")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Health-Related Quality of Life Among Persons Living with HIV/AIDS in Jordan: An Exploratory Study
Authors Algaralleh A , Altwalbeh D , Al-Tarawneh F
Received 22 August 2020
Accepted for publication 18 November 2020
Published 11 December 2020 Volume 2020:12 Pages 897—907
DOI https://doi.org/10.2147/HIV.S277941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Abdulnaser Algaralleh,1 Diala Altwalbeh,2 Fatima Al-Tarawneh2
1Department of Counseling and Special Education, Faculty of Educational Sciences, Mutah University, Mutah, Jordan; 2Department of Allied Medical Sciences, Faculty of Karak, Al-Balqa Applied University, Karak, Jordan
Correspondence: Abdulnaser Algaralleh Email [email protected]
Introduction: Diagnosis of HIV/AIDS infection can have adverse effects on the individual and may affect health-related quality of life (HRQoL). Numerous studies have previously assessed the HRQoL of persons living with HIV/AIDS (PLWHA) globally, but not in Jordan. The aim of the current study is to examine HRQoL among PLWHA residing in Jordan and to evaluate the effect of socio-demographic and disease-related factors on HRQoL.
Methodology: An exploratory approach employing a cross-sectional design was applied. The study applied a semi-structured face-to-face interview followed by administration of self-reported questionnaire using the World Health Organization’s Quality of Life HIV brief questionnaire (WHOQOL-HIV-BREF).
Results: Results showed that unemployment, low income, non-disclosure status, single status (separated, divorced or widowed), and having comorbidities were connected with poor HRQoL.
Conclusion: PLWHA require more than just being provided with antiretroviral therapy to rebuild their lives.
Keywords: health-related quality of life, PLWHA
Introduction
The Human Immunodeficiency Virus (HIV) is a retrovirus that is known to attack the immune system in human beings. Initially, an HIV infection has mild symptoms, so patients often mistake it for the flu. However, as the retrovirus further weakens the immune system, increasingly complex signs emerge; these include extreme weight loss, coughing, diarrhea, and swollen lymph nodes. When the immune system turns very weak, the person ends up seriously ill and may even develop other illnesses, diseases, and cancers such as meningitis, tuberculosis, and lymphoma. At this advanced stage, typically ten to fifteen years after the HIV infection, individual develop Acquired Immunodeficiency Syndrome (AIDS).1
HIV/AIDS has become a serious public health problem worldwide since it has affected millions of people across the globe. According to the Joint United Nations Program on HIV/AIDS (UNAIDS), nearly 37.9 million people throughout the world had HIV/AIDS in 2018. Out of these, 36.2 million were adults, and 1.7 million were children. The epidemic in the Middle East and North Africa (MENA), where Jordan is located, also shows a 10% increase in new infections and a 9% extend in the annual number of AIDS-related deaths between 2010 and 2018. But overall, MENA region gets the lowest HIV prevalence in the world (less than 0.1%), with 240,000 documented cases of HIV in 2018.2
Advances in medical care and access to antiretroviral therapy (ART) have significantly enhanced the outcomes for persons living with HIV/AIDS (PLWHA). In fact, it can be said that ART has transformed HIV infection into a chronic controllable but not yet curable disease, and the life expectancy of PLWHA has been prolonged significantly.3 However, better life expectancy also means that PLWHA might have to deal with an increased risk of prolonged morbidities that could be brought on by side-effects of administered medication as well as age-related comorbidities such as: cancers, diabetes, cardiac and pulmonary disease.4 Because of these changes, the primary intention behind caring for PLWAH has shifted toward enhancing their health-related quality of life (HRQoL).5 HRQoL is of significant importance for those living with chronic illnesses wherein therapeutic objectives extend beyond cure to include inhibiting the progression of the disease, decreasing the aftereffects of some debilitating symptoms, improving abilities, and modifying the adverse psychosocial consequences that may accompany the disease.6
Health-Related Quality of Life Among PLWHA
Healthcare providers across the world are making significant progress towards achieving the UNAIDS 90-90-90 HIV objectives: 90% of HIV infected persons will be detected, 90% of those detected will be on sustained ART, and 90% of those on ART will be virally suppressed. Given the transformation of HIV-AIDS from a lethal illness to a chronic condition, a fourth concept of 90 is being considered. Herein suitable HRQoL is held in equal significance to the other three.7 The Centers for Disease Control and Prevention (CDC) defines HRQoL as “an individual’s or group’s perceived physical and mental health over time. p.8”8
Numerous studies have previously assessed the HRQoL of PLWHA globally. These studies may vary in terms of their findings and the effects of the disease and other determinant factors on the different life’s dimensions. The adverse effects of HIV on HRQoL have been confirmed by many pieces of research,9–11 especially when contrasted with the general population,12–14 and to other chronic diseases such as diabetes mellitus type 2 and rheumatoid arthritis.15 In contrast, one study reported enhancement in quality of life because of lifestyle modification after HIV diagnosis.16
The determinants of HRQoL amongst PLWHA were summarized in two contemporary literature reviews,17,18 and two metanalyses,19,20 they comprised several sociodemographic, clinical, psychological, and behavioral elements. Notably, stigma, decrease socioeconomic status, unemployment, insufficient social support, being under 35 years, advancing HIV stage, having symptoms of HIV/AIDS, decreased immunological status, decreased adherence to ART, low CD4+ T cell count, and psychiatric and physical comorbidities were linked continuously with poorer HRQoL. Previous reviews showed contradictory results regarding ethnicity, gender, and partners' relationship with HRQoL. This might be because of the divergences in the population, research methodologies used in those studies, as well as the timeframe during which HRQoL was studied.
