")
Back to Journals » International Journal of General Medicine » Volume 14
Health-Related Quality of Life in Women with Breast Cancer Undergoing Chemotherapy in Brazil
Authors Marcelo Castro e Silva I , Lúcia Penteado Lancellotti C
Received 11 October 2021
Accepted for publication 14 December 2021
Published 23 December 2021 Volume 2021:14 Pages 10265—10270
DOI https://doi.org/10.2147/IJGM.S343804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Igor Marcelo Castro e Silva,1,2 Carmen Lúcia Penteado Lancellotti3
1Doctoral Program in Health Sciences, College of Medical Sciences, Santa Casa of São Paulo, Brazil; 2Department of Pathology, Federal University of Maranhão, São Luís, Maranhão, Brazil; 3Faculty of Medical Sciences, Santa Casa of São Paulo, São Paulo, Brazil
Correspondence: Igor Marcelo Castro e Silva
Department of Pathology, UFMA, Praça Madre de Deus, 01, Annex to the General Hospital, São Luís, Maranhão, Brazil
Email [email protected]
Introduction: Breast cancer (BC) is an austere public health problem, representing the most incident and prevalent malignancy among women worldwide.
Objective: To evaluate the health-related quality of life of women with breast cancer undergoing initial and final stages of chemotherapy treatment.
Methods: It was descriptive, correlational, analytical, prospective cross-sectional study that included 80 women diagnosed with breast cancer undergoing chemotherapy treatment. Health-related quality of life was assessed in two phases. The first one was on the initial day of the treatment and the second, 120 days after started the chemotherapy.
Results: Eighty adult women were part of the study, whose average age was 52.54. Overall quality of life decreased due to chemotherapy. It was noted the negative impact that the emotional role, the sexual function and the concern about hair loss on health-related quality of life. It was observed that fatigue, nausea and vomiting, appetite loss, diarrhea were frequent symptoms in comparison between the phases. Sexual function and satisfaction were dissatisfying and worsened during chemotherapy.
Conclusion: The quality of life related to the health of patients is negatively influenced during chemotherapy treatment, hence, requiring interventions in oncology and research in this sphere.
Keywords: breast, cancer, quality of life
Introduction
Health-related quality of life (HRQOL)
Refers to the impact of illness, disease aggravation or therapeutic interventions under the individual perception in this context of quality of life. That is, the perception of the change in the state of health by the individual and the impact of this change on their quality of life.1,2
In oncology, quality of life (QOL) comprehends the subjective perception of the patient regarding their disability and satisfaction with their current level of functional organization, making them consider themselves good or not, compared to what they perceive as possible or ideal.3,4
Breast cancer (BC) diagnosis, on its part, is experienced as a moment of anguish, suffering and anxiety. During treatment, the woman experiences losses, both physical and financial, as well as adverse symptoms, such decreased self-esteem, resulting from adaptations to physical, psychological, social, family and emotional changes caused by the disease.3–5
Due to the high incidence and harm that BC diagnosis and therapy establish in women’s lives, greater relevance has been given to the research of HRQOL measures of women with BC in recent decades, helping staff, patients and caregivers in deciding whether or not to continue therapy.
This study was aimed to evaluate the HRQOL of women with BC in the initial and final stages of chemotherapy treatment.
Patients and Methods
A descriptive, correlational, analytical, prospective study, was conducted between the months of January 2019 to February 2020, in a chemotherapy unit (CT) of a public hospital in the state of Maranhão, Brazil, reference to cancer treatment, with exclusive care of the Brazilian Unified Health System (SUS). The development of the study has met the national and international standards of ethics in research involving humans, of the National Health Council, and was approved by the Research Ethics Committee of the UNICEUMA University institution registered number 606. 999. The data confidentiality and compliance with the Declaration of Helsinki were maintained. Written informed consent was obtained from all participants.
The sample was for convenience, not probabilistic, including all patients with BC undergoing exclusive chemotherapy treatment, at any stage of the disease, aged 18 years or older and who agreed to participate in the study. Those patients who already had undergone any chemotherapy treatments and those with brain metastasis were excluded from the sample. Data collection was carried out in two phases. The first phase was done on the day the treatment started and the second was completed after 120 days.
