")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Health-Related Quality of Life in Patients After Surgically Treated Midface Fracture: A Comparison with the Croatian Population Norm
Authors Lupi-Ferandin S, Glumac S , Poljak N, Galic T, Ivkovic N , Brborovic O , Pecotic R, Dogas Z
Received 12 February 2020
Accepted for publication 18 March 2020
Published 9 April 2020 Volume 2020:16 Pages 261—267
DOI https://doi.org/10.2147/TCRM.S249116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Slaven Lupi-Ferandin,1 Sandro Glumac,2 Nancy Poljak,3 Tea Galic,4,5 Natalija Ivkovic,6 Ognjen Brborovic,7 Renata Pecotic,5,6 Zoran Dogas5,6
1Department of Maxillofacial and Oral Surgery, University Hospital of Split, Split, Croatia; 2Department of Anesthesiology and Intensive Care, University Hospital of Split, Split, Croatia; 3Study of Dental Medicine, School of Medicine, University of Zagreb, Zagreb, Croatia; 4Study of Dental Medicine, School of Medicine, University of Split, Split, Croatia; 5Department of Neuroscience, School of Medicine, University of Split, Split, Croatia; 6Sleep Medicine Center, School of Medicine, University of Split, Split, Croatia; 7Department of Social Medicine and Organization of Health Care, Andrija Stampar School of Public Health, School of Medicine, University of Zagreb, Zagreb, Croatia
Correspondence: Zoran Dogas
Department of Neuroscience, School of Medicine, University of Split, Soltanska 2, Split 21000, Croatia
Tel +385 21557903
Fax +385 21557895
Email [email protected]
Aim: To evaluate the health-related life quality of patients after surgically treated midface fractures.
Patients and Methods: This retrospective cohort study compared the 36-Item Short Form Health Survey (SF-36) scores of 42 male patients following surgically treated maxillary or zygomatic fractures with the reported normative data of the SF-36 for the Croatian population.
Results: The current study showed that the health-related life quality of surgically treated patients was comparable to similar age, gender, and regional demographics in the Croatian population norm. However, we revealed a significant deterioration of the “Emotional wellbeing” domain in younger patients (P = 0.03) and a severely affected domain of “Physical functioning” in older patients (P = 0.049).
Conclusion: There was a significant negative psychological impact from facial trauma on younger patients. In contrast, older patients were more prone to physical impairment. Therefore, follow-up visits are an opportunity to screen and refer younger patients to mental health services in a timely manner to prevent severe psychological difficulties and an opportunity to identify older patients who require physical therapy.
Keywords: quality of life, patient outcome assessment, maxillary fractures, zygomatic fractures, surgery, oral
Introduction
Facial fractures may result from a variety of injuries. They can be isolated or combined with other injuries.1 Therefore, a multidisciplinary approach is necessary in diagnostic and therapeutic protocols.2 The epidemiology of facial fractures has changed over time, as a result of numerous socioeconomic factors.1,3 Traffic accidents, interpersonal violence, and male gender prevalence are characteristics of this type of injury.1,4-6
The best aesthetic and functional outcomes of these complex facial fractures are obtained with early exact bone repositioning and rigid fixation using screws and plates.4,7,8 Both osteosynthesis materials and surgical approaches have evolved and have beneficial effects on postoperative results.3 Computerized tomography represents a diagnostic instrument and a proven tool for the estimation of a postoperative course.2 Unlike the mandible, the midface is composed of thin bones combined with vertical bone pillars.7 Thus, in the case of a traumatic event that requires a surgical procedure, there is a certain degree of repercussions to the midface that could contribute significantly to a patient’s physical and psychological wellbeing. There is presently a lack of data regarding physical and psychological impairment in such injuries,4,9-11 but health-related quality of life (HRQOL) protocols after facial trauma have been well recognized and adopted.4,12-14
The main purpose of the current study was to compare the 36-Item Short Form Health Survey (SF-36) scores of surgically treated maxillary and zygomatic fractures in male patients with the reported normative data of SF-36 for the Croatian population. The secondary aim was to correlate important clinical variables with different concepts of the SF-36. We hypothesized that surgically treated facial trauma has negative implications on patient quality of life.
