")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Health-Related Quality of Life and Its Associated Factors Among Burn Patients at Governmental Referral Hospitals of Amhara Regional State, Northwest Ethiopia, 2020: Institutional-Based Cross-Sectional Study
Authors Tibebu NS , Desie T , Marew C , Wubneh M , Birhanu A , Tigabu A
Received 10 February 2021
Accepted for publication 29 March 2021
Published 13 April 2021 Volume 2021:14 Pages 367—375
DOI https://doi.org/10.2147/CCID.S306211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Nigusie Selomon Tibebu,1 Tigabu Desie,1 Chalie Marew,1 Moges Wubneh,2 Adane Birhanu,2 Agimasie Tigabu2
1Department of Pediatrics and Child Health Nursing, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Adult Health Nursing, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Tigabu Desie
Pediatrics and Child Health Nursing @ Debre Tabor University, P.O.Box:272, Debre Tabor, Ethiopia
Email [email protected]
Introduction: Burns can have a considerable negative impact on physical and psychosocial functioning that affects the quality of life. The physical and psychological manifestations may compromise the quality of life of burned patients. The aim is to assess health-related quality of life and associated factors among burn patients at Amhara regional state governmental referral hospitals, Northwest Ethiopia, 2020.
Methods: Institution-based cross-sectional study was conducted from June 01 to July 15, 2020, in Amhara National regional state governmental referral hospitals. Systematic random sampling technique was used, and data were collected using structured Burn Specific Health Scale Brief Questionnaire through face-to-face interview and document review from patients time since burn 15 days and above. Data were entered into Epidata, and analysis was done by SPSS version 25. Descriptive statistics were computed, and binary logistic regression analysis was used to determine the association between the dependent and independent variables. Variables with a p-value of ≤ 0.05 in the multivariable analysis were considered statistically significant.
Results: Of 423 study participants, 95.7% responded completely. Among the respondents, 58.8% (group mean and median of 18.38 and 21) for physical domain and 57% (group mean and median of 44.73 and 53) for generic domains had a poor health-related quality of life. Overall poor health-related quality of life was 57.5% with a mean of 63.12. Third-degree burn, exposed burnt body part, total body surface area burned ≥ 20%, having an amputation and having a co-morbid illness with (P = 0.001) were associated with poor health-related quality of life.
Conclusion and Recommendation: This study revealed that more than half of the burn survivors had poor health-related quality of life. There shall be strengthened long-term physical and psychosocial domains (generic) intervention for burn survivors by giving more concern for those with the identified risk factors.
Keywords: Amhara, burn injury, Ethiopia, quality of life
Background
A burn is an injury to the skin or other tissue primarily caused by heat or due to radiation, radioactivity, electricity, friction, or contact with chemicals.1 In developing countries, burn incidences are drastically higher than in developed countries and the majority of these occur in low- and middle-income countries and almost two-thirds occur in the WHO African and south-east Asia regions.2 Burn injuries are classified as one of the most devastating of all injuries and major global public health crises. It is a serious pathology, potentially leading to severe morbidity and significant mortality and it has also a considerable health-economic impact.3
Surviving a severe burn injury is considered a traumatic experience. Due to substantial improvements in burn treatment, an increasing number of patients survive burns.4 Burns can have a considerable negative impact on daily activities and both physical and psychosocial functioning.5
The life of patients’ greatly affected in various aspects especially those who had severe and extensive burns.6,7 Disability in burn injury, especially the scars, may remain for several years, or even decades, and are considered the biggest problems for the patient’s QoL.8
Burns are potentially fatal injuries demanding specific upkeep and recovery as well as long-term hospitalization. During hospitalization, patients experience painful day-to-day procedures of wound cleaning and debridement; most of them also need excision and split-thickness autografts. At discharge, recovery is far from complete and the rehabilitation phase normally lasts longer periods.9 Various numbers of psychological or psychiatric abnormalities have been detected in burned patients during hospitalization. In one study, in excess of reaction to physical pain was the greatest prevalent complaint among the burned,10 while another study identified disturbed sleep and anxiety in approximately 50% of the patients.11
A further study reported that one-third of the patients experienced post-traumatic stress disorder.12 Evidence showed that confusion states and 20% of burn patients develop delirium, mainly at the beginning of hospitalization and mostly among severely burned patients.13
A study in Italy showed QoL is compromised in burn patients after hospital discharge; burn injury causes chief restrictions that range well beyond the physical area and involve emotional social and relational aspects.14 In a cross-sectional study conducted to assess QoL in Burn Injury Patients in Patiala QoL was poor in burn-injured patients and was affected by the severity of burn injury.15
The physical, psychological, and psychosocial manifestations may compromise the QoL of burned patients.16 Emotional problems and severity of the burn are important factors that can impair the QoL over time.17
Scarring and contractures are among the most common and difficult sequelae to treat in a burn injury. Burn injury to the head, neck, and face is associated with visible scars. Scars in visible areas are associated with social anxiety, avoidance, and poor QoL.18
Therefore, to prevent burn-related complications and keeping the good health-related quality of life among burn survivors is depended on the evidence.