Two sets of questions were used: a sociodemographic and clinical characterization, built by the researchers with data such as age, gender, marital status, education level, occupation, profession, religious activity, medical diagnosis, previous surgery, chemotherapy regimens applied in the first phase.
The questionnaire of HRQOL developed by the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire – Core 30 (EORTC QLQ-C30) and the Quality-of-Life Questionnaire – Breast Cancer Module (QLQ-BR23), both in Portuguese and validated in Brazil applied at all stages of the research.6
The questionnaire EORTC QLQ C30 is self-explanatory, consisting of 30 questions, divided into three dimensions: general quality of life, functional scales (called physical, emotional, cognitive, general and social function) and symptoms spectrum (including fatigue, pain, dyspnea, insomnia, loss of appetite, nausea and vomiting, constipation, diarrhea and financial difficulty).
The BR23 questionnaire, is a specific module for patients who have had breast cancer, consisting of 23 questions divided into two dimensions: functional scales (body image, future perspective, sexual function and sexual satisfaction) and symptom scales (effects of chemotherapy, hair loss concern, breast symptoms and arm symptoms).
To calculate the score in each one of the dimensions of the questionnaires applied (C-30 and BR-23), the EORTC Scores’ Manual was used [6]. The average of the responses obtained in each of the scale/dimensions (general quality of life – GQOL; functional scales; symptom scales; BR-23 items) were mathematically transformed into a scale from 0 to 100 points, in which 0 represented the worst state of health and 100, the best state of health. In turn, for the interpretation of the Symptom Scale, the value 0 meant higher quality of life and 100, a lower quality of life Index.
The statistical analysis was carried out through the SPSS v. 19 computer program (IBM – USA), considering a significance level of 5%.
To evaluate the dimensions affected in the patients’ quality of life during and after six months of chemotherapy cancer treatment, the test t-student was used for paired samples, where the means of the scores in the evaluated items of the questionnaires were compared.
Relations between quality-of-life dimensions, clinical and sociodemographic variables were analyzed according to the one-way ANOVA tests (for qualitative variables) and Pearson Linear Correlation (quantitative variables). For the use of the ANOVA test one-way, data normality (SHAPIRO-WILK test) and homogeneity of variances (LEVENE test) were previously tested. As corroborating post-techniques of ANOVA were used the TUKEY multiple comparison tests (for samples with equal variances) and GAMES-HOWELL tests (for samples with non-presumed variances). For variables that did not meet any of the ANOVA presuppositions, the nonparametric test MANN-WHITNEY was used.
Results
Eighty adult women, with mean age of ± 52 years, participated in the study. Most of the women were from São Luís (65%), home owners (78.75%), white (53.75%), married (56.25%) and catholic (58.75%). Regarding their level of education, most of them had completed High School (60%) and technical/specialist training (66.25%). In clinical results, the infiltrating ductal carcinoma histological type predominated (98.75%), as well as stage III (55.00%), mastectomy (46.25%) and the doxorubicin-cyclophosphamide taxol chemotherapy treatment scheme (ACT) (56.25%).
Regarding the evaluation of HRQOL of patients in Phase 01, in general there were higher evaluations of the average QOL scores for the dimensions of the functional scale and symptom scale. The worst QOL evaluation averages were present within the functional scale (sexual function) and symptom scale (insomnia) (Table 1).
