly diagnosed and previously treated patients with mPaC. Mean EORTC QLQ-C30 scores are shown for pain (A), fatigue (B), nausea/vomiting (C), diarrhea (D), dyspnea (E), insomnia (F), loss of appetite (G), constipation (H), and financial difficulties (I).Higher scores indicate a greater symptom burden. Gray bars represent reference values for the general population, blue bars represent data for newly diagnosed patients and Orange bars represent data for previously treated patients. Error bars represent standard deviations. Treatment regimens: a5-FU/cisplatin followed by GEM; bGEM followed by 5-FU/cisplatin; cFOLFIRINOX; dGEM; eFOLFIRI plus GEM; fGEM plus erlotinib; gGEM plus erlotinib followed by FOLFIRINOX; hnab-paclitaxel plus GEM administered concomitantly; inab-paclitaxel plus GEM administered sequentially; jmaintenance olaparib; kplacebo; lnal-IRI plus 5-FU/LV; m5-FU/LV. Abbreviations: EORTC QLQ-C30, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; 5-FU, 5-fluorouracil; 5-FU/LV, 5-fluorouracil and leucovorin; FOLFIRI, leucovorin, fluorouracil, and irinotecan; FOLFIRINOX, leucovorin, fluorouracil, irinotecan, and oxaliplatin; GEM, gemcitabine; mPaC, metastatic pancreatic cancer; nab, nanoparticle albumin-bound; nal-IRI, liposomal irinotecan. |
FACT-G
In the two studies examining FACT-G scores, patients with mPaC had worse overall HRQoL than the general population (39.0–82.6 vs 77.7–86.0). Contrasting results were found when comparing reported mean scores for the individual FACT-G scales (physical, social, functional, and emotional well-being) of newly diagnosed patients with mPaC17,28 with those of the general population52–54 (Figure 4). Ibraimi et al28 (N = 34) reported consistently lower scores than those of the general population for all four scales, while Cella et al17 reported different scores according to ECOG PS. Patients with a PS of 0 (n = 40) had a lower mean emotional well-being score than the general population (16.7 vs 17.0–19.9), and those with a PS of 1 (n = 65) had lower mean scores for physical (18.9 vs 22.7–24.0), emotional (15.6 vs 17.0–19.9) and functional (14.7 vs 18.5–22.0) well-being scales, indicating worse HRQoL in these domains than in the general population. Interestingly, regardless of PS, patients with mPaC had higher mean social well-being scores than the general population (23.5–24.1 vs 17.5–21.0) in this study.
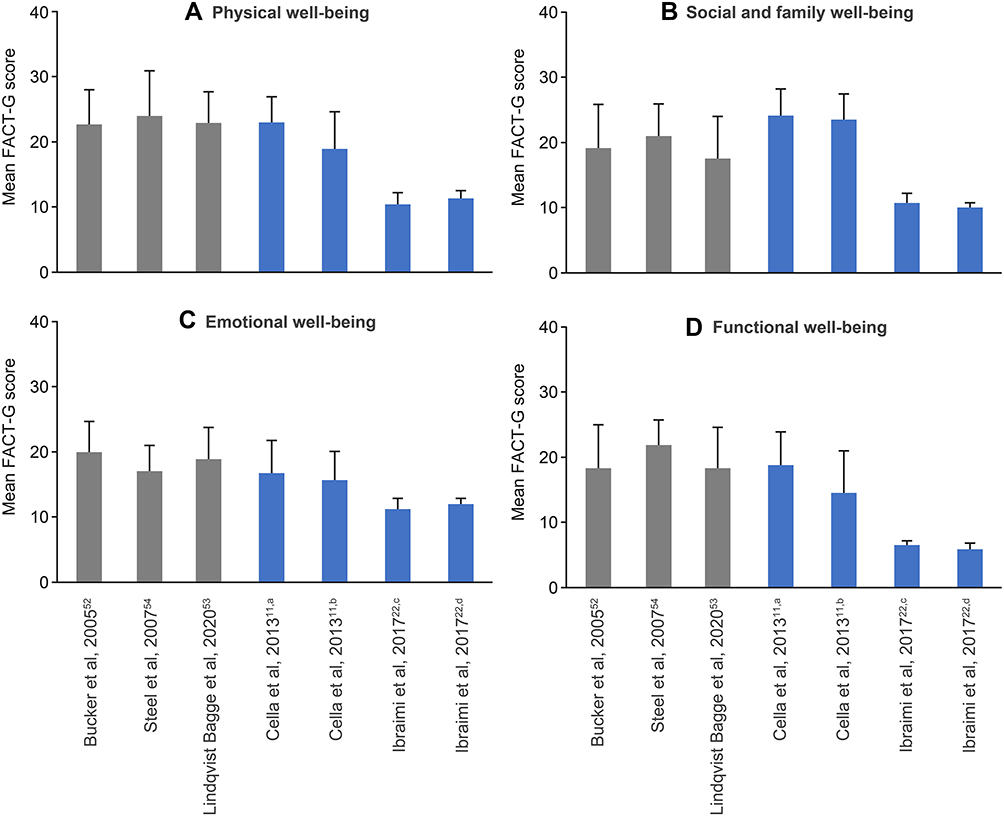 |
Figure 4 Baseline FACT-G scores for the general population and newly diagnosed patients with mPaC. Mean FACT-G scores are shown for physical well-being (A), social and family well-being (B), emotional well-being (C), and functional well-being (D). Higher scores indicate better health-related quality of life. Gray bars represent reference values for the general population and blue bars represent data for newly diagnosed patients. Error bars represent standard deviations. aPatient group: ECOG PS = 0; bpatient group: ECOG PS = 1; ctreatment regimen: GEM; dtreatment regimen: FOLFIRINOX. Abbreviations: ECOG PS, Eastern Cooperative Oncology Group Performance Status; FACT-G, Functional Assessment of Cancer Therapy-General; FOLFIRINOX, leucovorin, fluorouracil, irinotecan, and oxaliplatin; GEM, gemcitabine; mPaC, metastatic pancreatic cancer. |
EQ-5D
From the three articles that reported baseline health state utility scores using EQ-5D or ED-5D-5L for patients with mPaC,35,37,41 both newly diagnosed and previously treated patients had lower mean health utility scores (0.46–0.75 and 0.72, respectively) than the general population (0.80–0.92)55–60 (Figure 5). Picozzi et al35 (n = 28) and Ramage et al37 (n = 44) reported higher mean health state utility scores than Zhu et al,41 however, the latter investigators measured this score in a larger group of patients (N = 164).