In Ethiopia, the occurrence and health-related QoL in burn injuries have not been given attention. This can mainly be attributable to the lack of information on the magnitude and extent of the problem. Furthermore, the physical and psychosocial issues in the burn patient are profound. Psychological recovery parallels with physical recovery, so a survey on quality of life among burn patients needs to be addressed and the patients’ physical and psychological status upheld. Therefore, this study was intended to assess health-related QoL and associated factors among burn patients in Amhara national regional state. It will be used for health care providers to overcome the consequences of burn among the burn victims, and the patients will obtain appropriate intervention based on the identified problem in the region.
Methods and Materials
Study Area and Period
The study was conducted in Amhara National regional state governmental referral hospitals. Amhara Region is a regional state in Northern Ethiopia, and its capital is Bahir Dar. The region has only six referral hospitals until the end of this study. The study was conducted in three randomly selected referral hospitals. The region has 13 administrative zones with a total population of 20,018,988.19 Gondar University specialized referral Hospital is the oldest hospital in the country which is located in Gondar city, 750 km northwest of Addis Ababa (the capital city of Ethiopia). Felege Hiwot Referral Hospital and Tibebe Gion specialized teaching hospital are located in Bahir Dar (the capital city of Amhara National Regional State), 562 km northwest of Addis Ababa and 180 km southeast of Gondar. The study was conducted from June 01 to July 15, 2020.
Study Design and Participant Characteristics
An institution-based cross-sectional study design was conducted in Amhara national regional state referral hospitals. All burn patients who had to follow-up in Amhara referral hospitals were considered as source population and the study population was all selected burn patients in selected hospitals who fulfill inclusion criteria and available during the data collection period. Age greater than 18 years and time since burn 15 days and above who avail during the data collection period were included. However, patients who were mentally incompetent or critically ill (unable to give information) during data collection were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined by using single population proportion formula and the following assumptions were made during calculation. By our search; since there is no prior study done in Ethiopia on burn-related quality of life the sample size was calculated by considering, P = 50%, Level of confidence = 95%, and Margin of error (d) =5%.
Where n =sample size needed
P= the probability of good health-related quality of life among burn survivors
Z=significance level at a confidence interval of 95%
d=margin of error (0.05)
Z α/2=value of the standard normal distribution corresponding to a significant level of alpha (α) 0.05 which is 1. 96
By adding 10% non-response rate the final sample size was 423.
In Amhara regional state there were 06 governmental referral hospitals three representative hospitals were selected by lottery method which were half of the hospitals in the region. These were Gondar specialized referral hospital, Feleg Hiywot referral hospital and Tibebe Gion Teaching referral hospital. Average number of clients who received burn-related services at each facility in one month preceding the data collection period was taken from each hospital and by proportional allocation for each institute 164, 132, and 127 study subjects were participated from a total patient flow of 476, 383 and 367, respectively, in which the information has obtained from the hospital registration book of the selected hospitals. Then, divided by the calculated sample size (1228/423=3) to determine the interval (k-value) that was used to select the study participants. By using systematic random sampling technique the participants were selected with every 3 intervals and the first participant was selected by using lottery method.
Variables of the Study
Dependent Variable
Health-related quality of life
Independent Variables
Age, sex, educational level, marital status, occupation, place of burn, affected body part, %TBSA, cause of burn, depth of burn, types of complication, co-morbidities, and time since burn.
Operational Definition
Health-related QOL was assessed by recasting the participants to respond 30 burn-specific questions (BSHS-B) and each questions were have five options (12). The physical domain 9 questions (score 0–36) and psychosocial/Generic domain 21 questions (score 0–84); Then (BSHS-B) mean value of the response was considered to categorize participants as having good or poor quality of life for each domain. The overall health-related quality of life was also calculated by calculating the mean of 30 questions (score 0–120).
Poor QOL included those participants who had responded below the BSHS-B mean value of from those burn-specific questions.
Data Collection Tool and Techniques
Data were collected and registered by using a structured questionnaire. The data was collected using structured Burn Specific Health Scale Brief Questionnaire that adopted from WHO through face-to-face interview by applying COVID 19 preventive mechanisms and document review. Document review was conducted for those burn-related factor questions and length of time since burn. Six BSc nurses were recruited as data collectors. Training was given to them regarding appropriate use of the data collection instruments focusing on uniform interpretation of questions strict use of study criterion, explanation of study objectives, and getting consent from study participants. The questionnaire was translated into a local language which is Amharic (local language) version and back to English version by then utilized to collect the necessary information to assess QoL. Continuous supervision and daily checkup for content completeness and accurateness of the collected data were done.
Data Quality Assurances
A pretest was conducted on 5% (22 from Debre Tabor Hospital) of the sample size to check whether the questions to be interviewed are understandable by the respondents. Also, the internal reliability of the tool was checked and its Cronbach alpha coefficient value was 0.82–0.94.