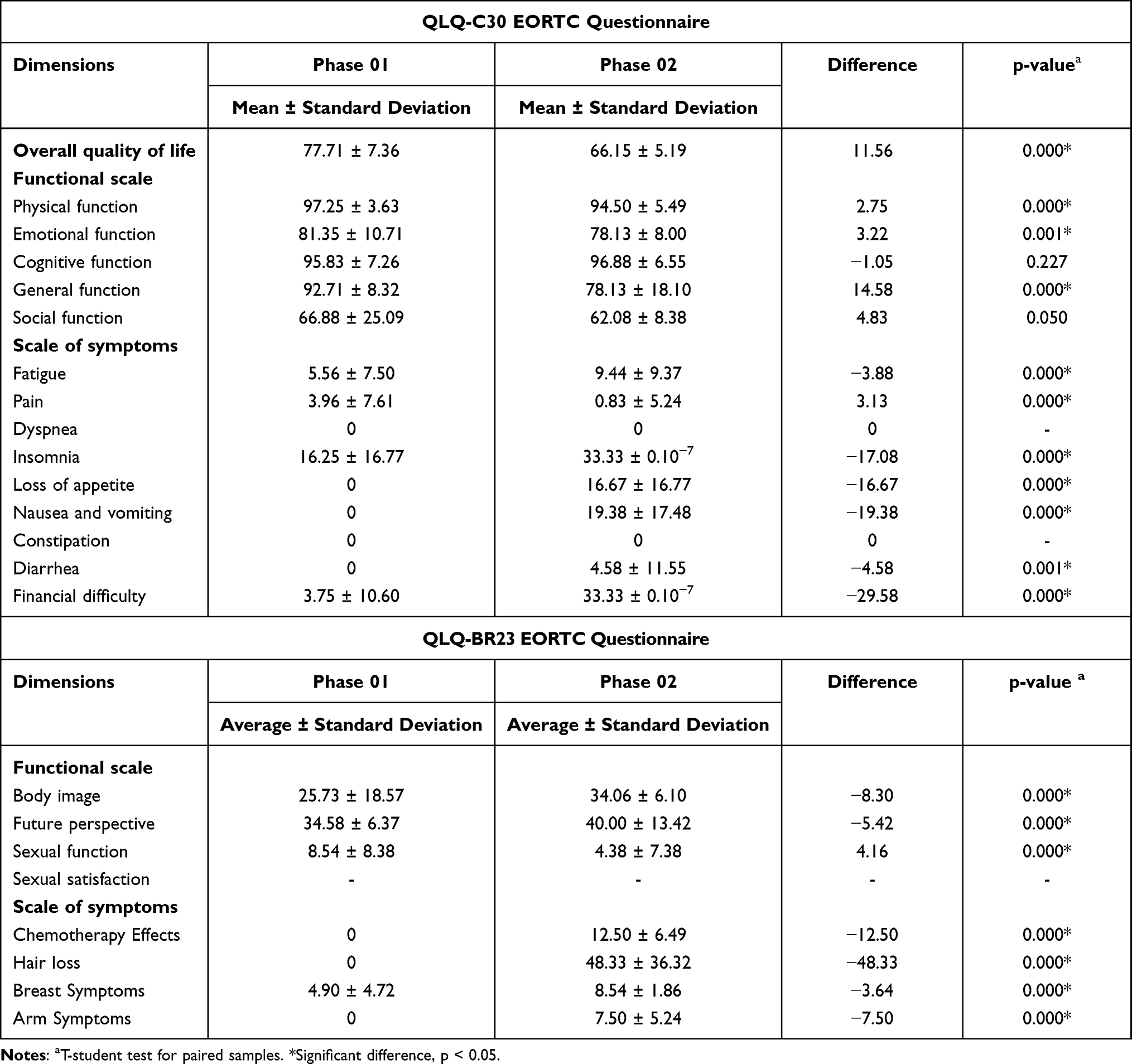 |
Table 1 Comparison of Health-Related Quality of Life Between Stages of Chemotherapy Treatment |
In Phase 02, better assessments were recorded for the Functional Scale (cognitive function) and symptom scale (dyspnea and constipation, both with average 0 in the evaluation). The worst evaluations were descriptive for the functional scale (sexual function) and symptom scale (concern with hair loss) (Table 1).
When we compared the average of the evaluation of the responses, have been observed improvement in the QOL of range of symptoms of pain, body image and future. The worsening in QOL was recorded for the Overall Quality of Life; the scale functional–physical role, emotional role, the overall function and sexual role; the scale of the fatigue symptoms, sleep, appetite loss, nausea and vomiting, diarrhea, financial difficulties, the effects of chemotherapy, and concern about hair loss, symptoms in the breast and the symptoms in the arm, with the largest difference from the average being the concern about the hair loss (Table 1). The factors related to dyspnea and constipation have not presented variation between the phases.
Discussion
The age group of the participants presented average age of 52.54 ± 9.54 years, matching the national profile, as in studies performed in the states of Ceará and Minas Gerais, investigating the HRQOL of women with breast cancer.7,8
Regarding the level of education, it was observed that most of the population studied were homeowners and had completed High School (60.00%; n = 48), reproducing something contrary to what the literature says, where they point BC involvement mostly in low-income women and precarious level of education in developing countries.9 It is inferred that, currently, through the national social economic context, a large part of the population has lost private healthcare insurance, resorting to the public health system.