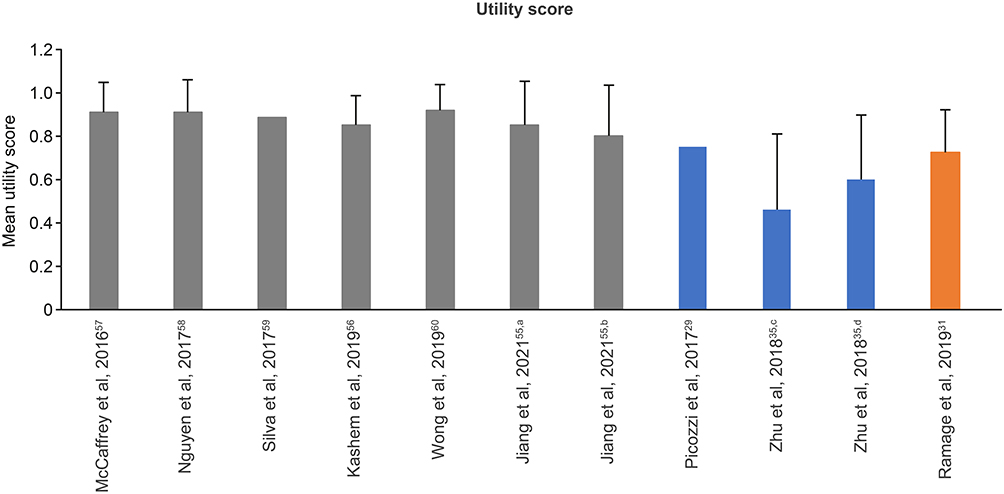 |
Figure 5 Baseline EQ-5D scores for the general population and newly diagnosed and previously treated patients with mPaC. Higher scores indicate better health-related quality of life. Gray bars represent reference values for the general population, blue bars represent data for newly diagnosed patients and orange bars represent data for previously treated patients. Error bars represent standard deviations. aAssessment face-to-face; bassessment online; ctreatment regimen: nPG plus SBRT; dtreatment regimen: GEM plus S-1 plus SBRT. Abbreviations: EQ-5D, 5-dimension EuroQoL questionnaire; GEM, gemcitabine; mPaC, metastatic pancreatic cancer; nPG, nanoparticle albumin-bound paclitaxel plus gemcitabine; S-1, dihydropyrimidine dehydrogenase inhibitory fluoropyrimidine; SBRT, stereotactic body radiation therapy. |
Response to Therapy
Studies finding changes in HRQoL in response to chemotherapy in patients with mPaC mainly investigated treatments with oxaliplatin-containing regimens,4,24,28,34 fluorouracil-based regimens,14,15,27,38,39 nPG,13,18,20,22,35,41 and other GEM-based regimens.25,30,31,33 Other studies evaluated the effect on HRQoL of high-intensity focused ultrasound (HIFU),32 [Lutetium-177-DOTA0-Tyr3]octreotate (177Lu-DOTATATE),40 everolimus,37 cytokine-induced killer (CIK) cells,19 and maintenance therapy with olaparib.23,26 Details are provided in Supplementary Table 8.
Oxaliplatin-Containing Regimens
Three studies evaluated HRQoL in patients with mPaC receiving oxaliplatin-containing regimens. Two of these compared FOLFIRINOX with GEM monotherapy: the French PRODIGE 4/ACCORD 11 trial (N = 342)4,24 and a smaller study conducted in Kosovo (N = 34).28 There were no statistically significant differences in HRQoL between the two groups at baseline in either study, as assessed using QLQ-C30 and FACT-Hep, respectively. In the PRODIGE 4/ACCORD 11 study, improvements in GHS were observed between baseline and 6 months in the FOLFIRINOX group (p < 0.001), while GHS in the GEM monotherapy group remained stable. Both treatment groups showed improvements in emotional function (p < 0.001) and deterioration in symptom scores for pain, insomnia, anorexia, and constipation (all p < 0.02).24 In the Kosovo study, improvements in HRQoL were significantly greater in the FOLFIRINOX group than in the GEM group for all FACT scales after 12 weeks of treatment (all p < 0.028).
A further study evaluated the effect of irinotecan combined with oxaliplatin and the novel dihydropyrimidine dehydrogenase inhibitory fluoropyrimidine S-1 as first-line treatment in a group of Chinese patients (N = 41).34 Using the KPS, this study found that the HRQoL of 63.4% of patients “apparently improved”, “improved”, or “remained stable” (7.3%, 24.4%, and 31.7% of patients, respectively) at each follow-up visit (median follow-up, 13 months) compared with baseline, while HRQoL in the remaining patients deteriorated.