Data Processing and Analysis
The data were checked for completeness and consistency. Data were also coded, filtered, and entered into Epi data version 4.6.0.0 and then exported to SPSS version 25 for analysis. Descriptive statistics were computed and the results have described in percentage and frequency using tables and BSHS-B mean was performed for each domain. Binary logistic regression analysis was used to determine the association between the dependent and independent variables. First bivariate logistic regression analysis was performed to assess the association of each independent variable with the outcome variable. Then, variables with a P-value of ≤0.25 in the bivariate analysis were included in the final model of multivariable analysis. The assumptions for multiple logistic regressions were checked and fulfilled. The goodness of fit was tested by Hosmer–Lemeshow test and was fitted to the model and it was 0.302. The direction and strength of statistical association were measured by the odds ratio with 95% CI. In multivariable analysis, the association between independent variables in association to the outcome variables which was measured using adjusted odds ratios, 95% confidence interval (CI), and P values of less than or equal to 0.05 was considered as statistically significant.
Ethical Considerations
Ethical clearance was obtained from the Ethical Review Committee of College of health science on behalf of Debre Tabor University. The verbal informed consent was acceptable and approved by the Ethical review board on the behalf of university, and that this study was conducted under the declaration of Helsinki. In addition to that, permission has been obtained from referral hospitals in Amhara national regional state to carry out the study. Verbal informed consent was obtained for each study participant; which has assured that participation is voluntary and they were informed that as there is not any incentive or harm for their participation in this study. To keep the anonymity of study participants, code numbers rather than personal identifiers were used during data collection and analysis. Confidentiality of information was secured by keeping the questionnaires and data in a secured place.
Result
Socio-Demographic Characteristics of Study Participants
Of 423 samples 405 respondents were participated with a response rate of 95.8%. Among the participant, 173 (42.7%) of them were in age groups between 18 and 30 years and the mean age of the respondents was 35.2 with SD ± 14.05 years and around two-third (69.4%) of the respondent were male (Table 1).
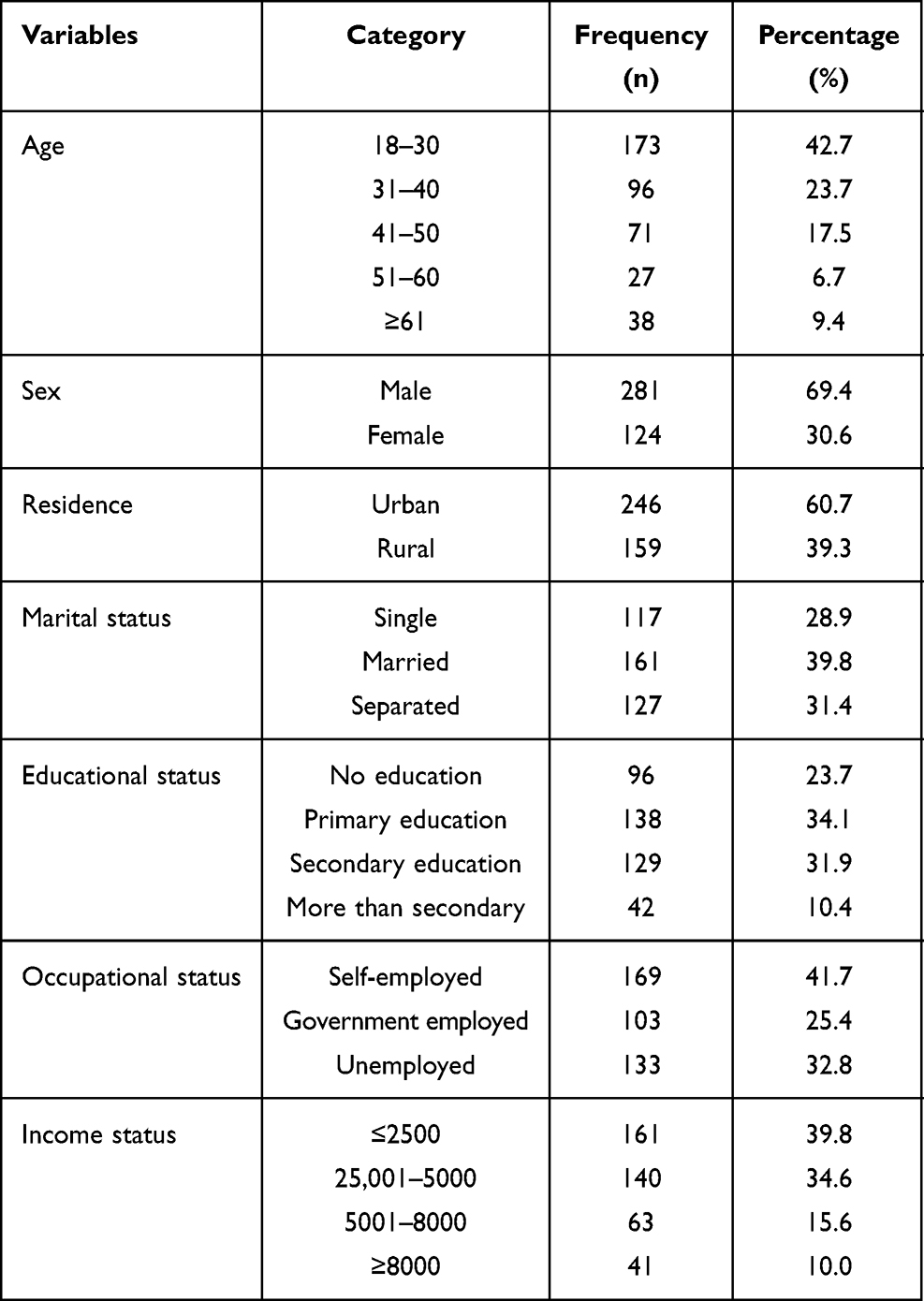 |
Table 1 Socio-Demographic Characteristics of Respondents at Amhara Regional State Referral Governmental Hospitals, Northwest Ethiopia from June 01 to July 15, 2020 (n=405) |
Burn-Specific Factors
Nearly half of the respondents 174 (43.0%) were encountered scald burn and 152 (37.5%) of them have trunk burns. Regarding the burn depth, 188 (46.4%) had 3rd-degree burn, 76.0% had ≥20% TBSA and around one-third of the study participants were with the complication of amputation (Table 2).