About race/ethnicity, there was a predominance of white skin color, narrowing with data from the Brazilian Breast Cancer Study Group.10 The evaluation of the race/ethnicity of the patients, however, did not have any objective criterion, being carried out by the perception of the interviewee.
The tumors’ characteristics found explain that most of the women obtained the diagnosis in locally advanced (CE III) and advanced (CE IV) staging. Public health service patients have a higher incidence of advanced stages, considering the long interval between suspicion and diagnostic confirmation, as well as the lower access to mammography and ultrasound of breasts and armpits when compared to the private sector.8 Through this context, we see the realization of more aggressive and invasive therapeutic treatments, as occurred in this study, where 46% of women were subjected to mastectomy.
Through the exponential growth of BC cases, as well as the consequences of chemotherapy treatment on the physical, psychological, social and spiritual conditions of this group, there are several studies that investigate the influence of CT on QOL of these patients.11
The evaluation of HRQOL has thus been used as an important tool in measuring the impact of the disease on the patient, enabling the creation of indicators of the disease severity and progression.12
This study made it possible to describe real-world data about the changes in HRQOL that CT can trigger. This helps oncologists to measure the effect of CT on potential biopsychosocial characters.13
In this study, the patients’ HRQOL is worse when comparing the period right before chemotherapy with that during the course of treatment. The overall quality of life (QOL) has decreased due to CT, inferring those women with BC have considered the worsening of their health status during CT. This fact was also observed by Binotto et al13 and Leinert et al14 who showed that overall health condition has worsened due to CT and increased symptoms associated with the treatment in question.
It was also noted the negative impact that the emotional function, sexual function and the concern about hair loss have generated on HRQOL. Patients with BC have a higher risk of developing changes in their psychological functions.8,15 Based on the literature, it is accepted there that might exist a significant involution in the scales of emotional functioning and body image, especially alopecia during CT. It is inferred that a modified and impaired body image is a peerless psychosocial issue for women with BC.16 This fact is listed in the intrinsic relationship of body image and the inherent perceptions of patients about what others think about them.13 Overall HRQOL, low social and emotional functioning patients with BC were greatly associated with concern about alopecia, contradicting Zhang et al,17 who understood that the severity of symptoms is directly associated with opposing psycho-behavioral characteristics.
It is pondered that no decreasing in breast and arm symptoms was felt throughout the treatment, however, pain has eased. Similar results were explained by Winters et al.18
When analyzing the QLQ-C30 symptom scale, it was observed that fatigue, nausea and vomiting, loss of appetite, diarrhea and financial difficulty were frequent symptoms in the comparison between the phases, as demonstrated by Lôbo et al19 and Konstantinidis et al20 for insomnia and by Benevides21 for insomnia and financial difficulty, suggesting that, at some point, the HRQOL of women was affected by the fall in financial income, insomnia and nausea.
Insomnia is a frequent symptom, usually followed by pain, anxiety, depression and fatigue. The treatment improves not only fatigue, but also, the patients’ mood and their QOL.4
Gozzo et al22 and Silva and Gonçalves4 report the importance, of valuing nausea and vomiting by health professionals, in clinical practice, establishing “individualized care for users”. Managing the events of chemotherapy treatment is essential for the healthy control of gastrointestinal toxicities.
Sexual function and sexual satisfaction in the sample were not satisfactory, and worsened during CT, thus signaling significant interference of the disease and treatment. HRQOL associated with sexuality may decrease or be ceased by the presence of dysfunction in this domain. The importance of a directed approach becomes essential, since most of the (medical) services cover only the physical context of BC and marginalize the acceptance of women to body modifications resulting from this cancer.23
These results corroborate the studies of Hall et al,24 which concluded that the vast majority of systemic effects of CT compromise women’s sexuality both in the short and long term. The increase in systemic adverse effects such as fatigue, nausea and vomiting, insomnia, loss of appetite and diarrhea corroborated the expected toxicity results for the treatment.
In the present study, social functioning was not impaired throughout the CT, meaning that physical condition and treatment did not interfere significantly in the way of how the patient connected to her social networks. Conflicting result with Binnoto et al13 and Gaston-Johansson et al.25 Social engagement and interaction are related to better HRQOL, when there is greater social support from family and friends to patients with BC.