Fluorouracil-Based Regimens
Four studies assessed the effects of fluorouracil-based regimens on HRQoL: a French Phase 2 study comparing the efficacy of leucovorin, fluorouracil, and irinotecan (FOLFIRI) followed by fixed-dose-rate GEM, with fixed-dose-rate GEM alone as first-line treatment of mPaC,14,38 a French Phase 3 study comparing treatment with 5-fluorouracil(5-FU)/cisplatin followed by GEM with the reverse sequence as first-line treatment of mPaC,15 and two studies comparing therapy with liposomal irinotecan plus 5-FU and leucovorin (5-FU/LV) versus 5-FU/LV alone in patients previously treated with a GEM-based regimen.27,39
In the French phase 2 study, 49 patients received FOLFIRI every 14 days for 2 months followed by fixed-dose-rate GEM on days 1, 8, 15, 29, 36, and 43; this sequence (FOLFIRI followed by GEM) continued until disease progression or limiting toxicity occurred. In the second arm of the study, 49 patients received fixed-dose-rate GEM alone on days 1, 8, 15, 29, 36, and 43 until disease progression or unacceptable toxicity occurred. The median follow-up of this study was 32.5 months. Patients in the FOLFIRI plus GEM group had a longer time until definitive HRQoL deterioration than those in the GEM alone group for QLQ-C30 physical function (HR, 0.47), nausea/vomiting (HR, 0.47), pain (HR, 0.47), dyspnea (HR, 0.41), insomnia (HR, 0.24), and appetite loss (HR, 0.47),38 and longer HRQoL deterioration-free survival for GHS (HR, 0.52), emotional function (HR, 0.35), and pain (HR, 0.50).14 In the French phase 3 study, 102 patients received 5-FU/cisplatin followed by GEM and 100 patients received the reverse sequence. In both arms of the study, patients experienced a definitive HRQoL deterioration over the course of follow-up (median follow-up, 44.0 months) assessed using QLQ-C30 GHS, with no significant difference between the treatment arms (p = 0.50).15
The first of the two studies comparing liposomal irinotecan plus 5-FU/LV with 5-FU/LV alone in patients previously treated with a GEM-based regimen was the phase 3 NAPOLI-1 trial (N = 236).27 Over 12 weeks of treatment, median QLQ-C30 GHS and scores for the majority of functional and symptom scales remained stable in both treatment groups, except for fatigue, which deteriorated in the liposomal irinotecan plus 5-FU/LV arm, and cognitive function and pain, which improved in the 5-FU/LV arm. The second study was a Japanese phase 2 trial (N = 79) that found small differences between arms in median change from baseline in QLQ-C30 GHS (0 vs +8), role function (0 vs +33), and fatigue (0 vs −11).39
nPG
Six studies investigated the effect of nPG on HRQoL. One study evaluated the effect of nPG in patients at different stages of disease,35 one compared the efficacy and other outcomes of GEM plus nab-paclitaxel given sequentially with GEM plus nab-paclitaxel given concomitantly,20 and two compared nPG with other treatments.18,41 The QoliXane study evaluated the HRQoL of patients receiving nPG as first-line treatment in a real-world setting (N = 600).13 Five hundred eighty-eight (98%) patients had completed QLQ-C30 questionnaires at baseline. Among these, 19% of patients maintained (improved or stable) their QLQ-C30 GHS scores and 9% of patients showed deterioration after 6 months of treatment (the remaining patients were non-evaluable). The phase 2 BIBABRAX study assessed the effect of nPG on elderly patients with untreated locally advanced pancreatic cancer or mPaC (N = 80).22 Of the 60 evaluable patients, 61.7% showed QLQ-C30 GHS deterioration between baseline and a maximum of 2 months after the last dose of study treatment was administered.
A US cross-sectional study assessed the effect of nPG on HRQoL of patients at different disease stages: newly diagnosed treatment-naive patients (n = 29), patients who had achieved a partial response or stable disease after at least three cycles of first-line nPG (n = 26), and patients with disease progression during at least one line of chemotherapy who were not currently receiving nab-paclitaxel (n = 17).35 The only difference observed was for the QLQ-C30 symptom scale of pain, with significantly lower scores for the last two groups than for treatment-naive patients (both p = 0.02). These two groups also had significantly lower pancreatic pain scores than treatment-naive patients (both p = 0.02), as assessed using QLQ-PAN26. The phase 2 SIEGE study evaluated whether sequential scheduling of nab-paclitaxel plus GEM might improve efficacy and other outcomes in patients with mPaC.20 In total, 75 patients received nab-paclitaxel plus GEM concomitantly and 71 patients received nab-paclitaxel plus GEM sequentially (GEM administered 24 hours after nab-paclitaxel). The median follow-up of this study was 21.4 months. QLQ-C30 GHS was generally stable and was similar between arms over time. Patients receiving nab-paclitaxel plus GEM sequentially had greater improvements in appetite at week 12 (p = 0.047) and less altered bowel habits at week 26 (p = 0.003) than those receiving nab-paclitaxel and GEM concomitantly.
Of the two studies that compared nPG with other treatments, one carried out in China assessed the effect of nPG (n = 75) compared with that of GEM plus S-1 (n = 89) on HRQoL (both treatments were given after radiotherapy).41 Median follow-up was 10.0 and 11.0 months for nPG and GEM plus S-1, respectively. After treatment, only patients in the GEM plus S-1 group reported improvement in HRQoL compared with baseline as measured by EQ-5D-5L (p < 0.001). In the phase 2 AFUGEM GERCOR study, the HRQoL of patients receiving nPG (n = 39) was compared with that of patients receiving nab-paclitaxel plus simplified leucovorin and fluorouracil (n = 75).18 Patients in the latter arm had longer HRQoL deterioration-free survival for GHS (HR, 0.80), all functional scales (HR, 0.64–0.82), and the majority of symptom scales (HR, 0.61–0.79), except for constipation (HR, 1.0), than those in the nPG arm.
Other GEM-Based Regimens
Four studies assessed the effect of other GEM-based regimens on HRQoL: a phase 2 study evaluating the response to GEM and etoposide in patients with locally advanced pancreatic cancer or mPaC,33 a retrospective study comparing the clinical efficacy of GEM plus S-1 with S-1 alone in senile patients with mPaC,31 a retrospective study assessing the efficacy of GEM in combination with dimethyl-biguanide hydrochloride (DMBG) compared with GEM alone in patients with advanced pancreatic cancer,30 and a phase 2 study assessing the efficacy of GEM plus erlotinib compared with FOLFIRINOX in patients with mPaC.25
In the phase 2 study that evaluated the response rate to GEM and etoposide, patients with locally advanced disease (n = 7) or mPaC (n = 33) received treatment for eight cycles (21 days per cycle). Of the evaluable patients with mPaC (n = 28), HRQoL improved in 11 individuals (39.3%) and was stable in two individuals (7.1%), as assessed using the BRE 43 QOL. In the retrospective study, 32 patients received GEM plus S-1 and 32 patients received S-1 alone. After treatment, both groups had higher scores for all QLQ-C30 functional scales relative to scores at baseline (all p < 0.001). Patients in the GEM plus S-1 group had significantly greater HRQoL improvements for all functional scales than those in the S-1 group (all p < 0.001). In another retrospective study, 32 patients received GEM in combination with DMBG and 33 patients received GEM alone. After treatment, patients in the GEM plus DMBG group had better HRQoL than those in the GEM alone group, with significantly higher KPS scores (p < 0.05) and significantly lower ZPS scores (p < 0.05). In the prospective observational phase 2 study, patients received GEM plus erlotinib for 4 weeks (N = 117). After this run-in phase, patients who developed skin rash (n = 90) continued receiving the same treatment for a median duration of 3.7 months, and those who did not develop skin rash (n = 27) switched to FOLFIRINOX therapy and received treatment for a median duration of 3.0 months. Patients whose treatment was switched to FOLFIRINOX had significantly worse QLQ-C30 GHS (p = 0.004), physical function (p = 0.021), emotional function (p = 0.003), and cognitive function (p = 0.008) than those who continued treatment with GEM plus erlotinib. Patients who received FOLFIRINOX also reported a higher symptom burden for fatigue (p = 0.003) and pain (p = 0.005) than those who continued treatment with GEM plus erlotinib.