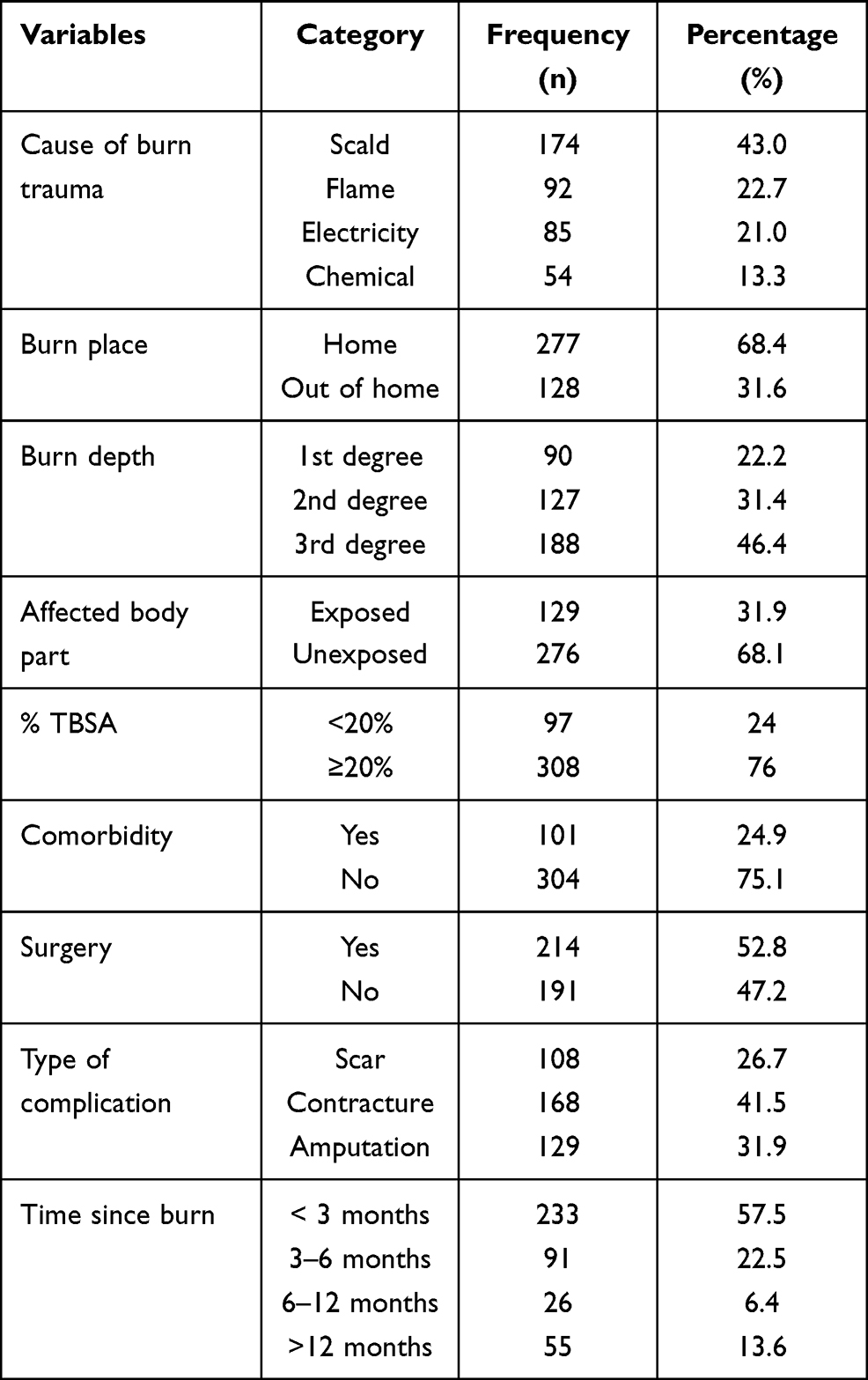 |
Table 2 Burn-Specific Factors Responded by Participants at Amhara Regional State Referral Governmental Hospitals, Northwest Ethiopia from June 01 to July 15, 2020 (n=405) |
In our study adjusted BSHS-B survey tool for assessing the quality of life of burn survivors responded by participants; around one-third of (28.4%) the study participants were had extreme difficulty in bathing independently and 109 (26.9%) were extremely not interested in doing things with their friends (Table 3).