Most of the published studies were carried out in United States, South Africa, India, Brazil, China, Uganda, Canada, Thailand, England, and Australia.21 No published literature could be found on the quality of life of PLWHA in the Arab world, except one study from Lebanon conducted by Abboud and colleagues in 2010.22
HIV/AIDS Status in Jordan
Jordan, with Amman as its capital, is an Arab country situated in the MENA region. Its total population is 10 million.23 In terms of epidemiology, Jordan has one of the lowest rates of HIV/AIDS, with an anticipated prevalence rate of 0.02% among the overall population. As of December 2017, the cumulative number of HIV/AIDS cases was 1408, which includes 383 Jordanians, of whom 129 have died (34%), this indicates that 254 cases were alive in Jordan as of 2017. About 71% and 6% of registered HIV/AIDS cases get the infection through sexual behaviors and drug use, respectively. However, these numbers fail to show the real magnitude of the HIV/AIDS problem in Jordan because a reliable surveillance is yet to be conducted.24 Since the first case of AIDS was diagnosed in Jordan in 1986, the Ministry of Health (MOH) has established the Jordan National AIDS Program (NAP) to combat AIDS and offer free ART to PLWHA. Additionally, MOH is making sturdy efforts to control the HIV/AIDS epidemic in collaboration with local and global institutions and partners such as community-based organizations (CBOs), non-governmental organizations (NGOs), government agencies, as well as global organizations.24
Several studies were conducted to learn more about the Jordanians’ knowledge, attitude and practices (KAP) – for the general population,25 University students,26,27 dentists,28 dental college students,29 nurses,30,31 Islamic religious leaders,32 men who have sex with men.33 In addition, the Department of Statistics (DOS) also conducts the recurrent “Jordan Population and Family Health Survey,” which offers the most up-to-date statistics about HIV/AIDS-related knowledge and attitudes.34 All these studies were descriptive, cross-sectional, either quantitative or qualitative, and they reflected a lack of information and fear of the disease, in addition to undeniable stigma and discriminatory attitudes towards PLWHA. Like many other countries in MENA region, the stigma is related to the public’s perception of HIV/AIDS as associated with marginalized groups such as injecting drug users, prostitutes, and homosexuals.35 However, none of these studies assessed actual PLWHA.
Existing conditions of increasing coverage of HIV testing and ART treatment for HIV infection in Jordan may lead to an increase in the life expectancy in PLWHA. Hence, assessment of the quality of life and its related factors among PLWHA should become a focus of HIV/AIDS care too. Though HRQoL in the PLWHA has not been before assessed in Jordan. The current study aimed to examine HRQoL among PLWHA residing in Jordan, and to evaluate the effect of sociodemographic and disease-related factors on quality of life. This primary step will facilitate the development of a holistic, evidence-based care program for this vulnerable group of people.
Methodology
Since it was the first study to assess the HRQoL among PLWHA in Jordan, an exploratory approach with a cross-sectional design was applied. The study took place over the course of four months in the summer of 2019. Eighteen respondents participated from Amman city through a nonprofit community base organization “CBO” that provides unpublicized consultations and supports for PLWHA. The study applied a semi-structured face-to-face interview followed by the administration of a self-reported questionnaire. Each respondent was interviewed by one of the researchers and asked a set of open-ended questions concerning some matters stated in the literature or questioned by the CBO’s staff, as the researchers needed to know more about them from the sufferers’ point of view.
The first question was about the disclosure of their HIV positive status; whether the respondent readily disclosed his/her HIV positive status to family and friends; yes or no; and why and when. They were also asked about the other’s willingness and acceptance of their disease. Further questions concerning disclosure were asked irrespective of their disclosure statuses, such as their willingness to inform the doctors, nursing or medical laboratory staff about their HIV serostatus if the condition requires this, their willingness to contribute to educational campaigns for at-risk groups, if the respondents know other PLWHA, and do they want to know other PLWAH. The second question explored how the infection affected the respondent regarding relationship with spouse, work, and spirituality. The third question was about the healthcare team; if the respondents found the healthcare team helpful, and if they had been treating the respondent with dignity or not. The fourth asked what must be done by the government to improve PLWAH quality of life. The remaining question was about any demanding matters the respondent wants to share with the researcher.
In the self-reported questionnaire, respondents were asked to judge their HRQoL over the past two weeks using WHO’s Quality of Life HIV brief questionnaire (WHOQOL-HIV-BREF), that is a multidimensional instrument with 31 facets divided into six domains: physical, psychological, level of independence, social relationships, environment and spirituality/religion/personal beliefs. The first two facets in the WHOQOL-HIV-BREF examine the HRQoL: question 1 investigates the general evaluation of the respondent’s quality of life, and question 2 evaluates their over-all health perceptions, totaling 31 items. Of these 31 facets, five are particular to PLWHA: symptoms, forgiveness and blame, social inclusion, worries about the future, as well as death and dying. A Likert type scale is used to score the questions where 1 indicates low negative perceptions, and 5 indicates high positive perceptions. Scores in the 6 negatively phrased questions were reversed.36 Domain scores were computed according to the instructions of WHOQOL HIV manual. The mean score within each domain is used to compute the domain score. The researchers then multiplied the mean scores by 4 to ensure that the results are comparable to the scores for the WHO Quality of Life-100. In the end, the scores were from 4 (worst) to 20 (best).37
The first portion of WHOQOL-HIV-BREF also included questions about sociodemographic and clinical variables connected with HRQoL, such as gender, age, marital status, education level, HIV serostatus, ART status (adherence or not), the year they were infected, year of diagnosis, and the method of infection. For this study, the researchers added three questions about employment status (either employed or not), income (enough or not), and the existence of other medical comorbidities that were quantified using the Charlson Comorbidity Index (CCI),38 and dichotomized either as having or not having comorbidities.
