")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Health-Related Quality of Life Among Myocardial Infarction Survivors: Structural Equation Modeling Approach
Authors Lamesgin Endalew H, Liyew B , Kassew T , Ewnetu Tarekegn G , Dejen Tilahun A, Sewunet Alamneh T
Received 15 February 2021
Accepted for publication 9 June 2021
Published 22 June 2021 Volume 2021:14 Pages 1543—1552
DOI https://doi.org/10.2147/JMDH.S296064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Helen Lamesgin Endalew,1 Bikis Liyew,2 Tilahun Kassew,3 Gebrekidan Ewnetu Tarekegn,4 Ambaye Dejen Tilahun,2 Tesfa Sewunet Alamneh4
1Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Emergency and Critical Care Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Psychiatry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Bikis Liyew
Department of Emergency and Critical Care Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, P.O.Box 196, Gondar, Ethiopia
Tel +251932731964
Email [email protected]
Background: Myocardial infarction is the fifth leading causes of disability-adjusted life years in low-income countries including Ethiopia. The aim of this study was to construct a hypothetical model to determine the factors affecting the health-related quality of life of myocardial infarction survivors at the cardiac center Ethiopia.
Methods: A cross-sectional study design was employed, and 421 myocardial infarction patients were enrolled through consecutive sampling technique from the outpatient clinic at the cardiac center of Ethiopia. The World Health Organization Quality of Life-BREF-26 tool was used to assess the problem. It consists of four domains such as physical, psychological, social relationships, and environmental health domains. The structural equation modeling (SEM) analysis was employed using STATA-14 software to examine the relationship between various exogenous and endogenous or mediating variables with overall quality of life.
Results: Psychological, physical, environmental health domains and sex had significant association with health-related quality of life (β=0.708, p< 0.001, β= 0.237, p=0.046, β=0.242, p=0.020, and β=0.189, p=0.017, respectively), whereas age had direct, negative association with health-related quality of life (β=− 0.007, p=0.026). Residence and level of education were not directly associated with health-related quality of life. Residence indirectly, negatively influenced health-related quality of life (β= − 0.379, p< 0.001). On the other hand, level of education indirectly, positively affects health-related quality of life (β=i0.133, p< 0.001).
Conclusion: Psychological health factors had the most substantial causal effect on health-related quality of life, which was larger than the causal effects of physical and environmental health-related factors. Developing and providing comprehensive interventions are necessary to assess and manage psychological, physical, and environmental health factors and to improve the quality of life in myocardial infarction patients.
Keywords: health-related quality of life, myocardial infarction, structural equation model, Ethiopia
Introduction
Myocardial infarction is a medical term for an event commonly known as a heart attack and it is defined as necrosis of heart muscles due to significant and sustained ischemia.1 It is the fifth leading cause of disability-adjusted life years in low-income countries.2–5 Health-related quality of life is a construct used to understand the impact of chronic disease on patients’ wellbeing.6,7 Even though the survival rate from Myocardial infarction has significantly increased due to the use of most up-to-date management modalities over the last few decades yet, these patients frequently experience negative physiological, psychological problems and a disrupted daily life.8–10 Myocardial infarction (MI) is one of the leading causes of death worldwide.11 The life-threatening nature of the disease, the need for long-term lifestyle changes, and medical regimens after MI often result in reduced health-related quality of life (HRQOL) among patients.12–14
According to World health organization (WHO), MI is the most prevalent condition among men and increases with age and education.15 The sudden and often profound physiological and psychological effects of the acute onset of MI along with the psychosocial impact of hospitalization harms the HRQOL.16 Due to the devastating consequences of MI patients report fear of another cardiac events, decreased energy levels, and an inability to perform their daily activities. They are also faced with the threat of family life changes, marital strain, financial worries, and fewer job opportunities.14,17,18 A case–control study conducted in the United States of America (USA) showed that survivors were approximately 2.7 times more likely to report poor general health compared to non-MI survivors, and 1.5 times more likely to report limitations to daily activities.19 A descriptive study conducted in South Korea also showed that the HRQoL of post-MI patients was moderately poor health-related quality of life.20 In another study conducted in Myanmar the overall HRQOL among MI patients was moderate.14 A descriptive study conducted in India showed that 15%, 63.33%, and 21.67% of MI patients had a good, average, and poor quality of life, respectively.21
Researchers reported that the potential predictive factors for the diminished HRQOL among MI patients are advanced age, female in sex, lower educational attainment, being divorced/widowhood, lower financial status.22–24 Being employed, having poor social support, presence of comorbid heart failure, anxiety and depression are the factors that decreases the likelihood of HRQOL among patients with MI.21,25–27 Patients who had a more active lifestyle, lower alcohol consumption being non-smokers presented higher HRQoL scores than their counterparts.28
Information on HRQoL can play a significant role in the clinical management of patients with cardiac problems, who often experience significant disease burden and need to make lifelong lifestyle modifications, as well as be used in quantifying the impact of the disease. Identifying factors that are significantly associated with HRQoL will serve as a useful guide to improve the patient’s life by preventing the factors. To the best of the researchers’ knowledge, there is no study conducted in our country to assess HRQoL among MI patients. As a result, recommended assessment and treatment approaches regarding this issue remain scarce. Therefore, this study can address the gap by assessing HRQoL among MI patients and their associated factors. Besides, the finding of this research would be input to patient-centered care, clinical decision making, and health policy decisions as well as an audit performance measure. This study aimed to build a HRQOL structural model of patients with MI, and determine the factors that affect the QOL, as well as their direct or indirect relationships.