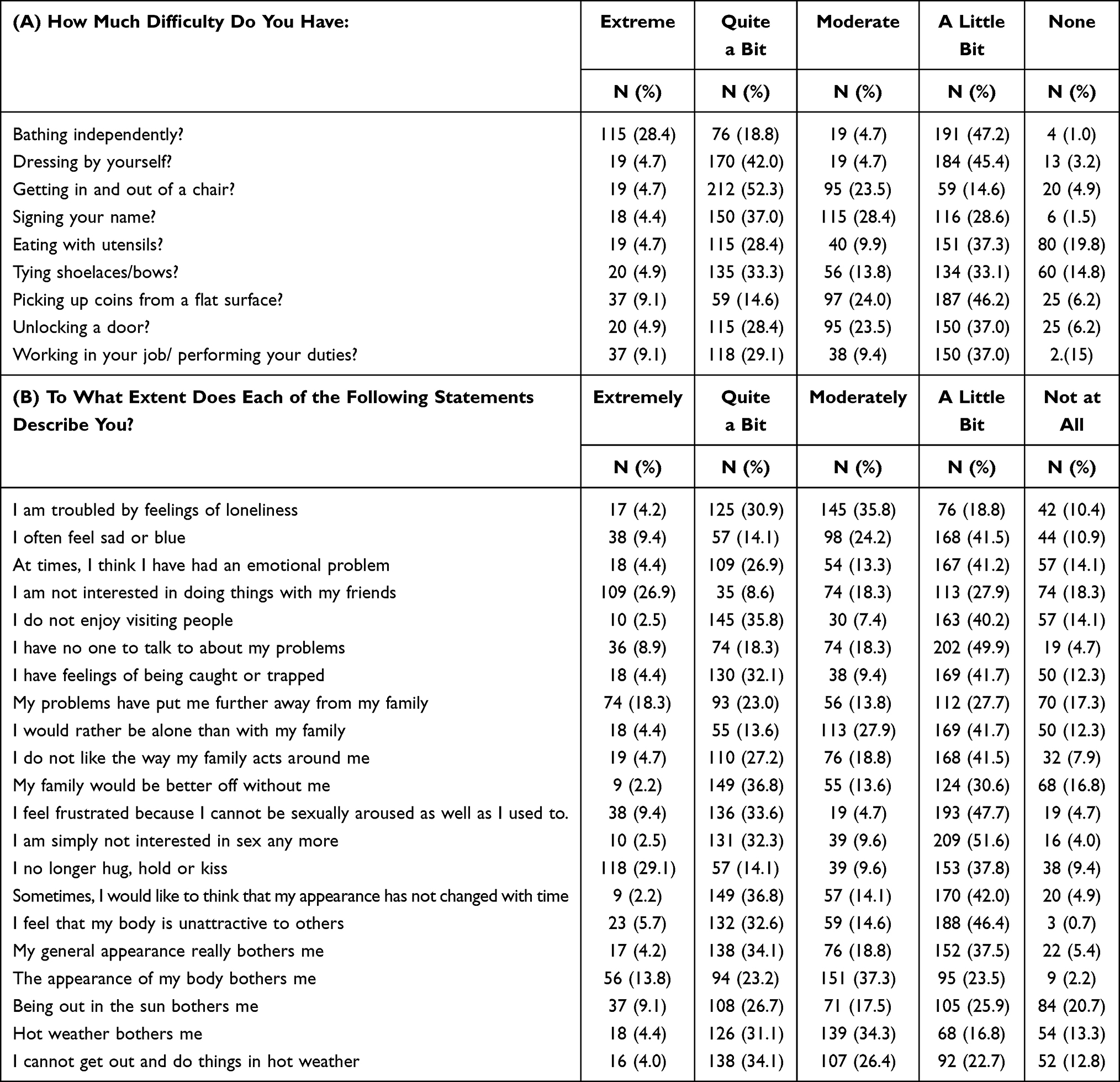 |
Table 3 Adjusted BSHS-B Survey Tool for Assessing Quality of Life of Burn Patients Responded by Participants at Amhara Regional State Referral Governmental Hospitals, Northwest Ethiopia from June 01 to July 15, 2020 (n=405) |
Health-Related Quality of Life Among Burn Patients
Among the respondents; 58.8% (BSHS-B group mean and median of 18.38 and 21) for physical domain and 57% (BSHS-B group mean and median of 44.73 and 53) for generic domains had a poor health-related quality of life. The overall health-related quality of life of study participants in this study revealed that 57.5% (BSHS-B group mean and median of 63.24 and 76.00 with Std. of 23.6) respondents had poor quality of life.