Patients and Methods
Study Design and Participants
The current retrospective cohort study analyzed the medical records of patients treated surgically for midface trauma at the Department of Maxillofacial and Oral Surgery at the University Hospital of Split, Croatia, between January 2003 and December 2013. Ethical approval for this study (Ethical Committee No. 2181-147-01/M.J.-12-2) was provided by the Ethical Committee of the University Hospital of Split (Chairperson Prof J. Bagatin) on June 14, 2012. All patients provided written informed consent.
The study enrolled male patients aged 18 years or older with a diagnosis of maxillary or zygomatic fracture caused by blunt trauma that was surgically treated by open reduction with rigid plate and screws fixation. Maxillary fracture patients had their fracture classified according to Le Fort patterns. Zygomatic fracture patients were patients with a zygomatic complex fracture. Patients with isolated dentoalveolar fractures of the upper jaw and isolated fractures of the zygomatic arch were excluded. Diagnosis was confirmed by computerized tomography. Polytraumatized patients and patients with severe concomitant brain injury (Glasgow coma scale score of less than nine) were also excluded. Finally, exclusion criteria also included cerebrovascular incident since surgery; neurological disorders; visual, hearing or motor impairment interfering with life quality assessment; mental illness; and alcohol (> 20 g per day or > 150 g per week) or controlled substance abuse.
We considered the healing process to end 12 months following the surgical procedure. After that period, the patients who met specific diagnostic and treatment criteria were first contacted by letter and via telephone by the same interviewer, who explained the study protocol in detail. For the 60 patients that fulfilled the inclusion criteria and were willing to participate in the study, demographic data was collected, and they received a letter with the SF-36 questionnaire. However, the 42 patients responded positively and were included in further analysis.
Health-Related Life Quality Assessment
The Croatian Adult Health Survey (CAHS) was carried out in 2003. Its main goal was to provide data for the prevention of cardiovascular disease in the Croatian population. The sample consisted of 9070 respondents aged 18 years or older, representative of the national and regional level.15 Subsequently, the Croatian Adult Health Cohort Study (CroHort) took place in 2008, which was the follow-up study of CAHS. Its aim was to re-interview the 9070 respondents from CAHS.16 SF-36 represents the theoretically established and empirically proven operationalization of two general health concepts: physical and psychological. It consists of 36 questions and eight health domains summarized into two dimensions: “physical health” (PCS) and “mental health” (MCS). Domains of “Physical functioning”, “Role limitations due to physical health”, “Pain”, and “General health” constitute the “physical health” dimension, while “Energy/fatigue”, “Social functioning”, “Role limitations due to emotional problems”, and “Emotional wellbeing” domains constitute the “mental health” dimension of patient quality of life. SF-36 measures the burden of the disease and the results of treatment from the patient’s own perspective.17 It has been translated into Croatian and validated for the population of the Republic of Croatia.18 Significantly, it was implemented in CAHS and CroHort studies.15 The data from eight SF-36 domains was calculated according to SF-36’s manual for each participant in this study and compared with data of the referent Croatian population (CroHort) while considering age, gender, and region affiliation.16,17
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics, version 24.0 (IBM Corp., Armonk, New York, USA). Continuous variables were expressed as means ± SD or medians and IQR in the case of asymmetrical distribution. Categorical variables were expressed as numbers and percentages. The comparison between the surgically treated male patients and the referent population (men from the Mediterranean region of Croatia) was done separately in younger patients (< 37 years) and in older patients (≥ 37 years) in order to ensure the appropriate comparison between the groups in terms of age. The cut-off value of 37 years was set based on the mean value of age in the patient group. The comparison of mean values of continuous variables between patients and the referent population was performed by using the independent samples t-test or the Mann–Whitney U-test, depending on the normality of distribution of the tested variables. A chi-square test was used to determine the relationship between two categorical variables. The Kruskal–Wallis test was used to test differences in various aspects of the patient’s health-related life quality (PCS, MCS, eight domains of the SF-36 questionnaire) while considering the type of fracture (Le Fort I, II, and III fractures or a zygomatic fracture). A correlation analysis (Pearson correlation coefficient) was applied to analyze the association between the time period after surgery and various aspects of the patient’s health-related life quality. The multiple linear regression model (Stepwise method) was used to evaluate whether the age, length of time following the surgery, or type of fracture represented a significant predictor of the patient’s health-related life quality outcomes. A significance level of 95% (P < 0.05) was applied.