Other Regimens
Eight studies evaluated the effect of other treatments on the HRQoL of patients with pancreatic cancer: a Spanish prospective observational study assessing the evolution of HRQoL in patients with mPaC receiving different treatment types as first-line chemotherapy,29 a prospective observational study investigating patients’ and physicians’ perspectives on treatment decision-making,36 a prospective observational study evaluating the HRQoL and symptom burden of patients with advanced pancreatic cancer treated with HIFU,32 a US retrospective study evaluating whether changes in HRQoL could predict survival in patients with mPaC,16 a US prospective observational study assessing the HRQoL of patients with various stages of pancreatic cancer undergoing different treatments,21 a phase 2 study evaluating the efficacy of adoptive immunotherapy with ex vivo-expanded CIK cells in patients who had disease progression after receiving GEM-based chemotherapy,19 and two studies assessing the HRQoL of patients with metastatic pancreatic neuroendocrine neoplasms receiving treatment with everolimus or 177Lu-DOTATATE.37,40
In the Spanish prospective observational study, evolution of HRQoL was evaluated in 113 patients with mPaC receiving first-line treatment with nPG (64.6%), GEM monotherapy (18.6%), FOLFIRINOX or modified FOLFIRINOX (12.4%), and other combinations (4.4%) during a median treatment duration of 3.9 months (maximum follow-up, 18 months). QLQ-C30 HRQoL scores significantly improved for all patients for GHS and the symptom scales for pain, appetite loss, insomnia, nausea/vomiting, and constipation (all p < 0.005). No significant changes were observed for HRQoL assessed with the EQ-5D. In the prospective observational study that investigated patients’ and physicians’ perspectives on treatment decision-making, HRQoL deteriorated over time for QLQ-C30 physical function (p = 0.003) and pain (p = 0.02) in 71 patients with mPaC undergoing first-line treatment. In another prospective observational study, 80 patients with advanced pancreatic cancer received standard chemotherapy and HIFU (up to two sessions) in a week without a chemotherapy cycle. After 6 months of HIFU, patients showed improvements in QLQ-C30 GHS (p = 0.02), physical function (p = 0.02), emotional function (p = 0.01), social function (p = 0.009), pain (p = 0.043), fatigue (p = 0.012), and appetite loss (p = 0.011). In the US retrospective study, 186 patients received a treatment combination with surgery, radiation, and chemotherapy (regimens not specified). Changes from baseline to 3 months were not statistically tested in this study. However, improvements in HRQoL QLQ-C30 scores were observed for emotional function, pain, insomnia, and constipation, and deterioration for GHS, physical function, role function, cognitive function, social function, fatigue, dyspnea, and financial difficulties. In the US prospective observational study, 30 of the 92 patients with various stages of pancreatic cancer who underwent different treatments had mPaC. This cohort of patients had a clinically meaningful HRQoL deterioration from baseline to the 3- and 6-month follow-up visits as assessed using FACT-G and FACT-Hep. In the phase 2 study, 20 patients received adoptive immunotherapy with ex vivo-expanded CIK cells after undergoing GEM-based chemotherapy as first-line treatment. After treatment, QLQ-C30 pain and insomnia significantly worsened (p = 0.004 and p = 0.002, respectively) and QLQ-PAN26 pancreatic pain and altered bowel habits significantly improved (p = 0.012 and p = 0.003, respectively).
Of the two studies that assessed the HRQoL of patients with metastatic pancreatic neuroendocrine neoplasms, the Phase 4 OBLIQUE trial evaluated the effect of everolimus on HRQoL in 48 individuals receiving treatment for a median duration of 27.8 months (median follow-up, 22.0 months). No significant change in QLQ-C30 GHS score from baseline to 6 months after treatment initiation was observed. The second study was a retrospective analysis evaluating safety and efficacy in patients with functioning pancreatic neuroendocrine tumors receiving 177Lu-DOTATATE (N = 34). The median follow-up for this study was 39.3 months. After 3 months from the last treatment cycle, there were significant improvements from baseline in QLQ-C30 GHS (p = 0.002), physical function (p = 0.008), role function (p = 0.006), emotional function (p = 0.002), and social function (p = 0.047), and a significant worsening of fatigue (p = 0.02).
Maintenance Therapy
In the phase 3 POLO study, patients with mPaC and a germline BRCA mutation whose disease had not progressed after first-line platinum-based chemotherapy received active maintenance treatment with olaparib for a median duration of 6.0 months (n = 92) or placebo for a median duration of 3.7 months (n = 62).23 The median follow-up in this study was 9.1 months in the olaparib arm and 3.8 months in the placebo arm. No significant change in HRQoL from baseline was observed in either arm as assessed with QLQ-C30, and there was no significant difference in the mean GHS change from baseline between the two trial arms. A significant between-group difference of −4.45 points was observed in the adjusted mean change from baseline for the physical function scale (p = 0.04).26
Discussion
This systematic review highlights the growing body of literature describing HRQoL in patients with mPaC, indicating that researchers and clinicians are increasingly incorporating effects on HRQoL as an endpoint in studies. A similar finding was reported in a systematic review that looked at HRQoL in patients with breast cancer.61 In the publications included in this systematic review, HRQoL was evaluated as part of a variety of study designs (clinical trials and prospective, retrospective, and cross-sectional observational studies), and was measured using a diverse set of instruments assessing the functional level and symptom burden of patients with mPaC.