The present study was limited by the lack of subsequent evaluations after the one performed at 06 months of CT, as in Binnoto et al.13 It was not possible to consider whether the impact of CT on HRQOL was reversible for the period evaluated at the beginning of treatment after an extensive period. Even with this factor, the aim of the study was achieved when assessing the impact of CT on the patient’s HRQOL and the identification of factors that affect the psychosocial parameters of the patient’s well-being.
Conclusion
The present study thus contributed to understand the patients’ needs during CT, as well as the coping and planning by the patient, healthcare team and family. The results conclude that the HRQOL of these patients is negatively influenced during chemotherapy treatment, requiring interventions in oncology and research in this area.
Health professionals directly linked to oncology should pay due attention to setbacks in the patient’s adjustment to treatment, as the period immediately after the start of treatment is a crucial point for the assessment of patient’s confronting needs. The quality of the information established and provided at this time leads to an improved sense of well-being.
The healthcare provider’s screening may consider patient perceptions of overall health status and QOL, physical, emotional and social functioning. In this construct, communication and empathy skills are of extreme importance in conducting psychosocial assessment.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest associated with this publication.
References
1. Saxena S, Orley J; Whoqol Group. Quality of life assessment: the World Health Organization perspective. Eur Psychiatry. 1997;12(S3):263s–266s. doi:10.1016/S0924-9338(97)89095-5
2. Silva IMC, Gonçalves EGR. Câncer de mama e meio ambiente: uma revisão integrativa. [Breast cancer and the environment: an integrative review]. Conexão Ci. 2017;12(1):110–115. doi:10.24862/cco.v12i1.529
3. Salvetti MDG, Pereira CSM, Donato SCT, Silva AM. Prevalência de sintomas e qualidade de vida de pacientes com câncer. [Prevalence of symptoms and quality of life of cancer patients]. Rev Bras Enfer. 2020;73(2):1–7.
4. Silva IMC, Gonçalves EGR. Avaliação da qualidade de vida relacionada a saúde de mulheres portadoras de câncer de mama. [Assessment of the health-related quality of life of women with breast cancer]; 2018. Available from: https://tedebc.ufma.br/jspui/handle/tede/tede/2084.
5. Fortes RC, Haack A, Frazão ERP. Qualidade de vida de mulheres com câncer de mama: uma revisão integrativa. [Quality of life of women with breast cancer: an integrative review]. Com Ciências Da Saúde. 2018;29(4). doi:10.51723/ccs.v29i04.395
6. Michels FAZ, Latorre MRDO, Maciel MS. Validity, reliability and understanding of the EORTC-C30 and EORTC-BR23, quality of life questionnaires specific for breast cancer. Rev Bras Epidemiol. 2013;16:352–363. doi:10.1590/S1415-790X2013000200011
7. Bezerra KB, Silva DSM, Chein MBC, et al. Qualidade de vida de mulheres tratadas de câncer de mama em uma cidade do nordeste do Brasil. [Quality of life of women treated for breast cancer in a city in northeastern Brazil]. Cien Saude Colet. 2013;18(7):1933–1941. doi:10.1590/S1413-81232013000700008
8. Barbosa PA, Cesca RG, Pacifico TED, et al. Qualidade de vida em mulheres com câncer de mama pós-intervenção cirúrgica em uma cidade da zona da mata de Minas Gerais, Brasil. [Quality of life in women with breast cancer after surgical intervention in a city in the Zona da Mata of Minas Gerais, Brazil]. Rev Bras Saúde Mater Infant. 2017;17(2):385–399. doi:10.1590/1806-93042017000200010
9. Coelho RCFP, Panobiano MS, Guimarães PRB, et al. Tratamento quimioterápico adjuvante e neoadjuvante e as implicações na qualidade de vida mulheres com câncer de mama. [Adjuvant and neoadjuvant chemotherapy treatment and implications for the quality of life of women with breast cancer]. Rev Enferm UFPE on Line. 2017;11(11):4732–4740.
10. Simon SD. Projeto amazonas- dados preliminares de câncer de mama no Brasil; 2015. [Amazon project - preliminary data on breast cancer in Brazil]. Available from: http://www.gbecam.org.br/downloads/Projeto_Amazona.pdf.