For the purpose of this study, the researchers worked with two independent bilingual nursing faculty members to translate the WHOQOL-HIV BREF instrument into Arabic. Then, it was translated back into English by other faculty members who had not seen the original survey earlier to ensure the accuracy of the instrument. The faculty members compared the original English version with the back-translated version to pinpoint differences and resolve any discrepancies. The Arabic version was evaluated by a panel of medical, nursing and psychology faculty members for its clarity and appropriateness to be used in the Jordanian society.
Ethical Considerations
Written permission was obtained to use the WHOQOL-HIV-BREF instrument in the course of this study. Mutah University Institution Review Board (IRB) and the selected CBO approved the study. The principles of the Declaration of Helsinki were followed. Each respondent was asked to sign a consent form after a thorough explanation for the study purposes and ensuring the privacy, confidentiality of the information, and the anonymity of their identities.
Data Analysis
The open-ended questions had been transcribed into the English language and analyzed manually. The self-reported questionnaires have been analyzed using the Statistical Package for Social Sciences (SPSS Version 17.0, Chicago, IL, USA). Descriptive statistics were computed for all the variables. Median was used as a cutoff point to transform continuous variables into dichotomous.39 Bivariate analysis was used to scrutinize the associations between sociodemographic and health-related variables with HRQoL results.
Results
First: The Analysis of the Open-Ended Questions
The analysis of the first question revealed that two third (66.7%) of the respondents preferred not to tell anyone about their HIV diagnosis, except for their treating physicians and their husbands or wives. Six respondents restricted the disclosure to one other immediate family member. The main reason for the minimal disclosure is to protect themselves and their families from stigma, discrimination, and shame. Besides, most of those respondents felt that society at large does not sympathize with PLWHA as it does with other illnesses. Most of the respondents think that letting others know about their diagnosis would result in fear, repulsion, rejection, and withdrawal by others. Also, breach of confidentiality is a significant reason for not disclosing. Yet, most of those who reveal their illness in less than one-year post-diagnosis, get a lot of social support and acceptance from people they informed. Additionally, the analysis showed that most of the respondents are ready to report that they have this disease if they consult a doctor, get laboratory tests, undergo a surgical operation, experience a traffic accident, or when they request for a blood donation. However, many respondents are not ready to appear in the media to persuade others of the necessary preventive means, because of the social stigma towards the patient, which often describe them as an immoral person. Besides, the respondents do not know other PLWHA even though most of them want to know other patients like themselves.
As for the second question, about the effect of the disease on marital relations, it was found that all the 9 married respondents got married before they got the infection and all their partners knew about their HIV-positive status. Most of the married respondents stated that the relationship between them and their partners was more friendly and supportive in most cases. There was only one exception, characterized by hatred as once the respondent’s wife knew that her husband had AIDS, she requested a divorce and finalized it soon enough. As for the respondents’ work, 3 of them were dismissed from their jobs after the routine tests showed that they are AIDS positive. One of these cases was for a chef who wanted to work abroad, the tests proved that he had the disease and the work contract was canceled, the other case was for a laboratory technician, and the third case was for a technician for medical devices. As for spirituality, the respondents reacted quite similarly to the news that they were infected. Some of them were surprised and shocked, others denied and did not believe the news of the test, but in the end, everyone surrendered to God’s judgment and destiny. They consider it as a test from God, and they believe that God can rid them from this disease. Most of them become more religious and closer to God through repenting, praying, and reading the Qur’an.
In regards to the health care teams, the results indicated that respondents felt that the government healthcare facilities (NAP clinic) only provided physical treatment (such as free ART, measuring viral load and CD4); they feel that no enough attention was paid to their psychological, social or financial needs. Due to this fact, these respondents gained access to the CBO for its precise HIV-related psychosocial services. Many respondents reported a good relationship with the treating healthcare team at the NAP clinic, and they mentioned that the team treats them respectfully and humanely. 50% of respondents declared that the outsider physicians and nurses are not cooperative and not empathetic; sometimes, the healthcare providers reject them when they know their HIV status. Respondents shared their experiences of refusal from nurses and physicians; one female respondent stated that more than five hospitals did not allow her to give birth inside them.
When asked what the government should do to improve the quality of life for PLWHA, the respondents agreed that they need integrated services in addition to healthcare services. These should include psychological and social care, financial support, and even spiritual support from religious clergy. Moreover, many respondents mentioned that the government should defend their right to work anywhere they want without any discrimination. Moreover, patients demand that the government establish an agency that provides job opportunities for them and helps them find their life partners and spouses. This is important because most HIV/AIDS patients are young, and if they do not get married on time, it may push towards deviant behavior as they may transfer the infection to others.
Regarding the last question about pressing issues they may want to discuss, the respondents pointed to the importance of social sensitization to avoid disgrace and discrimination against them.
Second: Analysis of Sociodemographic and Clinical Factors
When the results for the self-reported questionnaire were analyzed, researchers found that women made up the majority of the participants (55.6%). Additionally, it was found that 88.9% had high school or lower educational levels, 50% were single, and 70% were unemployed. Time since their HIV diagnosis went from 8 months to more than 14 years. 38.9% of the participants had other comorbidities. All of them were receiving ART and were asymptomatic. Majority of respondents (72.2%) got the infection through sexual relationships.