The HRQoL instrument employed most often was the EORTC QLQ-C30, followed by EQ-5D and FACT-G. Baseline scores measured using these instruments provide the necessary data with which to understand how the HRQoL of patients with mPaC before and after treatment compares with that of the general population. QLQ-C30 results showed that overall, newly diagnosed patients with mPaC have poorer GHS, lower emotional, role, and social function, and a greater symptom burden for pain, fatigue, appetite loss, and insomnia than the general population. Our findings corroborate those from a recent study comparing new systematically derived EORTC QLQ-C30 reference scores for treatment-naive patients with mPaC with general population “EORTC QLQ-30 norm” scores.62 This revealed poorer GHS, lower role and social functioning, and more severe symptoms of pain, fatigue, appetite loss, nausea and vomiting, constipation and insomnia in patients with mPaC compared with the general population.62 A study using FACT-G found that newly diagnosed patients had lower HRQoL across all domains (physical, social, functional, and emotional well-being) than the general population.28 However, a second study using FACT-G determined that patients with a worse performance status (ECOG PS of 1) had lower HRQoL than the general population for physical, emotional, and functional well-being, but those with a better performance status (ECOG PS of 0) had lower scores than the general population in only the emotional well-being domain.17 EQ-5D results also indicated that newly diagnosed patients with mPaC had worse HRQoL than the general population. Overall, these results confirm that mPaC is an aggressive malignancy that decreases the quality of life of individuals who develop it.
Studies providing baseline scores for previously treated patients can help us to understand how mPaC treatment preserves or improves patients’ HRQoL. QLQ-C30 results showed that previously treated patients had worse GHS, social function, and role function than the general population and, as for newly diagnosed patients, a greater symptom burden for pain, fatigue, appetite loss, and insomnia than the general population. EQ-5D results also showed that previously treated patients had worse HRQoL than the general population. Although QLQ-C30 and EQ-5D baseline scores of previously treated patients were lower than those of the general population, they were generally higher than corresponding scores for newly diagnosed patients. Additionally, some scores for previously treated patients indicated similar or even better HRQoL than those of the general population. Together, these results indicate that, in general, treatments seem to be preserving or improving the HRQoL of patients with mPaC.
Similar outcomes were reported among some studies assessing the effect of cancer treatment on HRQoL. In these, individuals who had received treatment showed improvements or maintenance of HRQoL compared with treatment-naive patients.16,29,35,62 Notably, patients with mPaC responsive to first-line chemotherapy enrolled in the POLO study showed markedly better HRQoL than treatment-naive patients, as reported in the literature.62 However, other studies showed HRQoL deterioration.21 The impact of therapy on HRQoL reflects the combined effects of the reduction in disease-related symptoms and the occurrence of treatment-related toxicities, and is thus a relevant measure of the potential overall benefit of a specific treatment for the patient. Our findings are in line with those of two other systematic literature reviews that evaluated the effect of treatment on the HRQoL of patients with pancreatic cancer. The first review found that 11 of the 14 identified studies assessing the effect of chemotherapy on HRQoL found improvement or preservation of HRQoL scores compared with baseline, with the rest showing HRQoL deterioration.63 The second review evaluated the effect of pancreatic resection on the HRQoL of patients with early-stage pancreatic cancer.64 Based on the 39 eligible studies, this review found that although there was a decline in HRQoL immediately after surgery, it recovered after 3–6 months and then remained stable over the long term.
The evidence identified in this systematic review suggests that some chemotherapy regimens improve HRQoL in patients with mPaC. Different studies have compared the effect of FOLFIRINOX on HRQoL with that of GEM and found that patients receiving FOLFIRINOX have greater improvements in HRQoL than those receiving GEM. Improvements in HRQoL over the course of treatment have also been reported for nPG and other GEM-based chemotherapies. Evidence suggests that 5-FU regimens that included irinotecan may preserve HRQoL better than 5-FU or GEM monotherapy; however, they did not appear to improve HRQoL compared with baseline.14,27,38
HRQoL scores are clinically important in patients with mPaC, where life expectancy is short. Standardization of the tools used to measure HRQoL would help to provide a more cohesive overview. This would help clinicians select the most appropriate therapeutic strategy to balance survival with QoL on a patient-by-patient basis, and would also help patients to make informed decisions about their own care. Whilst several cancer treatments have been shown to improve or maintain HRQoL, patients’ quality of life decreases upon disease progression. Therefore, it is vital that future clinical trials consider this alongside other primary outcomes such as OS. Furthermore, systematic evaluations should be performed to ensure that patient HRQoL is managed throughout treatment.
This literature review had a number of limitations. Fifteen of the 27 studies included in this study involved fewer than 100 patients and baseline characteristics of the patient populations differed between studies, limiting the validity of comparisons between them. Additionally, there were differences between studies in the frequency and timing of assessments, and some publications provided only limited information regarding HRQoL data collection and analyses. Studies investigating the effects of interventions generally had a short follow-up of only 3 or 6 months, and most publications did not report how many patients remained on study or completed the HRQoL assessment at each follow-up appointment.
In conclusion, despite the limitations of the available literature, there is a growing body of evidence reporting the HRQoL of patients with mPaC and the impact on HRQoL of currently available therapeutic interventions. Patients with mPaC generally have lower HRQoL than the general population. Improvements in HRQoL are being achieved with cancer treatments, which is an important outcome for patients with mPaC, particularly when life expectancy may be short. However, further improvements are needed to maintain or enhance HRQoL achieved during initial treatment because patients experience HRQoL deterioration as a result of disease progression.