Conceptual Framework and Hypothesized Model
Conceptual frameworks have been developed primarily to explain the theoretical underpinning of QoL. The four groups of factors influencing the HRQoL of patients with MI were identified through a comprehensive review of the literature (Figure 1).
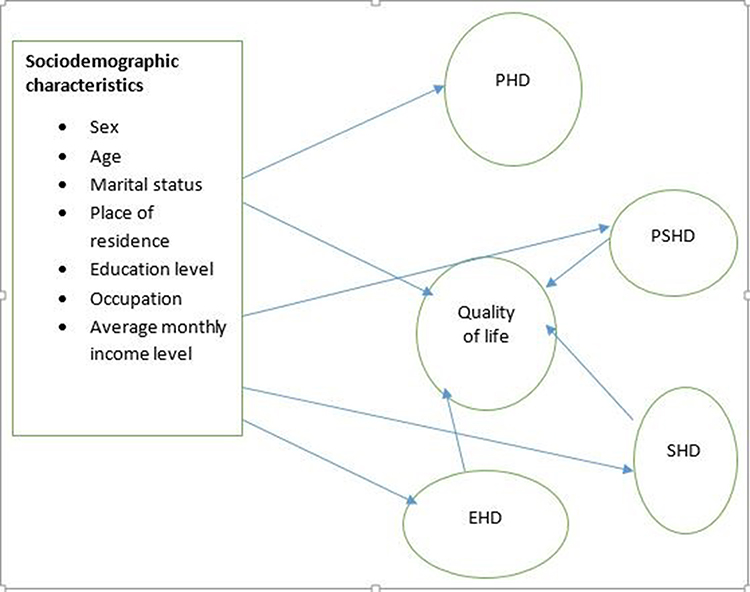 |
Figure 1 A hypothesized model for factors associated with health-related quality of life among myocardial infarction survivors attending at cardiac center Ethiopia. Abbreviations: PH, physical health domain; PSD, psychological health domain; SHD, social health domain; EHD, environmental health domain. Note: Single-headed arrow shows the direction of effect. |
Methods
Study Setting and Population
A cross-sectional study was conducted on patients with myocardial infarction who were attended for follow-up in Cardiac Center of Ethiopia from April 10 to June 25, 2020. It is found in Tikur Anbessa Specialized Hospital, Addis Ababa The facility has 30 beds and gives 24-hour services for both children and adults as deemed necessary. It has a total of 13 heart team members that includes six cardiologists, two cardiac surgeons, two cardiac anesthesiologists, one cardiac intensivist, and two percussionists.29 On average, there had been 600 patients with MI have a regular follow-up at the center in a month. All patients with a diagnosis of MI (both STEMI and NSTEMI), aged 18 years and above, those who have at least three months follow-up were included in the study. While those who were in severe conditions, with cognitive impairment, concurrent diagnosis of life-threatening diseases (eg, cancer), unable to communicate, a chronic severe psychiatric condition (eg, psychosis), and patients on antianxiety or antidepressant medications were excluded from the study.
Sample Size Determination and Sampling Technique
A general rule of thumb is that the minimum sample size should not be less than (K+1)/2 where K is the number of observed variables.18 According to the foregoing rule, the minimum required sample was 406 since we have 28 observed variables.30 A group of 421 patients with MI aged 18 years and above attending the cardiac center for follow-up were invited to took part in the study by a consecutive sampling technique. Data were collected by chart review and face-to-face interview. The necessary sample was taken by specifying all patients during the investigation time frame consecutively until the necessary sample size was gotten. Even if the pattern of follow-up depends on patients’ condition, most of the patients had one follow-up per month. Patients MI diagnosis (such as typical ischemia chest pain, elevated cardiac enzyme levels and typical ECG changes) was confirmed by using medical record.
Data Collection Tool and Measurement of Variables
The four domains of health-related quality of life (HRQOL) were measured by using the World Health Organization Quality of Life BREF (WHOQOL-BREF) tool. The WHOQOL-BREF is a 26-item instrument consisting of four domains: domain 1 (Physical health): pain and discomfort, medication and treatment, mobility, energy and fatigue, sleep and rest, daily activities, working capacity; domain 2 (psychological):positive feelings, negative feelings, self-esteem, memory and concentration, body image, spirituality/religion/personal beliefs, spirituality, religion, and personal beliefs; domain 3 (Social relationships): personal relations, sex, practical social support, and domain 4 (environment): financial resources, information and skills, recreation and leisure, home environment, access to health and social care, physical safety and security, physical environment and transport. Responses to the questions were a 5-point Likert scale, inquiring “how much‟, “how satisfied‟, or “how completely‟ the respondent feels concerning the domains listed. In order to get domain raw score and to make it comparable the average score of all items in each domain was multiplied by four (which ranged from 4 to 20). Then after domain raw score was linearly transformed to domain scores out of 100 (Domain score = (raw score-4)× (100/16)). The overall health-related quality of life was computed as the average of the scores of the four domains. Those respondents who score higher had better HRQOL, whereas, those score lower had the poorer HRQOL. Internal consistency of the WHOQoL –brief questionnaire was calculated for each domain of the instrument using Cronbach’s alpha. All domains of WHOQOL-BREF had high values of Cronbach’s alpha (α > 0.7). Items on socio-demographic, and clinical factors were prepared in accordance with previous works of literatures.21,23,27,31 The socio-demographic and clinical characteristics of the participants included gender, age, marital status, educational level, residency, occupation, monthly income, presence of comorbidity, type of MI, and duration of illness.