Third: Analysis of WHOQOL-HIV-BREF
The score distribution for each WHOQOL-HIV-BREF domain and individual facets is presented in Table 1. The summary of domain scores were: 12.10 (SD 3.14) for environmental health, 12.67 (SD 3.71) for the level of independence, 12.89 (SD 3.40) for social relationships, 13.89 (3.74) for physical health, 14.00 (SD 3.24) for psychological health and 14.39 (SD 4.19) for spirituality, religion, and personal beliefs. The lowest scores in individual facets were financial resources (mean 2.11 [SD 0.68] and participation in leisure activities (mean 2.50, SD 1.25) in the environmental health domain).
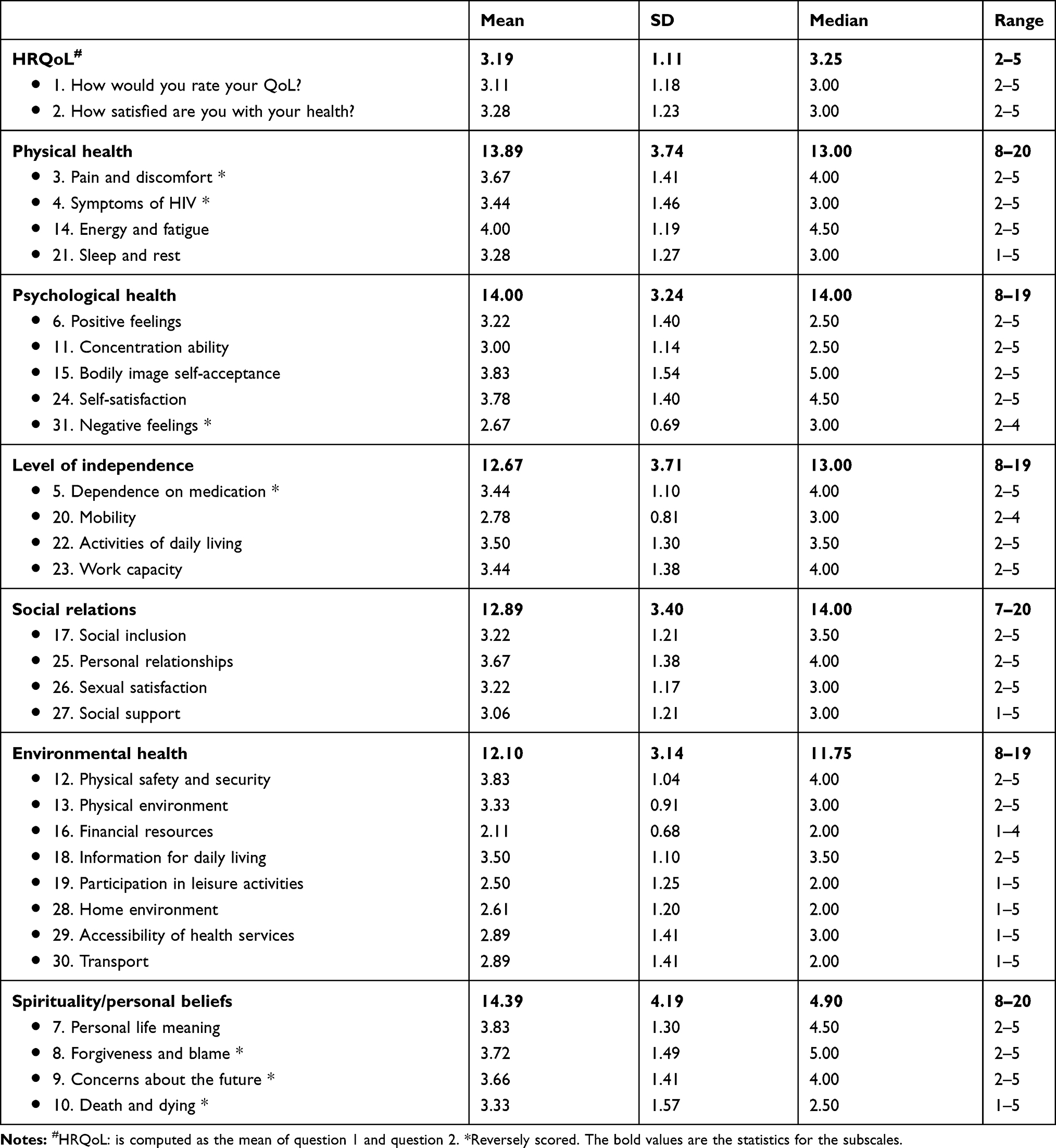 |
Table 1 Descriptive Statistics of the WHOHIV-BREF Domains and Facets (n = 18) |
In line with previous work;40 the mean scores of the first two facets were employed as a measure of HRQoL and considered as a dichotomous variable. Herein participants with mean ratings of >3.0 were considered to have a good quality HRQoL while others with mean ratings of ≤3.0 had a poor HRQoL. The mean scores for HRQoL score 3.19 (SD 1.11). The results showed that about half (50%) of PLWHA in Jordan rated their HRQoL as good and 50% rated it as bad. The bivariate analysis revealed that people who were single, unemployed, from low-income strata and had comorbidities displayed reduced level of HRQoL compared to their counterparts, as shown in Table 2.