Factors Associated with Health-Related Quality of Life Among Burn Patients
From the 16 socio-demographic and burn-specific factors seven independent variables were associated with the outcome variables during bivariate analysis. Variables with a P value less than or equal to 0.25 were entered into multivariable logistic regression. Finally, 5 variables were associated with multivariable analysis. Those variables associated with the outcome variables were third-degree burn (AOR: 4.37; 95% CI (2.37, 8.03)), exposed burnt body part (AOR: 2.93; 95% CI (1.74, 4.93)), % TBSA > 20% (AOR: 3.40; 95% CI (1.91, 6.07)), having amputation (AOR: 2.48; 95% CI (1.33, 4.63)) and having comorbid illness (AOR: 3.73; 95% CI (2.03, 6.88)). Those burn patients, who had a comorbid disease, were 3.7 times more likely to have a poor quality of life than participants without comorbidity. Those respondents who had third-degree burns were 4.4 times more likely to have a poor quality of life compared to those first-degree burn survivors (Table 4).
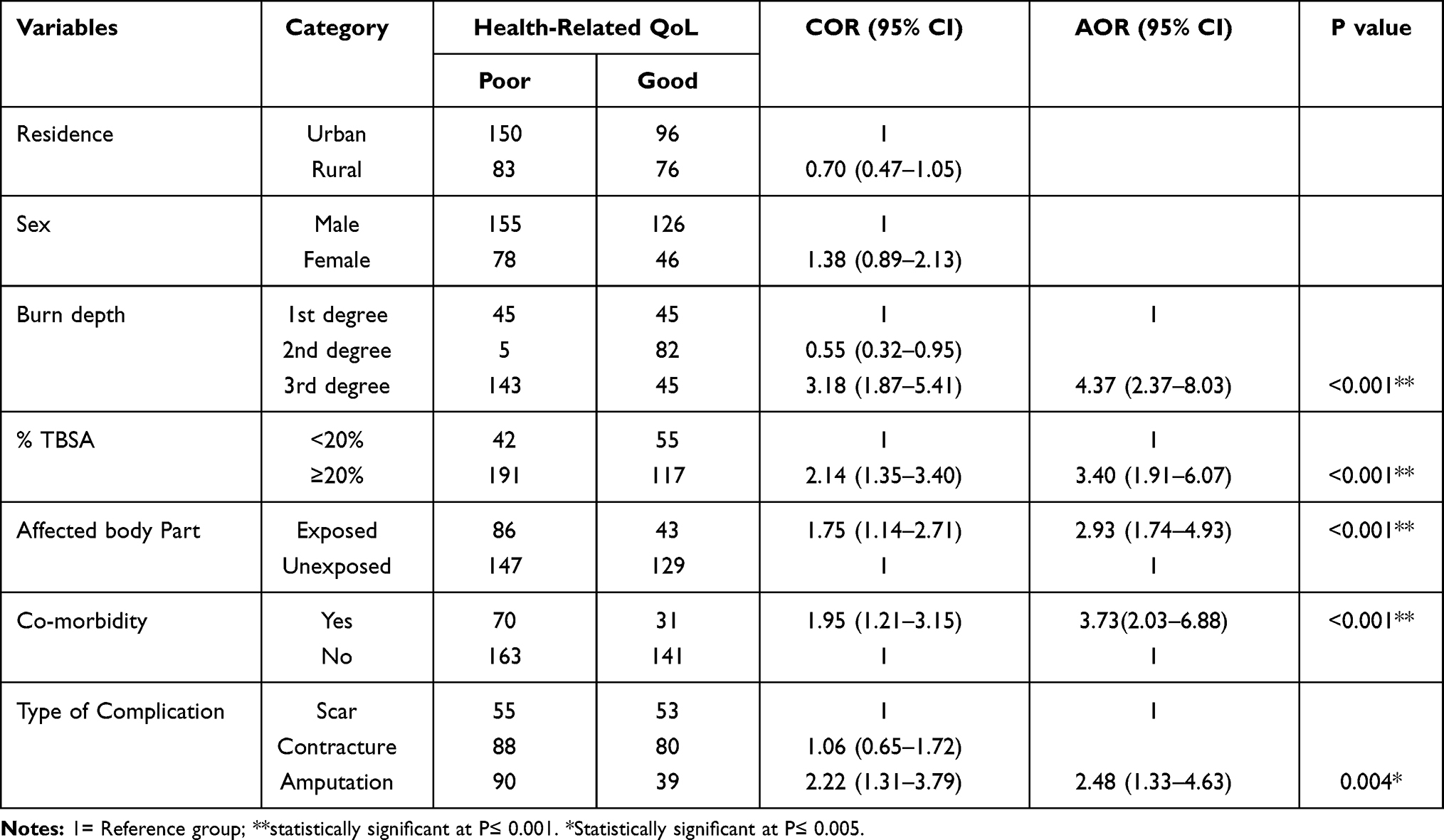 |
Table 4 Factors Associated with Health-Related Quality of Life Among Burn Patients at Amhara Regional State Referral Governmental Hospitals, Northwest Ethiopia from June 01 to July 15, 2020 (n=405) |
Discussion
Burn injuries are global health problems that result in increased mortality and decreasing QoL among burn survivors. So focusing on health-related QoL among burn survivors is essential to enhance the quality of life of the burn victims.
The main purpose of this study was to assess the quality of life and associated factors among burn patients in governmental referral hospitals of Amhara regional state. Study participants were burn patients on follow-up in selected governmental referral hospitals of Amhara regional state.