Data Collection Procedures
The data were collected using a structured questionnaire by both interviews and reviews of patient medical records. The questionnaire was first prepared in English and translated to Amharic, the working language of Ethiopia, and retranslated to English to maintain consistency. The questionnaire contained socio-demographic, clinical characteristics, and the WHO Quality of Life-BREF (WHOQOL-BREF) questions. First, every participant was interviewed about their socio-demographic characteristics and WHOQOL-BRiEF, and then reviewed the patients medical records regularly regarding clinical variables (eg, type of MI, presence of comorbidity, duration of illness and treatment). Interviews were held in a separate room after getting their service to maintain privacy. The pilot study was done among 40 MI patients at the University of Gondar specialized and Comprehensive specialized hospital. Data were collected by four trained clinical nurses by the Amharic version of the questionnaire for two months. Furthermore, the overall data collection process was closely supervised by the principal investigator and one master’s degree professional nurse. One day of training was given for both data collectors and supervisors for detailed information about the questionnaire before data collection. At the end of data collection, questionnaires were checked for completeness by the supervisor daily. Any ambiguity was addressed by communicating with the data collectors.
Data Processing and Model Building
Data were entered into Epi-info version 7.2.2.6 and analyzed by SPSS version 26 and STATA version 14. In the descriptive analysis, the mean with SD, frequency and percentages were used to see the distribution of the data. Before hypothesis testing, we conducted a correlation analysis using the measured variables. Multicollinearity between the variables was checked by pearson’s correlation coefficient. The absolute values of the correlation coefficients determined between the pairs of all independent variables were <0.70. Therefore, multicollinearity was not present in the data.32 The normality assumption was also checked by kurtosis and skewness. The kurtosis and skewness values for all of the variables used in this study were between ±1.96. So, the assumption of a normal distribution was satisfied.
Structural Equation Modeling (SEM) was employed using STATA-14 software to examine the relationship between various exogenous and endogenous or mediating variables. Because HRQOL and its domains were latent variables that constitute items with ordered responses. Their measurement model was analyzed using SEM because the multivariate normality assumption was satisfied after the items parceling.33 The analysis was started with the hypothesized model (Figure 1), and modifications were performed iteratively by adding path links or including mediator variables. The following tests were used in the goodness-of-fit tests for the model: χ2, comparative fit index (CFI), root mean squared error of approximation (RMSEA); Coefficient of determination (CD); Akaike’s information criterion (AIC); Bayesian information criterion (BIC); Log-likelihood.
Results
Socio‑Demographics’ and Clinical Characteristics
Among the 421 participants, more than half (56.8%) of the participants were male, and the mean age of the participants was 42.55±15.925 years. The majority of the study participant were residents from urban area (82.2%) and unmarried (62.2%). Regarding the educational status, 119 (28.3%) of them had attended secondary school education. The average estimated monthly income of the participants was 2672.41±3620.420 ETB, and 28.3% them were private workers. Twenty nine (6.9%) and 179 (42.5%) of the participants had comorbid heart failure and diabetes mellitus, respectively (Table 1).
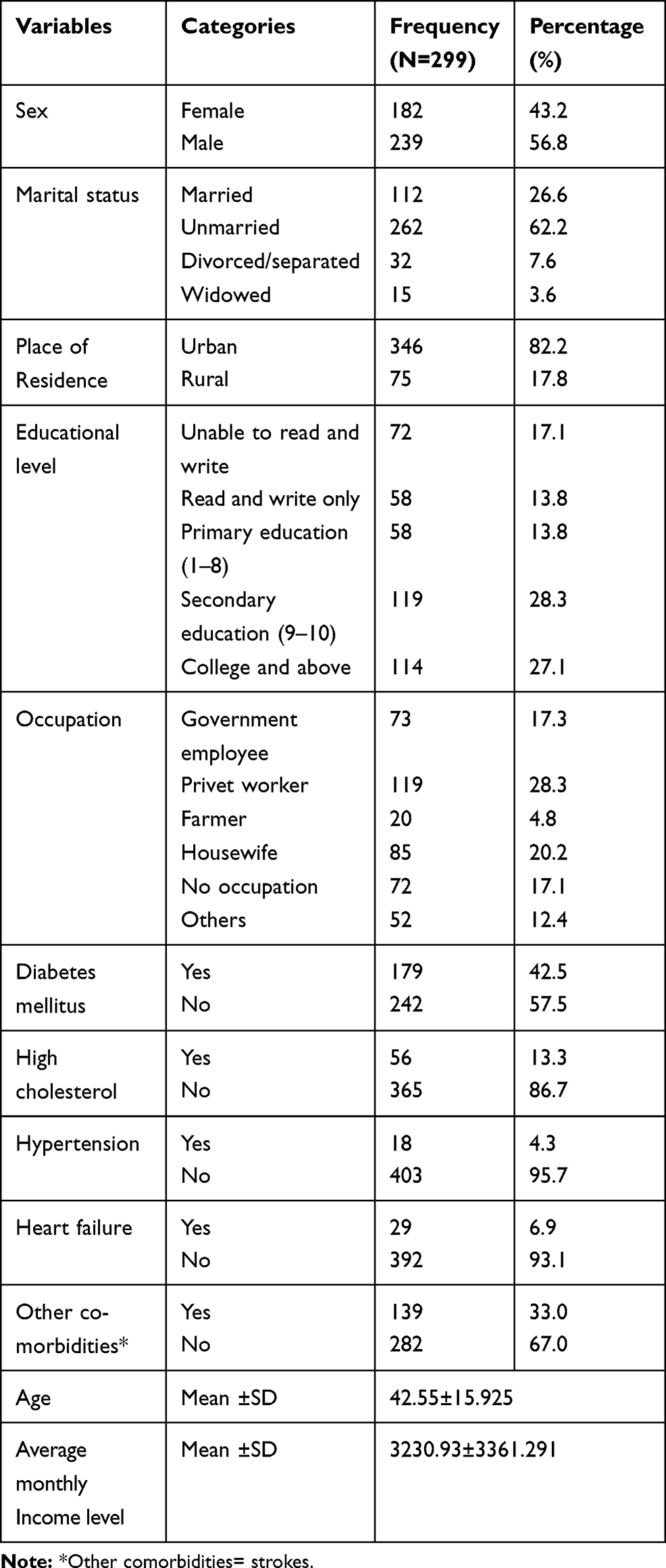 |
Table 1 Socio-Demographics and Clinical Characteristics of Patients with Myocardial Infarction at Cardiac Center, Ethiopia, 2020 (N= 421) |
The overall quality of life among the participant MI patients was 49.29±14.83 and this result indicated the patients had low QOL.() Among the four domains of HRQOL, the participants had highest score in the social health domain (52.02±24.61), and the psychological, physical and environmental health domain scores of the participants were 50.91±16.07, 47.96±16.50 and 46.30±16.54 respectively.