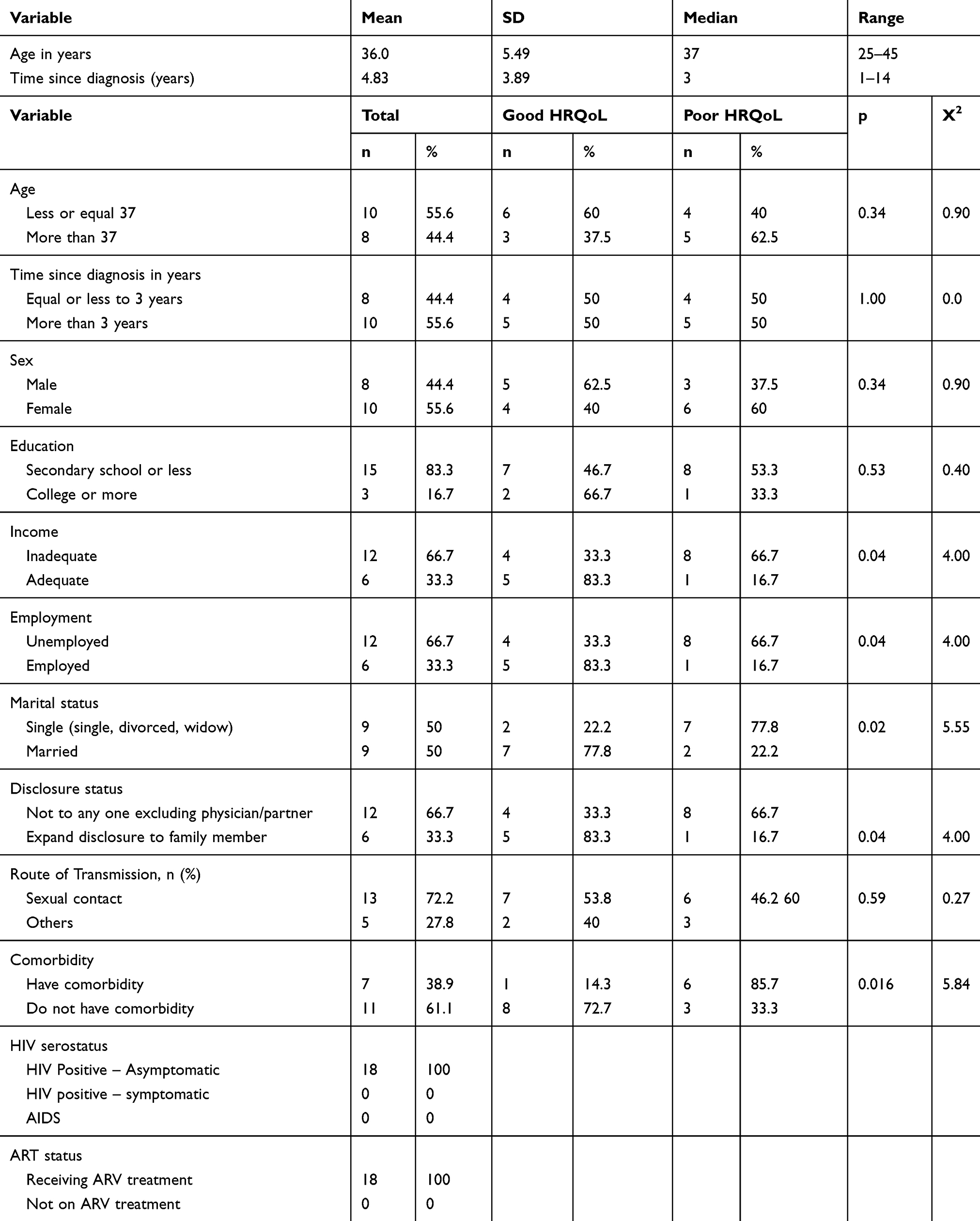 |
Table 2 Socio-Demographic and Clinical Variables for a Sample of 18 Respondents with Good or Poor HRQoL |
Discussion
An HIV diagnosis can harm the individual and may affect their HRQoL. The results of this study showed that 50% of PLWHA in this study manage positively with their HIV infection. This result could be explained by the relatively younger age and asymptomatic serostatus of the respondents, as well as their strict adherence to ARV treatment. Overall, the scores for total HRQoL in our study are generally consistent with data obtained by other researchers from Iran,41 Brazil,42 and China.12,14 The HRQoL scores for PLWHA in Jordan are to some extent lower than other countries such as Finland,43 Kazakhstan,44 and Ghana,45 but higher compared to Nigeria46 and Lebanon.22
The study showed that spirituality was highest rated among quality of life domains. In contrast, the environmental domain ranked lowest, notably for question about financial resources. This was confirmed when we added a question about income and found that inadequate income was correlated with poor quality of life, as will be discussed later. It seems that many of the respondents use religion to help them cope with their condition and help them find the purpose and acceptance of their diagnosis. Islam encourages followers to seek forgiveness and accept the path Allah has chosen for them (AL-Ghadar).47 Daily prayers and recitation of the Qur’an often help people rebuild their relationship with Allah. This is important because many patients often believe that their diagnosis as HIV/AIDS positive was a punishment for straying from the path that Allah has decreed for every Muslim.48 Other cultures also showed similar behaviors where individuals with HIV/AIDS became more devout after being diagnosed.49–51
In this study, the results exhibited that unemployment, low income, non-disclosure status, single status (separated, divorced, or widowed), and having comorbidities related to poor HRQoL.
It is not surprising that PLWHA who are unemployed or had low income reported a low quality of life. Research papers from other countries showed similar findings.17,20,45 Having a job and adequate income can enhance their socioeconomic status and facilitate for them social integration at the same time it gives them better opportunities for health protection and promotion.52 Therefore, respondents said that they want protection from law for their right to work in Jordan, where 90% of women and 87% of men openly discriminate against PLWHA. A recent survey by the DOS revealed that 82% of women and 80% of men refused to buy fresh vegetables if they found out that the vendor is HIV positive.34
Respondents who disclosed their HIV positive status had better HRQoL scores as compared to those who had not disclosed their disease to anyone other than their treating physicians and spouses. This could be explained by the unconditional love, support, and acceptance they received from family, which can help make life better. According to literature, PLWHA should be prepared and supported by health care professionals before they choose to disclose or not.17 This is key to confronting and reducing the stigma and discrimination they face at each step of life.