From the total of participants (N=405), 57.5% (95% CI, (52.8%, 62.2%) of them had poor quality of life. This proportion indicated that the QoL among burn patients is found to be poor. This finding shows that better QoL than the study had done in Sweden; in which 33% of the respondents have poor health-related QoL.18 Burn depth, % TBSA, type of complication, comorbidity, and affected body parts were associated with the outcome variable.
In this finding having third-degree burn were four times more likely to have poor QoL than those having first-degree burn. This is because the more severe the burn, the higher risk for the victim to accomplish the overall basic needs for life as a person. This is in line with the study conducted in Sweden showed that full-thickness burn injuries were had poor QoL than first-degree burns.18 It is also supported by the study done in Italy showed that those patients who had severe burn were challenged by poor QoL.20 It is also supported by the systematic review, which indicated that the severity of burns is a strong predictor of health-related quality of life following burns. More severe burns generally result in a poorer quality of life.21 The result also aligned with a study in Australia revealed that increased percentage of full-thickness burns per body surface area was a important predictor of poorer physical health status.22
Those participants having larger total surface area damage were three times higher to have poor QoL than with those who had smaller surface area burned participants. This is because the participants with extensive burn are more vulnerable to different risks like widespread disfiguring, a dalliance in healing than participants who get small surface area burn. This finding is similar to evidence which showed that the higher percent of total body surface area burn had a negative impact on health dimensions.20 It was also similar to a study done in Iran which showed that those participants who had a burn of large total body surface area were more likely to had poor quality of life than those with small body surface area victims.23
Finding revealed that those respondents who had an injury on their exposed body part were 2.9 times more likely to had poor QoL than those who had an injury on the unexposed body part. This is because injury on visible areas results in the victim to feel inferior to non-victims by comparing himself/herself with society. This study is supported by the study done in India indicated that the involvement of exposed parts, facial burn resulted in poor quality of life.24
The finding from this study showed that those burn injury survivors who have co-morbid illness were 3.7 times more likely to have a poor quality of life than those who had not comorbid illness. This finding is supported by the study conducted in Sweden, Patiala, china, and India which showed that having depression and psychiatry disorders was associated with poor quality of life.18,24–26 This is due to the reason that those who have comorbid illness in addition to burn injury have limited activity and have high chance of developing psychological distress which results in inability to perform a daily activity.27 This condition makes the patient have poor quality of life.
Finding from this research revealed that those burn injury survivors who had amputations were 4.4 times more likely to had poor quality of life than those who had scar after burn injury. This is because those who had amputation cannot perform their activity and they might be dependent on other to fulfill their daily need. This complication may also lead the patient to have low self-esteem, poor body image, and feel body is unattractive to others.27 These all things together lead the patient to have poor quality of life.
Strength: The study tried to investigate a new problem that had not conducted before nationally. It has used an instrument that is validated and standardized Adjusted BSHS-Brief tool.
Limitation: Since the cross-sectional nature of the study limiting it to show a causal association. Since the study has used close-ended questions it might limit the participants’ responses.
Conclusion and Recommendation
This study revealed that more than half of burn survivors had poor health-related quality of life. Having third-degree burn, larger % TBSA, affected body part on the exposed area, having an amputation as complication and having co-morbid illnesses were the predictors of poor health-related quality of life for burn victims.
Amhara national regional Health Bureau Better to establish burn rehabilitation center in the regional state. As well as treatment center shall emphasize the improvement of quality of life for those burn survivors. Health care providers shall have strengthened long-term physical and psychosocial intervention for burn survivors; especially those with larger % TBSA, deep burn injury, affected body part on HEENT, amputation, and those who had co-morbid illness. At last; researchers better to investigate by adding qualitative methods and other study designs.
Abbreviation
AOR, Adjusted Odds Ratio; BSHS-B, Burn Specific Health Scale Brief; CI, Confidence Interval; COR, Crude Odds Ratio; EQ-5D, EuroQol 5 Dimension; EQ VAS, EuroQol Visual Analogue Scale; HRQoL, Health-Related Quality of Life; QoL, Quality of Life; TBSA, Total Body Surface Area; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon request from the corresponding author.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Ethical Review Committee of College of health science on behalf of Debre Tabor University. The verbal informed consent was acceptable and approved by the Ethical review board on the behalf of university, and that this study was conducted under the declaration of Helsinki. In addition to that, permission has obtained from respective referral hospitals in Amhara national regional state to carry out the study. Verbal informed consent was obtained for each study participants; which have assured that participation is on voluntarily basis and they were informed that as there is no incentive or harm for their participation in this study. To keep the anonymity of study participants, code numbers rather than personal identifiers were used during data collection and analysis. Confidentiality of information was secured by keeping the questionnaires and data in a secured place.