11. Andrade ALP, Maciel EM, Rodrigues GP, et al. Influência do Tratamento Quimioterápico no Comportamento Alimentar e Qualidade de Vida de Pacientes Oncológicos. Rev Bras Cancer. [Influence of Chemotherapy Treatment on Food Behavior and Quality of Life of Cancer Patients]. 2019;65(2):e–08093. doi:10.32635/2176-9745.RBC.2019v65n2.93
12. Frenzel AP, Pastore CA, Gonzalez MC. The influence of body composition on quality of life of patients with breast cancer. Nutr Hosp. 2013;28(5):1475–1482.
13. Binotto M, Reinert T, Werutsky G, et al. Health-related quality of life before and during chemotherapy in patients with early-stage breast cancer. Ecancermedicalscience. 2020;14. doi:10.3332/ecancer.2020.1007
14. Leinert E, Singer S, Janni W, et al. The impact of age on quality of life in breast cancer patients receiving adjuvant chemotherapy: a comparative analysis from the prospective multicenter randomized ADEBAR trial. Clin Breast Cancer. 2017;17(2):100–106. doi:10.1016/j.clbc.2016.10.008
15. Perroud HA, Alasino CM, Rico MJ, et al. Quality of life in patients with metastatic breast cancer treated with metronomic chemotherapy. Future Oncol. 2016;12(10):1233–1242. doi:10.2217/fon-2016-0075
16. Lima EOL, Da Silva MM. Qualidade de vida de mulheres acometidas por câncer de mama localmente avançado ou metastático. [Quality of life of women with locally advanced or metastatic breast cancer]. Rev Gaúcha Enferm. 2020;41. doi:10.1590/1983-1447.2020.20190292
17. Zhang Y, Fritzsche K, Leonhart R, et al. Dysfunctional illness perception and illness behavior associated with high somatic symptom severity and low quality of life in general hospital outpatients in China. J Psychosom Res. 2014;77(3):187–195. doi:10.1016/j.jpsychores.2014.06.005
18. Winters ZE, Haviland J, Balta V, et al. Integration of patient-reported outcome measures with key clinical outcomes after immediate latissimus dorsi breast reconstruction and adjuvant treatment. J Br Surg. 2013;100(2):240–251.
19. Lôbo AS. Qualidade de Vida de Mulheres com câncer de mama em quimioterapia [Dissertação (Mestrado em Enfermagem)]. [Quality of Life of Women with Breast Cancer in Chemotherapy [Dissertation (Masters in Nursing)]].Fortaleza: Universidade Federal do Ceará; 2013.
20. Konstantinids T, Linardakis M, Samonis G, Philalithis A. Quality of life of patients with advanced cancer treated in a regional hospital in Greece. Hippokratia. 2016;20(2):139.
21. Benevides JMM. Qualidade de vida de mulheres pós-tratamento Neoadjuvante e adjuvante de câncer de mama; 2011. [Quality of life of women after neoadjuvant and adjuvant treatment for breast cancer]. Available from: https://tede.ufam.edu.br/handle/tede/44080.
22. Gozzo TDO, Moysés AMB, Silva PRD, Almeida AMD. Náuseas, vômitos e qualidade de vida de mulheres com câncer de mama em tratamento quimioterápico. [Nausea, vomiting and quality of life of women with breast cancer undergoing chemotherapy]. Rev Gaúcha Enferm. 2013;34:110–116. doi:10.1590/S1983-14472013000300014
23. Bushatsky M, Silva RA, Lima MTC, et al. Qualidade de vida em mulheres com câncer de mama em tratamento quimioterápico. [Quality of life in women with breast cancer undergoing chemotherapy treatment]. Ciênc Cuid Saúde. 2017;16(3). doi:10.4025/cienccuidsaude.v16i3.36094
24. Hall E, Cameron D, Waters R, et al. Comparison of patient reported quality of life and impact of treatment side effects experienced with a taxane-containing regimen and standard anthracycline based chemotherapy for early breast cancer: 6-year results from the UK TACT trial (CRUK/01/001). Eur J Cancer. 2014;50(14):2375–2389. doi:10.1016/j.ejca.2014.06.007
25. Gaston-Johansson F, Watkins CC, Kanu IK, et al. The effects of symptoms on quality of life during chemotherapy in African-American women with breast cancer. J Natl Black Nurses Assoc. 2015;26(2):7.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.