Abbreviations
BRE 43 QOL, quality of life form BRE 43; CI, confidence interval; CIK, cytokine-induced killer; DMBG, dimethyl-biguanide hydrochloride; ECOG PS, Eastern Cooperative Oncology Group Performance Status; EORTC, European Organization for the Research and Treatment of Cancer; EQ-5D, 5-dimension EuroQoL questionnaire; EQ-5D-5L, 5-dimension, 5-level EuroQoL questionnaire; 5-FU, 5-fluorouracil; 5-FU/LV, 5-fluorouracil and leucovorin; FACT-G, Functional Assessment of Cancer Therapy-General; FACT-Hep, Functional Assessment of Cancer Therapy-Hepatobiliary; FOLFIRI, leucovorin, fluorouracil, and irinotecan; FOLFIRINOX, leucovorin, fluorouracil, irinotecan, and oxaliplatin; GEM, gemcitabine; GHS, global health status; HIFU, high-intensity focused ultrasound; HR, hazard ratio; HRQoL, health-related quality of life; KPS, Karnofsky Performance Status scale; 177Lu-DOTATATE, [Lutetium-177-DOTA0-Tyr3]octreotate; mPaC, metastatic pancreatic cancer; nab, nanoparticle albumin-bound; nPG, nab-paclitaxel plus gemcitabine; OS, overall survival; QLQ-C30, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; QLQ-PAN26, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Pancreatic Cancer module 26; S-1, novel dihydropyrimidine dehydrogenase inhibitory fluoropyrimidine; ZPS, Zubrod-ECOG-WHO Performance Status scale.
Data Sharing Statement
Data sharing not applicable – no new data generated.
Acknowledgments
Medical writing support was provided by AccuScript Consultancy Ltd., Ludhiana, India, and Oxford PharmaGenesis Ltd., Oxford, UK, with funding provided by AstraZeneca as part of an alliance between AstraZeneca and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, who are codeveloping olaparib.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by AstraZeneca as part of an alliance between AstraZeneca and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, who are codeveloping olaparib. Both AstraZeneca and Merck & Co., Inc., Rahway, NJ, USA reviewed a draft during manuscript preparation and provided medical accuracy and IP review of the final draft.
Disclosure
Hyun Kyoo Yoo and Nikunj Patel are employees of AstraZeneca. Suvina Amin was an employee of AstraZeneca at the time of the study. Seongjung Joo is an employee of Merck & Co., Inc. The remaining authors have no competing interests in this work.
References
1. Ducreux M, Cuhna AS, Caramella C., et al. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(Suppl 5):v56–68. doi:10.1093/annonc/mdv295
2. Surveillance Epidemiology and End Results (SEER). Cancer stat facts: pancreatic cancer. 2019. Available from: https://seer.cancer.gov/statfacts/html/pancreas.html.
3. Sohal D, Kennedy E, Khorana A, et al. Metastatic pancreatic cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(24):2545–2558. doi:10.1200/JCO.2018.78.9636
4. Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. doi:10.1056/NEJMoa1011923
5. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369
6. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
7. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–376. doi:10.1093/jnci/85.5.365
8. Fitzsimmons D, Johnson CD, George S, et al. Development of a disease specific quality of life (QoL) questionnaire module to supplement the EORTC core cancer QoL questionnaire, the QLQ-C30 in patients with pancreatic cancer. EORTC Study Group on Quality of Life. Eur J Cancer. 1999;35(6):939–941. doi:10.1016/S0959-8049(99)00047-7
9. Cella DF, Tulsky DS, Gray G, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11(3):570–579. doi:10.1200/JCO.1993.11.3.570
10. Heffernan N, Cella D, Webster K, et al. Measuring health-related quality of life in patients with hepatobiliary cancers: the functional assessment of cancer therapy-hepatobiliary questionnaire. J Clin Oncol. 2002;20(9):2229–2239. doi:10.1200/JCO.2002.07.093
11. EuroQol Group. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy (New York). 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
12. Karnofsky DA, Abelmann WH, Craver LF, Burchenal JH. The use of the nitrogen mustards in the palliative treatment of carcinoma, with particular reference to bronchogenic carcinoma. Cancer. 1948;1(4):634–656. doi:10.1002/1097-0142(194811)1:4<634::AID-CNCR2820010410>3.0.CO;2-L
13. Al-Batran SE, Hofheinz RD, Reichart A, et al. Quality of life and outcome of patients with metastatic pancreatic cancer receiving first-line chemotherapy with nab-paclitaxel and gemcitabine: real-life results from the prospective QOLIXANE trial of the Platform for Outcome, Quality of Life and Translational Research on Pancreatic Cancer registry. Int J Cancer. 2021;148(6):1478–1488. doi:10.1002/ijc.33336
14. Anota A, Mouillet G, Trouilloud I, et al. Sequential FOLFIRI.3 + gemcitabine improves health-related quality of life deterioration-free survival of patients with metastatic pancreatic adenocarcinoma: a randomized Phase II trial. PLoS One. 2015;10(5):e0125350. doi:10.1371/journal.pone.0125350
15. Bonnetain F, Dahan L, Maillard E, et al. Time until definitive quality of life score deterioration as a means of longitudinal analysis for treatment trials in patients with metastatic pancreatic adenocarcinoma. Eur J Cancer. 2010;46(15):2753–2762. doi:10.1016/j.ejca.2010.07.023
16. Braun D, Gupta D, Staren E. Longitudinal health-related quality of life assessment implications for prognosis in stage IV pancreatic cancer. Pancreas. 2013;42(2):254–259. doi:10.1097/MPA.0b013e31825b9f56
17. Cella D, Butt Z, Kindler H, et al. Validity of the FACT hepatobiliary (FACT-hep) questionnaire for assessing disease-related symptoms and health-related quality of life in patients with metastatic pancreatic cancer. Qual Life Res. 2013;22(5):1105–1112. doi:10.1007/s11136-012-0217-4