Results
Study Population
Of the 60 patients that initially agreed to participate in this study and met the inclusion criteria of the study, the 42 patients sent back via letter the completed SF-36 test, so ultimately, we analyzed the data of 42 patients. The study population included 25 (59.5%) maxillary fracture patients and 17 (40.5%) zygomatic complex fracture patients. Among the maxillary fracture patients, there were three (7%) patients with a Le Fort I fracture, 14 (33%) patients with a Le Fort II fracture, and eight (19%) patients with a Le Fort III fracture. The median time for the assessment of patient health-related life quality following surgery was four years (IQR, 3 to 7). Between the two age groups of patients (< 37 years and ≥ 37 years), there were no statistically significant differences in the distribution of the types of fractures (χ2 = 2.035, df = 3, P = 0.565). In the group of younger patients, there were no significant differences with the referent population when considering age (Table 1). However, the group of older patients was younger than the referent population by an average of 6.3 years (Table 1). Finally, the body mass index of both patient age groups was comparable with the referent population (Table 1).
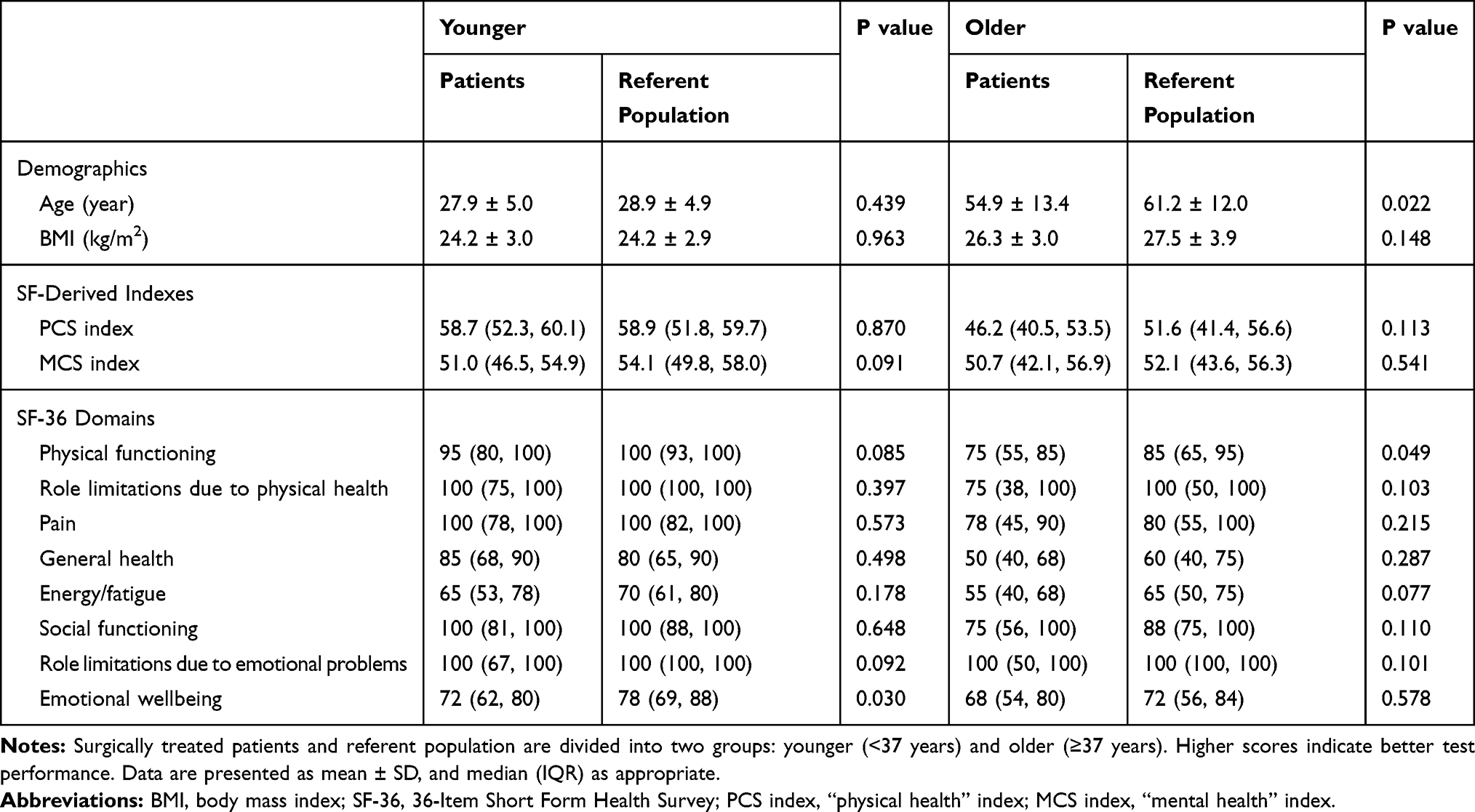 |
Table 1 Demographic Characteristics and 36-Item Short Form Health Survey Results in the Patients and Referent Population |
Patients and Referent Population
The results of SF-36 domains and indexes in the patients and referent population are presented in Table 1. There were no significant differences between either of the patient age groups and the referent population considering the PCS index or “Role limitations due to physical health”, “Pain”, “General health”, “Energy/fatigue”, and “Social functioning” domains. However, there was a significant difference in the “Emotional wellbeing” domain between younger patients and the referent population (Mann–Whitney U-test, P = 0.03). In addition, in the “mental health” dimension of life quality, we identified a few more subtle differences between younger patients and the referent population. Younger patients had markedly lower results in the MCS index (P = 0.091) and in the “Role limitations due to emotional problems” domain (P = 0.092), as compared to the referent population. On the other hand, there were no significant differences in the “Emotional wellbeing” domain between older patients and the referent population. In contrast to younger patients, older patients were mostly affected by the deterioration of the “physical health” dimension of life quality, since we observed a noticeably lower score in the domain of “Physical functioning” (P = 0.049), as compared to the referent population.
Type of Fracture and SF-36