Analysis of the Hypothetical Model
The final hypothetical model has contained both the structural (relationships among latent or observed variables) and measurement parts (the relationship between a latent variable and its indicators or items) (Table 2). The model included only seven exogenous variables (sex, age, monthly income, marital status, occupation, residency, and educational level), four mediator variables (domains of HRQOL), and one endogenous variable (HRQOL). The seven exogenous variables were both, directly and indirectly, related to HRQOL via the mediator variables. The estimated structural equation model showed that the psychological health factor had the most considerable causal effect on HRQOL, which was larger than the causal impacts of physical health and environmental health factors.
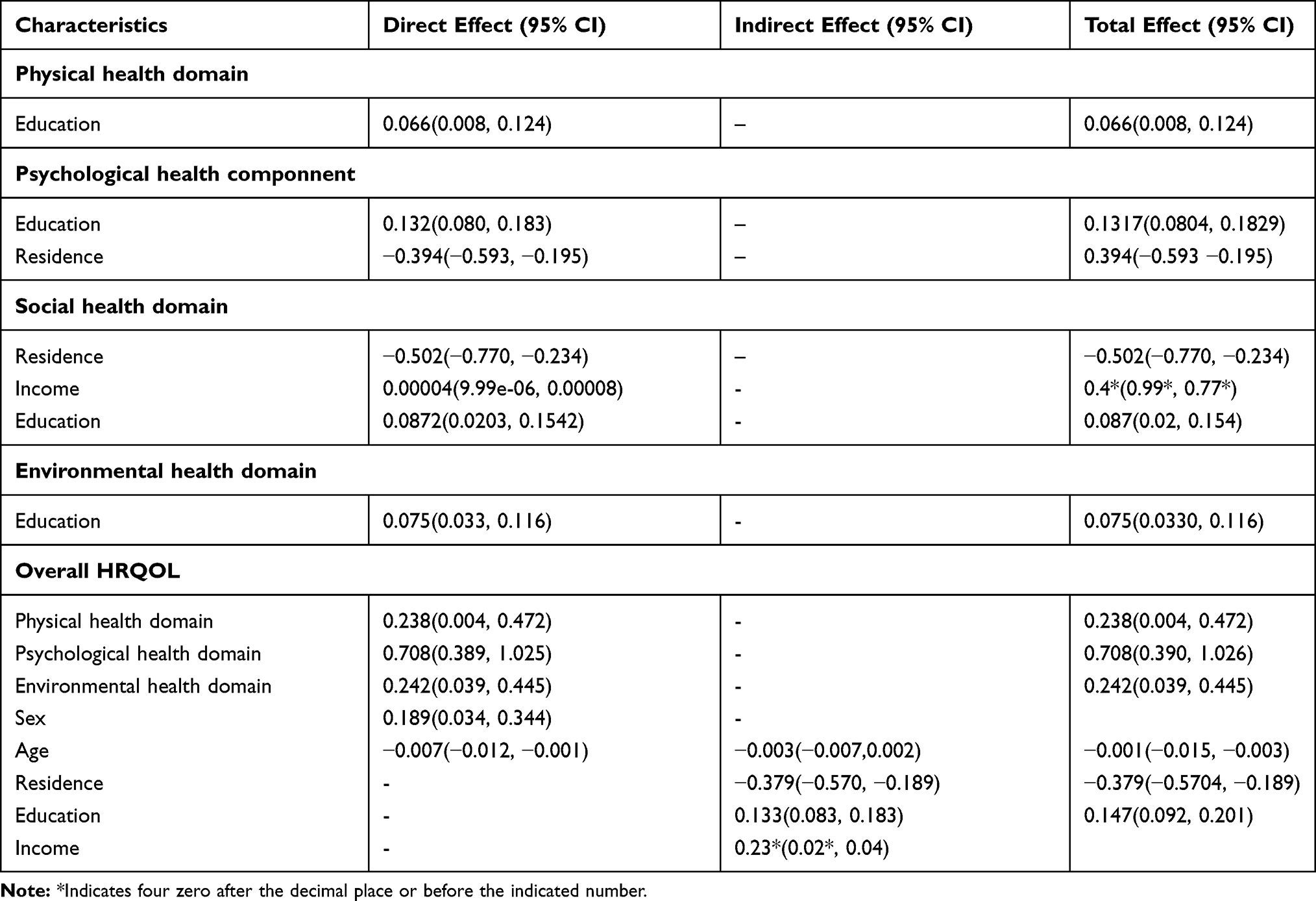 |
Table 2 The Direct, Indirect, and Total Effect of Socio-Demographical and HRQOL Domains Among Patients with MI Attending at Cardiac Center Ethiopia, 2020 |
In the hypothetical model, the following were statistically significant: physical health domain path in the HRQOL path (P = 0.045), psychological health domain path in the HRQOL path (P < 0.001), environmental health domain path in the HRQOL path (P =0.02), sex path in the HRQOL path (P = 0.017), age path in the HRQOL path (P = 0.026). Physical health was significantly associated with educational level (P = 0.026); psychological health domain was significantly associated with residence (P < 0.001) and educational level (P < 0.001). Furthermore, the social health domain was significantly associated with residence (P < 0.001), educational level (P=0.011), and monthly income (p=0.011), and environmental health domain was associated with educational level (P<0.001). In the hypothetical model, physical health domain path (P = 0.045), psychological health domain path (P < 0.001), environmental health domain path (P = 0.02), sex path (P = 0.017) and age path (P = 0.026) in the HRQOL path were statistically significant (Figure 2).