Acknowledgment
The author acknowledged co-authors, data collectors, and supervisors. The author is also deeply acknowledging Debre Tabor University. Last but not least, the respondents deserve sincere thanks for their kind responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Callaway MV, Connor SR, Foley KM. World Health Organization public health model: a roadmap for palliative care development. J Pain Symptom Manage. 2018;55(2):S6–S13. doi:10.1016/j.jpainsymman.2017.03.030
2. WHO. The Global Burden of Disease; 2018.
3. Park JO, Do Shin S, Kim J, Song KJ, Peck MD. Association between socioeconomic status and burn injury severity. Burns. 2009;35(4):482–490. doi:10.1016/j.burns.2008.10.007
4. Tompkins RG. Survival from burns in the new millennium: 70 years’ experience from a single institution. Ann Surg. 2015;261(2):263. doi:10.1097/SLA.0000000000000623
5. Ardebili FM, Nejad MB, Manzari ZS. Burn injury in Mottahari Burn Center in Tehran, Iran. World J Plast Surg. 2016;5(1):77.
6. Klinge K, Chamberlain DJ, Redden M, King L. Psychological adjustments made by postburn injury patients: an integrative literature review. J Adv Nurs. 2009;65(11):2274–2292. doi:10.1111/j.1365-2648.2009.05138.x
7. Othman N, Kendric D, Windi A. Epidemiology of burns and the outcome of management in Sulaimaniyah, Iraq: a prospective study. BMC Public Health. 2010;10(1):83. doi:10.1186/1471-2458-10-83
8. Jasper S, Rennekampff O, de Zwaan M. Psychiatric co-morbidity, body image problems and psychotherapeutic interventions for burn survivors: a review. Psychother Psychosom Med Psychol. 2013;63(11):423–428. doi:10.1055/s-0033-1343463
9. Esselman PC, Thombs BD, Magyar-Russell G, Fauerbach JA. Burn rehabilitation: state of the science. Am J Phys Med Rehabil. 2006;85(4):383–413.
10. Patterson DR, Carrigan L, Robinson R, Questad KA. Post-traumatic stress disorder in hospitalized patients with burn injuries. J Burn Care Rehabil. 2013;11:181–184. doi:10.1097/00004630-199005000-00002
11. Gunning A, van Heijl M, van Wessem K, Leenen L. The association of patient and trauma characteristics with the health-related quality of life in a Dutch trauma population. Scand J Trauma Resusc Emerg Med. 2017;25(1):41. doi:10.1186/s13049-017-0375-z
12. Zhang LJ, Cao J, Feng P, et al. Influencing factors of the quality of life in Chinese burn patients. Investigation with adapted Chinese version of the BSHS-B burns. Burns. 2014;40(4):731–736. doi:10.1016/j.burns.2013.09.011
13. Arceneaux L, Meyer III WJ. Treatment for common psychiatric conditions among children and adolescents during acute rehabilitation and reintegration phases of burn injury. Int Rev Psychiatry. 2009;21(6):549–558. doi:10.3109/09540260903343984
14. Novelli B, Melandri D, Bertolotti G, Vidotto G. Quality of life impact as outcome in burns patients.. G Ital Med Lav Ergon. 2009;31(1 SUPPL A):A58–A63.
15. Malik P, Garg R, Sharma KC, Jangid P, Gulia A. Quality of life in burn injury patients. Delhi Psychiatry J. 2012;15:308–315.
16. Mohammadi AA, Tohidinik HR, Zardosht M, Seyed Jafari SM. Self-burns in Fars Province, Southern Iran. World J Plast Surg. 2016;5:32–36.
17. Pishnamazy Z, Asiabar AK, Karimavi MH, Zaeri F, Zadeh RN. Quality of life in burn patients. J Payesh. 2012;11:103–110.
18. Akimenko MA. Vladimir mikhailovich bekhterev. J Hist Neurosci. 2007;16:100–109. doi:10.1080/09647040600550541
19. Population projection of Ethiopia for all regions at Wereda level from 2014 – 2017
20. Suppl AP. Quality of life impact as outcome in burns patients. G Ital Med Lav Ergon. 2009;31(1 SUPPL A):A58–A63.
21. Spronk I, Legemate CM, Dokter J, Van Loey NE, van Baar ME, Polinder S. Predictors of health-related quality of life after burn injuries: a systematic review. Critical Care. 2018;22(1):1–3. doi:10.1186/s13054-018-2071-4
22. Wasiak J, Lee SJ, Paul E, et al. Predictors of health status and health-related quality of life 12 months after severe burn. Burns. 2014;40(4):568–574. doi:10.1016/j.burns.2014.01.021
23. Kazemzadeh J, Rabiepoor S, Alizadeh S. The quality of life in women with burns in Iran. World J Plast Surg. 2019;8(1):33–42. doi:10.29252/wjps.8.1.33
24. Jain A, Rathore S, Jain R, Gupta ID, Choudhary GL. Assessment of depression and the quality of life in burn patients seeking reconstruction surgery. Indian J Burns. 2015;23(1):37.
25. Öster CR, Willebrand M, Ekselius L. Burn-specific health 2 years to 7 years after burn injury. Trauma Acute Care Surg. 2013;74(4):1119–1124.
26. Xie B, Xiao S-C, Zhu S-H, Xia Z-F. Evaluation of long term health-related quality of life in extensive burns: a 12-year experience in a burn center. Burns. 2012;38(3):348–355. doi:10.1016/j.burns.2011.09.003
27. Division TETACFT Burn clinical practice guideline.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.