There were no significant differences between the scores of SF-36 domains in terms of the type of fracture (Kruskal–Wallis test, P ≥ 0.194), but with a more extensive maxillary fracture, there is an obvious decrease in the PCS and MCS indexes. After testing two patient age groups, in the group of younger patients, the correlation between the scores in SF-36 domains and the type of fracture became even weaker (Kruskal–Wallis test, P ≥ 0.442). In the group of older patients, the domain of “General health” was most related to the fracture type (P = 0.095). The other domains of SF-36 were more comparable (P ≥ 0.112).
Time Period After Surgery and SF-36
There was a significant correlation between the time period following surgery and scores in the domains and indexes of SF-36. In the group of younger patients, there was a positive and moderate correlation between the time period after surgery and the “Role limitations due to physical health” domain (Pearson correlation coefficient, r = 0.448, P = 0.042). In the group of older patients, we found a positive and moderate correlation between the time period after surgery and the PCS index (Pearson correlation coefficient, r = 0.432, P = 0.049).
Determinants of Various Health Aspects for Patient Life Quality
The results of the regression model showed that age is the most significant predictor among various health aspects for patient life quality following a facial surgical procedure. With increasing age, there was a significant deterioration in the PCS index (P < 0.001) as well as in the “Physical functioning” (P = 0.019), “Pain” (P = 0.036), and “General health” (P = 0.001) domains, which collectively constitute the “physical health” dimension of patient life quality. Along with age, the time period since surgery was also an important determinant of the PCS index (a prolonged time period after surgery resulted in an increase in the PCS index, P = 0.017). Regarding the fracture type, the only significant determinant was the Le Fort I fracture (P = 0.035). Compared with other types of fractures, patients with a Le Fort I fracture, as the lightest fracture among those investigated, showed a significant improvement of functioning in the “Energy/fatigue” domain (24% on average).
Discussion
The current retrospective cohort study revealed that following facial surgery, younger patients suffer a significant decrease in the emotional wellbeing component of life quality, when compared to the referent population. Contrary to younger patients, older patients were more prone to difficulties associated with physical functioning. Therefore, surgeons should be aware that facial injury may put patients at increased risk for reduced life quality and should consider the potential psychological and rehabilitation needs for these patients. To our knowledge, this is the second study that has assessed HRQOL using the SF-36 questionnaire in patients after surgically treated midface injuries and the first that compared them against general population norms.