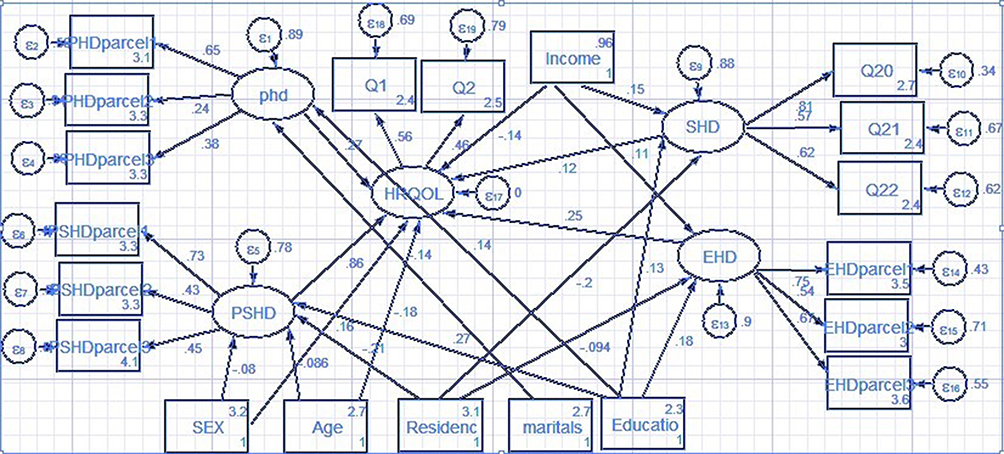 |
Figure 2 Structural equation model for a factor associated with HRQOL among patients with MI attending at cardiac center Ethiopia. Abbreviations: PHD, physical health domain; EHD, environmental health domain; SHD, social health domain; PSHD, psychological health domain; PHDparcil, average of Q3 and Q4; PHDparcil2, average of Q10 and 7; parcil13, average of Q4, Q8 and Q9; parcil21, average of Q13 and Q15; parcil22, average of Q10 and Q15; PHDparcil3, average of Q16, Q17, and Q17; PSHDparcil1, average of Q5 and Q6; PSHD parcil2, average of Q7, Q11; PSHDparcil3, average of Q19 and Q26; EHDparcil1, average of Q8, Q9 andQ25; EHD parcil2, average of Q12, Q13; EHDparcil3, average of Q14, Q23, and Q24. |
Test of the Goodness of Fit of the Hypothetical Model
The extent of SEM measures of overall model fit indicated corresponds to the empirical data. According to Browne and Cudeck, RMSEA values ≤ 0.05 can be considered as a good fit, values between 0.05 and 0.08 as an adequate fit, and values between 0.08 and 0.10 as a mediocre fit, whereas values > 0.10 are not acceptable.34 In this study, the RMSE value was 0.05. This indicates that the goodness of fit of the hypothetical model satisfied the recommended levels. The CFI ranges from zero to one with higher values indicating better fit; values greater than 0.95 interpreted as an acceptable fit. In this study, the CFI indicates that the goodness of fit of the hypothetical model satisfied the recommended level which was 1.00. Akaike’s information criterion (AIC) =31855.10; Bayesian information criterion (BIC)= 32158.3; Coefficient of determination (CD)=1.00; Log-likelihood = −15852.55. All of the tests of goodness of fit of the hypothetical model satisfied the recommended levels.
Effectiveness Analysis of the Hypothetical Model
The direct, indirect, and total effects of the factors associated with the HRQOL of the patients with MI are presented in Table 2. The psychological health domain had the greatest direct effect on the HRQOL with a score of 0.708. The environmental health domain had a direct effect on the HRQOL with a path coefficient of 0.242, and the physical health domain had a direct effect on HRQOL with a path coefficient of 0.238. Residence, education, and monthly income had an indirect effect on the HRQOL with a path coefficient of −0.379, 0.133, and <0.001, respectively at a significant p-value < 0.05. The psychological health domain had a total effect on HRQOL with a path coefficient of 0.708 (0.39, 1.026) at 95% CI (Table 2).