Additionally, it was found that singlehood is also associated with low HRQoL. This result is consistent with other studies which shows that a steady marital life, where the couple lives together as a family, can lead to higher HRQoL.10,43 That is because a stable family life provides the necessary emotional and social backing to PLWHA.53 Nonetheless, there have also been conflicting reports where patients who are living with a spouse or partner had a much poorer HRQoL than those who remained single.54,55 However, our research found that intimate relationships are essential for a better quality of life. The separated, divorced, and widowed participants in our study scored far worse for general HRQoL as compared to the married participants. Consequently, the single respondents asked for protection for their right to get married and build a family. For example, one participant had even asked his treating physician and CBO staff to help him find a wife.
The result unveiled a negative association between comorbidities and a good quality of life. These findings are in line with other studies carried among HIV patients,17,43,56 and also consistent with another research from Jordan showed that the quality of life for patients in medical-surgical wards with severe comorbidity had been affected negatively as compared to quality of life for patients with no comorbidity and patients with mild comorbidity.57
These conclusions fortify preceding discussions about concentrating on health outcomes that are often beyond the viral suppression for PLWHA. The significant issues discovered here should be taken into consideration when formulating policy for improving both quantity and quality of HIV/AIDS services. Similarly, healthcare providers and students must get holistic training that helps them empathize with the patients so they can provide care in a stigma-free environment. This important; particularly in light of previous studies that showed negative attitudes and limited willingness by healthcare providers to care for HIV-infected persons,28,30 in addition to low level of empathy in general.58
Conclusion
The study found the HRQoL to be moderate at best. However, it was found to be poor among respondents who did not have a job, had inadequate income, did not disclose their illness, were single, and had other comorbidities. It was revealed that PLWHA need more than just antiretroviral therapy to restart their lives. PLWHA require financial and social assistance so they can get used to the new “normal” life. It is also essential to set up community outreach programs to benefit others like the people who participated in this study.
Implications and Recommendations
Assessing the quality of life as part of the routine clinical assessment can help categorize patients with poor quality of life for appropriate interventions. Nurses can be very supportive in this process by identifying patient needs and referring them to suitable solutions in clinical and community settings. It is also essential to train physicians, nurses, social workers, psychologists, and religious clerics to deal with the physical, mental, social and spiritual needs of PLWHA holistically. Establishing a club or association that PLWHA can use to communicate with each other and with the community at large. This way, they can integrate into society to alleviate the social stigma of this disease. Finally, get legislators and policymakers to create special laws to promise the rights of PLWHA so they can have employment, a decent living. The laws should prevent them from being arbitrarily dismissed because of their illness, and guaranteeing them the right to study, get married, and have families and children. At the same time, it should describe their duties towards society, such as practicing caution not to transmit infection.
Limitations
This paper has not been able to provide a comprehensive view of QoL among the PLWHA of Jordan due to the practical constraints of the study, such as the inadequate number of participants. It was not possible to have a conversation with PLWHA who had not registered with the chosen community-based organization. It is also imperative that we consider the sensitive nature of this study and the associated stigma that PLWHA face every day. It can explain why they may not have been able to speak freely to us during the interviews, offering only socially desirable responses that they think people would want to hear. Further research is needed to include more PLWHA and take into account other variables include concurrent psychological morbidities, HIV stigma, and clinical symptoms such as pain and mental function. This should be an essential part of other future studies because these factors do seem to have an impact on the quality of life. To ensure that the studies are conclusive, there should be a comparison with the non-infected population across the country.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. World Health Organization. Fact Sheets/Detail/HIV/AIDS [Internet]. World Health Organization; 2019.
2. Joint United Nations Programme on HIV/AIDS (UNAIDS). Communities at the Centre: Defending Rights, Breaking Barries, Reaching People with HIV Services-Global AIDS Update 2019.[Internet]. 2019.
3. Oguntibeju OO. Quality of life of people living with HIV and AIDS and antiretroviral therapy. Hiv/Aids (Auckland, NZ). 2012;4:117.
4. Maciel RA, Klück HM, Durand M, Sprinz E. Comorbidity is more common and occurs earlier in persons living with HIV than in HIV-uninfected matched controls, aged 50 years and older: a cross-sectional study. Int J Infect Dis. 2018;70:30–35.
5. Drewes J, Gusy B, Ruden U. More than 20 years of research into the quality of life of people with HIV and AIDS – a descriptive review of study characteristics and methodological approaches of published empirical studies. J Int Assoc Provid AIDS Care. 2013;12(1):18–22. doi:10.1177/1545109712456429
6. Megari K. Quality of life in chronic disease patients. Health Psychol Res. 2013;1(3):27. doi:10.4081/hpr.2013.932
7. Kall M, Marcellin F, Harding R, Lazarus JV, Carrieri P. Patient-reported outcomes to enhance person-centred HIV care. Lancet HIV. 2020;7(1):e59–e68. doi:10.1016/S2352-3018(19)30345-5
8. Centers for Disease Control and Prevention. Measuring Healthy Days: Population Assessment of Health-Related Quality of Life. 2000.