It is well recognized that a greater intensity of the traumatic event reflects a greater repercussion on the HRQOL score;4 the recent study of Zwingmann et al showed that polytraumatized patients had lower scores in each domain of SF-36, as compared to those of the age- and gender-matched population norm.13 Therefore, HRQOL is an increasingly used tool in clinical practice. It serves to evaluate the results of treatment and also helps to select optimal therapeutic modalities.19 We performed the SF-36 questionnaire, which can be completed in five to 10 minutes and is applicable in busy clinical settings.17 None of our participants had any difficulties with completing the tests. Given that SF-36 questionnaire was validated in Croatian,18 and because we had values of the Croatian population norm,16 the current study has established its credibility.
Facial appearance affects the attractiveness of people, both in their own perception and others. The midface is a sensitive region due to its structural and three-dimensional complexity.7,8 Our premise was that midface trauma can be challenging not only for surgeons, but patients as well.
The current study showed that the “General health” domain in both patient age groups was comparable to the referent population for the same age, gender, and region. Also, the PCS index and the “Role limitations due to physical health”, “Pain”, “Energy/fatigue”, and “Social functioning” domain scores were comparable with the matched referent population. However, we have revealed that the “Emotional wellbeing” domain in younger patients differed significantly from the referent population. Furthermore, younger patients had evidently lower results in the MCS index and in the “Role limitations due to emotional problems” domain, both of which represent the “mental health” dimension of life quality, as compared to the referent population. Psychosocial issues related to these types of injuries in younger patients are poorly understood and have not been approached adequately.9,20,21 Bisson et al have found a lack of documentation regarding the psychological aspects of facial trauma patients.22 Next, there is a clear relationship between facial injury and severe posttraumatic repercussions, including anxiety, unemployment, alcohol abuse, marital conflicts, reduced life satisfaction, and discomfort regarding body image.4,9,23 Collectively, this injury and subsequent surgery may affect the “Emotional wellbeing” domain, specifically in younger patients who are more concerned with facial appearance and socioeconomic status. Moreover, lower scores in the “Emotional wellbeing” domain indicate that an injured person may also experience adverse psychological sequelae, such as posttraumatic stress disorder and depression.23,24 Interestingly, Bisson et al detected a prevalence of posttraumatic stress disorder of 27% among patients at 7 weeks following facial trauma, which was unexpectedly high.22 Therefore, follow-up visits provide an opportunity for surgeons to screen for these problems and make a referral to mental health services in a timely manner.25 Screening is a relatively simple procedure, but it is underestimated in common clinical practice. Emotional problems are often kept hidden, but have potentially catastrophic consequences if they remain undiagnosed.24 On the other hand, we did not identify any significant differences in the “Emotional wellbeing” domain between older patients and the referent population. The most probable explanation is that older patients are less concerned with facial appearance and socioeconomic status.
In contrast to younger patients, the “physical health” dimension was severely affected in older patients. Even though the older patient group in this study was 6.3 years younger than the referent population, meaning that rapid recovery was expected, older patients achieved noticeably lower results in the “Physical functioning” domain, as compared to the referent population. Significantly, multiple linear regression has additionally confirmed that age is the most significant determinant of an adverse “physical health” dimension of life quality following facial surgery, among other investigated health aspects (type of fracture and time period after surgery). With increasing age, there was a significant deterioration in the PCS index as well as in the “Physical functioning”, “Pain”, and “General health” domains, which all represent the “physical health” dimension of patient life quality. These findings suggest that midface injury may lower physical capacity and remarkably delay recovery in older patients. Also, it emphasizes the importance for physicians to closely monitor patient improvement and include patients in rehabilitation treatment, if necessary.25–27
After we compared patient life quality and the type of fracture, we were unable to identify a clear statistical correlation. Some have said that maxillary and zygomatic fractures have a similar degree of severity, but that is not unconditionally true.1 Thus, the absence of a clear difference may lie in the relatively small sample size. However, we noticed that with a more extensive maxillary fracture, there is an obvious decrease in the PCS index and, even more notably, in the MCS index. Furthermore, multiple linear regression revealed the Le Fort I fracture, in comparison to different types of fractures, as a significant determinant of life quality. The patients in this group have significantly improved functioning in the “Energy/fatigue” domain, which is in concordance with the anatomical extent of a Le Fort I fracture and with the extent of the surgical approach (mostly transoral, less invasive). Therefore, our results follow the direction of the findings of Girotto et al, which reported that patients with a comminuted Le Fort fracture have achieved lower results in the “mental health” dimension of life quality, as compared to other examined fracture types. Also, similar to our study, they showed that patients with less severe facial injuries have reported better health-related quality of life outcomes.4
Finally, multiple linear regression showed that the time period following surgery was a significant determinant of the PCS index in both patient age groups. This finding highlighted the significance of time period since surgery as a predictor of improvement in the “physical health” dimension of patient life quality.