18. Charton E, Bachet JB, Hammel P, et al. Impact on health-related quality of life deterioration-free survival of a first-line therapy combining nab-paclitaxel plus either gemcitabine or simplified leucovorin and fluorouracil for patients with metastatic pancreatic cancer: results of the randomized phase II AFUGEM GERCOR clinical trial. Cancer Med. 2019;8(11):5079–5088. doi:10.1002/cam4.2311
19. Chung M, Park J, Bang S, Park S, Song S. Phase II clinical trial of ex vivo-expanded cytokine-induced killer cells therapy in advanced pancreatic cancer. Cancer Immunol Immunother. 2014;63(9):939–946. doi:10.1007/s00262-014-1566-3
20. Corrie PG, Qian W, Basu B, et al. Scheduling nab-paclitaxel combined with gemcitabine as first-line treatment for metastatic pancreatic adenocarcinoma. Br J Cancer. 2020;122(12):1760–1768. doi:10.1038/s41416-020-0846-2
21. Crippa S, Dominguez I, Rodriguez J, et al. Quality of life in pancreatic cancer: analysis by stage and treatment. J Gastrointest Surg. 2008;12(5):783–793. doi:10.1007/s11605-007-0391-9
22. Feliu J, Jorge Fernandez M, Macarulla T, et al. Phase II clinical trial of nab-paclitaxel plus gemcitabine in elderly patients with previously untreated locally advanced or metastatic pancreatic adenocarcinoma: the BIBABRAX study. Cancer Chemother Pharmacol. 2021;87(4):543–553. doi:10.1007/s00280-020-04214-w
23. Golan T, Hammel P, Reni M, et al. Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer. N Engl J Med. 2019;381(4):317–327. doi:10.1056/NEJMoa1903387
24. Gourgou-Bourgade S, Bascoul-Mollevi C, Desseigne F, et al. Impact of FOLFIRINOX compared with gemcitabine on quality of life in patients with metastatic pancreatic cancer: results from the PRODIGE 4/ACCORD 11 randomized trial. J Clin Oncol. 2013;31(1):23–29. doi:10.1200/JCO.2012.44.4869
25. Haas M, Siveke J, Schenk M, et al. Efficacy of gemcitabine plus erlotinib in rash-positive patients with metastatic pancreatic cancer selected according to eligibility for FOLFIRINOX: a prospective phase II study of the ‘Arbeitsgemeinschaft Internistische Onkologie’. Eur J Cancer. 2018;94:95–103. doi:10.1016/j.ejca.2018.02.008
26. Hammel P, Kindler HL, Reni M, et al. Health-related quality of life in patients with a germline BRCA mutation and metastatic pancreatic cancer receiving maintenance olaparib. Ann Oncol. 2019;30(12):1959–1968. doi:10.1093/annonc/mdz406
27. Hubner R, Cubillo A, Blanc J, et al. Quality of life in metastatic pancreatic cancer patients receiving liposomal irinotecan plus 5-fluorouracil and leucovorin. Eur J Cancer. 2019;106:24–33. doi:10.1016/j.ejca.2018.09.029
28. Ibraimi Z, Moesinger R, Kurtishi I, Murtezani A. Comparison of clinical effectiveness of folfirinox versus gemcitabine on quality of life in patients with pancreatic cancer stage IV. Asian J Pharm. 2017;11(3):S609–S615.
29. Laquente B, Macarulla T, Buges C, et al. Quality of life of patients with metastatic pancreatic adenocarcinoma initiating first-line chemotherapy in routine practice. BMC Palliat Care. 2020;19(1):103. doi:10.1186/s12904-020-00610-4
30. Li C, Ni L, Cui X. Efficacy of DMBG and gemcitabine as a combination treatment on advanced pancreatic cancer, and their effect on miR-190, miR-196a, miR-221 and miR-222. Int J Clin Exp Med. 2020;13(2):582–589.
31. Liu Y, Wang Y, Hou C. The clinical efficacy of S-1 combined with gemcitabine in senile patients with advanced pancreatic cancer and the drugs’ effects on quality of life. Int J Clin Exp Med. 2020;13(3):1744–1750.
32. Marinova M, Feradova H, Gonzalez-Carmona MA, et al. Improving quality of life in pancreatic cancer patients following high-intensity focused ultrasound (HIFU) in two European centers. Eur Radiol. 2021;31(8):5818–5829. doi:10.1007/s00330-020-07682-z
33. Melnik MK, Webb CP, Richardson PJ, et al. Phase II trial to evaluate gemcitabine and etoposide for locally advanced or metastatic pancreatic cancer. Mol Cancer Ther. 2010;9(8):2423–2429. doi:10.1158/1535-7163.MCT-09-0854
34. Nie K, Zhang L, You Y, et al. Irinotecan combined with oxaliplatin and S-1 in patients with metastatic pancreatic adenocarcinoma: a single-arm, three-centre, prospective study. Ther Adv Med Oncol. 2020;12:1–8. doi:10.1177/1758835920970843
35. Picozzi V, Narayanan S, Henry Hu X, Vacirca J. Health-related quality of life in patients with metastatic pancreatic cancer. J Gastrointest Cancer. 2017;48(1):103–109. doi:10.1007/s12029-016-9902-9
36. Pihlak R, Frizziero M, Mak S, et al. P-274 RELEVANT study: patient and physician perspectives on clinically-meaningful outcomes in advanced pancreatic ductal adenocarcinoma. Ann Oncol. 2020;31(S3):S179. doi:10.1016/j.annonc.2020.04.356
37. Ramage JK, Punia P, Faluyi O, et al. Observational study to assess quality of life in patients with pancreatic neuroendocrine tumors receiving treatment with everolimus: the OBLIQUE study (UK Phase IV trial). Neuroendocrinology. 2019;108(4):317–327. doi:10.1159/000497330
38. Trouilloud I, DuPont-Gossard A, Malka D, et al. Fixed-dose rate gemcitabine alone or alternating with FOLFIRI.3 (irinotecan, leucovorin and fluorouracil) in the first-line treatment of patients with metastatic pancreatic adenocarcinoma: an AGEO randomised phase II study (FIRGEM). Eur J Cancer. 2014;50(18):3116–3124. doi:10.1016/j.ejca.2014.09.015
39. Ueno M, Nakamori S, Sugimori K, et al. Nal-IRI+5-FU/LV versus 5-FU/LV in post-gemcitabine metastatic pancreatic cancer: randomized phase 2 trial in Japanese patients. Cancer Med. 2020;9(24):9396–9408. doi:10.1002/cam4.3558
40. Zandee WT, Brabander T, Blazevic A, et al. Symptomatic and radiological response to 177Lu-DOTATATE for the treatment of functioning pancreatic neuroendocrine tumors. J Clin Endocrinol Metab. 2019;104(4):1336–1344. doi:10.1210/jc.2018-01991