9. Bekele T, Rourke SB, Tucker R, et al. Direct and indirect effects of perceived social support on health-related quality of life in persons living with HIV/AIDS. AIDS Care. 2013;25(3):337–346. doi:10.1080/09540121.2012.701716
10. Perez IR, Bano JR, Ruz ML, et al. Health-related quality of life of patients with HIV: impact of sociodemographic, clinical and psychosocial factors. Qual Life Res. 2005;14(5):1301–1310. doi:10.1007/s11136-004-4715-x
11. Vidrine DJ, Amick BC, Gritz ER, Arduino RC. Assessing a conceptual framework of health-related quality of life in a HIV/AIDS population. Qual Life Res. 2005;14(4):923–933. doi:10.1007/s11136-004-2148-1
12. Liping M, Peng X, Haijiang L, Lahong J, Fan L. Quality of life of people living with HIV/AIDS: a cross-sectional study in Zhejiang province, China. PLoS One. 2015;10(8):e0135705. doi:10.1371/journal.pone.0135705
13. Miners A, Phillips A, Kreif N, et al. Health-related quality-of-life of people with HIV in the era of combination antiretroviral treatment: a cross-sectional comparison with the general population. Lancet HIV. 2014;1(1):e32–e40. doi:10.1016/S2352-3018(14)70018-9
14. Lan G, Yuan Z, Cook A, et al. The relationships among social support and quality of life in persons living with HIV/AIDS in Jiangxi and Zhejiang provinces, China. AIDS Care. 2015;27(8):946–953. doi:10.1080/09540121.2015.1011072
15. Engelhard EAN, Smit C, van Dijk PR, et al. Health-related quality of life of people with HIV: an assessment of patient related factors and comparison with other chronic diseases. AIDS. 2018;32(1):103–112. doi:10.1097/QAD.0000000000001672
16. Tsevat J, Leonard AC, Szaflarski M, et al. Change in quality of life after being diagnosed with HIV: a multicenter longitudinal study. AIDS Patient Care STDS. 2009;23(11):931–937. doi:10.1089/apc.2009.0026
17. Degroote S, Vogelaers D, Vandijck DM. What determines health-related quality of life among people living with HIV: an updated review of the literature. Arch Public Health. 2014;72(1):1–10. doi:10.1186/2049-3258-72-40
18. Jin Y, Liu Z, Wang X, et al. A systematic review of cohort studies of the quality of life in HIV/AIDS patients after antiretroviral therapy. Int J STD AIDS. 2014;25(11):771–777. doi:10.1177/0956462414525769
19. Ghiasvand H, Waye KM, Noroozi M, Harouni GG, Armoon B, Bayani A. Clinical determinants associated with quality of life for people who live with HIV/AIDS: a meta-analysis. BMC Health Serv Res. 2019;19(1):768. doi:10.1186/s12913-019-4659-z
20. Ghiasvand H, Higgs P, Noroozi M, et al. Social and demographical determinants of quality of life in people who live with HIV/AIDS infection: evidence from a meta-analysis. Biodemography Soc Biol. 2020;65(1):57–72. doi:10.1080/19485565.2019.1587287
21. Vu GT, Tran BX, Hoang CL, et al. Global research on quality of life of patients with HIV/AIDS: is it socio-culturally addressed? (GAPRESEARCH). Int J Environ Res Public Health. 2020;17(6):2127. doi:10.3390/ijerph17062127
22. Abboud S, Noureddine S, Huijer HA, DeJong J, Mokhbat J. Quality of life in people living with HIV/AIDS in Lebanon. AIDS Care. 2010;22(6):687–696. doi:10.1080/09540120903334658
23. Department of Statistics. Statistical Yearbook of Jordan 2018. Amman; 2018.
24. Rahhal A. Evaluation of HIV/AIDS Activities in Jordan, July 2018. Amman; 2018.
25. Alkhasawneh E, McFarland W, Mandel J, Seshan V. Insight into Jordanian thinking about HIV: knowledge of Jordanian men and women about HIV prevention. J Assoc Nurses AIDS Care. 2014;25(1):e1–e9. doi:10.1016/j.jana.2013.06.001
26. Petro-Nustas W, Kulwicki A, Zumout AF. Students’ knowledge, attitudes, and beliefs about AIDS: a cross-cultural study. J Transcult Nurs. 2002;13(2):118–125. doi:10.1177/104365960201300204
27. Petro-Nustas W. University students’ knowledge of AIDS. Int J Nurs Stud. 2000;37(5):423–433. doi:10.1016/S0020-7489(00)00022-5
28. El‐Maaytah M, Al Kayed A, Al Qudah M, et al. Willingness of dentists in Jordan to treat HIV‐infected patients. Oral Dis. 2005;11(5):318–322. doi:10.1111/j.1601-0825.2005.01126.x
29. Ryalat ST, Sawair FA, Shayyab MH, Amin WM. The knowledge and attitude about HIV/AIDS among Jordanian dental students: (clinical versus pre clinical students) at the University of Jordan. BMC Res Notes. 2011;4(1):191. doi:10.1186/1756-0500-4-191
30. Hassan ZM, Wahsheh MA. Knowledge and attitudes of Jordanian nurses towards patients with HIV/AIDS: findings from a nationwide survey. Issues Ment Health Nurs. 2011;32(12):774–784. doi:10.3109/01612840.2011.610562
31. Nawafleh H, Francis K, Chapman Y. The influence of HIV/AIDS on the practice of primary care nurses in Jordan: rhetoric and reality. Int J Nurs Pract. 2005;11(5):200–205. doi:10.1111/j.1440-172X.2005.00528.x
32. Abu‐Moghli F, Nabolsi M, Khalaf I, Suliman W. Islamic religious leaders’ knowledge and attitudes towards AIDS and their perception of people living with HIV/AIDS: a qualitative study. Scand J Caring Sci. 2010;24(4):655–662. doi:10.1111/j.1471-6712.2009.00757.x
33. Alkaiyat A, Schaetti C, Liswi M, Weiss MG. Condom use and HIV testing among men who have sex with men in Jordan. J Int AIDS Soc. 2014;17(1):18573. doi:10.7448/IAS.17.1.18573