Discussion
In this study, we aimed to construct a hypothetical model and verify the significance of the direct/indirect paths of the model under the theoretical assumption that socio-demographic, physical, environmental, psychological, social health factors with the HRQOL of patients with MI. Direct comparisons with the findings of other studies are difficult because there are no other comprehensive HRQOL models of patients with MI survivors. In this study, the overall mean score of HRQOL among patients with MI survivors was 49.29±14.83. This finding revealed that the overall QOL among MI patients was low. This is consistent with a study conducted in the Republic of China,14 United States of America35, and Hong Kong.36 The possible reason for the low HRQOL might be due to the profound physiological and psychological impact of the acute onset of MI, as well as the psychosocial impact of hospitalization. This finding is higher than a study conducted in South Korea in which the mean score of HRQoL was 44.3±27.66. On the other hand, the current finding is lower than that of a study done in Myanmar in which the overall mean score was 82.02±8.84.14
In our study, from the four domains of HRQOL, the social health domain had the highest score followed by the psychological health domain. These scores were higher than those of the United States of America35 and Hong Kong.36 The possible reason for the variation might be due to the approach in measurement tool, the study design, and socio-cultural differences. In this study, HRQOL was assessed by using a 26-item WHOQOL-BREF questionnaire, while in the Republic of China the patient’s QOL was assessed by using the Short Form 36 health survey and the Myocardial Infarction Dimensional Assessment Scale. In this study, the physical health domain and environmental health domain mean score was lower as compared with the psychological and social health domain. In the current study Based on their response, one-third of the study participants reported that their quality of life was neither good nor poor, while more than one-fourth of the participants had poor QOL. Regarding health satisfaction, more than one-third of the study participants were very dissatisfied with their health and only 13.5% of the study participants were satisfied with their health. In this study, psychological factors were the most significant predictors of HRQoL of patients after MI which was consistent with previous studies.25,37
The current study revealed that the psychological health domain had the strongest and most direct effect on the HRQOL. In addition, in the structural modeling, the physical, psychological, environmental health domains, sex, and age paths were significantly associated with the HRQOL path. The physical role and general health of patients might be well recovered if there is symptomatic alleviation from efficient treatment and rehabilitation.38 This may be because patients may choose suitable work to adapt their physical functions and safety.39 However, the social function, psychological health, and emotional role of these patients were unsatisfactory which was mainly because patients could not coordinate the relationship between treatment and work.40 Oginska-Bulik found that “younger patients with MI had a higher quality of life”.41 This can be explained by higher physical functioning in younger patients after MI.42
Psychosocial factors are modifiable factors. It very well may be more powerful and proficient to focus on these determinant factors for recuperating health-related quality of life among patients with myocardial infarction when patients go through the interaction of medicines. Age and sex were the socio-demographic factors associated with HRQOL in patients with MI. This study reported that age was significantly associated with HRQoL in patients with MI. This is consistent with other previous studies.14,18,25,41,43 Based on the knowledge that MI incidence increases with age, and researchers would anticipate that older patients tend to experience several limitations such as cognitive impairment, loss of personal autonomy, or anxiety and depression. These situations again result in a poor quality of life.44 And also this study, reported that sex was significantly associated with HRQoL in patients with MI. This study was in line with other previous studies.14,25,41 In this study, social support was not a significant predictor of HRQoL. This is inconsistent with another previous study.45 The possible justification for this study might be due to the difference in sample size, socio-cultural difference, and measurement tool.
Besides, in Ethiopia, social relation health might be their social culture that gives support for diseased individuals with chronic diseases, and Patients manifest more physically than socially. This finding is supported by other studies that were conducted southwest46 and northwest47 Ethiopia among chronic diseases patients. Despite the current study, different studies showed that patients with low social support continued to have a lower HRQOL,18,45,48–50 and recommended that health providers must help patients by identifying available social support and breaking barriers to use social resources.
Strength of the Study
The HRQOL was assessed by using a standardized tool (WHOQOL_BREF) that is validated for both developed and developing countries. The present study also used structural equation modeling (SEM) that enables simultaneous analysis of the effect of multiple independent variables on several outcome variables and the subsequent direct evaluation of the respective effect of the independent variables on the outcome variables.
Limitations of the Study
Since this was a quantitative study it may not explore all the associated factors and it is advisable to use both quantitative and qualitative methods as well. Moreover, the present study has been conducted in a single-center which limits the generalizability of the finding in Ethiopia; further multicenter studies are needed to address this issue.
Conclusion
Psychological health factors had the most substantial causal effect on health-related quality of life, which was larger than the causal effects of physical and environmental health-related factors. Psychological, physical, environmental health domain and sex were the factors significantly associated with HRQOL. Age had a direct, negative association with HRQOL; residence indirectly and negatively influenced the HRQOL, and HRQOL was also indirectly and positively affected by educational level. Developing and providing comprehensive interventions are necessary to assess and manage psychological, physical, and environmental health factors for improving the QOL of patients with myocardial infarction. Early intervention and integrating treatment services for patients with MI who tend to have worse HRQOL by focusing on adjustable factors like psychosocial situations would be more effective in helping them to improve HRQOL. The special treatment, where it is offered for older patients and those who have lower educational level are recommended that helping the recovery of HRQOL to the normative level after experiencing MI.
Abbreviations
CVD, Cardiovascular Disease; CHD, Coronary Heart Disease; HRQOL, Health-Related Quality Of Life; MI, Myocardial Infarction; QOL, Quality Of Life; SEM, Structural Equation Modeling; STEMI, ST-segment myocardial infarction; NSTEMI, Non-ST segment myocardial infarction.
Data Sharing Statement
All data about this study are contained and presented in this document.
Ethics Approval and Consent to Participate
Ethical clearance and approval were obtained from the University of Gondar, college medicine and health sciences, school of nursing research review committee. An official letter of agreement was acquired from the organizations of the cardiac center in Ethiopia. This study was conducted following the Declaration of Helsinki. Prior to data collection, the objective of the study was explained to the respondents and after their willingness, written consent was secured before filling the questioner. Therefore, informed written consent was obtained from the participants, and confidentially was maintained by omitting their identification.