41. Zhu X, Li F, Shi D, et al. Health-related quality of life for gemcitabine and nab-paclitaxel plus radiotherapy versus gemcitabine and S-1 plus radiotherapy in patients with metastatic pancreatic cancer. Cancer Manag Res. 2018;10:4805–4815. doi:10.2147/CMAR.S166713
42. Arraras JI, Nolte S, Liegl G, et al. General Spanish population normative data analysis for the EORTC QLQ-C30 by sex, age, and health condition. Health Qual Life Outcomes. 2021;19:208. doi:10.1186/s12955-021-01820-x
43. Ficko SL, Pejsa V, Zadnik V. Health-related quality of life in Croatian general population and multiple myeloma patients assessed by the EORTC QLQ-C30 and EORTC QLQ-MY20 questionnaires. Radiol Oncol. 2019;53(3):337–347. doi:10.2478/raon-2019-0047
44. Finck C, Barradas S, Singer S, Zenger M, Hinz A. Health-related quality of life in Colombia: reference values of the EORTC QLQ-C30. Eur J Cancer Care (Engl). 2012;21(6):829–836. doi:10.1111/ecc.12000
45. Hinz A, Singer S, Brahler E. European reference values for the quality of life questionnaire EORTC QLQ-C30: results of a German investigation and a summarizing analysis of six European general population normative studies. Acta Oncol. 2014;53(7):958–965. doi:10.3109/0284186X.2013.879998
46. Juul T, Petersen MA, Holzner B, Laurberg S, Christensen P, Gronvold M. Danish population-based reference data for the EORTC QLQ-C30: associations with gender, age and morbidity. Qual Life Res. 2014;23(8):2183–2193. doi:10.1007/s11136-014-0675-y
47. Lehmann J, Giesinger JM, Nolte S, et al. Normative data for the EORTC QLQ-C30 from the Austrian general population. Health Qual Life Outcomes. 2020;18(1):275. doi:10.1186/s12955-020-01524-8
48. Mercieca-Bebber R, Costa DS, Norman R, et al. The EORTC Quality of Life Questionnaire for cancer patients (QLQ-C30): Australian general population reference values. Med J Aust. 2019;210(11):499–506. doi:10.5694/mja2.50207
49. Nolte S, Liegl G, Petersen MA, et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the United States. Eur J Cancer. 2019;107:153–163. doi:10.1016/j.ejca.2018.11.024
50. Nolte S, Waldmann A, Liegl G, et al. Updated EORTC QLQ-C30 general population norm data for Germany. Eur J Cancer. 2020;137:161–170. doi:10.1016/j.ejca.2020.06.002
51. Scott NW, Fayers PM, Aaronson NK, et al. EORTC QLQ-C30. Brussels, Belgium: EORTC; 2008.
52. Brucker PS, Yost K, Cashy J, Webster K, Cella D. General population and cancer patient norms for the Functional Assessment of Cancer Therapy-General (FACT-G). Eval Health Prof. 2005;28(2):192–211. doi:10.1177/0163278705275341
53. Lindqvist Bagge AS, Carlander A, Fahlke C, Olofsson Bagge R. Health-related quality of life (FACT-GP) in Sweden. Health Qual Life Outcomes. 2020;18(1):172. doi:10.1186/s12955-020-01420-1
54. Steel JL, Chopra K, Olek MC, Carr BI. Health-related quality of life: hepatocellular carcinoma, chronic liver disease, and the general population. Qual Life Res. 2007;16(2):203–215. doi:10.1007/s11136-006-9111-2
55. Jiang R, Janssen MFB, Pickard AS. US population norms for the EQ-5D-5L and comparison of norms from face-to-face and online samples. Qual Life Res. 2021;30(3):803–816. doi:10.1007/s11136-020-02650-y
56. Kashem T, Al Sayah F, Tawiah A, Ohinmaa A, Johnson JA. The relationship between individual-level deprivation and health-related quality of life. Health Qual Life Outcomes. 2019;17(1):176. doi:10.1186/s12955-019-1243-5
57. McCaffrey N, Kaambwa B, Currow DC, Ratcliffe J. Health-related quality of life measured using the EQ-5D-5L: south Australian population norms. Health Qual Life Outcomes. 2016;14(1):133. doi:10.1186/s12955-016-0537-0
58. Nguyen LH, Tran BX, Hoang Le QN, Tran TT, Latkin CA. Quality of life profile of general Vietnamese population using EQ-5D-5L. Health Qual Life Outcomes. 2017;15(1):199. doi:10.1186/s12955-017-0771-0
59. Silva MT, Caicedo Roa M, Galvao TF. Health-related quality of life in the Brazilian Amazon: a population-based cross-sectional study. Health Qual Life Outcomes. 2017;15(1):159. doi:10.1186/s12955-017-0734-5
60. Wong EL, Cheung AW, Wong AY, Xu RH, Ramos-Goni JM, Rivero-Arias O. Normative profile of health-related quality of life for Hong Kong general population using preference-based instrument EQ-5D-5L. Value Health. 2019;22(8):916–924. doi:10.1016/j.jval.2019.02.014
61. Mokhtari-Hessari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes. 2020;18(1):338. doi:10.1186/s12955-020-01591-x
62. Amin S, Joo S, Nolte S, et al. Health-related quality of life scores of metastatic pancreatic cancer patients responsive to first line chemotherapy compared to newly derived EORTC QLQ-C30 reference values. BMC Cancer. 2022;22(1):563. doi:10.1186/s12885-022-09661-7
63. Kristensen A, Vagnildhaug OM, Gronberg BH, Kaasa S, Laird B, Solheim TS. Does chemotherapy improve health-related quality of life in advanced pancreatic cancer? A systematic review. Crit Rev Oncol Hematol. 2016;99:286–298. doi:10.1016/j.critrevonc.2016.01.006
64. Macarulla T, Hendifar AE, Li CP, et al. Landscape of health-related quality of life in patients with early-stage pancreatic cancer receiving adjuvant or neoadjuvant chemotherapy: a systematic literature review. Pancreas. 2020;49(3):393–407. doi:10.1097/MPA.0000000000001507
65. Bachet J-B, Hammel P, Desramé J, et al. Nab-paclitaxel plus either gemcitabine or simplified leucovorin and fluorouracil as first-line therapy for metastatic pancreatic adenocarcinoma (AFUGEM GERCOR): a non-comparative, multicentre, open-label, randomised phase 2 trial. Lancet Gastroenterol Hepatol. 2017;2(5):337–346. doi:10.1016/S2468-1253(17)30046-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.