The strength of the current study lies in the presence of the large national CroHort study, which provided comprehensive data about the health of the Croatian population, including health-related quality of life data.16 Therefore, we were able to conduct the best possible comparison of our midface surgically treated patients, given that the referent CroHort population is representative by age, gender, and region affiliation.
The current study has several possible limitations. Because midface fractures have a low incidence and trauma patients are frequently reluctant to participate in research, the sample size was relatively small. However, the participation rate of 70% represents a very satisfactory result when it’s compared with other similar studies.9,22 In addition, we wanted similar proportions of maxillary and zygomatic fracture patients in our sample but considering that maxillary fractures are not as frequent as zygomatic fractures, we had to expand the inclusion period of our study to 10 years. Hence, the time moment of SF-36 assessment following surgery among patients was different, but on the other hand, it gave us an opportunity to investigate the impact of the time period since surgery on patients’ quality of life. Furthermore, this study included only male patients due to the epidemiological nature of facial injuries, which are far more common in male populations.5,6 Finally, some might argue that the older patient group of this study was 6.3 years younger than the referent population, but we believe that the difference is negligible.
Conclusion
The HRQOL was mostly comparable between our investigated group (male patients after surgically treated maxillary and zygomatic fractures) and the Croatian population norm. Younger patients following this type of trauma had a significantly lower score in the “Emotional wellbeing” domain of the SF-36. They can experience adverse psychological sequelae, which are preventable if they are detected on time. Therefore, follow-up visits are an opportunity to screen the patients and to refer them to mental health services, if necessary. A multidisciplinary team that includes a mental health professional is recommended for this type of trauma. So far, psychological issues as a result of facial trauma have not been approached adequately. On the other hand, older patients are more inclined to physical dysfunction; therefore, prolonged rehabilitation is advisable. We believe that our results laid a solid foundation for further large multicenter research that will thoroughly examine repercussions of midface fractures on the patient life quality over time, with advisable inclusion of mandible fractures that might have a different effect on the studied outcome.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This research was carried out by the Department of Maxillofacial and Oral Surgery at the University Hospital of Split, Croatia.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Erdmann D, Follmar KE, Debruijn M, et al. A retrospective analysis of facial fracture etiologies. Ann Plast Surg. 2008;60:398–403. doi:10.1097/SAP.0b013e318133a87b
2. Katzen JT, Jarrahy R, Eby JB, et al. Craniofacial and skull base trauma. J Trauma. 2003;54:1026–1034. doi:10.1097/01.TA.0000066180.14666.8B
3. Lupi-Ferandin S, Galic T, Ivkovic N, et al. Prevalence of obstructive sleep apnea in male patients with surgically treated maxillary and zygomatic fractures. Can J Surg. 2019;62:105–110. doi:10.1503/cjs.002818
4. Girotto JA, MacKenzie E, Fowler C, et al. Long-term physical impairment and functional outcomes after complex facial fractures. Plast Reconstr Surg. 2001;108:312–327. doi:10.1097/00006534-200108000-00005
5. Kostakis G, Stathopoulos P, Dais P, et al. An epidemiologic analysis of 1142 maxillofacial fractures and concomitant injuries. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:S69–S73. doi:10.1016/j.tripleo.2011.08.029