Acknowledgments
The authors are deeply indebted to the University of Gondar, College of Medicine and Health Science for giving the ethics approval for this study. Finally, we would like to expand our heartfelt thanks to cardiac center-Ethiopia administrators, staff members as well as data collectors, and respondents.
Author Contributions
All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Goeddel LA, Hopkins AN, Fernando RJ, Núñez-Gil IJ, Ramakrishna H. Analysis of the 4th universal definition of myocardial infarction—key concepts and perioperative implications. J Cardiothorac Vasc Anesth. 2019;33(12):3486–3495. doi:10.1053/j.jvca.2019.01.030
2. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–e603.
3. World Health Organization. Cardiovascular Diseases (Cvds). World Health Organisation; 2017.
4. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237–269.
5. Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A. Growing epidemic of coronary heart disease in low-and middle-income countries. Curr Probl Cardiol. 2010;35(2):72–115. doi:10.1016/j.cpcardiol.2009.10.002
6. Karimi M, Brazier J. Health, health-related quality of life, and quality of life: what is the difference? Pharmacoeconomics. 2016;34(7):645–649. doi:10.1007/s40273-016-0389-9
7. De Smedt D, Clays E, De Bacquer D. Measuring health-related quality of life in cardiac patients. Eur Heart J. 2016;2:149–150. doi:10.1093/ehjqcco/qcw015
8. Foxwell R, Morley C, Frizelle D. Illness perceptions, mood and quality of life: a systematic review of coronary heart disease patients. J Psychosom Res. 2013;75(3):211–222. doi:10.1016/j.jpsychores.2013.05.003
9. Eriksson M, Asplund K, Hochwälder J, Svedlund M. Changes in hope and health‐related quality of life in couples following acute myocardial infarction: a quantitative longitudinal study. Scand J Caring Sci. 2013;27(2):295–302. doi:10.1111/j.1471-6712.2012.01032.x
10. Morrow DA. Myocardial Infarction: A Companion to Braunwald’s Heart Disease E-Book. Elsevier Health Sciences; 2016.
11. Saeed T, Niazi G, Almas S. Type-D personality: a predictor of quality of life and coronary heart disease. East Mediterr Health J. 2011;17(1):46–50.
12. Boersma SN, Maes S, Joekes K, Dusseldorp E. Goal processes in relation to goal attainment: predicting health-related quality of life in myocardial infarction patients. J Health Psychol. 2006;11(6):927–941. doi:10.1177/1359105306069095
13. Kang K, Gholizadeh L, Inglis SC, Han HR. Interventions that improve health-related quality of life in patients with myocardial infarction. Qual Life Res. 2016;25(11):2725–2737. doi:10.1007/s11136-016-1401-8
14. Wang W, Thompson DR, Ski CF, Liu M. Health-related quality of life and its associated factors in Chinese myocardial infarction patients. Eur J Prev Cardiol. 2014;21(3):321–329. doi:10.1177/2047487312454757
15. Members WG, Roger VL, Go AS, et al. Executive summary: heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation. 2012;125(1):188–197. doi:10.1161/CIR.0b013e3182456d46
16. Lee YM, Kim RB, Lee HJ, et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):100. doi:10.1186/s12955-018-0921-z
17. Israel Study Group on First Acute Myocardial Infarction Benyamini Yael PhD benyael@ post. tau. ac. il Roziner Ilan MA Goldbourt Uri PhD Drory Yaacov MD Gerber Yariv PhD. Depression and anxiety following myocardial infarction and their inverse associations with future health behaviors and quality of life. Ann Behav Med. 2013;46(3):310–321. doi:10.1007/s12160-013-9509-3
18. Hawkes AL, Patrao TA, Ware R, Atherton JJ, Taylor CB, Oldenburg BF. Predictors of physical and mental health-related quality of life outcomes among myocardial infarction patients. BMC Cardiovasc Disord. 2013;13(1):69. doi:10.1186/1471-2261-13-69
19. Mollon L, Bhattacharjee S. Health related quality of life among myocardial infarction survivors in the United States: a propensity score matched analysis. Health Qual Life Outcomes. 2017;15(1):235. doi:10.1186/s12955-017-0809-3
20. Kaur R. A descriptive study done to assess the quality of life among post myocardial infarction patients attending cardiac OPDs. MOJ Womens Health. 2017;4(6):00103.
21. Kim HM, Kim J, Hwang SY. Health-related quality of life in symptomatic postmyocardial infarction patients with left ventricular dysfunction. Asian Nurs Res. 2015;9(1):47–52. doi:10.1016/j.anr.2014.11.004
22. Runge MS, Stouffer G, Patterson C. Netter’s Cardiology E-Book. Elsevier Health Sciences; 2010.
23. Kanga K, Gholizadeha L, Inglisa SC, Hanb HR. Correlates of health-related quality of life in patients with myocardial infarction: a literature review. Int J Nurs Stud. 2017;73:1–16.
24. Sönmez Y, Uskun E, Pehlivan A. Knowledge levels of pre-school teachers related with basic first-aid practices, Isparta sample. Türk Pediatri Arsivi. 2014;49(3):238. doi:10.5152/tpa.2014.1581
25. Arnold SV, Masoudi FA, Rumsfeld JS, Li Y, Jones PG, Spertus JA. Derivation and validation of a risk standardization model for benchmarking hospital performance for health-related quality of life outcomes after acute myocardial infarction. Circulation. 2014;129(3):313–320. doi:10.1161/CIRCULATIONAHA.113.001773
26. Bucholz EM, Strait KM, Dreyer RP, et al. The effect of low perceived social support on health outcomes in young patients with acute myocardial infarction: results from the VIRGO study. Circ Cardiovasc Qual Outcomes. 2014;7(suppl_1):A104–A104.