34. Department of Statistics. Jordan Population and Family Health Survey 2017–2018. Amman; 2019.
35. Mumtaz GR, Hilmi N, Majed EZ, Abu-Raddad LJ. Characterising HIV/AIDS knowledge and attitudes in the Middle East and North Africa: systematic review and data synthesis. Glob Public Health. 2020;15(2):275–298. doi:10.1080/17441692.2019.1668452
36. WHOQoL HIV Group. WHOQOL-HIV for quality of life assessment among people living with HIV and AIDS: results from the field test. AIDS Care. 2004;16(7):882–889. doi:10.1080/09540120412331290194
37. World Health Organization. Users’ Manual for Scoring and Coding WHOQOL-HIV Instruments. 2002.
38. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Clin Epidemiol. 1987;40(5):373–383.
39. DeCoster J, Gallucci M, Iselin A-MR. Best practices for using median splits, artificial categorization, and their continuous alternatives. J Exp Psychopathol. 2011;2(2):197–209. doi:10.5127/jep.008310
40. Ruutel K, Pisarev H, Loit HM, Uuskula A. Factors influencing quality of life of people living with HIV in Estonia: a cross-sectional survey. J Int AIDS Soc. 2009;12(1):13. doi:10.1186/1758-2652-12-13
41. Kalan ME, Han J, Taleb ZB, et al. Quality of life and stigma among people living with HIV/AIDS in Iran. Hiv/Aids (Auckland, NZ). 2019;11:287.
42. Hipolito RL, Oliveira D, Costa T, Marques SC, Pereira ER, Gomes AMT. Quality of life of people living with HIV/AIDS: temporal, socio-demographic and perceived health relationship. Rev Lat Am Enfermagem. 2017;25.
43. Nobre N, Pereira M, Roine RP, Sintonen H, Sutinen J. Factors associated with the quality of life of people living with HIV in Finland. AIDS Care. 2017;29(8):1074–1078. doi:10.1080/09540121.2017.1281879
44. Zhakipbayeva BT, Nugmanova ZS, Tracy M, Birkhead GS, Akhmetova GM, DeHovitz J. Factors influencing the quality of life in persons living with human immunodeficiency virus infection in Almaty, Kazakhstan. Int J STD AIDS. 2019;30(13):1318–1328. doi:10.1177/0956462419876484
45. Osei-Yeboah J, Owiredu W, Norgbe GK, et al. Quality of life of people living with HIV/AIDS in the Ho Municipality, Ghana: a cross-sectional study. AIDS Res Treat. 2017;2017:6806951.
46. Abasiubong F, Ekott JU, Bassey EA, Etukumana EA, Edyang-Ekpa M. Quality of life in people living with HIV/AIDS in Niger Delta Region, Nigeria. J Ment Health. 2010;19(2):211–218. doi:10.3109/09638230903469210
47. Omer T, Lovering S, Al Shomrani M. The lived experience of living with HIV/AIDS in the western region of Saudi Arabia. Divers Equal Health Care. 2014;11.
48. Ibrahim K, Songwathana P. Cultural care for people living with HIV/AIDS in Muslim communities in Asia: a literature review. Pac Rim Int J Nurs Res. 2009;13(2):148–157.
49. Arrey AE, Bilsen J, Lacor P, Deschepper R. Spirituality/religiosity: a cultural and psychological resource among Sub-Saharan African migrant women with HIV/AIDS in Belgium. PLoS One. 2016;11(7):e0159488. doi:10.1371/journal.pone.0159488
50. Pinho CM, Dâmaso BFR, Gomes ET, Trajano M, Andrade MS, Valença MP. Religious and spiritual coping in people living with HIV/Aids. Rev Bras Enferm. 2017;70(2):392–399. doi:10.1590/0034-7167-2015-0170
51. Tsevat J. Spirituality/religion and quality of life in patients with HIV/AIDS. J Gen Intern Med. 2006;21(Suppl 5):S1. doi:10.1111/j.1525-1497.2006.00640.x
52. Calixto O-J, Anaya J-M. Socioeconomic status. The relationship with health and autoimmune diseases. Autoimmun Rev. 2014;13(6):641–654. doi:10.1016/j.autrev.2013.12.002
53. Pereira M, Canavarro MC. Gender and age differences in quality of life and the impact of psychopathological symptoms among HIV-infected patients. AIDS Behav. 2011;15(8):1857–1869. doi:10.1007/s10461-011-9928-8
54. Briongos Figuero L, Bachiller Luque P, Palacios Martin T, González Sagrado M, Eiros Bouza J. Assessment of factors influencing health‐related quality of life in HIV‐infected patients. HIV Med. 2011;12(1):22–30. doi:10.1111/j.1468-1293.2010.00844.x
55. Tran BX. Quality of life outcomes of antiretroviral treatment for HIV/AIDS patients in Vietnam. PLoS One. 2012;7(7):e41062. doi:10.1371/journal.pone.0041062
56. George S, Bergin C, Clarke S, Courtney G, Codd MB. Health-related quality of life and associated factors in people with HIV: an Irish cohort study. Health Qual Life Outcomes. 2016;14(1):115. doi:10.1186/s12955-016-0517-4
57. Ahmad MM, Al-Daken L, Ahmad HM. Quality of life for patients in medical–surgical wards. Clin Nurs Res. 2015;24(4):375–387. doi:10.1177/1054773813519470
58. Altwalbeh D, Khamaiseh AM, Algaralleh A. Self-reported empathy among nursing students at a University in Jordan. Open Nurs J. 2018;12(1):255–263. doi:10.2174/1874434601812010255
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.