6. Ansari MH. Maxillofacial fractures in Hamedan province, Iran: a retrospective study (1987–2001). J Craniomaxillofac Surg. 2004;32:28–34. doi:10.1016/j.jcms.2003.07.010
7. Manson PN, Clark N, Robertson B, et al. Subunit principles in midface fractures: the importance of sagittal buttresses, soft-tissue reductions, and sequencing treatment of segmental fractures. Plast Reconstr Surg. 1999;103:
8. Manson PN, Hoopes JE, Su CT. Structural pillars of the facial skeleton: an approach to the management of Le Fort fractures. Plast Reconstr Surg. 1980;66:54–62. doi:10.1097/00006534-198007000-00010
9. Levine E, Degutis L, Pruzinsky T, et al. Quality of life and facial trauma: psychological and body image effects. Ann Plast Surg. 2005;54:502–510. doi:10.1097/01.sap.0000155282.48465.94
10. Monson E, Caron J, McCloskey K, et al. Longitudinal analysis of quality of life across the trauma spectrum. Psychol Trauma. 2017;9:605–612. doi:10.1037/tra0000254
11. Sharma G, Kaur A. Quality of life after orbito-facial trauma. Orbit. 2017;36:407–410. doi:10.1080/01676830.2017.1337204
12. Conforte JJ, Alves CP, Sanchez Mdel P, et al. Impact of trauma and surgical treatment on the quality of life of patients with facial fractures. Int J Oral Maxillofac Surg. 2016;45:575–581. doi:10.1016/j.ijom.2015.11.022
13. Zwingmann J, Hagelschuer P, Langenmair E, et al. Lower health-related quality of life in polytrauma patients: long-term follow-up after over 5 years. Medicine (Baltimore). 2016;95:e3515. doi:10.1097/MD.0000000000003515
14. Rozario D. How well do we do what we do, and how do we know it? The importance of patient-reported experience measures in assessing our patients’ experience of care. Can J Surg. 2019;62:E7–E9. doi:10.1503/cjs.006618
15. Vuletic S, Polasek O, Kern J, et al. Croatian Adult Health Survey–a tool for periodic cardiovascular risk factors surveillance. Coll Antropol. 2009;33(Suppl 1):3–9.
16. Uhernik AI, Vuletic S, Kern J, et al. The Croatian adult health cohort study (CroHort) –background, methodology & perspectives. Coll Antropol. 2012;36(Suppl 1):3–7. doi:10.5671/ca.2012361s.3
17. Ware JE
18. Maslic Sersic D, Vuletic G. Psychometric evaluation and establishing norms of Croatian SF-36 health survey: framework for subjective health research. Croat Med J. 2006;47:95–102.
19. Herce Lopez J, Rollon Mayordomo A, Lozano Rosado R, et al. Quality of life in long-term oral cancer survivors: a comparison with Spanish general population norms. J Oral Maxillofac Surg. 2009;67:1607–1614. doi:10.1016/j.joms.2008.12.039
20. Lui A, Glynn S, Shetty V. The interplay of perceived social support and posttraumatic psychological distress following orofacial injury. J Nerv Ment Dis. 2009;197:639–645. doi:10.1097/NMD.0b013e3181b3b127
21. Sahni V. Psychological Impact of Facial Trauma. Craniomaxillofac Trauma Reconstr. 2018;11:15–20. doi:10.1055/s-0037-1603464
22. Bisson JI, Shepherd JP, Dhutia M. Psychological sequelae of facial trauma. J Trauma. 1997;43:496–500. doi:10.1097/00005373-199709000-00018
23. Gandjalikhan-Nassab SA, Samieirad S, Vakil-Zadeh M, et al. Depression and anxiety disorders in a sample of facial trauma: a study from Iran. Med Oral Patol Oral Cir Bucal. 2016;21:e477–82. doi:10.4317/medoral.21068
24. Glynn SM, Shetty V. The long-term psychological sequelae of orofacial injury. Oral Maxillofac Surg Clin North Am. 2010;22:217–224. doi:10.1016/j.coms.2010.01.008
25. Choudhury-Peters D, Dain V. Developing psychological services following facial trauma. BMJ Qual Improv Rep. 2016;5:
26. Ologunde R, McLeod NMH. Use of patient-reported outcome measures in oral and maxillofacial trauma surgery: a review. Br J Oral Maxillofac Surg. 2018;56:371–379. doi:10.1016/j.bjoms.2018.03.010
27. De Sousa A. Psychological issues in acquired facial trauma. Indian J Plast Surg. 2010;43:200–205. doi:10.4103/0970-0358.73452
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.