27. Lidell E, Höfer S, Saner H, Perk J, Hildingh C, Oldridge N. Health-related quality of life in European women following myocardial infarction: a cross-sectional study. Eur J Cardiovasc Nurs. 2015;14(4):326–333. doi:10.1177/1474515114535330
28. Pettersen KI, Reikvam A, Rollag A, Stavem K. Understanding sex differences in health-related quality of life following myocardial infarction. Int J Cardiol. 2008;130(3):449–456. doi:10.1016/j.ijcard.2007.10.016
29. Sebah MB, Tadesse KD, Mohammed AD, et al. Immediate outcome and predictors of percutaneous Mitral Balloon commissurotomy: a 5 years experience in cardiac center Ethiopia. Cardiol Cardiovasc Res. 2019;3(3):55. doi:10.11648/j.ccr.20190303.13
30. Schumacker RE, Lomax RG. A Beginner’s Guide to Structural Equation Modeling. psychology press; 2004.
31. Kang K. Health-related quality of life in patients with myocardial infarction: trends and predictors. 2018.
32. Woo JP. The Concept and Understanding of Structural Equation Model. Seoul: Hannarae; 2012:275–361.
33. Matsunaga M. Item parceling in structural equation modeling: a primer. Commun Methods Meas. 2008;2(4):260–293. doi:10.1080/19312450802458935
34. Ne MW, Cudeck R. Alternative ways of assessing model fit. Test Struct Equ Model. 1993;154:136.
35. Gandek B, Sinclair SJ, Kosinski M, Ware JJE. Psychometric evaluation of the SF-36® health survey in medicare managed care. Health Care Financ Rev. 2004;25(4):5.
36. Doris S, Thompson DR, Yu CM, Oldridge NB. Assessing HRQL among Chinese patients with coronary heart disease: angina, myocardial infarction and heart failure. Int J Cardiol. 2009;131(3):384–394. doi:10.1016/j.ijcard.2007.10.043
37. Ginzburg K, Ein-Dor T. Posttraumatic stress syndromes and health-related quality of life following myocardial infarction: 8-year follow-up. Gen Hosp Psychiatry. 2011;33(6):565–571. doi:10.1016/j.genhosppsych.2011.08.015
38. Dreyer RP, Xu X, Zhang W, et al. Return to work after acute myocardial infarction: comparison between young women and men. Circ Cardiovasc Qual Outcomes. 2016;9(2_suppl_1):S45–S52. doi:10.1161/CIRCOUTCOMES.115.002611
39. Lamberti M, Ratti G, Gerardi D, et al. Work-related outcome after acute coronary syndrome: implications of complex cardiac rehabilitation in occupational medicine. Int J Occup Med Environ Health. 2016;29(4):649. doi:10.13075/ijomeh.1896.00643
40. Mirmohammadi SJ, Sadr-Bafghi SM, Mehrparvar AH, et al. Evaluation of the return to work and its duration after myocardial infarction. ARYA Atheroscler. 2014;10(3):137.
41. Ogińska-Bulik N. Type D personality and quality of life in subjects after myocardial infarction. Kardiologia Polska. 2014;72(7):624–630. doi:10.5603/KP.a2014.0066
42. Park S-K, Kim H-S, Cho I-S, Ham O-K. Gender differences in factors influencing quality of life among patients with coronary artery disease. J Korean Acad Fundam Nurs. 2009;16(4):497.
43. Ho PM, Eng MH, Rumsfeld JS, et al. The influence of age on health status outcomes after acute myocardial infarction. Am Heart J. 2008;155(5):855–861. doi:10.1016/j.ahj.2007.11.032
44. Audi G, Korologou A, Koutelekos I, et al. Factors affecting health related quality of life in hospitalized patients with heart failure. Cardiol Res Pract. 2017;2017:1–12. doi:10.1155/2017/4690458
45. Rankin SH, Fukuoka Y. Predictors of quality of life in women 1 year after myocardial infarction. Prog Cardiovasc Nurs. 2003;18(1):6–62. doi:10.1111/j.0889-7204.2003.01570.x
46. Muze M, Hailu E, Woldemichael K, Fekecha B. Health related quality of life and its associated factors among diabetic patients attending diabetes clinic in Jimma university teaching hospital, Ethiopia, 2014. J Diabetes Metab. 2017;8(751):2.
47. Reba K, Argaw Z, Walle B, Gutema H. Health-related quality of life of patients with diagnosed type 2 diabetes in Felege Hiwot Referral Hospital, North West Ethiopia: a cross-sectional study. BMC Res Notes. 2018;11(1):1–6.
48. Bucholz EM, Rathore SS, Gosch K, et al. Effect of living alone on patient outcomes after hospitalization for acute myocardial infarction. Am J Cardiol. 2011;108(7):943–948. doi:10.1016/j.amjcard.2011.05.023
49. Boersma SN, Maes S, van Elderen T. Goal disturbance predicts health‐related quality of life and depression 4 months after myocardial infarction. Br J Health Psychol. 2005;10(4):615–630. doi:10.1348/135910705X52525
50. Leifheit-Limson EC, Reid KJ, Kasl SV, et al. Changes in social support within the early recovery period and outcomes after acute myocardial infarction. J Psychosom Res. 2012;73(1):35–41. doi:10.1016/j.jpsychores.2012.04.006
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.